Article Text

Abstract
Objective To assess the efficacy and safety of modified-release (MR) versus immediate-release (IR) prednisone in newly diagnosed glucocorticoid (GC)-naïve patients with polymyalgia rheumatica (PMR).
Methods Patients were randomised to double-blind MR prednisone (taken at approximately 22:00) or IR prednisone (taken in the morning), 15 mg/day for 4 weeks. The primary end point was complete response rate (≥70% reduction in PMR visual analogue scale, duration of morning stiffness and C reactive protein (CRP) (or CRP <2× upper limit of normal (ULN))) at week 4. Non-inferiority was decided if the lower 95% confidence limit (MR vs IR prednisone) was above −15%. 400 patients were planned but only 62 were enrolled due to difficulties in recruiting GC-naïve patients with PMR with CRP ≥2×ULN.
Results The percentage of complete responders at week 4 was numerically greater for MR prednisone (53.8%) than for IR prednisone (40.9%). Non-inferiority of MR versus IR prednisone was not proven in the primary analysis on the per protocol population (N=48; treatment difference: 12.22%; 95% CI −15.82% to 40.25%). However, sensitivity analysis on the full analysis population showed an evident trend favouring MR prednisone (N=62; treatment difference: 15.56%; 95% CI −9.16% to 40.28%). Adverse events were generally mild and transient with no unexpected safety observations.
Conclusions The study showed a clear trend for favourable short-term efficacy of MR prednisone versus IR prednisone in early treatment of PMR. Further studies are warranted.
Trial registration number EudraCT number 2011-002353-57; Results.
- Polymyalgia Rheumatica
- Corticosteroids
- Autoimmune Diseases
- Inflammation
- Treatment
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Key messages
What is already known about this subject?
Optimising the timing of glucocorticoid (GC) administration in relation to endogenous cortisol rhythms and symptom severity using modified-release (MR) formulations can improve therapeutic potential in inflammatory conditions, as already demonstrated in rheumatoid arthritis.
Preliminary studies suggest that MR prednisone may also have benefits in polymyalgia rheumatica (PMR), but data from randomised controlled trials are lacking.
What does this study add?
This randomised controlled study showed a clear trend for a larger reduction in key PMR symptoms and levels of pro-inflammatory cytokine interleukin (IL)-6 with MR prednisone compared with immediate-release (IR) prednisone, although only 62 of a planned 400 patients were enrolled due to difficulties in recruiting GC-naïve patients with PMR and the study did not meet its primary objective of showing non-inferiority.
How might this impact on clinical practice?
Results from this study, though limited, suggest favourable efficacy of MR prednisone over IR prednisone in patients with PMR, and further confirmation should be sought from larger clinical trials.
Experience from this study demonstrates that careful consideration of PMR inclusion and response criteria is required.
Introduction
Polymyalgia rheumatica (PMR) is a common inflammatory rheumatic disease of older people1 characterised by new-onset bilateral shoulder and/or hip girdle pain with pronounced stiffness and an acute phase response.2 ,3 Glucocorticoids (GCs) are the mainstay of treatment and rapidly improve PMR symptoms;4 an initial flexible minimum effective GC dose of 12.5–25 mg prednisone (recognising demographics, comorbidities, comedications, GC risk factors and disease severity) is recommended by the 2015 European League Against Rheumatism (EULAR) / American College of Rheumatology (ACR) guidelines.5 ,6
Patients with inflammatory conditions such as PMR typically show circadian variations in clinical symptoms related to altered concentrations of inflammatory cytokines, melatonin and cortisol, with key symptoms usually most severe in the early morning.7–10 Modified-release (MR) prednisone has been developed to optimise oral GC treatment strategies with respect to circadian rhythms of inflammation by releasing prednisone ∼4 hours after the administration of the tablet in the late evening. The CAPRA (Circadian Administration of Prednisone in Rheumatoid Arthritis) studies confirmed that optimising the timing of GC administration improves the benefit:risk ratio of long-term, low-dose GC treatment in patients with rheumatoid arthritis (RA).10–12 Preliminary studies in PMR suggest that MR prednisone may also have benefits in this inflammatory condition.13
This randomised, double-blind, active-controlled, parallel-group, non-inferiority phase III clinical study aimed to assess the efficacy and safety of evening MR prednisone compared with morning administration of immediate-release (IR) prednisone in newly diagnosed patients initiating GC treatment for PMR.
Methods
Setting, patients and treatments
The study (EudraCT number 2011-002353-57) was conducted between March 2013 and March 2014 at 41 secondary care centres across nine European countries. Patients aged ≥50 years, newly diagnosed with PMR and previously untreated with GCs for PMR, were eligible for inclusion. According to the 2012 EULAR/ACR provisional classification criteria for PMR,14 ,15 the diagnosis had to be confirmed by all of the following at screening: (1) new-onset bilateral shoulder pain with/without hip girdle pain; (2) a PMR visual analogue scale (VAS) score ≥50 (0–100 scale); (3) duration of morning stiffness >45 min and (4) acute phase response shown by elevated C reactive protein (CRP; ≥2 times the upper limit of normal (ULN)). Patients were randomised in a 1:1 ratio to MR or IR prednisone for 4 weeks, and received 15 mg IR prednisone/placebo between 5:00 and 9:00 and 15 mg MR prednisone/placebo at 22:00±30 min. No rescue medication was used, and other medications for the treatment of PMR, including analgesics and coanalgesics, were prohibited during the study.
Study assessments
Every morning and evening, patients completed an electronic diary (Log Pad, PHT Corporation), recording how their PMR had affected them (PMR VAS), their overall pain (global pain VAS), pain in their arms and shoulders (shoulder pain VAS), their overall level of fatigue/tiredness (fatigue VAS), duration of morning stiffness and time of medication intake. Interleukin-6 (IL-6), CRP and erythrocyte sedimentation rate (ESR) were measured at baseline, week 1 (CRP/ESR only) and week 4. Adverse events (AEs) were recorded throughout the study.
Statistical analyses
The primary objective was to demonstrate non-inferiority of MR prednisone administered in the evening versus IR prednisone administered in the morning, with regard to the percentage of complete responders at week 4 (primary end point). Complete response was defined as ≥70% improvement from baseline in PMR VAS, duration of morning stiffness and CRP (or CRP <2×ULN)).16 The primary end point was analysed using logistic regression with treatment as a factor and baseline PMR VAS score, duration of morning stiffness and CRP as covariates. Non-inferiority was concluded if the lower limit of the two-sided 95% CI was above −15%.
The primary analysis was performed using the per protocol population (PPP) with sensitivity analysis performed using the full analysis population (FAP; all randomised patients who received ≥1 dose of study treatment). Assuming a complete response rate of 69%16 in the comparator arm at week 4, an expected treatment difference of 0%, a non-inferiority bound of −15%, 80% power and a two-sided α of 0.05, a sample size of 300 patients in the PPP (∼400 randomised patients) was required. Further methodology can be found in the online supplementary material.
supplementary data
Results
Study patients
The study enrolled, randomised and treated 62 patients (21 male patients, 41 female patients), all Caucasian, with a mean age of 69 years (see online supplementary table S1). All patients were included in the FAP and safety population, while 48 patients (77.4%) were included in the PPP. The study experienced a high screen failure rate (62/124 patients screened), primarily due to an insufficiently high CRP value (77% of screen failures did not have CRP ≥2×ULN). The difficulties in recruiting GC-naïve patients with PMR fulfilling the inclusion criteria, and cessation of production of the comparator Decortin 1 mg tablets, led to the premature termination of the study after 11 months' recruitment. Participant flow is shown in figure 1.
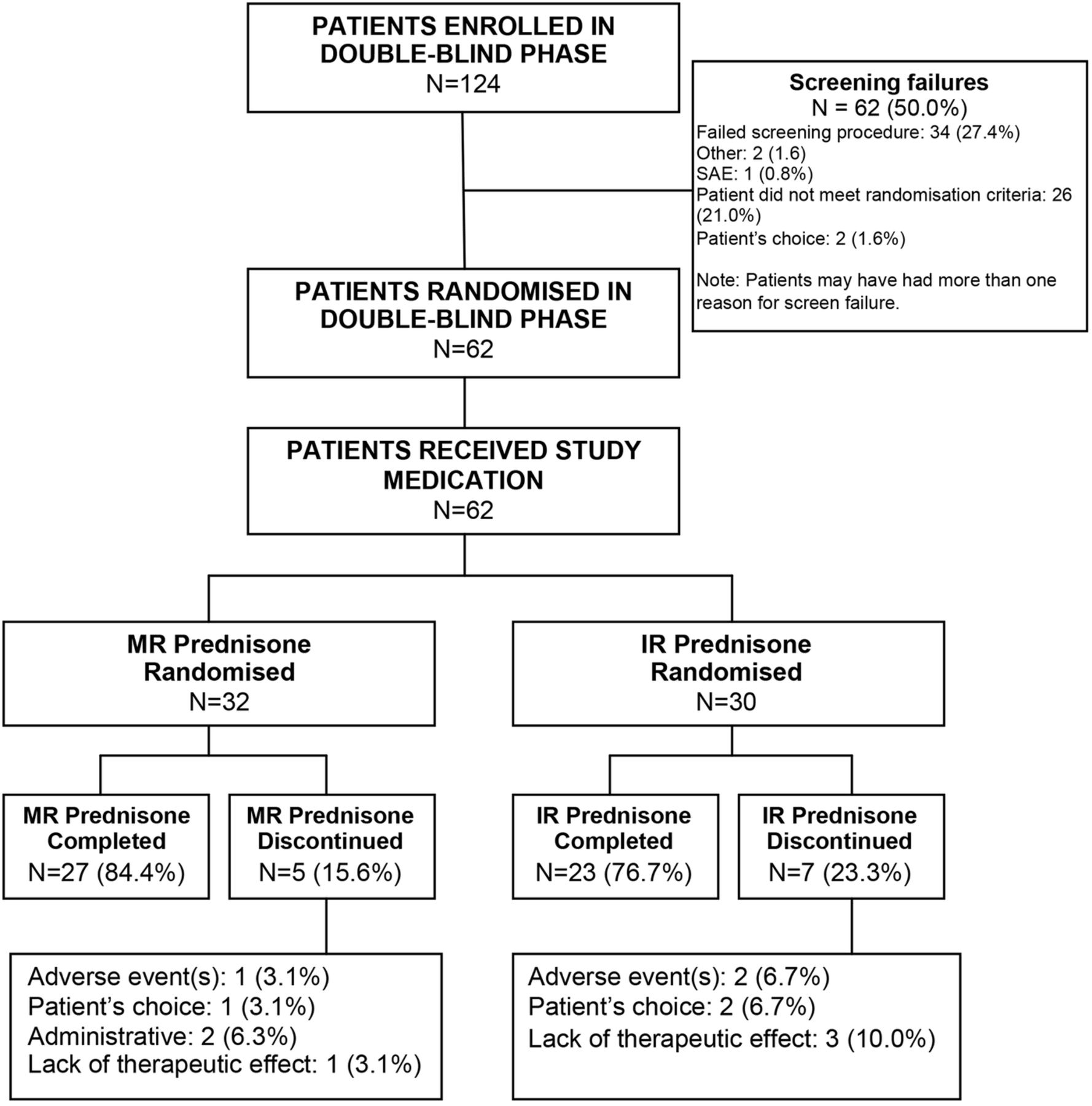
{kind=link}
Participant flow.
Primary end point
The percentage of complete responders at week 4 was numerically higher for MR prednisone (53.8%) than for IR prednisone (40.9%, table 1), although non-inferiority of MR versus IR prednisone was not proven in the primary PPP analysis (treatment difference: 12.22% in favour of MR prednisone; 95% CI −15.82% to 40.25%). Sensitivity analysis on the FAP showed a trend in favour of MR prednisone (treatment difference: 15.56%; 95% CI −9.16% to 40.28%). The study was relevantly underpowered (N=48 vs planned 300 patients in the PPP) due to recruitment difficulties and early study termination.
Response rates
Secondary end points
A clear consistent trend for a larger favourable effect of MR prednisone compared with IR prednisone was observed for all secondary end points (except CRP and ESR) at weeks 1 and 4 (table 2). The percentage of responders (patients with ≥70% improvement from baseline) was also greater for MR prednisone than for IR prednisone at weeks 1 and 4 for all secondary end points (see online supplementary table S2). Clinically significant mean reductions and treatment differences of more than 10 points in favour of MR prednisone were observed for PMR VAS, global pain VAS and shoulder pain VAS (table 2). MR prednisone was markedly more effective than IR prednisone in reducing morning stiffness duration from as early as week 1 (mean reduction of 326 vs 160 min, table 2), which was supported by the percentage of responders (44% vs 17%, online supplementary table S2).
Secondary efficacy results (full analysis population)
MR prednisone indicated good efficacy in reducing IL-6 levels compared with IR prednisone at week 4 (decrease from baseline of −37.4 vs −29.8 pg/mL, table 2). Notable reductions in CRP and ESR were observed in both treatment groups, with a larger decrease for IR prednisone (although we noted that baseline CRP values were higher in the IR prednisone group, and mean CRP values at week 4 were lower for MR prednisone (8.4 mg/L) than for IR prednisone (17.9 mg/L)).
Safety
The AEs reported during the study are presented in online supplementary table S3. While more patients experienced AEs in the MR prednisone group (19 (59%); 8 (25%) related) than the IR prednisone group (9 (30%); 3 (10%) related), this was not driven by any specific AEs and the majority of subjects in both treatment groups experienced non-related AEs. Two patients experienced serious AEs (pancytopenia and temporal arteritis), which were not treatment-related. Three patients prematurely discontinued due to AEs: upper abdominal pain in the MR prednisone group and temporal arteritis and burning sensation in the IR prednisone group (figure 1).
Discussion
In this study, the complete response rate at week 4 was numerically greater with MR prednisone (53.8%) than with IR prednisone (40.9%). Non-inferiority of MR prednisone versus IR prednisone was not proven for the primary end point; however, even with only 48 patients in the PPP (vs the 300 planned), the point estimate was clearly in favour of MR prednisone and the lower 95% confidence limit was only marginally below (−15.82%) the decided non-inferiority threshold of −15%. Sensitivity analysis on the FAP supported the trend in favour of MR prednisone, and secondary efficacy results were encouraging, showing a clear consistent trend for a stronger effect of MR prednisone compared with IR prednisone. Of note, evening MR prednisone was associated with significantly greater reductions in IL-6 levels than morning IR prednisone, suggesting a more effective downregulation of night cytokine synthesis.17 These results are similar to findings in the CAPRA studies in RA.10 ,12 Consistent with the CAPRA-1 study, we observed no significant difference between MR prednisone and IR prednisone on other inflammatory markers (CRP and ESR).
The study experienced a higher than expected screen failure rate (50%), primarily due to patients demonstrating lower CRP values not fulfilling the strict inclusion criteria when referred. It appears that in suspected PMR, primary care practitioners are willing to refer GC-naïve only patients with mild elevation or normal levels of inflammatory markers. However, it is likely that this population may contain predominantly non-inflammatory PMR mimics.18
The CAPRA studies have already confirmed that optimising the timing of GC administration improves the benefit:risk ratio of low-dose GC treatment in RA, and the open-label extension of the CAPRA-1 study11 and other publications19 ,20 confirmed positive long-term effects. A recent clinical experimental study further supports the use of chronotherapy in PMR.9 Although the formal criteria of non-inferiority were not met, our study showed a clear trend for a favourable clinical effect of MR prednisone over IR prednisone in patients with PMR. Further confirmation should be sought from a large clinical trial in patients with PMR, with careful consideration of inclusion and response criteria, based on the present study experience.
Acknowledgments
The authors would like to thank all the study investigators and participants and members of the study team from Mundipharma Research GmbH & Co. KG. Karen Mower (Scientific Editor) provided medical writing assistance that was funded by Mundipharma Research Limited.
References
Footnotes
BD and FB share senior authorship.
Contributors MC, MH, BD and FB were involved in the development of study protocol. MC, BD and FB were involved in patient recruitment and data acquisition. SL was involved in data analysis. MC, MH, SL, BD and FB were involved in manuscript preparation and approved the final version of the manuscript.
Funding The investigation was supported by Mundipharma Research Limited.
Competing interests MC received grant/research support from Horizon Pharma, is a consultant for Mundipharma International and is on the speaker’s bureau for Mundipharma International. MH is an employee of Mundipharma Research GmbH & Co. KG. SL is an employee of Mundipharma Research GmbH & Co. KG. BD received grant/research support from NAPP Pharmaceuticals, and is a consultant for Servier, Roche, Merck, GSK & Mundipharma. FB received grant/research support from Horizon Pharma, is a consultant for Mundipharma International and Horizon Pharma, and is on the speaker’s bureau for Mundipharma International and Horizon Pharma.
Ethics approval The Independent Ethics Committee of each centre reviewed and approved the protocol, and written informed consent was obtained from all patients before enrolment.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement No additional data are available.