Article Text

Abstract
Objective Clinical trials have not consistently demonstrated differences between tumour necrosis factor inhibitor (TNFi) plus methotrexate and triple therapy (methotrexate plus hydroxychloroquine plus sulfasalazine) in rheumatoid arthritis (RA). The study objective was to estimate the efficacy, radiographic benefits, safety and patient-reported outcomes of TNFi–methotrexate versus triple therapy in patients with RA.
Methods A systematic review and network meta-analysis (NMA) of randomised controlled trials of TNFi–methotrexate or triple therapy as one of the treatment arms in patients with an inadequate response to or who were naive to methotrexate was conducted. American College of Rheumatology 70% response criteria (ACR70) at 6 months was the prespecified primary endpoint to evaluate depth of response. Data from direct and indirect comparisons between TNFi–methotrexate and triple therapy were pooled and quantitatively analysed using fixed-effects and random-effects Bayesian models.
Results We analysed 33 studies in patients with inadequate response to methotrexate and 19 in patients naive to methotrexate. In inadequate responders, triple therapy was associated with lower odds of achieving ACR70 at 6 months compared with TNFi–methotrexate (OR 0.35, 95% credible interval (CrI) 0.19 to 0.64). Most secondary endpoints tended to favour TNFi–methotrexate in terms of OR direction; however, no clear increased likelihood of achieving these endpoints was observed for either therapy. The odds of infection were lower with triple therapy than with TNFi−methotrexate (OR 0.08, 95% CrI 0.00 to 0.57). There were no differences observed between the two regimens in patients naive to methotrexate.
Conclusions In this NMA, triple therapy was associated with 65% lower odds of achieving ACR70 at 6 months compared with TNFi–methotrexate in patients with inadequate response to methotrexate. Although secondary endpoints numerically favoured TNFi–methotrexate, no clear differences were observed. The odds of infection were greater with TNFi–methotrexate. No differences were observed for patients naive to methotrexate. These results may help inform care of patients who fail methotrexate first-line therapy.
- Rheumatoid Arthritis
- DMARDs (synthetic)
- DMARDs (biologic)
- Methotrexate
- TNF-alpha
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Key messages
What is already known about this subject?
Previous studies have reported that tumour necrosis factor inhibitor (TNFi)–methotrexate and triple therapy (methotrexate/hydroxychloroquine/sulfasalazine) are equivalent in patients with rheumatoid arthritis (RA); however, many of these studies were not adequately powered while also suggesting deeper responses associated with TNFi–methotrexate.
What does this study add?
In this network meta-analysis, American College of Rheumatology 70% response criteria (ACR70) at 6 months (primary endpoint) was more likely with TNFi–methotrexate versus triple therapy in patients with an adequate response to methotrexate. Other endpoints did not favour either therapy, although the calculated ORs favoured TNFi–methotrexate in their directionality.
How might this impact on clinical practice?
The greater depth of response suggested by TNFi–methotrexate compared with triple therapy may inform therapy in patients with RA who failed previous methotrexate therapy.
Introduction
The current treatment paradigm for patients with rheumatoid arthritis (RA) consists of disease-modifying antirheumatic drugs (DMARDs), including conventional synthetic DMARDs (csDMARDs) and biologic DMARDs (bDMARDs). The American College of Rheumatology (ACR) and the European League Against Rheumatism (EULAR) propose methotrexate as the first step in the treatment of patients with active RA.1 ,2 Although ∼30% of patients achieve full clinical remission with methotrexate monotherapy, 70% require a step-up treatment that includes the addition of either csDMARDs or bDMARDs.3 Several studies have suggested that initial combination therapy is superior to initial methotrexate monotherapy, whether this is a combination of csDMARDs or the combination of methotrexate with a tumour necrosis factor inhibitor (TNFi).4–12 In patients with inadequate response to methotrexate, the addition of another agent(s) can lead to improved outcomes. Adding a TNFi was superior to adding placebo to methotrexate monotherapy13; similarly, it has been shown that csDMARD triple therapy (adding hydroxychloroquine and sulfasalazine to methotrexate) is superior to methotrexate monotherapy.14 However, it is uncertain whether methotrexate plus TNFi is superior to a combination of csDMARDs or vice versa. Using a completers analysis, the Treatment of Early Aggressive Rheumatoid Arthritis (TEAR) trial concluded that there was no difference between triple therapy and TNFi (specifically, etanercept) plus methotrexate for the endpoints ACR 20% response criteria (ACR20), ACR50, or Disease Activity Score including 28-joint count (DAS28; the primary endpoint) at weeks 48 and 102 in a population of patients who were mostly methotrexate-naive.5 However, there were differences favouring etanercept–methotrexate in several endpoints—radiographic progression and the percentage of patients achieving ACR70—suggesting that etanercept plus methotrexate was more effective than triple therapy in achieving clinically relevant outcomes over time.5 In the TEAR trial, more patients dropped out than the 10% expected (33% by week 48 and 37% by week 102); it is therefore possible that true differences between the two treatments were missed at weeks 48 and 102 because of inadequate power.5 Two randomised controlled trials (RCTs) compared triple therapy to TNFi–methotrexate as second-line therapy. In the Swefot trial in patients with early RA, TNFi–methotrexate was found initially to be superior to triple therapy in patients for whom methotrexate monotherapy had failed, but by year 2 this difference was no longer significant. This study had lower enrolment than originally planned, and a type 2 error at year 2 could not be excluded.3 ,15 Similar results were reported from the Rheumatoid Arthritis Comparison of Active Therapies (RACAT) trial, which also did not reach its target sample size for the primary endpoint of a 0.3-unit difference in DAS28 at week 48.16
Network meta-analysis (NMA) is a model that allows indirect comparisons of interventions through the use of a network of interventions and comparisons.17 NMA can provide estimates of relative efficacy between all interventions connected through the network of trials, even those that have never been compared directly.17–19 Thus, through combining direct and indirect evidence, NMAs have the potential to allow greater precision of point estimates and more power to determine between-group differences relative to single clinical trials or classical pair-wise meta-analyses.20 The objective of this NMA was to evaluate the clinical efficacy, radiographic outcomes, patient-reported outcomes (PROs) and safety of TNFi–methotrexate combination therapy compared with triple therapy in patients with active RA who were methotrexate-naive or had an inadequate response to methotrexate. As ACR and EULAR guidelines recommend methotrexate as first-line therapy in RA, the results in patients with inadequate response to methotrexate are likely more clinically relevant.
Methods
Design
We conducted a systematic literature review of EMBASE, MEDLINE and the Cochrane library, followed by an NMA. We followed the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines in the development and reporting of this analysis,21 which can be found in the online supplementary appendix.
supplementary data
Search strategy
The search strategy combined indexed and free-text terms for disease and interventions of interest and used the Scottish Intercollegiate Guidelines Network (SIGN) filter for RCTs in EMBASE and MEDLINE. No study filter was used in the Cochrane (Central Register of Controlled Trials (CENTRAL)) Library search. The three databases were searched through Ovid. The list of search terms can be found in the online supplementary material methods. Separate reproducible searches were conducted and were supplemented by a manual bibliography check of identified relevant review articles (including previously published systematic reviews and Cochrane reviews), and conference abstracts search in two professional conferences for 2012, 2013 and 2014. Conference abstracts were searched to complement data unavailable in the corresponding full-text publications. Studies available only as a conference meeting abstract were not included.
Eligibility criteria
Included studies were full-text manuscripts of RCTs conducted in adult patients with RA, stratified by methotrexate experience (inadequate responders vs naive). Patients were treated with either TNFi–methotrexate combination therapy or triple therapy (methotrexate + hydroxychloroquine + sulfasalazine). TNFis included in the analysis were adalimumab, certolizumab pegol, etanercept, golimumab, infliximab and biosimilar infliximab. Studies reported at least one endpoint of clinical efficacy, radiographic progression, PRO or safety at 13 weeks, 26 weeks, 1 year or 2 years of follow-up (full list in online supplementary table S1).
Study identification and data extraction
Abstracts and full-text articles were screened by two reviewers, and data were extracted by one reviewer and validated by a second independent reviewer. Any uncertainties were resolved by a third reviewer.
Endpoints
As both treatment combinations have been shown to be effective in the treatment of RA, the prespecified primary endpoint of this analysis was ACR70 at 6 months in order to compare the depth of response of each of these regimens; other endpoints and time points analysed are listed in table 1. The ACR responses were analysed at 3 months, 6 months, 1 year and 2 years.
Endpoints analysed in the network meta-analysis
Assessment of bias
The quality of each study was assessed using the Cochrane Collaboration's tool for assessing risk of bias for RCTs (see online supplementary table S2).22 We did not assess publication bias; however, all studies that met the eligibility criteria were included in the analysis.
Network meta-analysis
For all studies, the feasibility of an NMA was assessed by the academic authors who examined box plots of clinically important baseline characteristic distributions to explore the level of heterogeneity among treatment groups. Accordingly, the following assumptions were made: the sets of trials do not differ with respect to the distribution of effect modifiers, all doses of methotrexate are equivalent and the various TNFis identified were considered as one type of therapy.
The analysis was conducted using WinBUGS V.1.4.3 (MRC Biostatistics, Cambridge Institute of Public Health, Cambridge, UK). Vague (‘flat’) distributions were used such that any parameter value was equally likely. This approach assigns more weight in assuming the therapies are equivalent compared with applying informed prior or traditional frequentist approaches. Fixed-effects and random-effects models were run for each network of evidence and fitted with preferred model fit determined by the deviance information criterion (DIC). A model with a lower DIC score was considered a better fit. Both models were run for 3 months (13 weeks), 6 months (26 weeks), 1 year and 2 years. To evaluate simulation convergence, history, trace plots and Brooks-Gelman-Rubin statistics diagnostics were examined. Three chains were run each with 40 000 iterations and the traces were visually inspected.
For dichotomous endpoints, a logit model was used to estimate the odds of attaining an endpoint. ORs and 95% credible intervals (CrIs) of triple therapy versus TNFi–methotrexate were calculated, with ORs <1 indicating a better performance for TNFi–methotrexate for clinical efficacy and radiographic outcomes, and ORs >1 indicating a better performance for TNFi–methotrexate for safety outcomes. For continuous endpoints, a weighted mean difference between mean changes from baseline for treatments at follow-up was estimated using end-of-trial mean scores or change in mean score from baseline. Values >0 for difference in mean change from baseline of triple therapy versus TNFi–methotrexate indicated better performance for TNFi–methotrexate.
Handling of missing data was conducted according to the Cochrane Handbook for Systematic Reviews.23 When an endpoint of interest was not reported adequately or not in a format we could incorporate, attempts to inform missing data were undertaken, including contacting the authors of the study and cross-checking against previously published NMAs reporting the data point of interest. We used the best available data from the specific time points indicated (ie, the Ns were not inflated to the number of randomised patients). We used the intent-to-treat method (with various imputation methods) as much as possible; for studies using completer-only or modified intent-to-treat methods, those data were used for the analysis. For studies missing SDs, an average of the SDs of all other studies in the same network was used for a particular study. Randomised arms with more than 20% crossover at any time point were not analysed beyond the time point where crossover occurred because treatment effects could not be attributed to the initial therapy once these crossovers took place.
Sensitivity analyses using non-responder imputation and completers data were compared with the main results of the study to determine whether the method used to account for missing data affected the results. Comparison between the results from the NMA and a classical pair-wise direct comparison were used to determine consistency.
Results
Studies identified
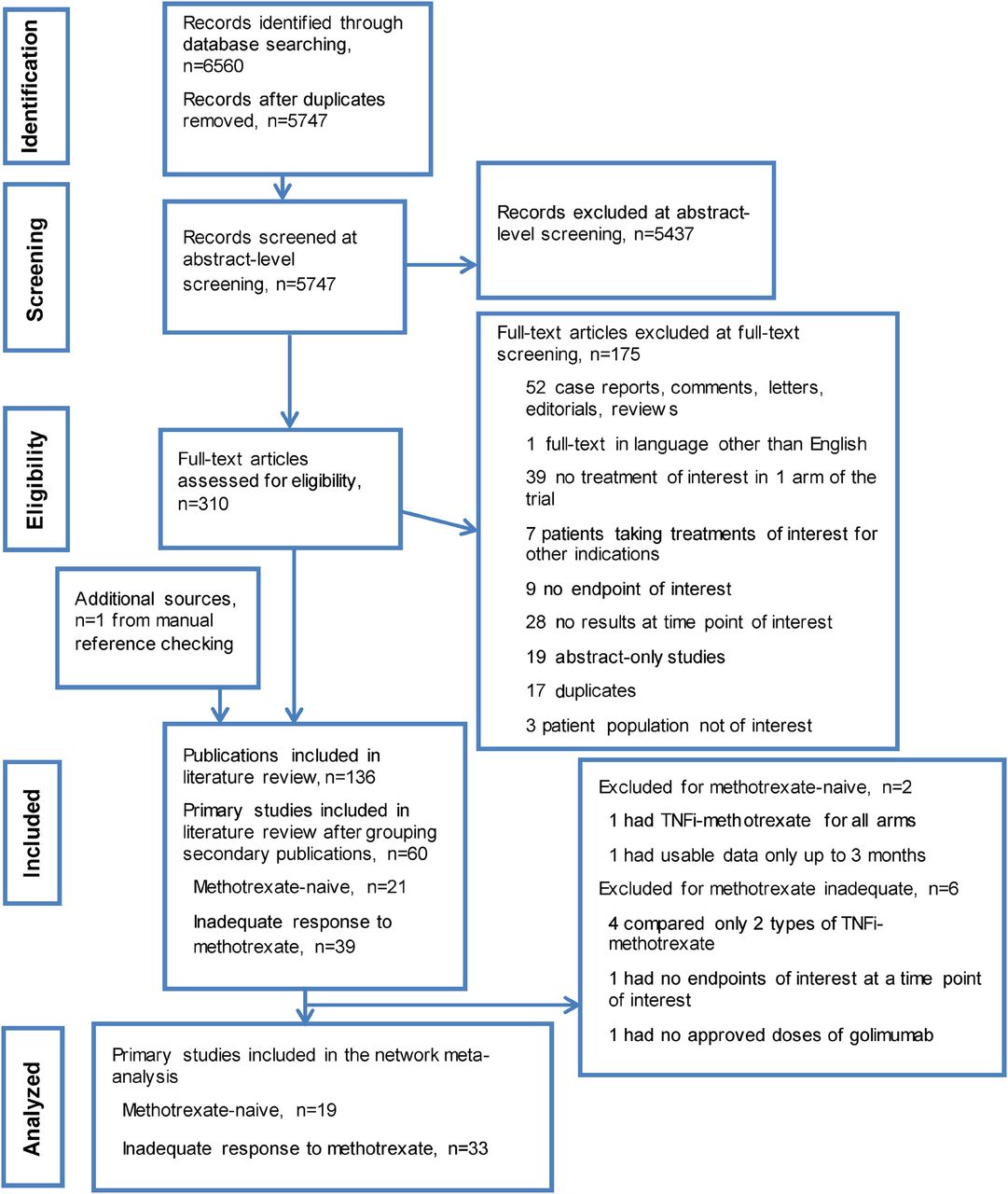
The search yielded 6560 abstracts and citations from EMBASE, MEDLINE, and the Cochrane (CENTRAL) library. After screening, 60 full-text primary studies were identified for possible inclusion, which corresponded to 136 records. Of the 60 studies, 393 ,24–61 were in patients with inadequate response to methotrexate, and 214 ,5 ,7 ,11 ,14 ,62–77 were in methotrexate-naive patients. A PRISMA diagram documenting the search, screening and trial selection process, and reasons for exclusion is shown in figure 1.21
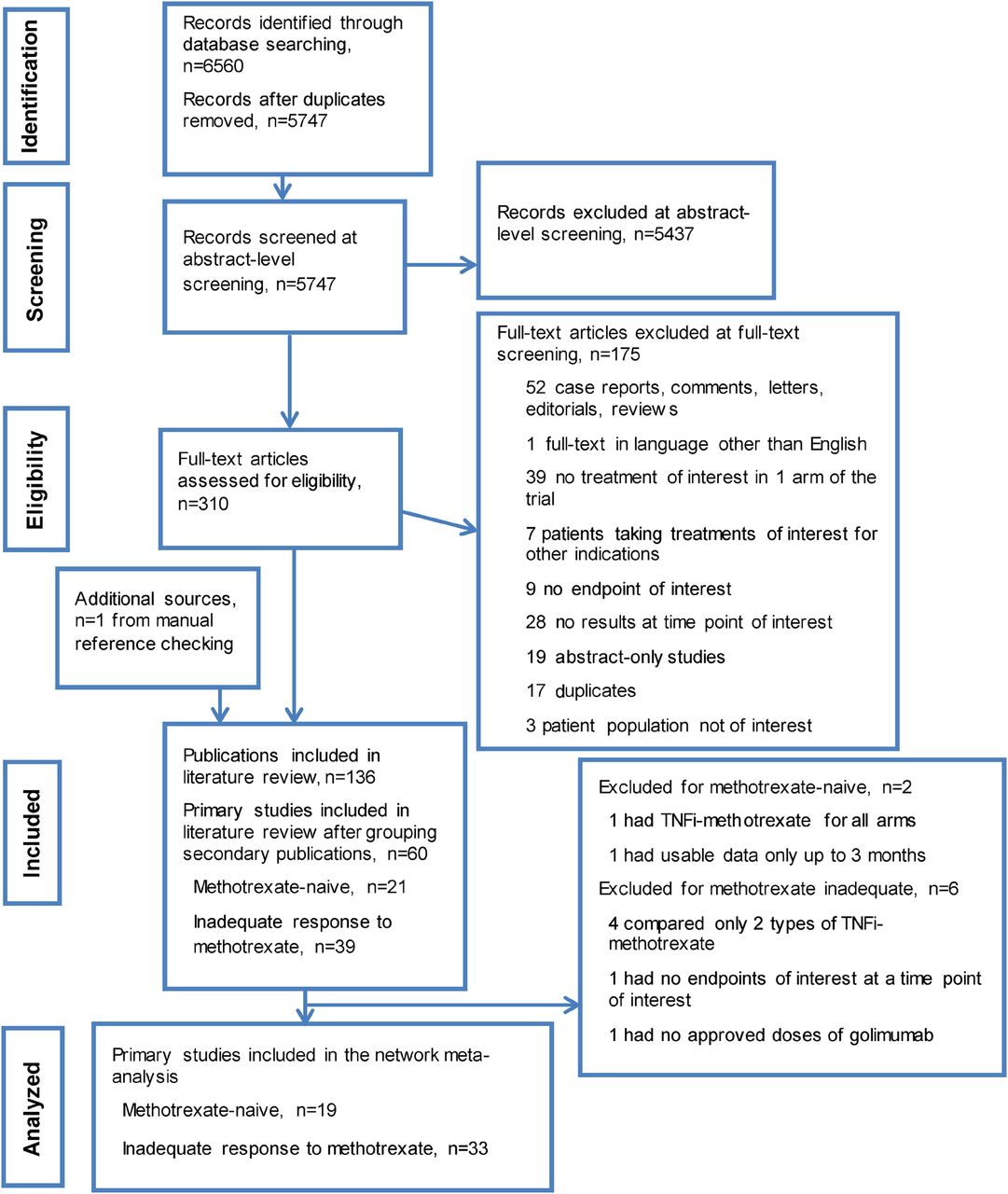
PRISMA diagram documenting the search and screening process. Articles were identified by searching MEDLINE, EMBASE and Cochrane CENTRAL databases from 1 January 1990 to 9 September 2014; manual bibliography checks of previously published systematic reviews and Cochrane reviews supplemented these searches. Conference abstracts from the American College of Rheumatology Annual Meetings and the Annual European Congresses of Rheumatology in 2012, 2013 and 2014 were used to supplement data not included in the corresponding full-text publications. TNFi, tumour necrosis factor inhibitor.
Characteristics of studies
Patients with inadequate response to methotrexate
Inadequate response to methotrexate was defined as the presence of active RA despite current use of methotrexate; however, we observed differences in definitions across the studies. The descriptions of patients included the following: patients with active RA on methotrexate before the study, patients on stable doses of methotrexate for at least 4 weeks before study enrolment, patients who had active RA despite methotrexate treatment and patients with inadequate response to methotrexate treatment. Study and baseline characteristics of the studies are listed in online supplementary table S3. The baseline mean age was 37–61 years. Female enrolment ranged from 43% to 100%; the proportion of patients who were rheumatoid factor–positive (RF+) was 61–100%; and mean disease duration was 1.3–14.3 years. Baseline DAS28–erythrocyte sedimentation rate (ESR) ranged from 4.6 to 6.9 and DAS28–C-reactive protein (CRP) from 4.3 to 6.0. Our feasibility assessments of box plots of baseline characteristics across studies (see online supplementary figures S1–S14) determined that there were no clinically meaningful differences in treatment cohorts across the studies.
Methotrexate-naive patients
The definition of patients who were naive to methotrexate differed across the trials. In most cases, the definition was no prior exposure to methotrexate; however, a few studies allowed limited exposure to methotrexate. Also included was a study enrolling patients who had not received methotrexate within 6 months before randomisation78 as well as a single study that allowed ≤40 mg of total methotrexate in <20% of patients before the study period.5 Another study allowed patients with DMARD treatment, but only 10% of patients had received methotrexate before; therefore, it was included in this group of methotrexate-naive studies.14 The baseline mean age was 47–54 years; female enrolment was 53–85%; the RF+ proportion was 49–100% (see online supplementary table S3). Mean disease duration was 0.1–10 years; baseline DAS28-ESR was 5.5–6.9 and DAS28-CRP ranged from 5.0 to 6.2. Baseline radiographic score and modified total Sharp score (mTSS) showed a wide distribution, with the majority reporting mean scores of 10–20, and others up to 44.77 The feasibility assessment of box plots of distributions of baseline characteristics (see online supplementary figures S15–S26) determined that there were no clinically meaningful differences in baseline characteristics across the studies.
Network meta-analysis results
Patients with inadequate response to methotrexate
The 39 trials from the systematic review were further assessed for the availability of appropriate treatment arms (approved doses), and if none were present, the trial was excluded from the analyses; 23 (59%) had unclear risk of bias, 15 (38%) had low risk of bias and 1 (3%) had a high risk of bias.27 Online supplementary table S4 describes special considerations for studies or treatment arms from certain studies that were not included in the NMA. Four trials were not used in the analyses because they compared two types of TNFi–methotrexate combinations.28 ,56 ,58 ,60 One trial was excluded because none of the endpoints of interest at the time points of interest were reported.59 Another did not evaluate an approved dose for golimumab and was excluded.38 Certain treatment arms from 10 trials evaluated non-approved doses of the TNFis, and hence could not be included in the analyses.30–32 ,34 ,45 ,47 ,48 ,53 ,57 Finally, in five trials, data were used until randomisation was truly maintained, up to 6 months in four trials33 ,43 ,48 ,52 and up to 1 year in another trial,49 before allowance of additional RA treatments. Thus, 33 primary studies3 ,15 ,24–27 ,29–37 ,39–55 ,57 ,61 ,79–111 and their follow-up analyses (67 records total) in patients with inadequate response to methotrexate were included in the NMA. The full list of studies included in the NMA and the endpoints available for analysis in each study is shown in online supplementary table S5.
Efficacy
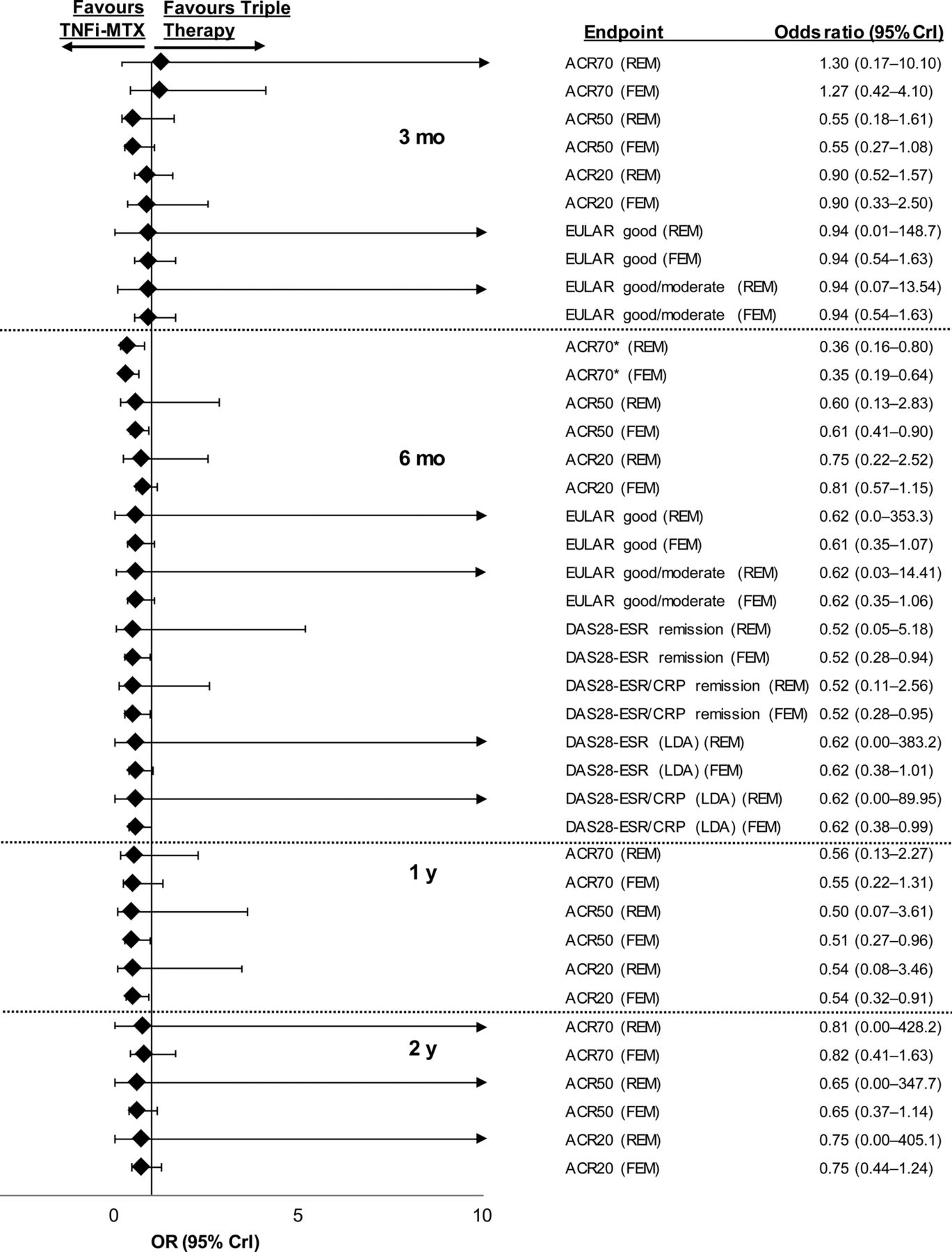
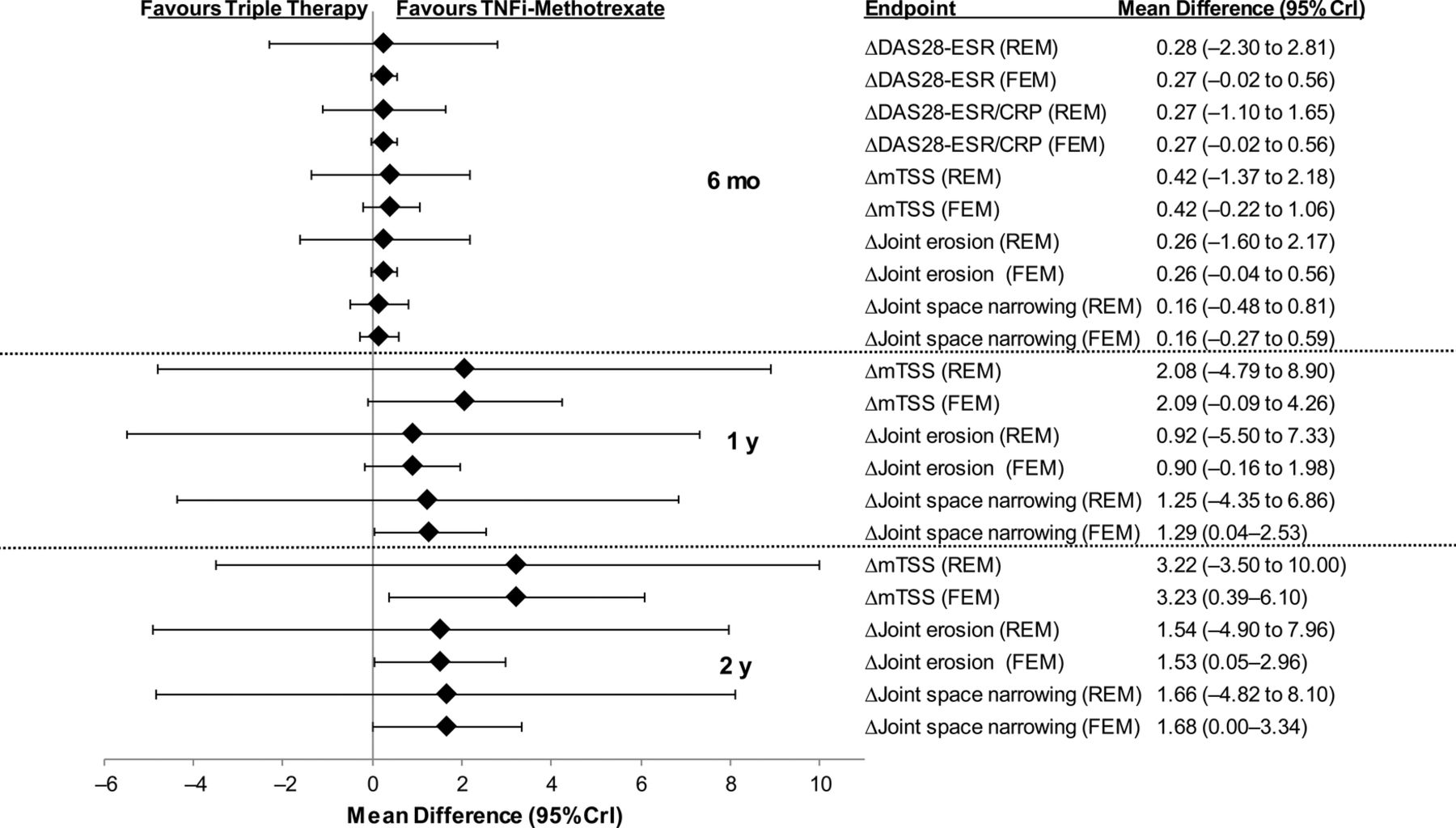
The number of studies used for each analysis along with DIC values for fixed-effects and random-effects models are shown in online supplementary table S6; the network of evidence for the primary endpoint is shown in online supplementary figure S27. Patients with inadequate response to methotrexate were less likely to achieve ACR70 with triple therapy than with TNFi–methotrexate at 6 months in the fixed-effects (OR 0.35, 95% CrI 0.19 to 0.64) and random-effects (OR 0.36, 95% CrI 0.16 to 0.80) models (figure 2; full results in online supplementary table S7). Although the values of the OR for the other efficacy endpoints of ACR20/50, DAS28-ESR remission or low disease activity, DAS28-ESR/CRP remission or low disease activity favoured TNFi–methotrexate, the CrIs extended past 1 and thus a true difference between the two regimens could not be confirmed for these endpoints. Similarly, mean differences for DAS28-ESR and DAS28-ESR/CRP at 6 months did not favour either treatment (figure 3).
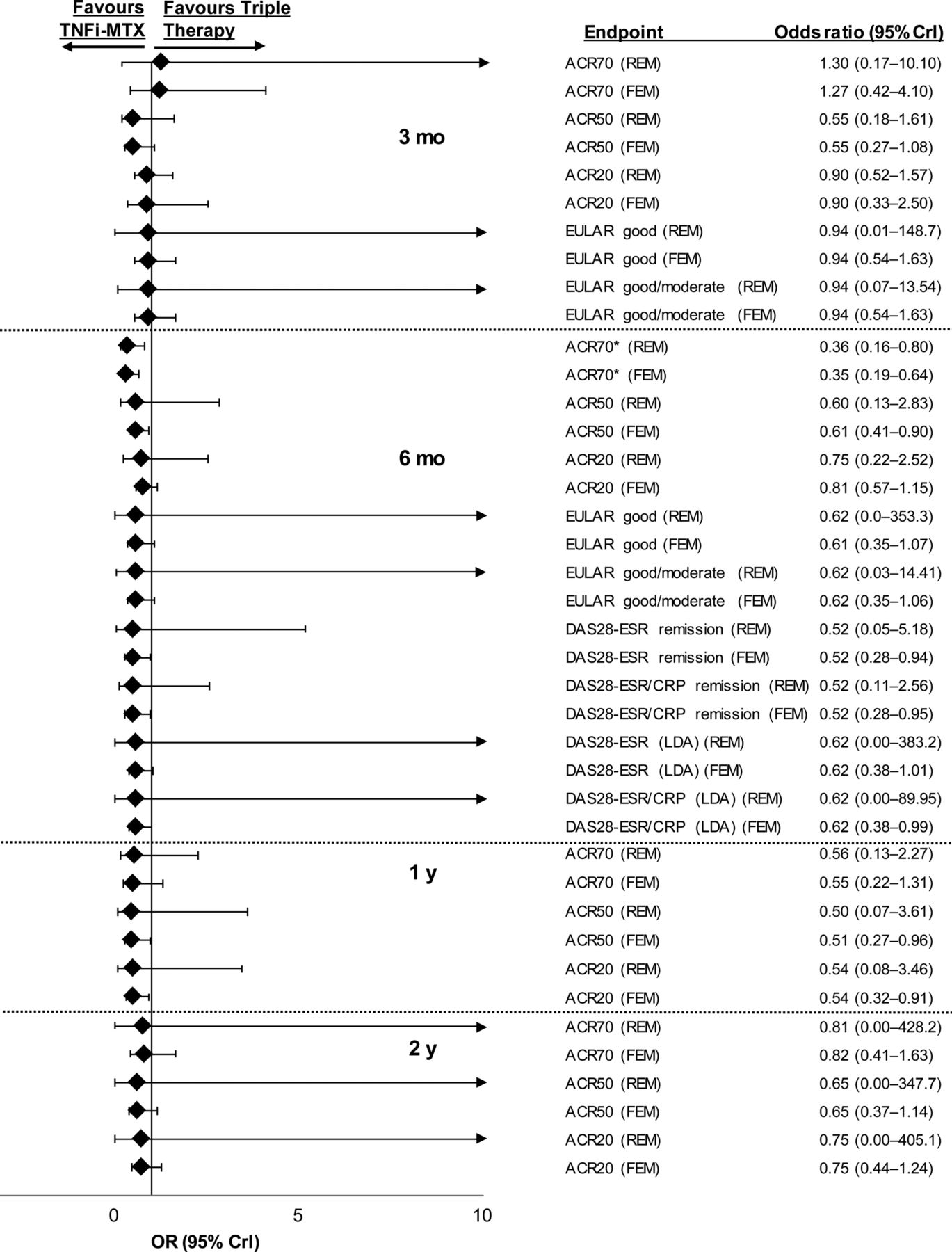
Relative treatment effects concerning efficacy endpoints in patients with inadequate response to methotrexate for triple therapy versus TNFi–methotrexate at 3 months, 6 months, 1 year and 2 years. ACR70/50/20, American College of Rheumatology 70%/50%/20% response criteria; CrI, credible interval; CRP, C-reactive protein; DAS28, Disease Activity Score including 28-joint count; ESR, erythrocyte sedimentation rate; EULAR, European League Against Rheumatism; FEM, fixed-effects model; LDA, low disease activity; MTX, methotrexate; REM, random-effects model; TNFi, tumour necrosis factor inhibitor. *ACR70 at 6 months was a prespecified primary endpoint.

Mean differences in efficacy and radiographic outcomes in triple therapy versus TNFi–methotrexate in patients with inadequate response to methotrexate. CrI, credible interval; CRP, C-reactive protein; DAS28, Disease Activity Score including 28-joint count; ESR, erythrocyte sedimentation rate; FEM, fixed-effects model; mTSS, modified total Sharp score; REM, random-effects model; TNFi, tumour necrosis factor inhibitor.
Mean differences for radiographic endpoints at 6 months, 1 year and 2 years are shown in figure 3. Overall, the mean differences between TNFi–methotrexate and triple therapy did not favour either therapy for the radiographic endpoints of mTSS, joint erosion or joint space narrowing. However, differences were observed in the fixed-effects model, but not the random-effects model for mTSS, joint erosion and joint space narrowing that favoured TNFi–methotrexate over triple therapy at 2 years.
Safety
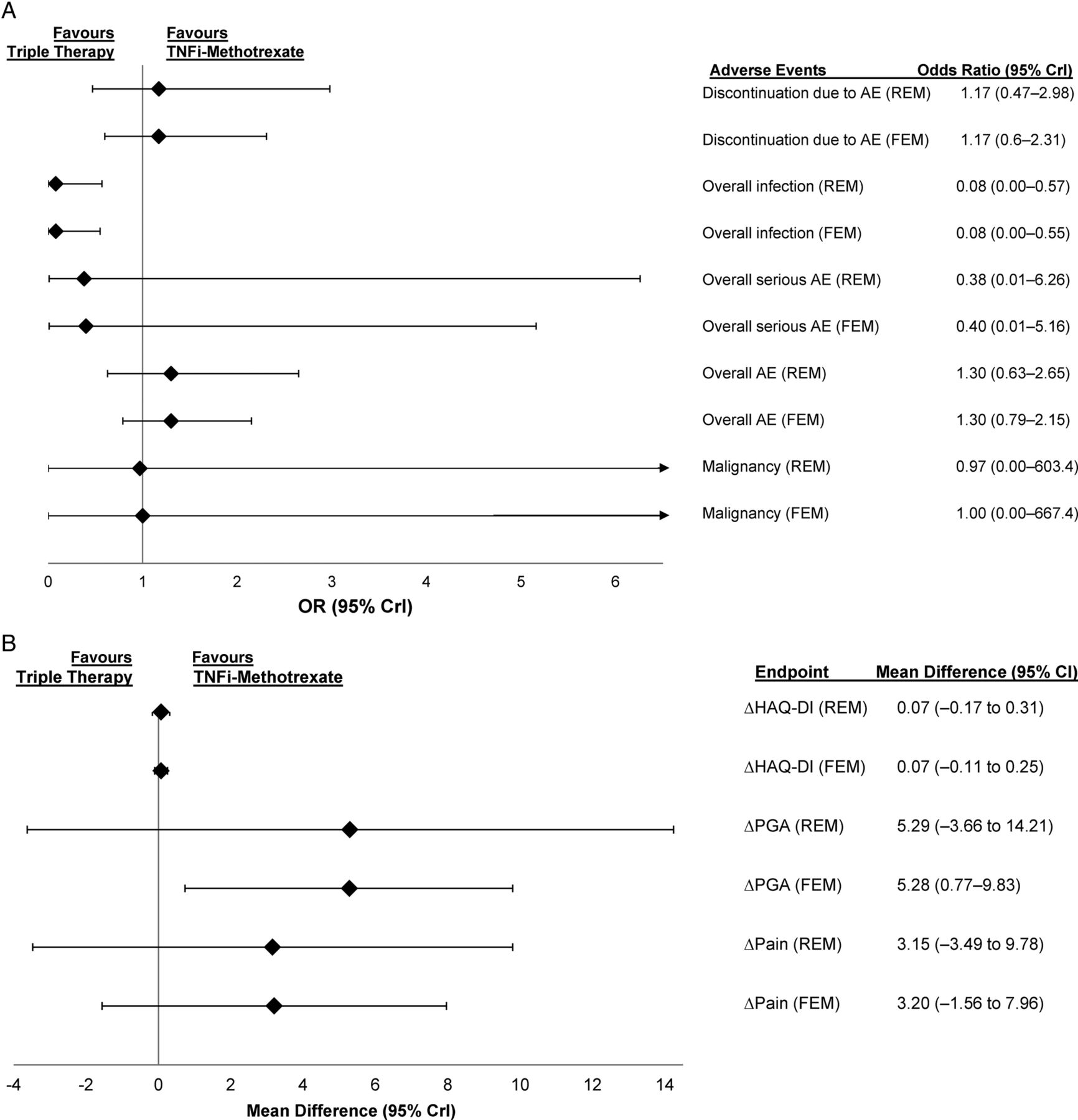
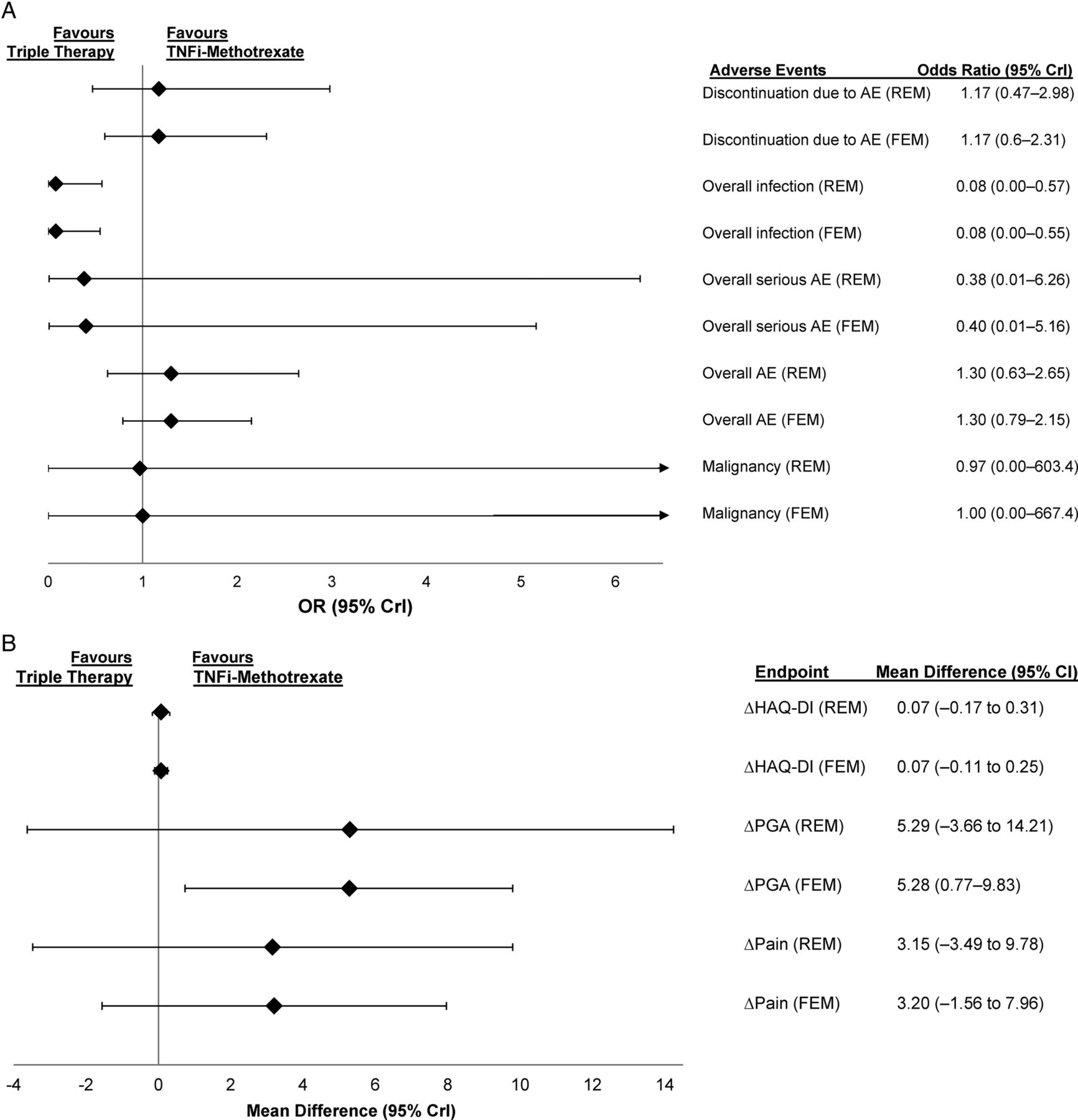
Triple therapy showed lower odds of infection in the random-effects (OR 0.08, 95% CrI 0.00 to 0.57) and fixed-effects (OR 0.08, 95% CrI 0.00 to 0.55) models. For the other safety endpoints of overall adverse events (AEs), discontinuation due to AEs, serious AEs and malignancy, the likelihood of achieving these endpoints were similar between triple therapy and TNFi–methotrexate (figure 4A; full results in online supplementary table S8).
{kind=link}
{kind=link}
{kind=link}
{kind=link}
(A) ORs comparing safety outcomes and (B) mean differences in patient-reported outcome endpoints in patients treated with triple therapy versus TNFi–methotrexate in patients who had inadequate response to methotrexate at 6 months. AE, adverse event; CrI, credible interval; FEM, fixed-effects model; HAQ-DI, Health Assessment Questionnaire-Disability Index; PGA, patient general assessment; REM, random-effects model; TNFi, tumour necrosis factor inhibitor.
Patient-reported outcomes
TNFi–methotrexate was favoured for mean difference in patient's general assessment in the fixed-effects, but not random-effects model at 6 months (figure 4B); full results in online supplementary table S7). The two treatments were comparable for Health Assessment Questionnaire-Disease Index and pain scores at 6 months. Comparisons were not available for the other time points.
Methotrexate-naive patients
Further exploration of study design and treatment characteristics of the 21 studies (see online supplementary table S3) was conducted to assess if all available treatment arms or time points could be included in the analyses. Fourteen studies (67%) had low risk of bias; seven studies (33%) had an unclear risk of bias. Among the studies available, further exploration of the study design and treatment characteristics was conducted to assess if all available treatment arms or time points could be included in the analyses (see online supplementary table S8). A few considerations were given to certain studies to ensure that only approved doses were included or that study populations at all time points considered for the analysis represented the true randomised population; these are shown in the online supplementary table S9. In three trials,37 ,92 ,104 participants were allowed to switch treatments or add additional DMARDs. These studies were not analysed beyond the time point when >20% of participants no longer maintained randomisation. One trial (CONCERTO) evaluated TNFi–methotrexate in all treatment arms and was not included in the analyses.64 ,112–114 Another study (BeST) was excluded because patients were allowed to receive additional DMARDs in the methotrexate and TNFi–methotrexate arms after 3 months.11 ,115 ,116 One trial evaluated TNFi–methotrexate in all treatment arms resulting in it not being feasible to be included in the analyses.112 Thus, 19 primary studies and their associated follow-up analyses were included in the NMA.4 ,5 ,7 ,14 ,16 ,62 ,63 ,65–77 ,117–141
Participants in the TEAR5 trial were assessed for DAS28-ESR at 6 months. Those randomised to the two step-up arms were allowed to add on assigned therapies (etanercept or hydroxychloroquine plus sulfasalazine) if DAS28-ESR was ≥3.2 with methotrexate monotherapy. Data from the first 6 months from the two step-up arms were collapsed to form a methotrexate monotherapy arm in the NMA because no additional treatments were introduced during that time. After 6 months, TEAR was analysed as the original four-arm trial. The COmbination of Methotrexate and ETanercept (COMET) trial randomised patients into two arms from baseline to 1 year and to four arms after 1 year until study conclusion at 2 years. Both randomisations occurred at baseline; thus COMET was analysed as a two-arm trial until 1 year.4 After the 1-year time point, COMET was analysed as a four-arm trial, with arms randomised to switch treatment regimen labelled as ‘switch 1’ (combination etanercept plus methotrexate therapy for the first 52 weeks; after 52 weeks patients continued methotrexate, and etanercept was switched to placebo) and ‘switch 2’ (methotrexate monotherapy plus placebo for the first 52 weeks; after 52 weeks patients continued to receive methotrexate, and placebo was switched to etanercept). The full list of studies of methotrexate-naive patients included in the NMA and the endpoints available for analysis are shown in online supplementary table S10.
Efficacy
The number of studies used in each analysis along with DIC values for fixed-effects and random-effects models are shown in online supplementary table S11; the network of evidence for the analysis of the primary endpoint is shown in online supplementary figure S28. Full results of the NMA are shown in online supplementary table S12 and figure S29; OR values <1 indicate a better performance for TNFi–methotrexate over triple therapy. For the primary endpoint, ACR70 at 6 months in methotrexate-naive patients, the OR in the fixed-effects model was 0.76 (95% CrI 0.36 to 1.50); for the random-effects model, the OR was 0.77 (95% CrI 0.31 to 1.76). Achievement of ACR70 at 2 years was more likely in patients treated with TNFi–methotrexate compared with triple therapy in the fixed-effects model (OR, 0.44, 95% CrI 0.22 to 0.82) but not the random-effects model (OR 0.43, 95% CrI 0.14 to 1.28). Similarly, the likelihood of no radiographic progression was more likely in patients treated with TNFi–methotrexate compared with triple therapy in the fixed-effects model (OR 0.48, 95% CrI 0.25 to 0.9) but not the random-effects model (OR 0.47, 95% CrI 0.15 to 1.41). No differences were indicated based on ORs for ACR50 or ACR20 at 6 months or 2 years, or in DAS28-ESR remission at 2 years. Mean differences between TNFi–methotrexate and triple therapy did not favour either therapy in either model for the efficacy endpoints for DAS28-ESR/CRP or DAS28-ESR at 3 months, 6 months, 1 year, or 2 years.
Mean differences between TNFi–methotrexate and triple therapy for the radiographic endpoints of change in joint space narrowing, change in joint erosion or change in mTSS at 2 years did not favour either therapy in either model. (see online supplementary figure S30). No comparisons were available for these endpoints at other time points.
Safety
The ORs showed no difference in the odds of discontinuations due to AEs, overall AEs, serious infections and aspartate aminotransferase elevation between TNFi–methotrexate and triple therapy in patients naive to methotrexate (see online supplementary table S13 and figure S31A).
Patient-reported outcomes
Comparisons were available for the Health Assessment Questionnaire-Disability Index and patient general assessment (PGA) at 2 years; no difference in likelihood of achieving these outcomes was observed between TNFi–methotrexate and triple therapy (see online supplementary table S12 and figure S31B).
Sensitivity analysis
The sensitivity analysis of DAS28-ESR remission at 2 years using non-responders data from the COMET trial gave similar results for the comparison of triple therapy versus TNFi–methotrexate. The TEAR trial reported non-responder imputation and completer data for DAS28-ESR change from baseline at 3 months, 6 months, 1 year and 2 years. The results of the sensitivity analysis were consistent with the direction and magnitude of our main results, with a few exceptions, including mean change in DAS28-ESR at 3 months and 2 years when non-responders imputation data were used. At 3 months, the fixed-effects model result using TEAR last observation carried forward data was 0.21 (95% CrI −0.03 to 0.46), whereas in the sensitivity analysis using non-responders imputation data, the resulting mean difference from the fixed-effects model between TNFi–methotrexate and triple therapy was 0.30 (95% CrI 0.06 to 0.54). Although at 2 years, the observed result was similar to the results obtained from the last observation carried forward analysis, there was a change in the directionality of the relative treatment effect, with a trend of TNFi–methotrexate performing better in the sensitivity analysis using non-responders imputation data.
Discussion
This is the first study to provide a systematic, qualitative and quantitative review of the published literature across critical efficacy, radiographic, safety and PRO endpoints in patients with RA receiving TNFi–methotrexate or triple therapy. This NMA showed that in methotrexate-naive patients there was no difference in the likelihood of achieving clinical efficacy endpoints between triple therapy and TNFi–methotrexate. Although most endpoints favoured TNFi–methotrexate in terms of OR directionality, such a result is not likely to be clinically relevant. In patients with inadequate response to methotrexate, the NMA shows better outcomes for patients treated with TNFi–methotrexate versus triple therapy with respect to the primary endpoint of ACR70 at 6 months; other endpoints were favourable in terms of directionality of the OR, but the limits of the CrIs indicated no clear difference for either therapy. In patients with inadequate response to methotrexate, triple therapy had 65% lower odds than TNFi–methotrexate in achieving ACR70 at 6 months. Trends showing benefits of TNFi–methotrexate were observed across the majority of endpoints. Taken together, these results indicate that the two treatment strategies are comparable, although TNFi–methotrexate may be associated with deeper responses.
Our results suggest that the addition of a TNFi to methotrexate after inadequate response to methotrexate could result in better outcomes compared with the addition of sulfasalazine and hydroxychloroquine, chiefly with ACR70 at 6 months. Our finding is therefore applicable to most patients who do not achieve a good response with methotrexate monotherapy.3 It should be noted that current EULAR guidelines recommend that patients without unfavourable prognosis fail at least two csDMARDs before proceeding to biologic therapy2; unfortunately, this could not be examined in this analysis. Nevertheless, our results support the current ACR guidelines and the current recommendation of adding TNFi to methotrexate in patients with an unfavourable prognosis per EULAR.1 ,2 Notably, although the OR directionality favoured TNFi–methotrexate over triple therapy in this population at 1 and 2 years, CrIs extended past 1, indicating no increased likelihood of response for either therapy; however, comparison of these time points were limited by the number of studies and data points available for analysis. Therefore, the durability of the difference between TNFi–methotrexate and triple therapy in patients with inadequate response to methotrexate is uncertain.
Our results suggest that patients given combination therapy as first-line treatment benefit comparably from triple therapy and TNFi–methotrexate. Results of recent studies suggest that in patients naive to methotrexate, outcomes at 2 years are similar among patients treated with methotrexate monotherapy and ‘step-up’ to combination therapy and those treated early with TNFi–methotrexate combination therapy or triple therapy.5 ,16 Starting treatment with methotrexate monotherapy is recommended by EULAR and the ACR1 ,2 and is the approach most often used in clinical practice. Importantly, initial treatment with a biologic agent would not be reimbursed in most countries and is not necessary in all patients; therefore, although of interest, these findings would not be applicable to most patients with early RA naive to methotrexate. It is noteworthy that the present analysis was designed and conducted before the most recent recommendations, thus it was deemed important to the investigators to include these data. It should also be noted that the use of corticosteroids in some patients is a potential confounder to these results but due to randomisation, it is likely that steroids were used equally in all treatment groups within any trial.
In patients with inadequate response to methotrexate, the majority of safety outcomes were similar between the two treatment regimens; however, an increased risk of infection was noted for TNFi–methotrexate. Safety outcomes were also similar between the treatment regimens in patients naive to methotrexate. Improvements in PGA and pain scores were greater for patients treated with TNFi–methotrexate compared with triple therapy in those with inadequate response to methotrexate (random-effects model only); negligible differences between the two regimens were observed in PGA scores in the methotrexate-naive population.
In this NMA, we present the results from fixed-effects and random-effects models. Typically, random-effects models are preferred because it is generally accepted that baseline characteristics and potential effect modifiers do not have equal distribution across trials, unlike fixed-effects models, which assume a common treatment effect size across trials comparing the same interventions.142 In our limited sample of studies, we found the baseline clinical values across the trials considered for the NMA to be clinically uniform. Beyond examining box plots to assess the distribution of baseline characteristics, an informal graphical check of the treatment effect modifiers of clinically important baseline values was performed. As available data were sparse, we could not come to a conclusive finding of any treatment effect modifier among the available baseline values. The fixed-effects model results are most applicable to our data set because we could not ascertain any systematic differences between the patient populations included, and we compared only two or fewer studies per intervention in each network.
Advantages of NMAs over traditional meta-analyses include the ability to compare directly and indirectly.17 This NMA was designed using best practice guidelines to identify all RCTs available; all available literature was considered. Stratifying the base analysis population by prior exposure to methotrexate alleviates concerns over the prior treatment and response differences across the studies. The combinations of TNFi–methotrexate were prespecified and included only approved doses of TNFi for the treatment of RA; triple therapy was specifically a combination of methotrexate, hydroxychloroquine and sulfasalazine. All available efficacy, radiographic, PRO and safety endpoints were assessed to provide an overall understanding of the relative treatment estimates for the comparison of triple therapy to TNFi–methotrexate.
Limitations of this analysis were that few studies with a common comparator (methotrexate monotherapy) were available; in particular, there was a lack of methotrexate monotherapy arms in studies that evaluated triple therapy. Therefore, results were driven by the few studies that had head-to-head comparison between triple therapy and TNFi–methotrexate and should be interpreted cautiously. We also considered all doses of methotrexate as equal between the treatment arms in the network, which is a potential confounder to our results. Also, certain studies were not included because their endpoints differed from other studies or included patients who received other therapies or used definitions of methotrexate-naive that included patients who had received methotrexate. Furthermore, any negative results not available to the searched databases because of publication bias are excluded from our analysis. Finally, not all endpoints used for inclusion in the study could be analysed in the NMA; for safety, the only specific AEs that could be analysed in the NMA were infection, malignancy and aspartate aminotransferase elevation.
In conclusion, in patients who were naive to methotrexate treatment, neither triple therapy nor TNFi–methotrexate showed an increased likelihood of achieving ACR70 at 6 months; at the group level, these two treatment strategies appear comparable. The majority of secondary endpoints favoured TNFi–methotrexate in terms of OR directionality, although the limits of the CrIs indicated no clear likelihood of better response with either therapy. TNFi–methotrexate showed increased odds of achieving ACR70 at 6 months over triple therapy, suggesting a possible deeper response with TNFi–methotrexate over triple therapy. These conclusions are in line with the recent ACR guidelines and the EULAR recommendations for the treatment of RA in patients with poor prognostic markers. In patients without poor prognostic markers, it would be reasonable to use either therapy combination.
Acknowledgments
Medical writing support was provided by Dikran Toroser, PhD, CMPP (Amgen) and Miranda Tradewell, PhD, and Rick Davis, MS (Complete Healthcare Communications, LLC, funded by Amgen). Manpreet Sidhu, PhD, and Neil Hawkins, PhD, reviewed and provided input on the study protocol, input on analyses approaches and assumptions, and review of analyses results and interpretation.
References
Footnotes
Contributors All authors meet the criteria for authorship, participated in the writing and/or critical revision of the manuscript, and have seen and approved the submitted version. JC, DC, RF, KN, JP, DHT, VT, RvV and GW contributed to the conception, design or planning of the study. KN, VT, SU and RvV were involved in data acquisition. JC, DC, RF, KN, JP, VT, SU and RvV analysed the data. JC, DC, RF and JP drafted the manuscript. All authors interpreted the results and critically revised the manuscript.
Funding Amgen Inc.
Competing interests RF has received grants and non-financial support from Amgen. VT, SU and KN are employees of ICON plc, which received grants and consulting fees from Amgen. RvV has received grants from Abbvie, Amgen, Bristol-Myers Squibb, GlaxoSmithKline, Pfizer, Roche and Union Chimique Belge, and personal fees from Abbvie, Amgen, Biotest, Bristol-Myers Squibb, Celgene, Crescendo, GlaxoSmithKline, Janssen, Eli Lilly, Merck, Novartis, Pfizer, Roche, Union Chimique Belge and Vertex. DHT, JC and DC are employees and stockholders of Amgen. JP received grants from Amgen and received consulting fees from Abbvie, Amgen, Bristol-Myers Squibb, Eli Lilly, Merck, Novartis, Pfizer, Roche and Union Chimique Belge. GW had nothing to disclose.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement No additional data are available.