Article Text

Abstract
Introduction Decreasing the diagnostic delay in axial spondyloarthritis (axSpA) remains a major challenge. Here, we assessed the value of serum inflammatory biomarkers to distinguish early axSpA from other pathologies in a large cohort of patients referred with early back pain.
Methods Serum c reactive protein (CRP), erythrocyte sedimentation rate (ESR) and calprotectin were determined in the SPondyloArthritis Caught Early (SPACE) cohort (n=310), an early back pain inception cohort. Additionally, explorative serum biomarkers derived from the literature (interleukin-27 (IL-27), human β-defensin-2 (hBD-2) and lipcolin-2 (LCN-2)) were determined by ELISA in full-blown patients with ankylosing spondylitis (AS) (n=21) and healthy controls (n=20).
Results Serum CRP and ESR levels were not elevated in early axSpA versus ‘control’ back pain patients. Serum calprotectin was elevated in early axSpA versus controls (p=0.01) but failed to identify early axSpA at the individual level (positive predictive value of 38.7%). As to explorative biomarkers, serum levels of IL-27 were not detectable, and hBD-2 and LCN-2 serum levels were not elevated in full-blown AS versus healthy controls (p=0.572, p=0.562, respectively). Therefore, these markers were not further determined in the SPACE cohort.
Conclusions None of the candidate serum inflammatory markers were useful as diagnostic markers in the early phase of axSpA.
- Spondyloarthritis
- Inflammation
- Low Back Pain
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Key messages
What is already known about this subject?
Some serum markers of inflammation are elevated in a fraction of the patients with full blown axial spondyloarthritis in comparison with healthy individuals. However, there are no established diagnostic serum biomarkers allowing the identification of axial spondyloarthritis in patient with early back pain.
What does this study add?
This study demonstrated that serum biomarkers of inflammation, including CRP and ESR, are not elevated in patients with early axial spondyloarthritis. Calprotectin levels were slightly elevated, but lacked specificity and sensitivity to be applied as a diagnostic biomarker.
How might this impact clinical practice?
Taken together with a series of other studies, our data suggest that the disease processes driving axial spondyloarthritis are not reflected by alterations in the peripheral blood compartment. Direct visualization of these processes, for example by molecular imagingof affected tissues, might be a more successful approach to identify biomarkers for axial spondyloarthritis.
Introduction
Reliable diagnosis of axial spondyloarthritis (axSpA) in the earliest phases of the disease remains an important unmet medical need. Ample evidence indicates that (1) signs and symptoms of active disease are as severe in early disease as in full-blown disease, with similar impact on function and quality of life1–3 and (2) active early axSpA can be effectively treated with non-steroidal anti-inflammatory drugs (NSAIDs) and/or tumour necrosis factor inhibitors (TNFi).4–6 Moreover, current treatments fail to significantly inhibit pathological new bone formation when started in full-blown disease;7–9 although awaiting formal proof, starting the same treatments in very early disease may also impact on structural progression.10 ,11 Although the time between first symptoms and diagnosis of axSpA has already been significantly reduced over the past decade by a combination of early referral strategies and the use of MRI to image axial inflammation,12–16 it remains a challenge to further reduce the diagnostic delay and to reliably distinguish early back pain due to axSpA from other causes of back pain.17–19
One potential way to address this challenge is the use of serum inflammatory biomarkers. A couple of inflammatory biomarkers have been reported to be elevated in active, full-blown axSpA. C reactive protein (CRP) and erythrocyte sedimentation rate (ESR) are both acute-phase reactants which are elevated in active SpA and decrease on effective treatment.20–23 Moreover, calprotectin (also called S100A8/A9), a calcium binding protein, is expressed and secreted during macrophage infiltration in SpA synovitis.24–26 Calprotectin was recently shown to be a good serum biomarker for treatment responses in proof-of-concept trials in SpA and to independently predict radiographic progression in axSpA.27 ,28 Despite their value at the group level, the value of these serum biomarkers for diagnosis of axSpA in patients with early back pain remains unknown as they are neither very sensitive (eg, only one-third of patients with active ankylosing spondylitis (AS) have an elevated CRP)20 ,22 nor specific as they reflect inflammation (whatever the origin) rather than axSpA as such.
Besides these inflammatory biomarkers that were already extensively studied in AS, our recent literature review identified a few other potentially interesting serum biomarkers (M. Turina et al, submitted for publication). Lin et al29 recently described that levels of interleukin-27 (IL-27), a heterodimeric cytokine composed of p28 and Epstein-Barr Virus-induced gene 3 (EBI3) which belongs to the IL-12 family, were elevated in full-blown AS when compared with healthy controls but this finding has not yet been confirmed in an independent study. Human β defensin-2 (hBD-2) and lipocalin-2 (LCN-2) are two antimicrobial peptides which are up-regulated by IL-17 and are consistently found at elevated levels in serum of patients with active psoriasis and inflammatory bowel disease (IBD).30–35 Considering the central role of IL-17 in the pathophysiology of axSpA36–38 and the pathophysiological and clinical overlap of axSpA with psoriasis and IBD,39 these two biomarkers could also be of potential interest.
Accordingly, the aim of the present study was to assess the biomarker value of established inflammatory serum markers (CRP, ESR and calprotectin) as well as more exploratory biomarkers (IL-27, hBD-2 and LCN-2) for the diagnosis of axSpA in patients with early back pain.
Methods
Patients and samples
Serum was collected from 350 individuals after obtaining written informed consent to participate in the studies. Cohort 1 (SPondyloArthritis Caught Early (SPACE)) consisted of 310 individuals with ‘early’ back pain (defined as at least 3 and maximally 24 months) and an age of onset below 45 years, referred for early evaluation of potential AxSpA.40 This study protocol is approved by the local Ethics Committees of the participating centers. Cohort 2 consisted of 21 established patients with AS according to the modified New York (mNY) criteria; all patients were TNFi naïve.41 Full descriptions of these cohorts were reported previously.40 ,41 Finally, we also obtained serum from 19 healthy controls. Serum samples of cohorts 2 and 3 were retrieved from our biobank for this analysis according to the study protocol as approved by the Medical Ethics Committee of the Academic Medical Center/University of Amsterdam (2013_057).
Serum inflammatory biomarkers
From cohort 1, serum CRP and ESR levels were determined by local laboratories. Serum calprotectin levels were determined by ELISA (Hycult Biotech, Uden, the Netherlands) using a 1:60 dilution and according to the manufacturer's protocol.27 ,28
From cohort 2 and the healthy controls, serum IL-27, hBD-2 and LCN-2 levels were determined by ELISA according to the manufacturer's protocol (eBiosciences, San Diego, California; Phoenix pharmaceuticals, . Belmont California; and Research & Diagnostic Systems, Minneapolis, USA, respectively). The dilutions were 1:2, 1:50 and 1:50, respectively.
Statistical analysis
Data between groups were compared using Mann-Whitney U tests. P values <0.05 were considered statistically significant. Data were presented as box plots (Tukey) indicating the median and IQRs. Whiskers represent 1.5 IQR and black dots represent outliers. Statistical analyses were performed with SPSS V.21.0 (SPSS , Chicago, USA).
First, we compared CRP, ESR and calprotectin levels in patients of the SPACE cohort fulfilling the ASAS criteria versus those who did not fulfil the criteria. Second, we performed a subanalysis between patients fulfilling the imaging and a clinical arm of the ASAS criteria. The imaging arm can be fulfilled only if abnormal MRI (according to the ASAS/OMERACT definition) or X-sacroiliac joints (X-SIJs) (according to mNY) abnormalities are visible, and since calprotectin is an independent marker for axial spinal progression, it might better associate with the imaging arm of the ASAS criteria. Therefore, we conducted similar analyses in patients fulfilling the imaging arm (n=36) of the ASAS axSpA criteria versus those not fulfilling the criteria (n=191). Finally, we have tested the potential value of serum IL-27, hBD-2 and LCN-2 by comparing these levels in established active AS (cohort 2) versus healthy controls. Active disease in AS was defined as a Bath ankylosing spondylitis disease activity score (BASDAI) score >4.
Results
The baseline characteristics of cohort 1 are shown in table 1. Of note, 119 patients fulfilled the ASAS axSpA criteria (of which 36 fulfilled the imaging arm) and 191 did not fulfil the ASAS axSpA criteria.
Demographics and disease activity measures of the SPACE cohort (cohort 1)
CRP, ESR and calprotectin levels in early AxSPA
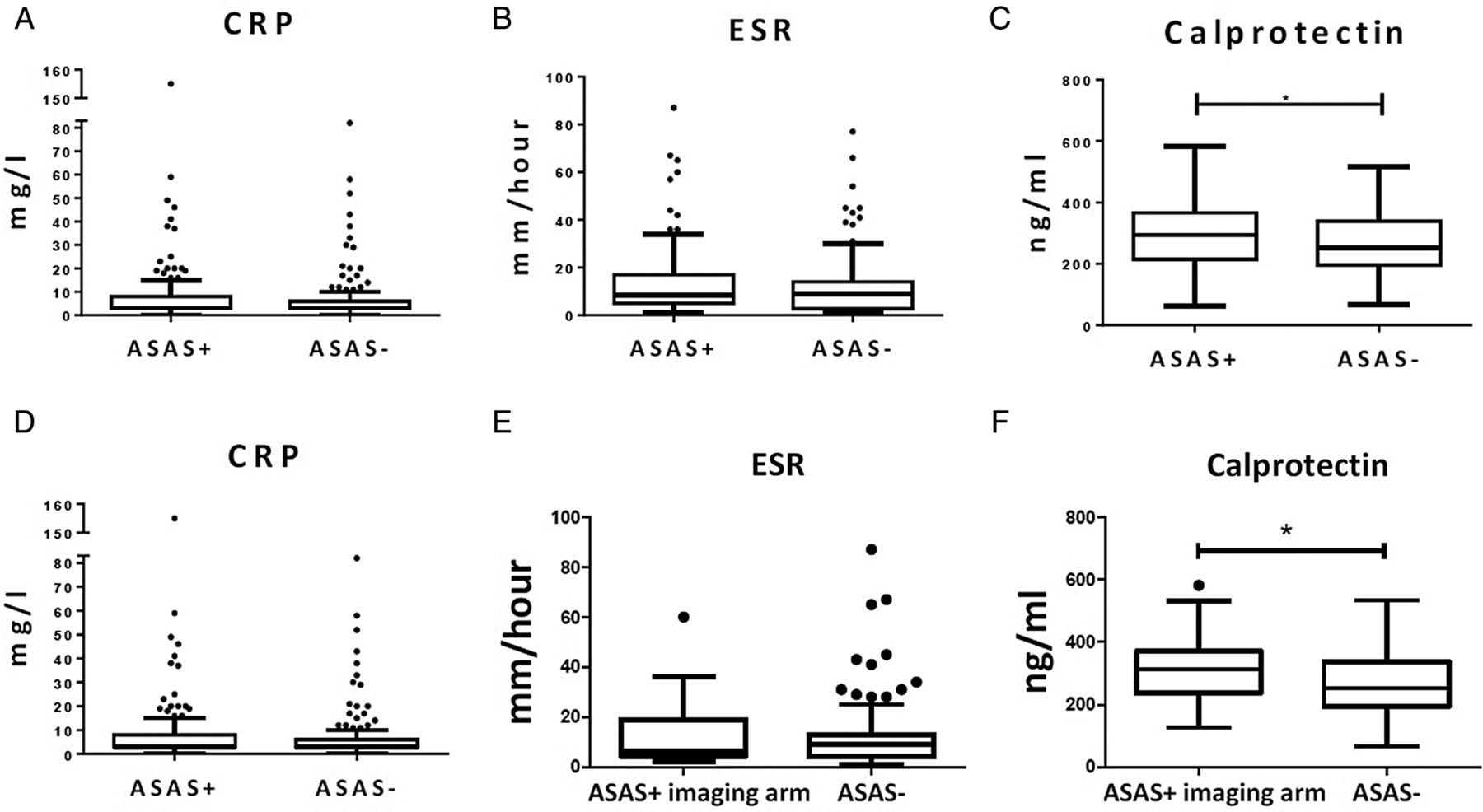
We first assessed whether CRP, ESR and calprotectin levels, known to be elevated in full-blown ankylosing spondylitis, were also elevated in patients with early back pain fulfilling the ASAS axSpA criteria.42 The median (IQR) levels of CRP (3.00 (3.00–8.00) mg/L vs 3.00 (3.00–6.00) mg/L; p=0.317) (figure 1A) and ESR (8.50 (5.00–17.00) mm/hour vs 9.00 (2.75–14.00) mm/hour; p=0.208) (figure 1B) were not significantly different between patients fulfilling and not fulfilling the ASAS axSpA criteria in the SPACE cohort. In contrast, calprotectin levels (294 214–367 ng/mL vs 251 196–339 ng/mL; p=0.01) were significantly higher in patients with early back pain fulfilling versus those not fulfilling the ASAS axSpA criteria (figure 1C). However, the discriminating value of calprotectin at the individual level was low: using a cut-off value for calprotectin at a specificity of 90% (412.40 ng/mL), the sensitivity was 10.0% and the positive predictive value (PPV) 38.7%. The post-test probability of having axSpA is thus not increased in comparison with the pretest probability (119 of 310 or 38.4%).
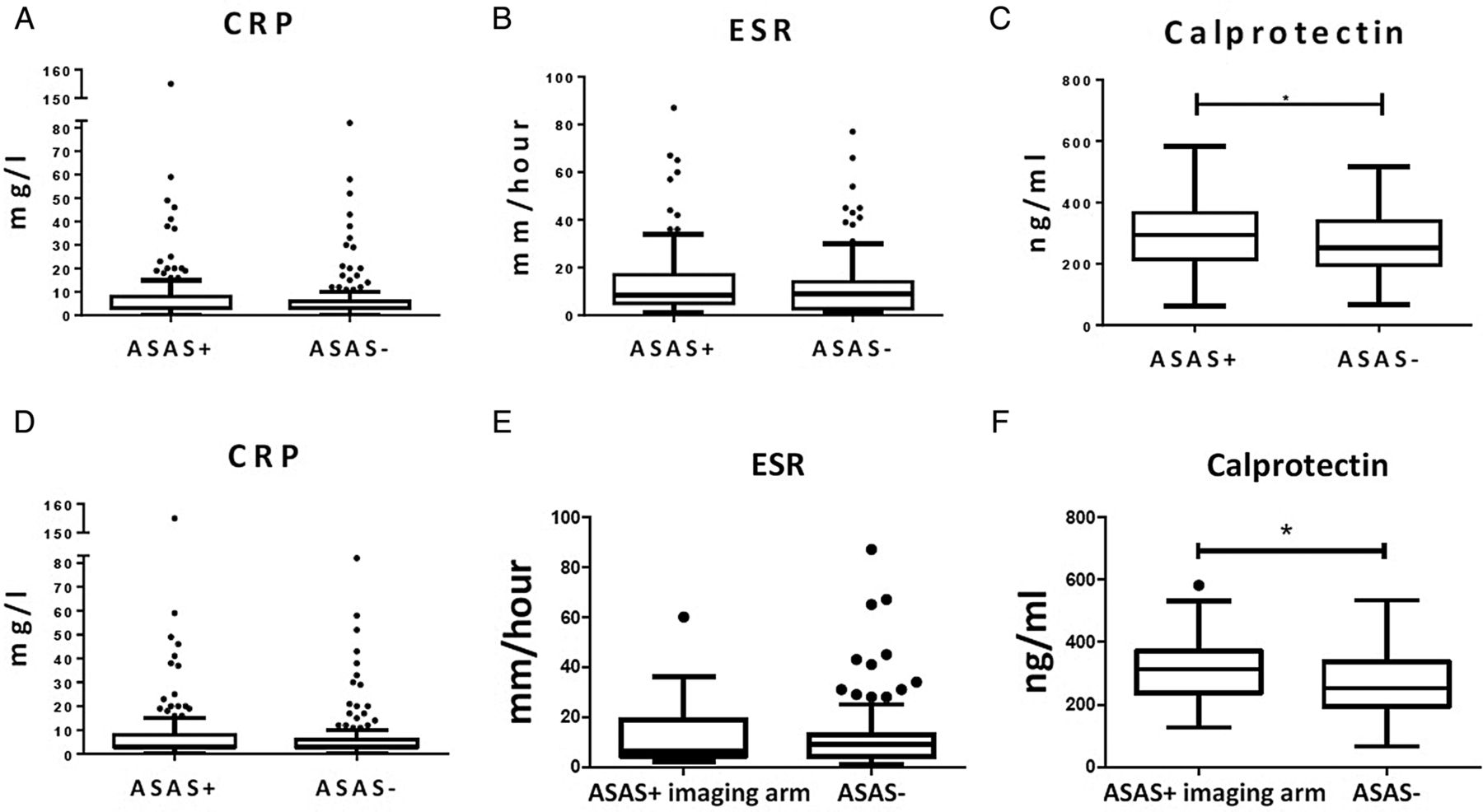
Serum levels of (A), C reactive protein (CRP), (B), erythrocyte sedimentation rate (ESR) and (C), calprotectin of cohort 1 (SPACE) with patients with early back pain fulfilling the ASAS axial spondyloarthritis (axSpA) criteria (n=119) versus patients with early back pain not fulfilling the ASAS axial SpA criteria (n=191); and serum levels of (D), CRP, (E), ESR and (F), calprotectin of cohort 1 (SPACE) with patients fulfilling the ASAS axSpA criteria according to the imaging arm (n=36) versus patients not fulfilling the ASAS axial SpA criteria (n=191). Boxplot (Tukey): Data are presented as median (IQR). Whiskers represent 1.5 IQR and black dots represent outliers. *p<0.05 by Mann-Whitney U test. ASAS, Assessment of SpondyloArthritis international Society.
CRP, ESR and calprotectin levels in the imaging arm of early AxSPA
We conducted similar analyses in patients fulfilling the imaging arm (n=36) of the ASAS axSpA criteria versus those not fulfilling the criteria (n=191). Again, levels of CRP (4.00 (3.00–9.00) mg/L vs 3.00 (3.00–6.00) mg/L; p=0.175) (figure 1D) and ESR (6.50 (4.25–19.00) mm/hour vs 9.00 (4.00–13.00) mm/hour; p=0.512) (figure 1E) were not different between the early patients with axSpA fulfilling the ASAS imaging arm and controls not fulfilling the ASAS criteria (figures 1D and E). Levels of calprotectin (313 (237–371) ng/mL vs 253 (195–338) ng/mL; p=0.01) were significantly higher in patients with early back pain fulfilling the imaging arm of the ASAS axSpA criteria versus those not fulfilling the criteria (figure 1F). As for the global axSpA group, however, the discriminatory value at the individual level was low. Using again a cut-off for calprotectin at the 90% specificity level (249.95 ng/mL) as an example, the PPV was 80% but the sensitivity was only 7.7%.
IL-27, hBD-2 and LCN-2 in full-blown as versus healthy controls
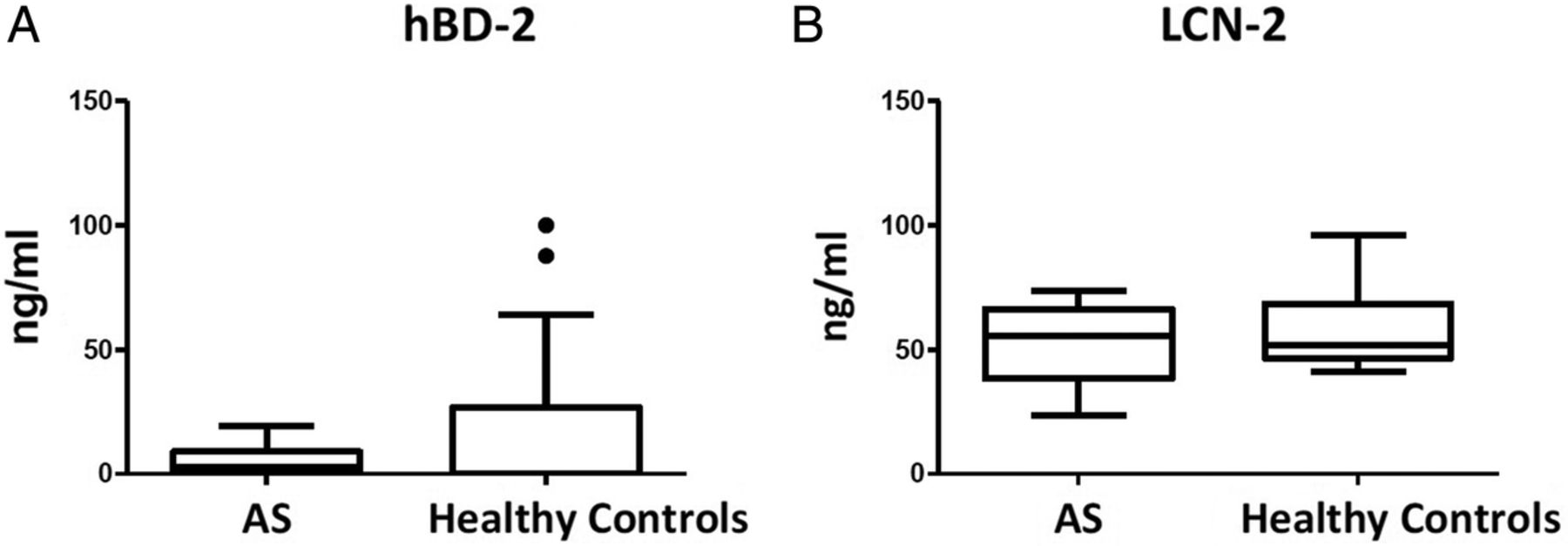
Since CRP, ESR and calprotectin were not useful as diagnostic biomarkers for axSpA in the SPACE cohort, we explored the potential value of three additional potential biomarkers. To this purpose, we first assessed their serum levels in established active AS (cohort 2) versus controls. IL-27 was undetectable in all but one serum sample of AS and healthy controls (data not shown). Serum levels of hBD-2 (median and IQR: 2.61 (0.00–8.93) ng/mL vs 0.00 (0.00–26.65) ng/mL; p=0.572) (figure 2A) and LCN-2 (55.47 (38.14–66.30) ng/mL vs 51.82 (46.59–68.57) ng/mL; p=0.562) (figure 2B) were clearly detectable but were not elevated in AS versus healthy controls. Since none of the three markers were elevated in AS, we did not proceed with testing the serum levels in the early back pain (SPACE) cohort.

{kind=link}
{kind=link}
Serum levels of (A), human β defensin-2 (hBD-2) and (B), lipocalin-2 (LCN-2) in active full-blown ankylosing spondylitis (AS, n=21) versus healthy controls (n=20). Data are presented as median (IQR). Boxplot (Tukey): data are presented as median (IQR). Whiskers represent 1.5 IQR and black dots represent outliers. *p<0.05 by Mann-Whitney U test. *p<0.05 by Mann-Whitney U test.
Discussion
We set up this study to assess whether inflammatory serum biomarkers can contribute to the diagnosis of axSpA in individuals presenting with early back pain. A first important finding is that serum CRP and ESR levels are not elevated in patients with early axSpA versus patients with back pain from different origins, despite the fact that elevated CRP is one of the features included in the ASAS axSpA criteria. Currently, there are no known true reliable and robust biomarkers available in established axial SpA (or ankylosing spondylitis). Therefore, testing several other biomarkers in early axial SpA was not useful. Here, we solely selected those biomarkers with some evidence as potential value in established axial SpA, including CRP, ESR and calprotectin in patients with early axial SpA. Accordingly, specificity, sensitivity and PPV analyses did not allow discrimination between patients and controls (data not shown). Importantly, however, the values of CRP and ESR were assessed here in a univariate analysis as the aim was to identify biomarkers that can easily and reproducibly be used to screen patients with early back pain to diagnose axSpA early. Although CRP and ESR do not appear to be useful tools for this purpose, this does not imply that these markers cannot be useful in individual patients when combined with other SpA features in a multivariate approach.
A second interesting finding is that, in contrast to CRP and ESR, calprotectin levels were significantly increased in early axSpA versus controls with back pain. This finding is consistent with a series of previous studies suggesting that calprotectin may slightly outperform CRP as a marker of tissue inflammation in SpA,26–28 ,43 potentially because this protein is released during infiltration of myeloid cells in tissues and may thus more directly reflect some of the pathological processes in SpA. However, the difference in serum calprotectin levels detected at the group level between early axSpA and controls was not robust enough in terms of sensitivity and specificity to translate in a useful discriminative tool to identify patients with axSpA. These findings are consistent with studies on other serum inflammatory markers including IL-6,44 ,45 α-2-macroglobulin,46 MMP-347–50 and PTX-3,51 which have been explored already in established axSpA but were not robust enough to apply in a diagnostic setting in early axSpA.
The lack of increase in serum levels of inflammatory biomarkers in axSpA versus controls is most likely related to two issues. First, these biomarkers do not reflect an SpA-specific process but rather inflammation in general and therefore lack specificity. Intercurrent infections or the presence of another chronic inflammatory disease may lead to elevated CRP, ESR and/or calprotectin in patients with mechanical back pain. One way to circumvent this issue would be to measure factors that are more specifically related to the immunopathology of axSpA, such as biomarkers reflecting the activation of the IL-23/IL-17 axis. Despite their value in psoriasis and IBD, however, the IL-17-driven antimicrobial peptides hBD-2 and LCN-2 were not elevated in axSpA. This might be due to the fact that these peptides are mainly produced by epithelial cells, including keratinocytes and gut epithelial cells, and that IL-17 may act on different cell types in axSpA. Further investigations in the mechanistic aspects of SpA immunopathology remain warranted to identify novel potential biomarkers.
A second reason for the absence of elevated serum levels of inflammatory markers such as CRP and ESR may be the fact that inflammation is restricted to specific tissue compartments and does not extend to the systemic circulation and/or lymphoid organs in SpA. This concept is supported by the fact that (1) in this study a majority of early patients with axSpA have CRP and ESR levels within the normal range despite active disease (n=171, 55.2%), (2) even in the subset of patients with positive MRI demonstrating active inflammation in the SI joints, CRP, ESR and calprotectin levels were not further increased and (3) also in established SpA with active disease CRP levels are elevated in only one-third of the patients.20–23 Accordingly, we previously focused our research on the immunopathology of affected tissues, such as the synovial membrane and found striking and reproducible alterations which, however, were not reflected in the peripheral blood compartment.52 ,53 If this concept is correct, the search for diagnostic markers should probably be focused on non-invasive measurements of tissue pathology (including MRI, positron emission tomography-CT and other types of molecular imaging) rather than on serum biomarkers.
Acknowledgments
The authors would like to thank D Pots and IC Blijdorp for their help in this study. The authors would also like to thank KL Germar for providing language help and for critically proofreading the article.
References
Footnotes
Contributors MT, NY and DB were involved in study concept and design. MT, NY, FvG, MvO, IB and ML acquired the data. MT, NY, FvG, MvO, IB, RR, ML, RL and DB were involved in analysis and interpretation of data. All authors were involved in drafting the article or revising it critically for important intellectual content and all authors approved the final version to be published.
Competing interests MCT was supported by an unrestricted fellowship from Janssen and DB was supported by a VICI grant from The Netherlands Organization for Scientific Research (NWO), by a Consolidator Grant from the European Research Council (ERC), and by a grant from the Dutch Arthritis Foundation (Reumafonds). NY, FvG, MvO, IJB, RR, CL and RL have no conflict of interests.
Patient consent Obtained.
Ethics approval LUMC, AMC, Regional Committee for Medical and Health Research Ethics (Oslo, Norway).
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement No additional data are available.