Article Text

Abstract
Objective To update the evidence pertaining to the diagnosis, prognosis and classification of patients with early arthritis (EA), and to inform the 2016 European League Against Rheumatism (EULAR) recommendations for the management of patients with EA.
Methods MEDLINE, EMBASE and Cochrane databases were searched up to October 2015. The first part of the systematic literature review (SLR) involved a search for studies investigating the recognition and referral of EA. The second part involved a search for studies to identify the place of laboratory and imaging tests in establishing a diagnosis and a prognosis in patients with EA.
Results Regarding the issue of referral of patients with EA (1643 hits), 4 studies were included. These studies were in support of early referral for patients with EA. Regarding the issue of diagnosis and prognosis of patients with EA (11 435 hits), 88 studies were included, evaluating mainly the value of rheumatoid factor (RF) and anticitrullinated-peptide antibodies (ACPAs). Sensitivity of these antibodies for a RA diagnosis in patients with EA was moderate (40–80%). Specificity was higher, notably for ACPAs (frequently >80%). ACPAs also showed better prognostic performance than RF (negative predictive values around 80%). We confirmed that structural damage on baseline X-rays is predictive of further radiographic progression in patients with EA. Regarding other imaging modalities, data are sparse.
Conclusions This SLR highlights the importance of early referral for patients with EA and confirms that RF and mainly ACPAs as well as a search for structural X-rays changes may help in the diagnosis and prognosis of patients with EA.
- Early Rheumatoid Arthritis
- Ant-CCP
- Rheumatoid Factor
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Key messages
What is already known about this subject?
Patients with inflammatory arthritis should be referred to rheumatologists as early as possible.
In patients with early arthritis (EA), the presence of rheumatoid factor (RF) and/or anticitrullinated-peptide antibodies (ACPAs) as well as radiographic erosions, independently contribute to predicting long-term radiographic progression.
What does this study add?
Patients with EA referred to a rheumatologist within 3 months show better outcomes than those with later referral.
RF and ACPAs are useful tests in patients with EA but ACPAs have more diagnostic and prognostic value than RF.
Structural damage on baseline X-rays of hands and feet is predictive of further radiographic progression in patients with EA.
How might this impact on clinical practice?
This systematic literature review (SLR) highlights the importance of early referral of patients with EA to the rheumatologist and confirms that the RF and mainly ACPAs serological status, as well as the radiographic status, are of value in the diagnosis and prognosis of patients with EA.
Data on the diagnostic and prognostic value of other imaging modalities (ultrasound, MRI) are sparse and do not allow a proper judgement to date.
Introduction
When a patient presents with early arthritis (EA), a quick and definite diagnosis is needed to initiate early treatment. The early start of disease-modifying antirheumatic drugs (DMARDs) may improve clinical and radiographic outcomes.1–5 A diagnosis of EA may involve several steps, from the detection and confirmation of arthritis to the final diagnosis by a rheumatologist. Predicting a prognosis in a patient with EA is also important in order to offer the best treatment for that patient.
In 2007, the European League Against Rheumatism (EULAR) recommendations for EA management have been published.6 These recommendations on EA covered the entire spectrum of EA management, including recognition of arthritis, referral, diagnosis, prognosis, classification, information, education, non-pharmacological interventions and monitoring of the disease process.6 Between January 2005 (when the systematic literature review (SLR) informing the 2007 recommendations had been performed) and 2015, many publications in the field of EA have been released, notably with crucial data from prospective cohorts of patients with EA.7 ,8 Therefore, the 2007 EULAR recommendations on EA management had to be updated.
The first step in the update was to perform a SLR of the literature available from 2005 onward. Here we report on this SLR that involves the themes referral, diagnosis, prognosis and classification of patients presenting with EA. A separate SLR on the treatment of patients with EA is reported in a separate article.
Methods
Research questions
The first step included the formulation of five key research questions to be addressed in the SLR. The research questions were proposed by the convenor (BC) and the methodologist (RL), then amended and approved by the expert committee. These research questions encompassed the recognition (1) and referral (2) of patients with EA, the diagnosis of EA (3), its prognosis (4) and its classification (5) (see online supplementary material S1). The research questions were framed, defined and structured according to EULAR standardised operating procedures9 using the ‘Patients, Intervention, Comparator or Control, Outcome, Type of study (PICOT) format’ (see online supplementary material S2).10
supplementary material
Literature search
Literature available until October 2015 was reviewed by two supervised research fellows (CD and CH). This SLR was considered a follow-up of several previous EULAR SLRs: the 2005 SLR performed for the EULAR recommendations for management of EA6 as well as two other SLRs performed by other EULAR task forces.11 ,12
The first part of the SLR aimed to assess the recognition of arthritis and referral to a medical specialist. It was an update of a previous SLR performed until 2010.11
The second part of the SLR was conducted to determine the value of laboratory and imaging tests in the diagnosis and the prognosis of EA, to study the differential diagnosis in patients with EA and to evaluate the performance of EA classification criteria in patients with a diagnosis of EA. Except for the imaging tests, this SLR was an update of the previous SLR performed until 2005 for the 2007 EULAR recommendations for EA management.6 For imaging tests, we used 2011 as a start date because of the previous SLR performed until 2011.12
The search was performed by a skilled librarian form the Columbia University, New York, USA and covered the databases MEDLINE, EMBASE, Cochrane, Central, Database of Abstracts of Reviews of Effects (DARE), Health Technology Assessment (HTA) and National Health Service (NHS) and those for the 2014 and 2015 American College of Rheumatology (ACR) and EULAR annual meetings. In addition, the reference lists of articles were manually searched to identify additional articles. Specific medical subject headings and additional keywords were used to identify all relevant studies (see online supplementary material S3).
Study selection
Inclusion criteria were formulated according to the PICOT framework (see online supplementary material S2). According to these predetermined selection criteria, titles and abstracts of all citations were screened and the full text of potentially relevant articles was reviewed. The search was limited to studies published in English that had a study population of more than 50 adults (≥18-year old) with EA included (arbitrary cut-off). Study types included controlled trials and observational studies. We did not exclude studies based on quality scores.
Data extraction, risk of bias and level of evidence
Two authors (CID and CH) used a predetermined data summary form to collect data on the study design, sample size, patient and control characteristics, definition of outcome measures and statistical analyses performed. Disagreements were resolved by consensus (CID, CH, BC and RL). Risk of bias of included studies was analysed by a checklist based on the criteria proposed by the Oxford Centre for Evidence-based Medicine.13 Level of evidence was evaluated for each included study according to the risk of bias analysis.
Results
Literature search results
For the first part of the SLR we retrieved 1643 citations. After screening titles and abstracts, 20 articles remained for detailed review; 4 studies met our inclusion criteria and were included (figure 1).
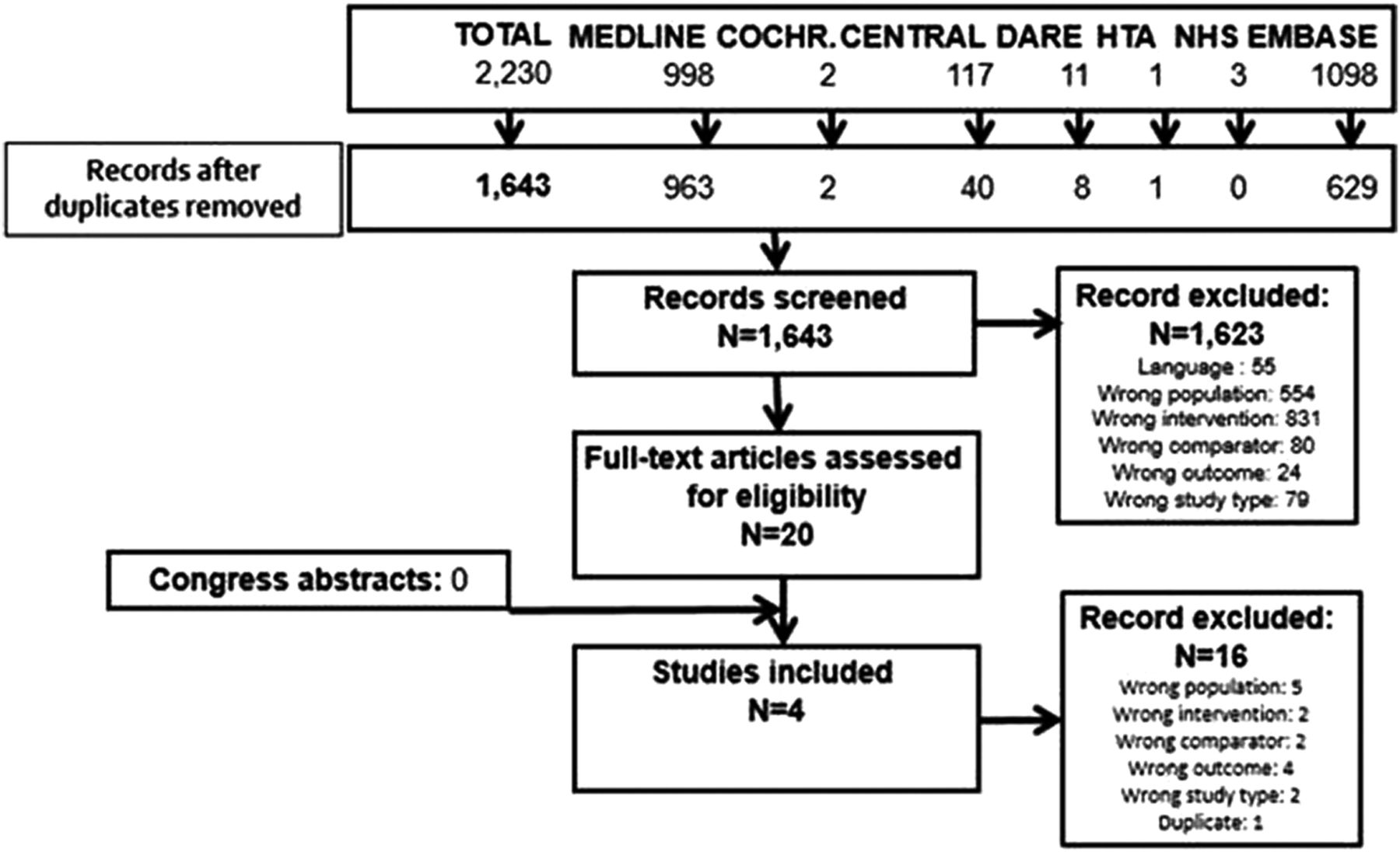
Flow chart of the first part of the systematic literature review.
For the second part, the search yielded 11 435 citations of which 162 articles remained for detailed review. Of these, 86 articles were excluded after reviewing the full text. The search of the ACR and EULAR annual meetings databases yielded 12 additional studies. So, 88 articles remained for review (figure 2).

{kind=link}
{kind=link}
Flow chart of the second part of the systematic literature review.
Recognition of EA and referral to a medical specialist
Previous SLR
This first research question was an update of a previous SLR published in 2013 by another EULAR task force that searched the literature available until November 2010.11 This previous SLR had identified four self-administering questionnaires to trace inflammatory arthritis.14–17 In addition, this previous SLR retrieved two studies supporting the need for early diagnosis and treatment to reduce joint damage and improve clinical outcomes, ideally within 3 months of symptom onset.2 ,18
Current SLR
Recognition of arthritis by general practitioners (GPs)
The aim of the search was to retrieve studies evaluating tools to be applied by a GP in patients with suspected EA to distinguish the presence of inflammatory arthritis from other conditions (table 1A). Two studies described simple questionnaires (inquiring about pain, swelling and stiffness) that had rather high sensitivity (94% and 86%) and specificity (93% and 93%) for EA.19 ,20 The main limitation of these two studies was that they have not been validated in independent cohorts yet.
Studies evaluating recognition and referral of early arthritis (EA) patients
Referral to a medical specialist
The aim of the search was to retrieve studies evaluating whether timing of referral to a rheumatologist may influence the outcome of patients with EA. Two studies suggested a better outcome in patients who had been referred early (within 3 months) than in those who had been referred later (table 1B).5 ,21 In one study, orthopaedic surgery has occurred less frequently in those who had been referred early (within 3 months) as compared with those who had been referred late (92 patients in the early referral group (n=533) vs 123 in the late referral group (n=518) had orthopaedic surgery).21 In another study, prolonged (≥1 year) drug-free remission was more frequent in patients that had been referred early (31 of 168 (18%)) as compared with late (41 of 389 (11%)).5 Patients that had been referred late (beyond 12 weeks) had a 1.3-fold higher rate of radiographic progression than did patients that had been referred early.5
Laboratory tests and imaging exams in the diagnosis of EA
Previous SLR
Laboratory tests
We have updated the SLR of the 2007 EULAR recommendations on EA management (that included literature until 2005).6 The previous recommendations included the following laboratory tests in the diagnostic procedure: complete blood cell count, urinary analysis, transaminase and antinuclear antibody testing and, depending on the context, tests for uric acid, Lyme's disease and parvovirus infection, urethral or cervical swab cultures, antibacterial serology and tests for hepatitis B or C infection. These recommendations were entirely based on the opinions of the consulted experts and a dedicated literature search had not been performed. Diagnostic value of rheumatoid factor (RF) and anticitrullinated-peptide antibodies (ACPAs) had not been specifically evaluated.
Imaging tests
We have updated a previous SLR of the literature available until June 2011, informing the 2013 EULAR recommendations for the use of joint imaging in the clinical management of RA.12 In this previous set of recommendations, ultrasonography (US) and MRI were considered ‘useful to improve the certainty of a RA diagnosis’. In contrast, bone/joint scintigraphy and positron emission tomography had reportedly little benefit for detecting joint inflammation over clinical examination alone.
Current SLR
The aim of the current search was to retrieve studies evaluating the diagnostic value of laboratory tests and/or imaging tests in patients presenting with EA in terms of classifying them as RA or as other inflammatory rheumatic diseases. The design of the included studies is reported in online supplementary material S4. We have found 28 studies for laboratory tests and 5 for imaging tests. In all included studies, the outcome was confirmation of the diagnosis of RA. The time for evaluation of this outcome was usually 1 year.
Laboratory tests
The included studies mainly evaluated RF (21 studies22–42) and ACPAs, in particular anticyclic citrullinated peptide (anti-CCP) antibodies (26 studies22–30 ,32–48) (see online Supplementary materials S5). The value of RF for the diagnosis of RA in patients presenting with EA was heterogeneous. In almost two-thirds of the studies, sensitivity of RF for a RA diagnosis was moderate, between 40% and 60%. In the last third, sensitivity was higher (60–80%). Half of the studies reported a specificity of RF for a RA diagnosis between 60% and 80%. In the other half, specificity was higher (80–100%). ACPAs’ sensitivity for a RA diagnosis was similar to that of RF, with values between 40% and 60% in 10 studies and between 60% and 80% in 6 studies. On the other hand, the specificity of ACPA testing for a RA diagnosis was higher than that of RF testing, with more than three-quarters of the studies reporting values between 80% and 100%. According to seven of the studies, testing (and interpreting) the combined results of RF as well as ACPAs was of minor additional benefit for the specificity, in comparison with testing one of each alone.22 ,27 ,28 ,33 ,37 ,38 ,40 The value of RF and ACPA titres was investigated in only two studies.32 ,37 In the study by Funovits et al,32 positivity of RF or ACPAs with high titres (defined by a value higher than three-fold the normal rate) was associated with a diagnosis of RA (OR 3.9 (3.0 to 5.0)), almost twice as frequently than positivity with low titres (OR 2.2 (1.8 to 3.3)).
The type of ACPAs most frequently studied was anti-CCP antibodies. Seven studies have also evaluated anticitrullinated vimentin antibodies, and did not report additional benefits in diagnosing RA compared with anti-CCP antibodies.25 ,31 ,36 ,42 ,44 ,46 ,48 One study has evaluated anticarbamylated (anti-CarP) antibodies and found a sensitivity of 53% and a specificity of 80% for a diagnosis of RA, but combining anti-CarP antibodies with RF and ACPAs was not better than ACPAs and RF alone.41
As in the previous SLR, we did not find appropriately designed studies that evaluated C reactive protein (CRP) levels, erythrocyte sedimentation rates (ESRs), antinuclear antibodies or any other serological test performed in patients with EA and aiming at defining specific diagnoses other than RA. In particular, no such studies in which the outcome was a diagnosis of inflammatory arthritis other than RA was retrieved. Therefore, we were unable to evaluate the usefulness of laboratory tests for the diagnosis of diseases other than RA.
Imaging tests
The included studies evaluated mainly MRI (three studies35 ,49 ,50) (see online supplementary materials S5). Other imaging modalities were US (one study51) and bone densitometry (BMD) performed on hand X-rays (one study52). Included MRI studies evaluated the likelihood that various MRI features (bone oedema, synovitis and tenosynovitis) found in patients with EA evolved into a diagnosis of RA. Based on these studies, presence of MRI bone oedema on wrist and metatarsophalangeal joints and presence of MRI hand tenosynovitis are reportedly specific (specificities more than 80%) but not sensitive (sensitivities <35%) markers for a diagnosis of RA. Therefore, the clinical relevance of MRI to establish a diagnosis of RA in patients with EA appears to be limited. According to the included US study, detection of hand flexor or extensor tenosynovitis by US appeared to be associated with RA diagnosis in patients with EA (OR 6.3 (2.2 to 18)) but, as for now, these data were only published in a congress abstract and sensitivity and specificity were not reported.51 So, our current SLR does not allow us to conclude on the clinical use of US as a diagnostic marker for RA in patients with EA.
Laboratory tests and imaging tests in the prognosis of EA
Previous SLR
Laboratory tests
The previous 2007 EULAR recommendations for EA management had identified a high ESR, a high CRP level and the presence of RF and/or anti-CCP antibodies as independent predictors for long-term radiographic progression.
Imaging tests
The previous SLR preceding the 2013 EULAR recommendations for the use of joint imaging tests in the clinical management of RA had identified the presence of synovitis on US or MRI, joint damage on conventional radiography and bone marrow oedema (osteitis) on MRI as predictors of subsequent radiographic progression in early RA.12 An independent predictor of progression of erosions was reportedly ‘early bone loss’ in the hand, measured as a decrease in estimated BMD in the first year of disease by digital X-ray radiogrammetry. Inflammatory changes on bone scintigraphy seemed to be associated with radiographic progression.
Current SLR
The aim of the search was to retrieve studies evaluating the prognostic value of laboratory tests and/or imaging tests in terms of radiological and functional outcome and clinical remission. Details of the selected studies are reported as online supplementary material S4.
We found 35 studies for laboratory tests and 12 studies for imaging tests.
Laboratory tests
Included studies evaluated mainly RF (19 studies24 ,25 ,47 ,53–68) and ACPAs, in particular anti-CCP antibodies (25 studies24 ,25 ,47 ,55–66 ,69–78) (see online supplementary materials S6). Apart from three studies47 ,61 ,64 on clinical remission, all included studies used radiographic progression as the primary outcome, although with various definitions.
The value of RF as a prognostic marker in patients with EA was reportedly heterogeneous and extremely dependent on the prevalence of radiographic progression in the cohorts. Depending on the studies, positive predictive values (PPVs) of RF for radiographic progression ranged from 20% to 92%, without a clear trend towards one or the other of these extreme values. Negative predictive values (NPVs) were better, with half of the studies reporting a NPV of RF for radiographic progression between 60% and 80%, and the other half reporting even higher NPVs (80–100%). PPVs of ACPAs for radiographic progression in patients with EA were also heterogeneous, with approximately half of the studies reporting low PPVs with values between 20% and 40%, and the other half reporting high PPVs with values over 80%. On the other hand, NPVs of ACPAs for radiographic progression were high, around 80% in the majority of the included studies.
According to four of the studies, testing (and interpreting) the combined results of RF as well as ACPAs did not provide added benefit to the prognostic value of RF or ACPAs alone.56 ,59–61 We retrieved three studies reporting an influence of autoantibody titres on radiographic progression.24 ,25 ,57 In two studies, classifying patients by ACPA titres revealed a dose–response relationship between increased baseline ACPA titres and radiographic progression.25 ,57 In the third study, structural damage at 2 years (Larsen scores) was significantly higher when baseline RF titres were high as compared with low or absent.24
Two studies of multibiomarker disease activity (MBDA) assessment were retrieved.78 ,79 The correlation of the MBDA score with radiographic progression was weak (OR per unit of increase: close to 1.0 (1.0 to 1.1)). The association of higher (>44) MBDA scores and radiographic progression was better (OR vs low score 3.9 (1.0 to 14.3)), but, while the NPV for this cut-off was high (97%), the PPV did not exceed 20%; and thus MBDA scores appear to be of minor value for clinical practice.
One study investigated the value of anti-CarP antibodies.68 In this study, the prognostic value of anti-CarP was similar to that of anti-CCP antibodies.
Our search did not identify studies on the prognostic value of ESR and CRP level in patients with EA.
Imaging tests
Included studies evaluated mainly baseline hands and feet X-rays (six studies), with different radiological parameters according to the studies (van der Heijde-modified total Sharp score, joint erosions, BMD loss) (see online supplementary materials S6).47 ,58–60 ,72 ,75
Structural damage on baseline X-rays of hands and feet was associated with further radiographic progression, with particularly high NPVs (around 90%). This suggests that in the absence of baseline structural damage the likelihood of further erosive evolution is low. PPVs of baseline X-rays were reportedly low (around 30%) but this should be nuanced by the low prevalence of the outcome in the cohorts.
Other studies evaluated MRI (one study80) and US (three studies64 ,81 ,82). Given the available data in these studies, it was difficult to assess the predictive values of these imaging tests in patients with EA. The US studies were conducted using various parameters, outcomes and populations, and therefore the clinical relevance of US as a marker of prognosis in patients with EA appeared to be limited thus far. Power–Doppler (PD) at baseline seemed to be the most relevant US parameter, with an OR for the prediction of an increase in the erosion sharp score ≥5 at 1 year of 1.2 (1.0 to 1.4) per unit of increase in the PD score (scale 0–3 for each joint).81 Only one MRI study was included,80 reporting an increase of only 10% (OR 1.1 (1.0 to 1.2)) in the risk of radiographic progression (change in Genant-modified Sharp score >3 units) at 1 year for every increase of 5 units in the bone oedema MRI score (scale 0–90).
Studies addressing the prognostic value of other imaging modalities (scintigraphy, positron emission tomography) were not found.
Differential diagnosis for patients referred with undifferentiated EA
Previous SLR
On the basis of expert opinion, the previous 2007 EULAR recommendations advised excluding diseases other than RA before giving a definite diagnosis.6 These other diseases included (but were not limited to) infectious arthritis, connective tissue disease, reactive arthritis and other spondyloarthritides and crystal arthropathies.
Current SLR
In five of the six studies retrieved, RA appeared to be the diagnostic category with highest frequency, between 20% and 45% of all patients (table 2).22 ,23 ,37 ,83 ,84 Other diagnoses frequently noted for patients with EA in these studies were psoriatic arthritis, peripheral spondyloarthritis, crystal-induced arthritis, connective tissue disease and reactive arthritis.
Differential diagnosis for patients referred with undifferentiated EA
Performance of current EA classification criteria
Previous SLR
Previous EULAR SLRs had not addressed this topic. Most of the current classification criteria were established <10 years ago and the frequency of articles in this field is increasing, in particular for the 2010 ACR/EULAR criteria for RA.
Current SLR
The aim of the search was to retrieve studies evaluating the prognostic value (in terms of radiographic progression or persistent disease) of the 2010 ACR/EULAR criteria for RA, ClASsification criteria for Psoratic Arthritis (CASPAR) criteria and 2009 Assessment of SpondyloArthritis international Society (ASAS) criteria, for early RA, early psoriatic arthritis and early peripheral spondyloarthritis, respectively (table 3).
Predictive performance of the 2010 ACR/EULAR classification criteria
We decided to include in our SLR studies using ‘prescription of methotrexate or (an)other DMARD(s)’ as a ‘proxy’ for an RA diagnosis by rheumatologists, just as for the development of the criteria.32 We also included studies using structural damage as an external standard for evaluating 2010 ACR/EULAR performance.
We found 13 studies related to 2010 ACR/EULAR criteria.45 ,85–96 The PPVs of these criteria to predict the persistent use of DMARDs was high, around 80% in all included studies. NPVs were lower but still over 60% in all studies. Only three studies evaluated the prediction of erosive disease: 2010 ACR/EULAR criteria had high NPVs (between 70% and 100%) but low PPVs.87 ,94 ,96
Studies about CASPAR or ASAS 2009 criteria were not found.
Discussion
Our results, as well as evidence from previously published literature,11 clearly supports the need for early referral (ideally within 3 months of symptom onset) of patients with EA to a rheumatologist, in order to reduce the likelihood of joint damage and to improve clinical outcomes. Our current SLR identified two studies of questionnaires that can be used by GPs to help detecting inflammatory arthritis. Unfortunately, these questionnaires were tested with only small samples and were not confirmed in independent validation cohorts. Validated tools that help GPs diagnose and refer EA are lacking.
According to our results, RA is the most frequent diagnosis that patients with EA will achieve. For this reason, an important limitation to the extrapolation of our results is that most of the literature data concerned patients with early RA and not patients with early undifferentiated arthritis. Another limitation is the heterogeneity of the outcomes definition according to the studies. For the studies on diagnosis, due to the lack of a clear gold standard for RA diagnosis, definition and prevalence of the outcome ‘RA diagnosis’ varied between the studies. The studies on prognosis used various definition for the outcome ‘radiographic progression’.
RF and ACPAs are the most frequently evaluated laboratory tests. In the literature, the sensitivity of these autoantibodies for an RA diagnosis in patients with EA is variable but moderately high on average (between 40% and 80%). An explanation for this variability is the difference in patient populations (in particular with regard to disease duration) across the studies. Specificity is better, notably for ACPAs with values frequently over 80%. These diagnostic values are slightly lower than those typically reported and this could be explained by the short disease duration of patients with EA. Prognostic values of RF and ACPAs in terms of predicting radiographic progression were very dependent on the prevalence of radiographic progression in the studies but NPVs were in general higher for ACPAs (around 80%) than for RF. PPVs were lower for both autoantibodies, probably because radiographic progression was infrequent. Our results allow us to conclude that both autoantibodies are useful tests in patients with EA, but that ACPAs have a higher diagnostic and prognostic value than RF in patients with EA.
Moreover, we can confirm that structural damage on baseline hands and feet X-rays is predictive of further radiographic progression in patients with EA. Regarding other imaging modalities, data are sparser and longitudinal studies are required to explore the diagnostic and prognostic value of MRI and US in patients with EA.
Finally, the 2010 ACR/EULAR classification criteria for RA appropriately predicts the persistent use of DMARDs after 1–5 years. This observation is consistent with a meta-analysis published in 2012, reporting a pooled sensitivity of 0.8 (0.7 to 0.8) and pooled specificity of 0.7 (0.6 to 0.8) for the criteria.97
In view of our results, it seems that more clinical research is needed to improve diagnosis and prognosis. Such research should aim at better referral questionnaires, better biomarkers, better evaluation of US and MRI and the development of prediction algorithms for long-term outcome.
Acknowledgments
The authors thank EULAR for supporting this SLR; Louise Falzon, librarian at the Center for Behavioral Cardiovascular Health, Columbia University Medical Center, New York, and former Trial Search Coordinator from the Cochrane Musculoskeletal Group, for assisting with the design of the search strategy; Sofia Ramiro (Leiden University Medical Center) and Cédric Lukas (rheumatology department, Lapeyronie Hospital, Montpellier University) for expert advice.
References
Footnotes
Contributors All authors took part in drafting the article or revising it critically for important intellectual content and final approval of the version to be published. CH, CID, BC and RL conceived this review. CH and CID reviewed the literature. CH, CID, BC and RL conducted the interpretation and analysis. CH, CID, BC and RL contributed to drafting the manuscript. Louise Falzon assisted with the design of the search strategy. Cédric Lukas reviewed the manuscript.
Competing interests CID has received honoraria from BMS, MSD, Pfizer, Roche-Chugai and UCB, and research grants from MSD, Pfizer, Roche-Chugai and UCB. CH has no conflict of interest. BC has received honoraria from BMS, Janssen, Lilly, MSD, Novartis, Pfizer, Roche-Chugai and UCB and research grants from Pfizer, Roche-Chugai and UCB, RL has received honoraria and/or research grants from AbbVie, Ablynx, Amgen, AstraZeneca, Bristol Myers Squibb, Celgene, Janssen, Galapagos, GlaxoSmithKline, Novartis, Novo Nordisk, Merck, Pfizer, Roche, Schering-Plough, TiGenix, UCB. RL is director of Rheumatology Consultancy BV.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement No additional data are available.