Article Text

Abstract
Objective To analyse the treatment outcome of patients with ankylosing spondylitis (AS) in the European AS infliximab cohort (EASIC) study after a total period of 8 years with specific focus on dosage and the duration of intervals between infliximab infusions.
Methods EASIC included patients with AS who had received infliximab for 2 years as part of the ASSERT trial. After that period, rheumatologists were free to change the dose or the intervals of infliximab. Clinical data were status at baseline, end of ASSERT and for a total of 8 years of follow-up.
Results Of the initially 71 patients with AS from EASIC, 55 patients (77.5%) had completed the 8th year of anti-tumour necrosis factor (TNF) treatment. Of those, 48 patients (87.3%) still continued on infliximab. The mean infusion interval increased slightly from 6 to 7.1±1.5 weeks, while 45.8% patients had increased the intervals up to a maximum of 12 weeks. The mean infliximab dose remained stable over time, with a minimum of 3.1 mg/kg and a maximum of 6.4 mg/kg. In patients receiving <5 mg/kg infliximab, the mean infusion interval increased to 7.0±1.2 weeks. In total, the mean cumulative dose per patient and per year decreased from 3566.30 to 2973.60 mg.
Conclusions We could observe that over a follow-up of 8 years of treatment with infliximab, >85% patients still remained on the same treatment, without any major safety events. Furthermore, both the infusion intervals and also the mean infliximab dose were modestly reduced in ≥70% of the patients without the loss of clinical efficiency.
- Ankylosing Spondylitis
- TNF-alpha
- Inflammation
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Key messages
What is already known about this subject?
Anti-TNF treatment is the gold standard in patients with axial spondyloarthritis. Patients treated with anti-TNF need to stay on this treatment over many years.
What does this study add?
Doses of infliximab in patients with axial spondyloarthritis may be modified and decreased in the long-term.
How might this impact on clinical practice?
Physicians may consider adapting the doses of infliximab in patients who show good and sustained clinical response in the long term.
Ankylosing spondylitis (AS), the main subtype of spondyloarthritides (SpA), is a chronic inflammatory rheumatic disease that affects about 0.5% of the adult Caucasian population and usually starts in early adulthood.1 AS is clinically characterised by inflammatory back pain due to sacroiliac and/or spinal inflammation which may eventually lead to an increase in new bone formation.
Non-steroidal anti-inflammatory drugs are considered as first line pharmacological therapy for AS. However, international recommendations advise the use of tumour necrosis factor (TNF) blockers for patients with AS who have persistently high disease activity despite conventional treatment.2
Several trials have shown that treatment with infliximab is efficacious in patients with active AS, confirming the findings of the pivotal Ankylosing Spondylitis Study for the Evaluation of Recombinant Infliximab Therapy (ASSERT) trial with 279 patients.3 MRI revealed a significant decrease in spinal inflammation in this study.4 Whether TNF blockers slow or inhibit structural damage in AS is still a matter of debate.5
Long-term data on the clinical efficiency and safety of anti-TNF therapy in AS are still scarce.6 7 However, such data are critical for appropriate economic analyses related to anti-TNF therapy.8
The European AS infliximab cohort (EASIC) was initiated by a group of European rheumatologists as an open label investigator-driven international multicentre trial9 with patients who had received infliximab for 2 years as part of the ASSERT trial.10 In this trial, which was one of the first trials with anti-TNF therapy, the disease activity of the included patients was relatively high as compared to later clinical trials with increased but still showed relatively milder signs and symptoms of disease activity. All the patients were initially treated with infliximab at the usual dosage of 5 mg/kg after the initial saturation phase. After 2 years of continuous treatment (end of ASSERT, extension phase to EASIC), rheumatologists were free to change the dose or the intervals of infliximab. The latest data of all the patients after 7 years of continuous infliximab treatment are now being published with the focus on treatment efficiency and safety.11
In the current report, we present the results of the patients completing the EASIC extension after a total treatment period of 8 years and with specific focus on dosage and the duration of intervals between infliximab infusions.
Of the 71 patients with AS who were initially included in EASIC, 55 patients completed the eighth year of anti-TNF treatment (77.5%). Of those, 48 patients still continued on infliximab (87.3%), while the remaining 7 patients switched to another biological agent for different reasons (12.7%). The reasons for dropping out of EASIC have already been reported elsewhere.10 At baseline, the mean age of these 55 patients was 50.6±8.5 years and 40 patients (83.3%) were male.
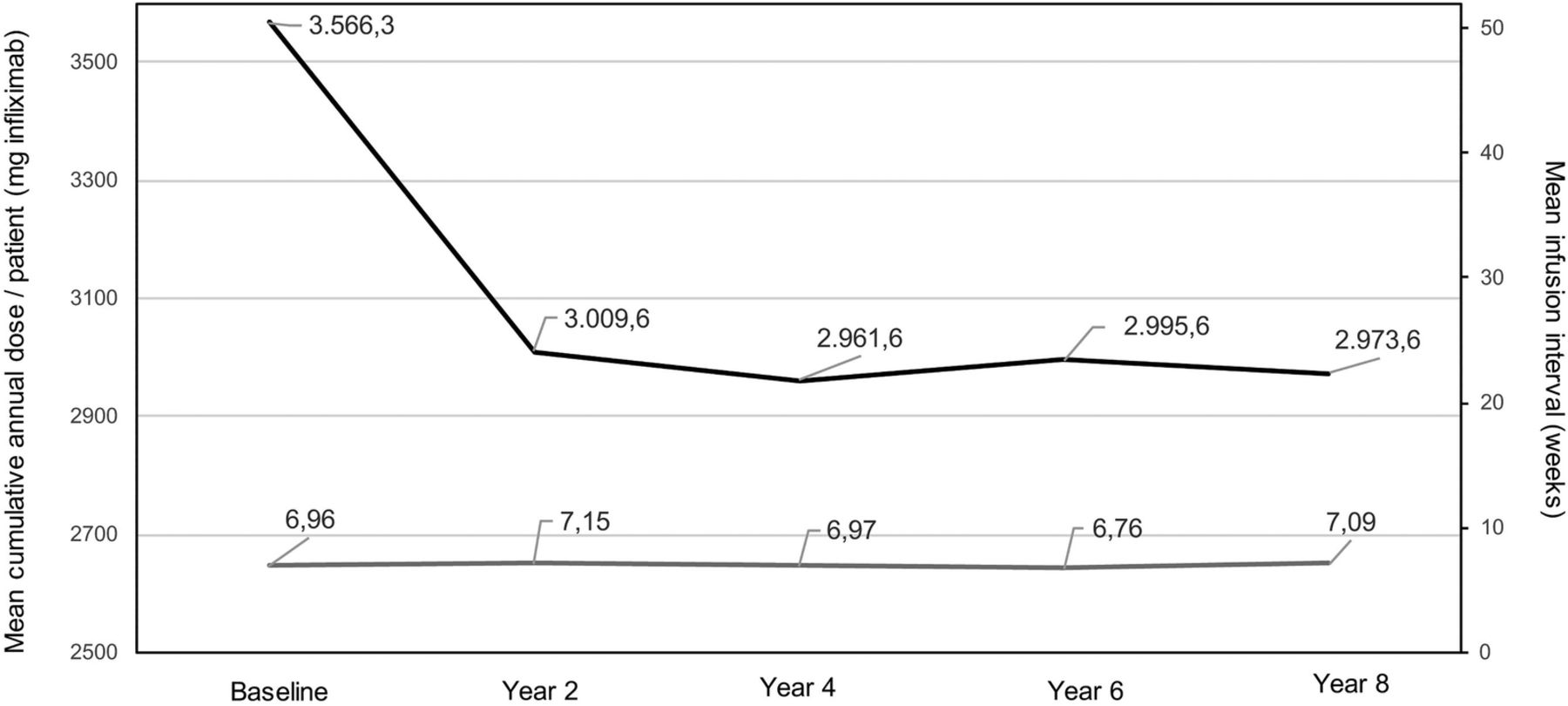
The mean interval between infusions increased slightly between year 2 (end of ASSERT) and year 8, from 6.0±1.0 weeks (as per initial study protocol) to 7.1±1.5 weeks, respectively. Overall, 24/48 patients (50%) still received infliximab in a standardised way with 6-week intervals between infusions, while 22/48 patients (45.8%) had increased the intervals up to a maximum of 12 weeks and 2/48 patients (4.2%) received infliximab every 5 weeks. The mean dose and the mean weight of the patients remained stable over time. The mean weight was 82.3±15.1 kg at start of ASSERT (baseline), 82.2±15.6 kg at the end of ASSERT (year 2) and 82.5±15.5 kg at the end of EASIC (year 8). The mean dose of infliximab per infusion and per patient was 4.7±0.8 mg/kg at baseline, 4.6±0.8 at year 2 and 4.7±0.8 at year 8, with a minimum dose of 3.1 mg/kg and a maximum dose of 6.4 mg/kg. In more detail, 30 patients (62.5%) were receiving a dose <5 mg/kg, 5 patients (10.4%) remained at 5 mg/kg and 13 patients (27.1%) had increased their dose to up to 6.4 mg/kg. Furthermore, there were numerical differences between the mean dose of infliximab and the dose interval at the end of the study. In the group of patients receiving a dose of <5 mg/kg of infliximab, the mean infusion interval at year 8 was 7.0±1.2 weeks, while in the group receiving a dose of 5 mg/kg of infliximab it was 7.4±1.3 weeks and in the group receiving a dose >5 mg/kg of infliximab was 6.6±1.9 weeks. In total, the mean cumulative dose per patient and per year decreased from 3566.30 to 2973.60 mg (figure 1, Wilcoxon p<0.001).
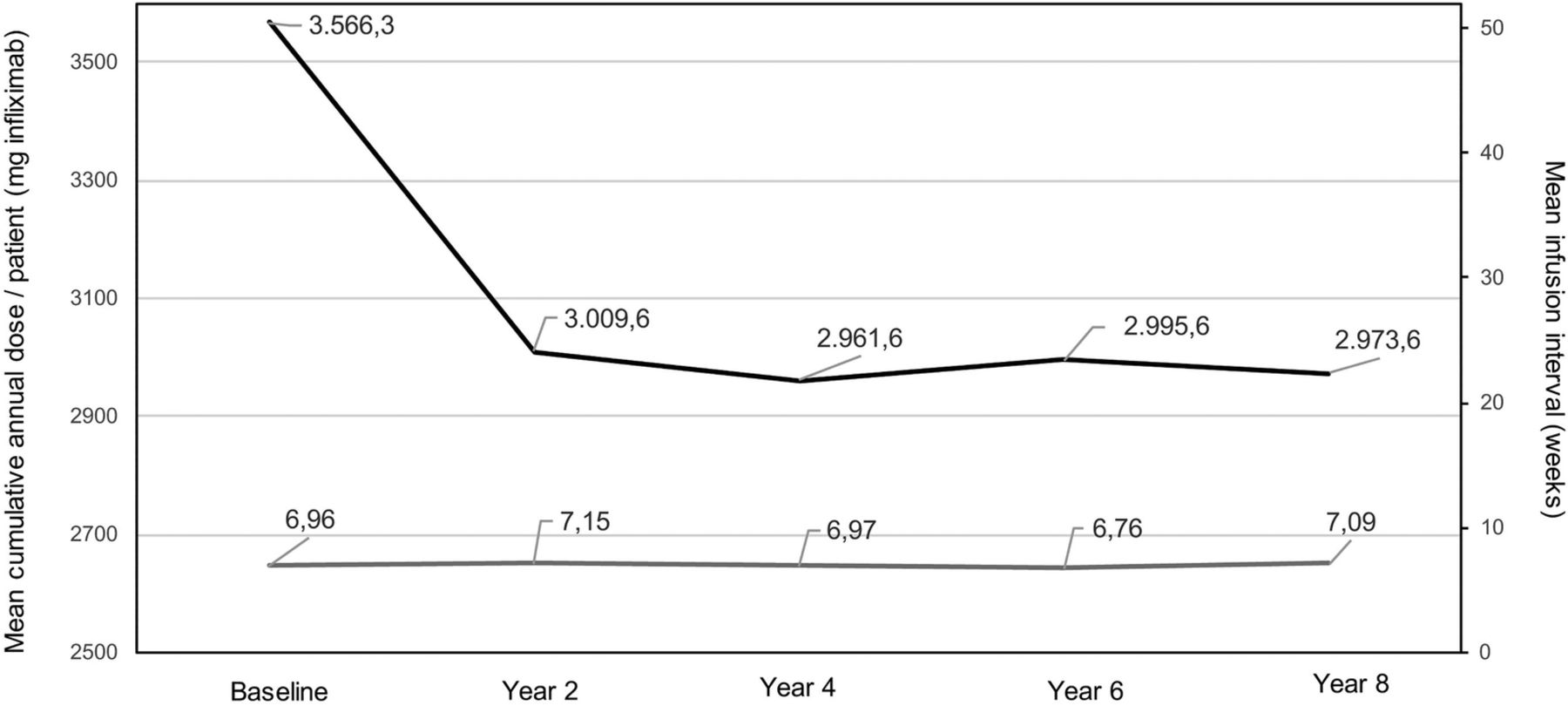
Course of the mean cumulative dose per patient and year (black line, in mg infliximab) and mean infusion interval (grey line, in weeks) over the 8 years of treatment with infliximab in European ankylosing spondylitis infliximab cohort (EASIC).
Throughout the observation period, the mean Bath AS Disease Activity Index, Bath AS Functional Index, and the patient's global and C reactive protein values remained low without differences between year 2 and year 8 of the study, with exception of the Bath AS Metrology Index, which initially improved but returned to values similar to those noted at baseline (figure 2). This observation made late in the course of the study can be possibly explained by the natural decrease in spinal mobility that develops with age—similar to what has been described also for normal individuals over a similar time period.12

{kind=link}
{kind=link}
Course of disease related outcomes for efficiency over the entire study period of 8 years. Data are presented are mean values for all completers of the present analysis still being treated with infliximab (n=48, CRP mg/dL). BASDAI, Bath Ankylosing Spondylitis Disease Activity Index; BASFI, Bath Ankylosing Spondylitis Functional Index; BASMI, Bath Ankylosing Spondylitis Metrology Index; CRP, C reactive protein.
In this present additional follow-up study there were no additional safety signals as compared to previous reports on EASIC.10 ,13
Taken together, the EASIC cohort is one of the largest cohorts of patients with AS (or radiographic axial SpA) receiving treatment with infliximab. These results confirm the favourable outcome of patients with AS who received anti-TNF therapy over many years. The persistently decreased values of the clinical variables suggest a good control of disease activity and function. We could observe that over a follow-up period of 8 years of treatment with infliximab, including 5 years of treatment in daily practice and not based on a standardised treatment protocol, more than 85% of the patients still remained on infliximab treatment, without experiencing any major safety events. Furthermore, the infusion intervals and the mean infliximab dose, were modestly reduced in ≥70% of the patients without any loss of clinical efficiency.
As far as we are aware, this is a rather unique experience with the use of a TNF blocker in patients with AS in a real world setting. Since the data were collected in different European centres, a bias due to inclusion of patients from only one center has been avoided. Nevertheless, larger studies would be helpful to confirm the results of this observational study.
Acknowledgments
The authors would like to acknowledge all the patients who continued supporting the efforts during the 8-year period of this study.
References
Footnotes
Funding Janssen Biologics provided financial support for the conduction of this investigator-initiated study.
Competing interests None declared.
Ethics approval The Ethical committees of all participating centres approved this study.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement No additional data are available.