Article Text

Abstract
Objectives We aimed to investigate the prevalence of dyslipidemia in patients with osteoarthritis (OA) and whether OA and dyslipidemia are associated.
Methods We performed a systematic literature review and a meta-analysis, including cross-sectional, cohort and case–control studies, to assess the number of patients with OA and/or dyslipidemia. We calculated the mean (±SD) prevalence of dyslipidemia in patients with and without OA and the risk of dyslipidemia (OR, 95% CI) among patients with OA.
Results From 605 articles screened, 48 were included in the analysis (describing 29 cross-sectional, 10 cohort and 9 case–control studies). The mean prevalence of dyslipidemia was 30.2%±0.6% among 14 843 patients with OA and 8.0%±0.1% among 196 168 without OA. The risk of dyslipidemia was greater with than without OA overall (OR 1.98,95% CI 1.43 to 2.75, p<0.0001) and with knee OA (OR 2.27, 1.33 to 3.89, p=0.003) and hand OA (OR 2.12, 1.46 to 3.07), p<0.0001).
Conclusion The risk of dyslipidemia was twofold greater with than without OA, so lipid disturbances could be a risk factor for OA. Such a result supports the individualisation of the metabolic syndrome-associated OA phenotype.
- Osteoarthritis
- Dyslipidemia
- Cholesterol
- Metabolic Syndrome
- Meta-analysis
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Key messages
What is already known about this subject?
Metabolic disturbances such as obesity or diabetes mellitus are associated with osteoarthritis (OA), but data about the link between OA and lipid disturbances remain conflicting.
What does this study add?
This is the first systematic review and meta-analysis demonstrating an association between OA and dyslipidemia. This result reinforces the concept of the metabolic syndrome-associated OA phenotype.
How might this impact on clinical practice?
This study emphasises the need to screen and manage cardiovascular comorbidities, especially lipid disturbances in patients with OA in clinical daily practice.
Introduction
Osteoarthritis (OA) is the most common joint disease and a major cause of pain and disability. It is currently considered a disease with multiple distinguishable phenotypes: post-traumatic, ageing-related, genetic and metabolic syndrome (MetS)-associated OA.1 Metabolic OA, the most commonly studied phenotype, is defined by the association between OA and MetS, associating obesity, hyperglycaemia with insulin resistance, dyslipidemia and hypertension.2 Metabolic OA mainly affects middle-aged people (45–65 years) and leads to knee, hand and generalised OA. The association between OA and MetS has been reported in several epidemiological studies.3 4 The pathophysiological link between both diseases could be chronic low-grade systemic inflammation occurring in both conditions.5
The association of OA with each MetS component has been investigated.6 Obesity and overweight are independently linked to hand OA, with a twofold increased risk.7 This association suggests the release of inflammatory mediators by adipose tissue adipokines. We recently reported an association between OA and diabetes mellitus, with a 1.46-fold increased risk of OA with diabetes mellitus and a 1.41-fold increased risk of diabetes mellitus with OA.8 The link between both pathologies could be explained by the action of pro-inflammatory cytokines and oxidative stress occurring in both diseases.9–12
The link between OA and the other components of MetS remains debated. Experimental studies have suggested that lipid disturbances could be involved in OA pathophysiology,13 but epidemiological studies revealed heterogeneous results.
With a systematic literature review and meta-analysis, we aimed to investigate the prevalence of dyslipidemia in patients with OA and assess whether OA and dyslipidemia are associated.
Methods
The systematic review was registered on PROSPERO (CRD: 42016037290).
Literature search
We performed a systematic search of articles in MEDLINE via PubMed, EMBASE and the Cochrane library. The keywords used for the PubMed search were (((‘Dyslipidemias’[Mesh] OR ‘Hypertriglyceridemia’[Mesh]) OR ‘Hypercholesterolemia’[Mesh]) OR ‘HDL’[All Fields] OR ‘LDL’[All Fields] OR ‘Triglycerides’[All Fields] OR ‘Hyperlipidemias’[Mesh]) OR ‘Cholesterol’[Mesh] OR ‘Metabolic Syndrome X’[Mesh] AND ‘Osteoarthritis’[Mesh] AND (‘humans’[MeSH Terms] AND (English[lang] OR French[lang])). No time limit was set for publication date, and articles published up to 1 January 2016 were searched. We also searched the abstracts from international meetings of the American College of Rheumatology (ACR), European League Against Rheumatism, Société Française de Rhumatologie, European Society of Cardiology, Endocrine Society’s Annual Meeting and European Congress of Endocrinology.
Study selection
We selected articles published in English or French that described observational studies of adults (>18 years of age) with cohort, case–control and cross-sectional designs. Studies were included if they specified the number of patients with OA and dyslipidemia and/or the prevalence or incidence of OA in patients with dyslipidemia and/or dyslipidemia in patients with OA, and/or the mean values of parameters of dyslipidemia in patients with and without OA and/or the existence or not of an association between OA and dyslipidemia. We excluded non-observational studies (therapeutic trials, reviews, letters and case reports). Articles that did not mention the number of patients with OA or dyslipidemia and those that did not evaluate the link between the two diseases were excluded. The selection of articles was based on titles and abstracts, then full texts.
Data synthesis
We extracted the following data: publication data (title of the article, first author, journal and publication date), study design (type of study, year(s) of inclusion, study quality score), population (total number of patients included, mean age and sex of patients), methodology of articles (the definition used for OA and dyslipidemia, OA location) and data needed for statistical analysis (number of patients with OA and/or dyslipidemic patients; mean total cholesterol (TC), low-density lipoprotein (LDL), high-density lipoprotein (HDL) and triglyceride (TG) levels (mg/dL or mmol/L); and number of patients receiving statins, number with MetS and number with obesity or mean body mass index (BMI) in kg/cm2). The quality of the study was estimated by using the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) scale, the score expressed in percentage of positive answers in relation to the number of items selected.14
Statistical analysis
First, we performed a descriptive analysis of the prevalence of dyslipidemia in patients with and without OA and used the number of patients with dyslipidemia and total number with and without OA. To estimate this prevalence from cohort longitudinal prospective studies, we used baseline data. Prevalence was expressed as mean±SD Second, we calculated the mean TC, LDL, HDL and TG levels in patients with and without OA. Third, for studies examining an association between OA and dyslipidemia, we calculated the risk of dyslipidemia with OA by estimating the overall OR with 95% CIs. The data were extracted from studies examining the number of dyslipidemic patients with and without OA. We used Revman V.5.3 for the meta-analysis with a fixed-effects model. Heterogeneity was assessed by the I² index; with I²>50% (high heterogeneity), we used a random-effects model, and with I2 <50% (low heterogeneity), we used a fixed-effects model. With strong heterogeneity, we used a randomised-effects analysis. To investigate potential publication bias, we have performed the funnel plot. The association was considered positive with OR >1, and the result was considered statistically significant with p≤0.05. We performed sensitivity and subgroup analyses.
Results
Characteristics of studies included
The selection of articles is reported in the flow chart (figure 1). We identified 605 publications; 48 articles (including 13 abstracts) from 43 studies were included (2 articles from the SEKOIA study, 4 from the FRAMINGHAM study and 2 from the National Health and Nutrition Examination Survey III). One abstract15 was obtained from the EMBASE database and not from screening congress abstracts. The 48 articles described 29 cross-sectional, 10 cohort and 9 case–control studies. Among them, 29 articles involved the OA population and 19 the general population (table 1). We did not find any studies based on a cohort of patients with dyslipidemia, which explains why the prevalence or relative risk of OA in patients with dyslipidemia was not calculated. Table 2 shows the definitions of OA and dyslipidemia in selected studies.
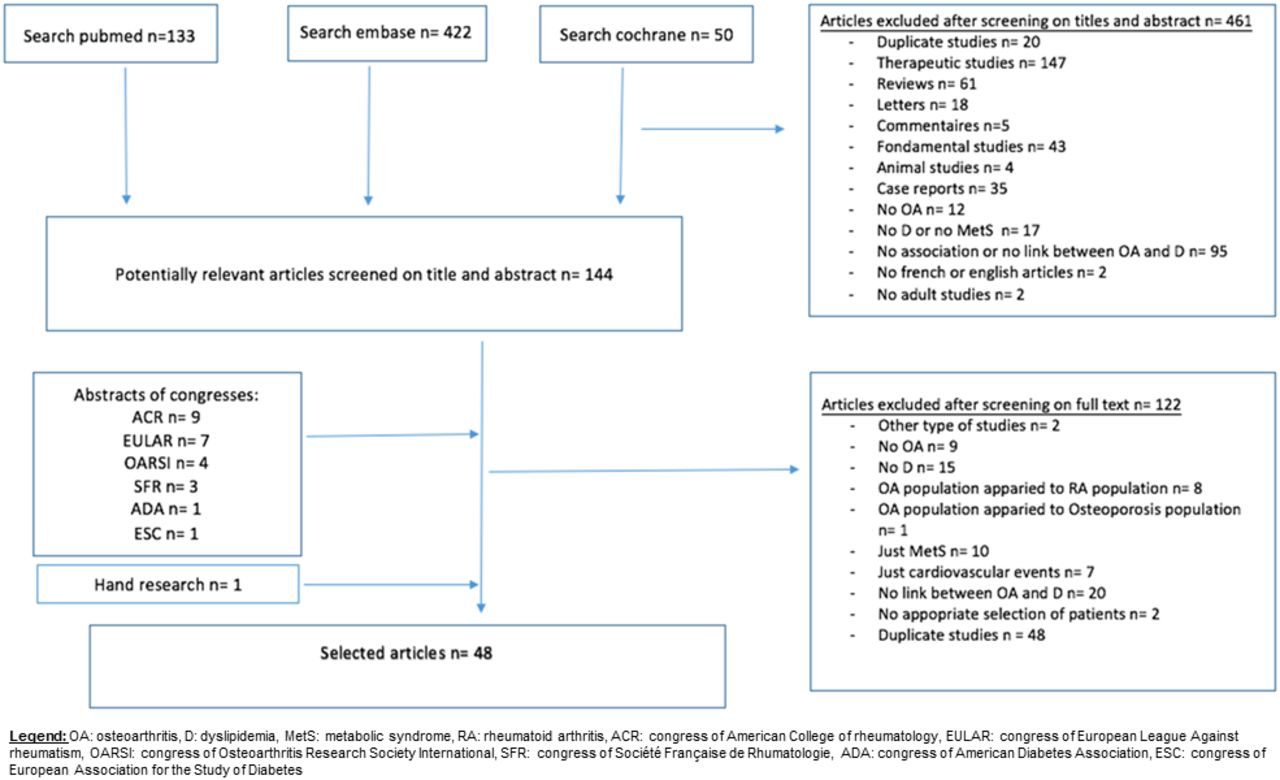
Flow chart of articles in the study
Description of the 48 articles studies selected for analysis
Characteristics of the 48 included articles: definitions of osteoarthritis (OA) and dyslipidemia, outcomes and Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) study quality
The median STROBE quality score was 69.1% (range 42%–91%). Nine articles had a STROBE quality score <60% (table 3).
In total, 30 articles assessed the association of OA and dyslipidemia, 30 assessed the prevalence of dyslipidemia among patients with OA and 22 assessed mean lipid level values among patients with OA (table 3).
Patient characteristics
This study involved 306 044 patients. The mean age range was 39.0±4.716 to 77.5±9.0 years.17 The mean proportion of females was 53.2% (range 40.6%18 to 100%19–22). The localisation was the knee in 23 articles,3 15 16 19–21 24–40 hand in 9,15 22 41–47 generalised OA in 3,25 31 47 hip in 3,25 34 37 spine in 248 49 and shoulder in 1.17 MetS was reported in nine articles,4 20 24 28 30 36 40 43 50 the prevalence of MetS ranged from 5%24 to 97.5%.40 The prevalence of obesity ranged from 7.8%51 to 100%15 40 and BMI from 22.3±2.730 to 37.3±5.9 g/cm2.40 Seven articles described the use of statin treatment (table 3).
Characteristics of the population on the 48 included articles: number, age, gender, overweight proportion
Prevalence of dyslipidemia among patients with and without OA (table 4)
Main results of prevalence of dyslipidemia and mean lipid-level values in patients with osteoarthritis (OA) and non-OA patients
The mean prevalence of dyslipidemia was 30.2%±0.6% among 14 843 patients with OA and 8.0%±0.1% among 1 96 168 without OA. The mean prevalence with knee OA was 27.6%±1.4%,15 20 24 25 28 30–35 37 38 hand OA 37.6%±1.6%,22 43–47 generalised OA 30.5%±3.9%,25 31 47 hip OA 20%±2.1%25 34 37 and symptomatic OA was 21%.28 44
Mean lipid-level values with and without OA (table 4)
The mean lipid-level values for patients with and without OA were for TC, 245±25.1 and 233.1±17.5 mg/dL; LDL, 126.5±20.7 and 136.9±15.9 mg/dL; HDL, 54.4±8.9 and 53.1±7.5 mg/dL; and TG, 137.3±80.3 and 131±27.3 mg/dL.
Association between dyslipidemia and OA
Overall, 30 articles indicated the presence or the absence of an association between OA and dyslipidemia; 21 (70%) showed a positive association between OA and dyslipidemia3 4 15 18 19 21 23 24 25 30 31 39 40 47 48 52–57 ; 12/18 articles (67%) with STROBE score >60% found a positive association.3 4 18 19 21 24 30 47 48 52 54 55 In addition, 4/7 articles19 25 31 47 that reported an OR adjusted on age and BMI found a positive association. Among the three with negative association findings after adjustment, two had a STROBE score >60%.34 37
Overall risk of dyslipidemia with OA: meta-analysis
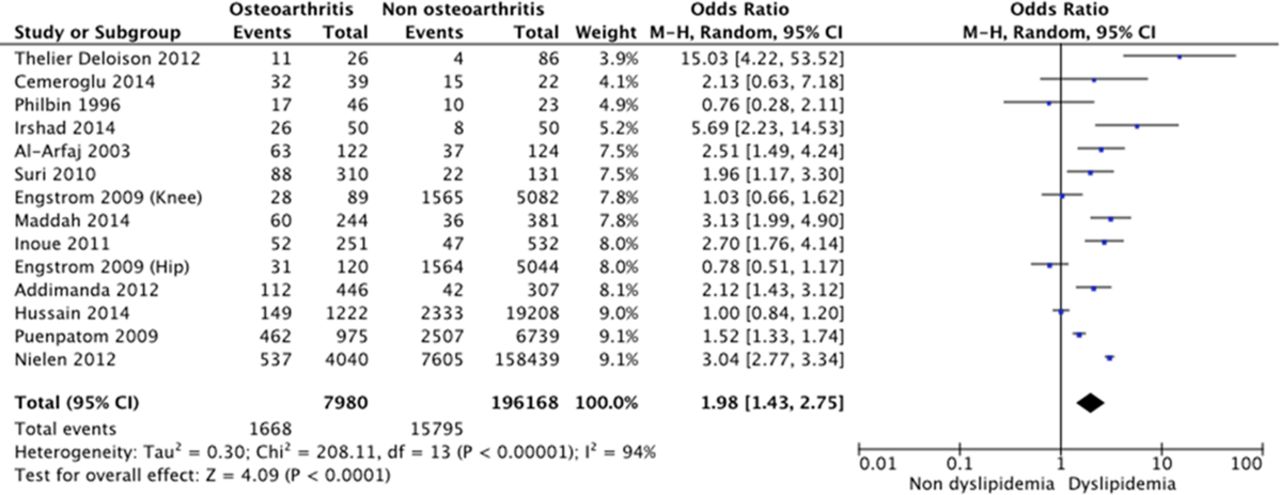
Among 204 148 patients from 13 articles,4 15 22 24 30 31 34 37 47 48 54–56 the overall OR was 1.98 (95% CI 1.43 to 2.75, p<0.0001; I2=94%), evaluated by a random-effects model (figure 2).

{kind=link}
{kind=link}
Forest plot for dyslipidemia among patients with and without osteoarthritis (OA).
Risk of dyslipidemia with OA: sensitivity analyses
To strengthen our results, we performed four sensitivity analyses. First, we removed the studies that did not use ACR criteria or Kellgren-Lawrence grading for OA diagnosis: among 2568 patients from the six remaining articles,22 24 30 31 47 56 the risk of dyslipidemia was increased with than without OA (OR 2.64, 95% CI 2.14 to 3.26, p<0.00001, I2=0%). Second, we excluded studies with a STROBE score <60%: among 203 629 patients from the nine remaining articles,4 24 30 34 37 47 48 54 55 the risk of dyslipidemia remained increased with than without OA (OR 1.63, 1.13 to 2.36, p=0.009, I2=95%). Third, we excluded studies that specified the use of statin treatment because the definition of dyslipidemia in these studies was based on only lipid values and did not account for statin treatment. Among 41 539 patients from the 10 remaining articles,4 15 24 30 31 34 37 47 48 56 the risk of dyslipidemia remained increased with than without OA (overall OR 1.93 ,1.42 to 2.61, p<0.0001, I2=87%). Fourth, we pooled the results of the articles that reported an age-adjusted and BMI-adjusted OR. Among 31 764 patients, from the four articles,31 34 37 47 there was no association between dyslipidemia and OA (OR 1.31, 95% CI 0.88 to 1.95, p<0.0001, I2=83%).
Risk of dyslipidemia with OA: subgroup analyses
We performed a subgroup analysis by OA localisation. The increased risk of dyslipidemia with OA persisted with knee OA (among 26 805 patients, OR 2.27, 1.33 to 3.89, p=0003, I2=88%)15 24 30 31 34 37 and hand OA (among 814 patients, OR 2.12, 1.46 to 3.07, p<0.0001, I2=0%)22 47 but not hip OA (among 24 934 patients, OR 0.86, 0.69 to 1.08, p=0.18, I2=0%).34 37
Discussion
We investigated the potential association between OA and dyslipidemia with a systematic review and meta-analysis and found a 30% prevalence of dyslipidemia with OA, which seems much higher than in the non-OA population (8.0%). Furthermore, the meta-analysis revealed an increased risk of dyslipidemia, by 1.98, with than without OA and was observed with knee as well as hand OA.
The mean prevalence of dyslipidemia in hand OA was 37.6%±1.6%, much higher than the mean prevalence of 30.2%±0.6% with OA overall. Moreover, the risk of dyslipidemia was increased twofold with hand OA (OR 2.12, 95% CI 1.46 to 3.07). These results again confirm the systemic metabolic component of hand OA, as recently reported in the NEO study.58 The pathophysiological link between hand OA and MetS might be explained by the action of the adipose-tissue source of proinflammatory cytokines and the action of visceral fat.58
Hip OA, defined by joint replacement, was not associated with dyslipidemia possibly because of a selection bias of patients: cardiovascular comorbidities often associated with dyslipidemia might have restricted the indication for surgery due to the perioperative period. Furthermore, mechanical stress is more involved than metabolic stress in this joint.
For knee OA, the mean prevalence of dyslipidemia was 27.6%±1.4% and the association between knee OA and dyslipidemia was confirmed with increased risk of dyslipidemia (OR 2.27, 95% CI 1.33 to 3.89). The association between knee OA and MetS is sometimes conflicting. Han et al,27 Inoue et al,30 and Hussain et al37 did not find any positive association possibly because of different OA definitions. A recent study showed that the most important risk factor of knee OA was mechanical stress (before and after adjustment for metabolic factors), which limits the identification of a systemic metabolic component in knee OA.
Our meta-analysis has some limitations. The heterogeneity between studies was high, probably because of differences in OA localisations, definition of OA and dyslipidemia, statin therapy could not have been taken into account, and types and quality of studies. Dyslipidemia referred to lipid abnormalities such as hypercholesterolemia, low HDL level, high LDL level or hypertriglyceridemia. Because of the different definitions of dyslipidemia, we chose to define dyslipidemia first by high LDL level, then low HDL level, then hypercholesterolemia and hypertriglyceridemia. To counteract this heterogeneity, we performed sensitivity analyses to check whether the association between OA and dyslipidemia persisted after removing studies with poor methodology and found that the association persisted in all sensitivity analyses. Moreover, the heterogeneity of the studies was assessed by the I² index and we adapted the method to its value. The results of the meta-analysis are not modified by removing the most heterogeneous studies (data not shown). We were not able to integrate confounding factors such as age, BMI, HTA, smoking and physical activity in the overall statistical analysis. Obesity is a major risk factor of development and progression of OA. Obesity increases the risk of OA of the weightbearing joints due to excessive mechanical stress but is also associated with dyslipidemia in MetS.59 We identified seven articles accounting for confounding factors of dyslipidemia and OA: four showed a positive association after adjustment on age and BMI. However, when we meta-analysed the seven articles that reported an age-adjusted and BMI-adjusted OR, there was no association between dyslipidemia and OA, but raw data before adjustment on age and BMI are used. Finally, the impact of statin treatment could not be assessed because of the lack of data concerning its prescription. In fact, we have no details about statin use in dyslipidemic and non-dyslipidemic patients. However, Riddle et al did not find beneficial effect of statins on the structural progress at patients monitored for a knee osteoarthritis.60
In this funnel plot, the distribution of common values is not heterogeneous. Likewise, we can consider that there is no major publication bias in our meta-analysis.
We demonstrated an association between dyslipidemia and OA, but the pathophysiological explanation for the causal relationship has not been clearly defined. Experimental studies suggest the existence of lipid metabolism dysfunction in OA. Mice with altered HDL metabolism showed knee OA despite abnormal weight gain.61 Gierman et al showed that dietary cholesterol intake increased spontaneous cartilage damage in mice.62 High LDL levels promote synovial inflammation and ectopic bone formation in mouse OA models.63 Oxidised-LDL (oxLDL) could be involved in the development and progression of OA by stimulating synovial cells (macrophages, synovial fibroblasts and endothelial cells) and chondrocytes. A treatment strategy that lowers the level of oxLDL could be interesting.64
In conclusion, this is the first systematic review and meta-analysis demonstrating an association between OA and dyslipidemia, which illustrates the role of metabolic disturbances beyond glucose metabolism in OA pathophysiology. Such a study emphasises the need to screen and manage cardiovascular comorbidities in patients with OA in clinical practice.
Acknowledgments
Laura Smales (BioMed Editing, Toronto, Canada)
References
Footnotes
Twitter @Larhumato
Contributors PB, KL, FB and JS were involved in conception and design. PB and KL were involved in acquisition of data and statistical analysis. PB, KL, CM, FB and JS were involved in analyses and interpretation of data, drafting of the manuscript, revision of the manuscript and final approval, had full access to all the data in the study and take responsibility for the integrity of the data and the accuracy of data analysis.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement No additional data are available.