Article Text

Abstract
Early initiation of treatment in patients with inflammatory arthritis at risk of persistence and/or erosive progression is important because it is associated with a reduced rate of progression of joint damage and functional disability. It has been proposed that a window of opportunity exists, during which disease processes are less matured and disease modification can be more effective. The phase of arthralgia preceding clinical arthritis is likely to be an important part of this window of opportunity, during which treatment might prevent progression to clinical arthritis. Several proof-of-concept trials in individuals with arthralgia are now evaluating this hypothesis. Central to such trials is the ability to identify groups at high risk of rheumatoid arthritis (RA) in whom preventive treatment can be tested. This review describes the relevance of adequate prediction making, as well as the accuracy of different types of predictors (including imaging and serological markers) with their value in predicting the progression of arthralgia to arthritis. Despite promising results, studies have been performed in heterogeneous patient populations and most findings have not been validated in independent studies. Future observational or preventive studies should be conducted with homogeneous patient groups (eg, patients fulfilling the European League Against Rheumatism criteria for arthralgia at risk of RA) in order to increase interstudy comparability and to allow result validation.
- rheumatoid arthritis
- treatment
- disease activity
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Key messages
What is already known about this subject?
Adequate risk prediction in patients with arthralgia is crucial for the development of clinically meaningful preventive trials and for implementation of positive trial results.
What does this study add?
Predictors for progression to arthritis in arthralgia patients were reviewed; except for ACPA, none are replicated, which is partly due to heterogeneity in patient selection.
How might this impact on clinical practice?
Before using these predictors in prognostication, results should be validated and studied in homogeneous groups of patients with arthralgia.
The relevance of adequate prediction making
Research into the earliest phases of rheumatoid arthritis (RA) is important because early treatment is associated with better outcomes. To facilitate this research the European League Against Rheumatism (EULAR) study group of risk factors for RA has defined several stages of RA development: genetic risk factors for RA, environmental risk factors for RA, systemic autoimmunity associated with RA, symptoms without clinical arthritis and unclassified arthritis (UA).1 These stages are based on the presumed order in which different risk factors exert their effects. Individuals in the first three stages are generally asymptomatic. Over time symptoms may develop—initially often in the absence of clinically evident arthritis. In patients with established RA, the different phases may be identified retrospectively. However, it is clinically important to be able to predict with accuracy and confidence the future development of RA during its prearthritis stages. During recent years the phase of arthralgia has gained increasing interest as the risk of progression to RA is (in most cases) likely to be higher in symptomatic than in asymptomatic ‘at risk’ individuals. In addition, this is the way individuals typically present to medical care.
The phase of arthralgia is likely to be an important part of the so-called window of opportunity. Studies in patients with classified RA have revealed that an earlier start of treatment is associated with better outcomes.2 3 Because at presentation with clinical arthritis most patients will have a chronic disease, it is hypothesised that the period preceding clinical arthritis might be important. Within this prearthritis phase, disease processes might be less matured, making patients more susceptible to DMARDs. A review of murine studies suggested that DMARD initiation (eg, methotrexate and abatacept) prior to clinical arthritis was effective.4 Several ongoing proof-of-concept trials in individuals with arthralgia are evaluating the hypothesis that DMARD initiation can prevent progression to clinically evident arthritis. Results of two randomised controlled trials have been published; the first included 83 patients with anticitrullinated protein antibodies (ACPA)-positive and/or rheumatoid factor(RF)-positive arthralgia who were treated with dexamethasone or placebo, and the second included 82 patients with ACPA-positive and RF-positive arthralgia with C reactive protein (CRP) levels ≥3 mg/L and/or subclinical synovitis on ultrasound (US) or MRI of the hands, who were treated with a single infusion of rituximab or placebo.5 6 Although a decrease in ACPA levels and a delay in arthritis onset were reported, neither intervention prevented the development of RA. This failure to prevent RA development may indicate that (1) the hypothesis is false (ie, that the disease is not more modifiable in its arthralgia phase compared with its arthritis phase), or (2) the wrong drugs were tested, or (3) the studies included too few patients with a high risk of progression to RA, making it less easy to observe a preventive effect.
The importance of including patients with a high risk of progression to RA was illustrated in a recent post-hoc analysis of data from the Probable Rheumatoid Arthritis: Methotrexate versus Placebo Treatment (PROMPT) trial, in which patients with UA were treated with methotrexate with the aim of preventing progression to RA.7 The risk of progression to RA was ~30%, and without further stratification, methotrexate did not modify this risk. However when only patients with a high (>80%) 1-year predicted risk of progression to RA were evaluated, methotrexate was highly effective in preventing RA development. In addition, methotrexate was also associated with disease-modifying antirheumatic-drug (DMARD)-free remission in this high-risk group (36% vs 0% in the placebo group). Although these post-hoc analyses were based on small sample sizes, these data demonstrate the relevance of including patients with a sufficiently high risk in preventive trials. The results of ongoing proof-of-concept trials in arthralgia are awaited over the next decade.
Not all of the ongoing preventive trials have fulfilment of the 2010 classification criteria for RA as primary outcome. This is supported by the fact that the presence of persistent clinical arthritis or a clinical diagnosis of RA is an outcome that fits with daily clinical practice.
Before implementing potential positive findings of preventive trials in daily rheumatological practice, we need to know which patients with arthralgia would otherwise develop RA and should be offered treatment, and conversely which patients should be reassured that disease progression is unlikely (figure 1).

Adequate risk prediction is crucial for the design of informative preventive trials and for implementation of positive trial results.
Types of predictors
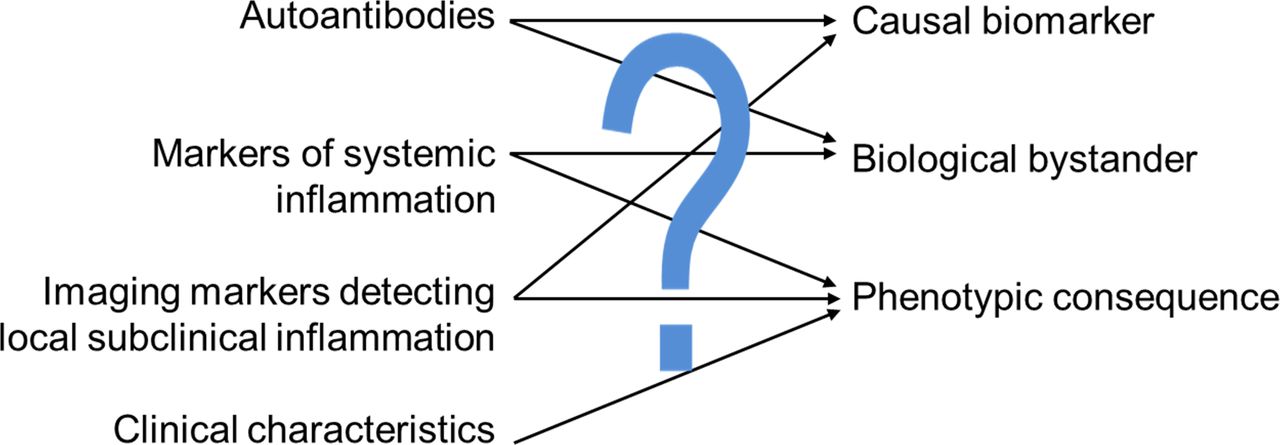
Optimally performing biomarkers are often causally related to the underlying biological process. Examples include the combination of increased free thyroxine (FT4) and decreased serum thyrotropin (TSH) levels, which are pathognomonic for hyperthyroidism, and the urinary human chorionic gonadotropin (HCG)-based pregnancy test, which is seldom negative in pregnant women and high HCG levels are rarely present in settings other than pregnancy. Predictors can also be bystanders, markers that are side products of the biological process but characteristic of the disease. Other predictors are phenotypic in nature (figure 2). RA has a complex aetiopathology and its development is not easily reflected by a single marker. The presence of ACPA within RA is strongly predictive of erosive progression and may be causally related to the development of bone erosions, but its role in the development of RA is unclear and its presence is not 1:1 related to disease development. Furthermore, it has become clear that in addition to RF and ACPA, several other autoantibodies are present in RA.8–10 These different sets of autoantibodies do not seem to relate to specific (sub)phenotypes of RA and may thus be considered as bystanders, although very useful in the diagnostic process.11 In the absence of pathognomonic markers, multiple biomarkers should be combined to predict which patients with arthralgia will progress to RA.

Predictors of rheumatoid arthritis development belong to different categories. A predictor of disease might directly reflect the underlying biological process, it can be a biological bystander of disease, or it might have no relation at all with the underlying biology and is a phenotypic marker.
Differentiating arthralgia suspicious for progression to RA from other arthralgias
Before reviewing the accuracy of different types of predictors, appreciation of the population studied is important. Arthralgia is a non-specific symptom and the biological nature of joint pain is diverse. Consequently, the risk to progress to RA is different for patients with arthralgia in different settings.
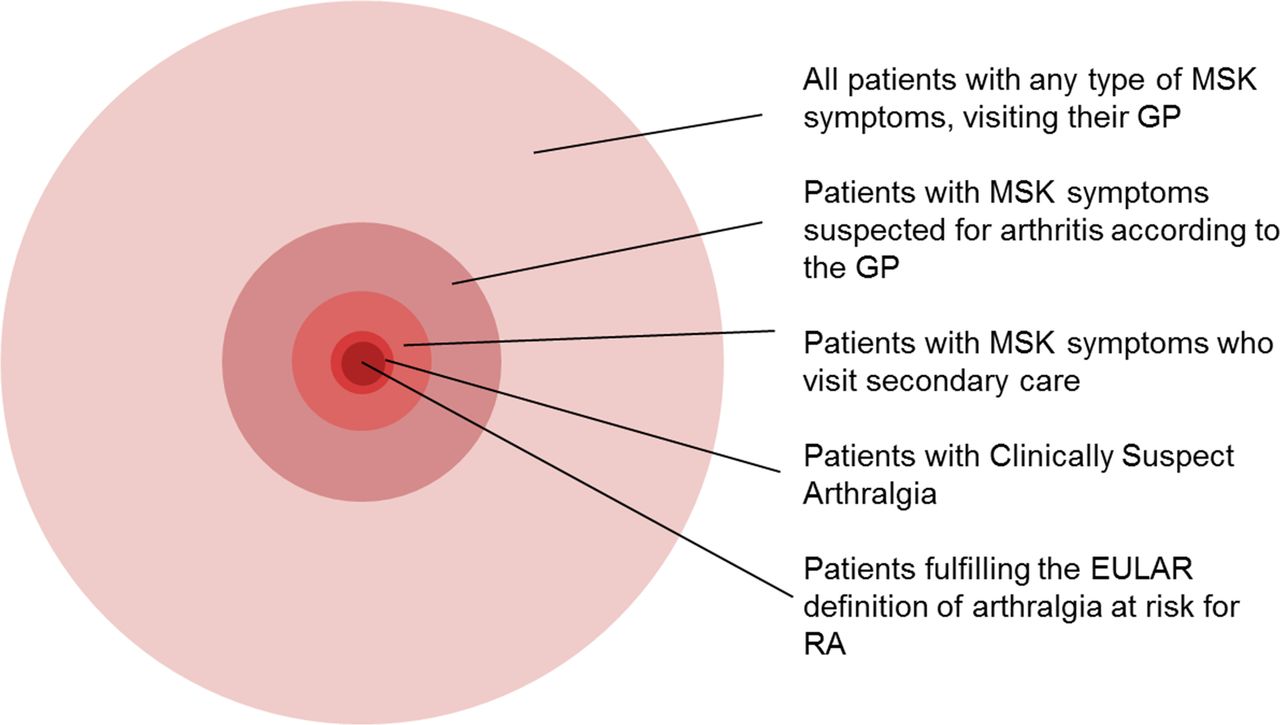
Musculoskeletal (MSK) symptoms are very prevalent in primary care.12 Primary care data from the Netherlands suggest an annual incidence of non-traumatic MSK symptoms of ~300/1000.13–15 In other words, almost one-third of the population visits the general practitioner (GP) at least once a year with an MSK symptom. The vast majority of these patients have explanations for their joint symptoms other than the beginning of a systemic inflammatory arthritis, and inflammatory arthritis is considered by GPs in only a minority of patients (figure 3). A separate Dutch GP study recorded an incidence of suspected arthritis of ~3/1000/year; most patients had a monoarthritis, and 60% had self-limiting symptoms.16 A small proportion of patients had suspected oligoarthritis or polyarthritis, and symptom persistence was more common in this group. These data support the notion that GPs are able to differentiate inflammatory from non-inflammatory cases of MSK symptoms and that the incidence of suspected inflammatory arthritis in primary care is low.

Clinical expertise of GPs and rheumatologists in differentiating patients with arthralgia. This figure is constructed based on the following references: The clinical expertise of GPs and rheumatologists is effective in differentiating patients with arthralgia; of all patients with MSK symptoms visiting their GPs (~300/1000/year13–15), only a small subset is suspected for arthritis (~3/1000/year).16 Of all patients with any MSK symptoms visiting secondary care (~8/1000/year53), only 7% were identified as CSA.17 The incidence of any MSK symptom in secondary care is higher than the incidence of patients with suspected arthritis in primary care, as GPs also refer patients with MSK symptoms in whom they did not suspect arthritis to be present. 74% of patients with CSA had a positive EULAR definition.19 CSA, clinically suspect arthralgia; GP, general practitioner; EULAR, European League Against Rheumatism; RA, rheumatoid arthritis; MSK, musculoskeletal symptoms.
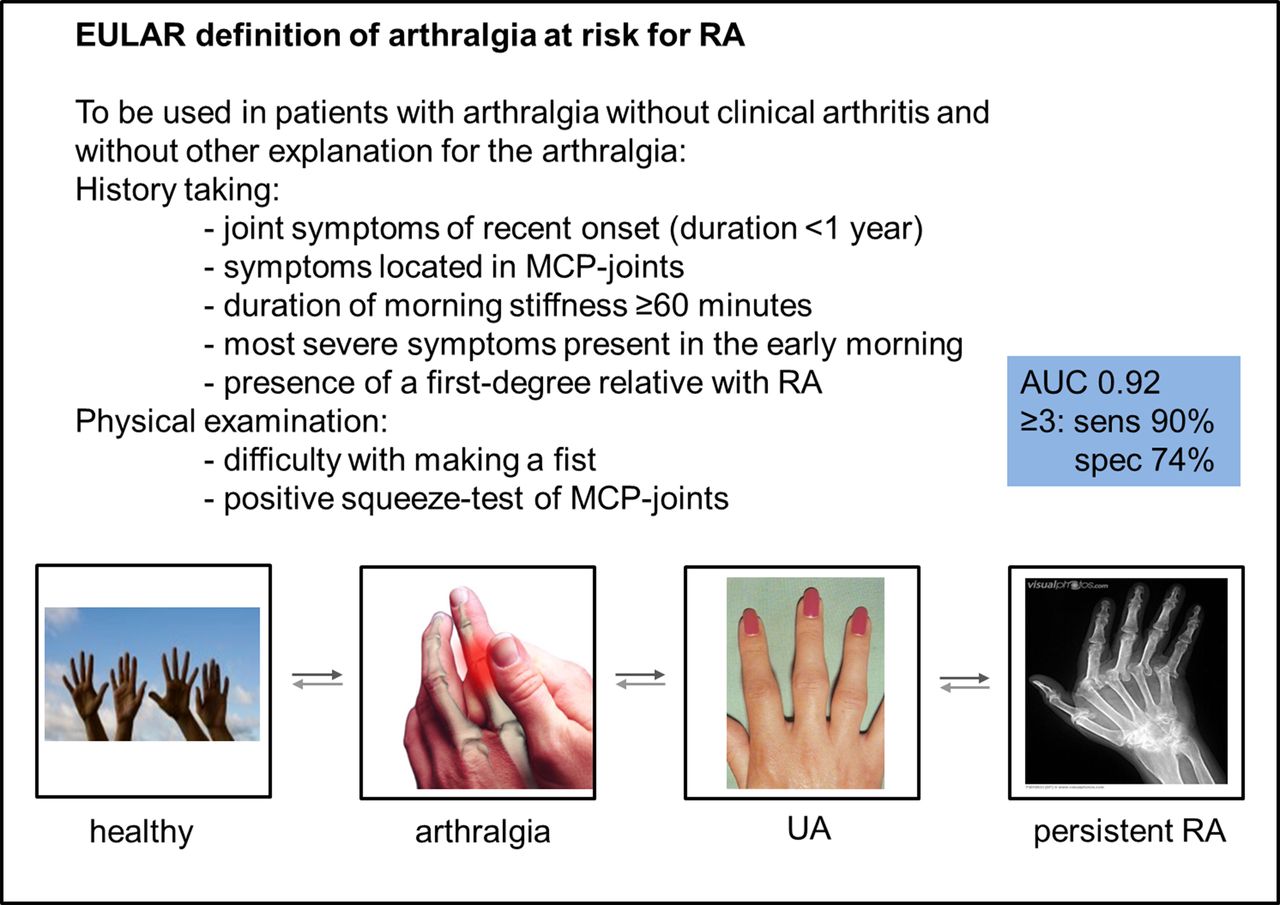
A similar observation has been made in secondary care. Most patients with arthralgia referred to rheumatologists have a diagnosis other than (imminent) RA. In addition, of patients presenting with arthralgia of uncertain cause, the large majority are not considered to be at risk of RA by their rheumatologists. A recent study revealed that only 7% of these patients with arthralgia were identified as clinically suspicious for progression to RA (clinically suspect arthralgia, CSA).17 Importantly, for patients with CSA, the odds for progression to RA were 55 times larger than the odds for patients with unexplained arthralgia. The rheumatologists’ clinical expertise had a high accuracy (93%), sensitivity (80%) and specificity (93%) for future RA. Although these data support the use of the rheumatologist’s clinical experience in identifying patients with arthralgia who are at risk of RA, a drawback is that this approach is subjective. This is a particular problem for research studies, where homogeneous groups of patients should be included. A EULAR task force has recently explicated this clinical expertise in clinical items that are measurable.18 The resulting EULAR definition of arthralgia suspicious for progression to RA consists of seven clinical items and can be used in patients with arthralgia in whom imminent RA is considered the most likely explanation for the symptoms (figure 4). The definition was validated in the rheumatological practices of 18 European rheumatologists (area under the curve: 0.92) with clinical expertise as the reference. The first longitudinal study of patients with CSA showed that the definition had a high sensitivity and served to further harmonise patients, as patients with arthralgia who were identified as CSA by their rheumatologist but had <3 clinical items indeed had a lower risk of progression to RA.19
{kind=link}
{kind=link}
{kind=link}
{kind=link}
EULAR-defined characteristics describing arthralgia at risk for RA. The reported AUC, sensitivity and specificity were calculated within newly presenting patients with CSA in outpatient clinics of European expert rheumatologists (who were part of the task force who defined arthralgia at risk for RA) with clinical expertise as reference.18 A sensitive definition requires the presence of at least three items and a specific definition requires the presence of at least four items. AUC, area under the curve; EULAR, European League Against Rheumatism; MCP, metacarpophalangeal; RA, rheumatoid arthritis; sens, sensitivity; spec, specificity; UA, undifferentiated arthritis.
Altogether, patients with arthralgia in secondary care who are considered as CSA and fulfil the EULAR definition of arthralgia represent a very small proportion of all individuals suffering from joint pain (figure 3). An optimised selection of patients with arthralgia will result in an increased risk of RA in the population, and—as a result of Bayes’ theorem—this will also result in higher post-test chances when performing additional tests, such as laboratory or imaging tests, in this subset of patients with arthralgia.
Search strategy
The accuracy of different types of laboratory or imaging markers for predicting RA development is reviewed below. With the assistance of a medical librarian, we searched in the medical literature databases PubMed, Embase (Ovid version), Web of Science and Cochrane Library up to June 2017. Central terms in our search strategy were arthralgia, arthritis, autoantibodies, serological markers and imaging. In total 145 references on autoantibodies, 117 on serological markers and 310 on imaging markers were extracted. Reference lists of the identified articles were hand-searched for additional articles. From the total list of references, we selected the studies on patients with arthralgia with a longitudinal cohort design.
The predictive accuracy of autoantibody testing in arthralgia
Nested case–control studies have shown that autoantibodies can be present years before the disease becomes manifest.20 21 Such studies use blood samples collected historically from patients known at the time of the study to have RA. Since, for patients presenting with arthralgia, it is relevant to know absolute risks for development of arthritis, this review focused on longitudinal studies. Most cohort studies that investigated the presence of autoantibodies have studied seropositive (ACPA and/or RF) patients in clinically ill-defined groups; one cohort study evaluated patients with CSA (table 1). In agreement with previous nested case–control studies, several longitudinal cohort studies have shown that the presence of ACPA associated with the development of clinical arthritis.22–26 The value of the level of ACPA (within ACPA-positive patients) in predicting arthritis development is unclear. While two studies, reporting on the same cohort, found an association between ACPA level and arthritis development,22 23 two other studies did not.26 27 Although these three cohorts selected ACPA-positive patients with arthralgia using different inclusion criteria (seropositive arthralgia, CSA or ACPA-positive persons with non-specific MSK symptoms) in different settings (primary and/or secondary care), the contrasting results are not yet explained. In addition to ACPA level, other ACPA characteristics have also been studied. The number of epitopes recognised by ACPA was associated with arthritis development in several studies in ACPA-positive patients with arthralgia.28–30 In addition, a decrease in galactosylation and an increase in core fucosylation of serum ACPA IgG1, indicating a change towards a more inflammatory phenotype of these autoantibodies, have been observed prior to the onset of RA.31
Autoantibodies in the preclinical phase of RA
The value of RF in the preclinical phase of RA has also been studied.22–24 26 32 Two studies, on the same cohort, performed stratified analyses and observed that within ACPA-positive patients, the additive presence of RF associated with arthritis development.22 23 These studies did not contain ACPA-negative patients; hence, no information could be provided on the single presence of RF. Two studies, on the same cohort, did contain an RF-negative group and showed in univariable analyses that the presence of RF conferred a higher risk of arthritis; however, after adjusting for the concomitant presence of ACPA, this association was lost.24 26 Therefore it remains to be determined if the single presence of RF in arthralgia is a true predictor, although one study suggested that high levels of RF are a predictor in contrast to low levels of RF.26
Finally the presence of anticarbamylated protein (anti-CarP) antibodies in the preclinical phase of RA was studied. One study in autoantibody-positive individuals observed an association between anti-CarP antibodies and the development of arthritis,33 whereas another study in patients with CSA did not observe an additive value of anti-CarP when ACPA and RF status is known.26
In conclusion, the presence of ACPA is associated with arthritis development while this is less clear for RF and anti-CarP antibodies. A disadvantage of most current studies is that patients are selected based on autoantibodies; thus, there is no autoantibody-negative reference group. In addition, as inclusion of patients in these cohorts was driven largely by ACPA positivity, these patients would not necessarily have been defined as CSA and would not necessarily have fulfilled the EULAR definition of arthralgia. Furthermore as noted above, some of the available data are based on analyses of the same patient cohorts (studies in table 1 reported on six cohorts). Finally, in clinical practice where patients present with arthralgia, it is important to estimate absolute risks for progression to arthritis, but many studies did not provide these risks. Studies that did determine positive predictive values (PPVs) observed that the PPV of ACPA (independent of RF) ranged between 16% and 50%.22 26 This broad range can be explained by differences in patient settings, since PPVs are dependent on the prior risks of arthritis development, which varied in the different settings that were studied.
The predictive accuracy of non-antibody serological markers in arthralgia
Various acute phase reactants, cytokines, chemokines and other systemic markers have been studied in the preclinical phase of RA (table 2). Results of studies evaluating CRP and erythrocyte sedimentation rate (ESR) are conflicting. Some studies have identified an association between CRP or ESR and arthritis development,24 31 while others have not.22 27 30 34–36 The only study showing an association between CRP level at study entry and development of arthritis included patients with CSA and did not select on the presence of autoantibodies.24 Studies that showed no predictive value of CRP were mostly conducted in autoantibody-positive arthralgia.22 27 30 34–36 This could imply that CRP has a predictive value in autoantibody-negative patients in particular; further studies are needed to clarify this.
Non-antibody serological markers in the preclinical phase of RA
Other serological markers have been assessed. In one study, differences were observed in the lipid profile of patients with and without progression to arthritis. After correction for ACPA, a lower apolipoprotein A1 level was associated with arthritis development.37 Another study evaluated 14-3-3η and showed that the PPV of 14-3-3η for arthritis development was 86%. However, when corrected for ACPA and RF, 14-3-3η did not predict onset of arthritis.38 Other serological biomarkers showed trends towards higher levels in patients with progression to arthritis.34 36 None of these markers was evaluated in other studies.
In conclusion, most results on serological markers of inflammation have not been validated in independent studies. Only CRP has been studied in several cohorts of patients with seropositive arthralgia and was shown to be of limited value.
The predictive accuracy of imaging markers detecting subclinical inflammation in arthralgia
Different imaging modalities (US, MRI, positron emission tomography and scintigraphy) have been used to study the presence of local subclinical inflammation24 27 29 32 35 39–46; most studies focused on US (table 3) or MRI (table 4).
Ultrasonography in the preclinical phase of RA
MRI in the preclinical phase of RA
Studies assessing the value of US have provided inconsistent results; some studies did not observe significant associations between US abnormalities and arthritis development,27 43 44 while others did.35 45 46 The studies that did not observe an association either included patients with seropositive arthralgia, ACPA-positive persons with non-specific MSK symptoms or patients with new-onset inflammatory arthralgia; studies that did observe an association included patients with arthralgia based on clinical characteristics, and differences in results might be partly explained by differences in patient selection. Furthermore, US protocols, joint regions assessed and US features reported on differed across the studies. It is also important to note that none of the studies have used a healthy reference population to define thresholds at which US findings should be classified as abnormal. Since a previous study has shown that US lesions (greyscale synovial effusion or synovitis with or without power Doppler signal) are also present in the majority (88%) of healthy volunteers, it might be important to correct for normal, physiological findings when defining a positive US.47 Finally, few studies have evaluated the predictive value of US abnormalities in relation to the presence of other predictors; therefore, the additive value of US abnormalities to regularly used biomarkers is unknown. Despite these shortcomings, the data obtained suggest that of the different US features, power Doppler signal might have the highest predictive value for the development of arthritis.45 46
Studies on the predictive value of MRI have been performed. Studies within autoantibody-positive non-specified arthralgia did not observe associations between MRI features at the knee (bone marrow oedema (BME) or synovitis) and progression to clinical arthritis.29 39 A small MRI study evaluating synovitis and BME in small joints of 28 patients with ACPA-positive arthralgia was also negative.40 However, larger studies in 150 patients with CSA revealed that MRI-detected inflammation was associated with progression to arthritis, independent of ACPA, CRP and clinical factors.24 41 Interestingly, in multivariable analyses, the effect size of MRI-detected inflammation was almost equal to that of ACPA (HR 5.1 for MRI and 6.4 for ACPA). MRI-detected tenosynovitis had a higher accuracy than synovitis or BME.24 Altogether subclinical inflammation identified by MRI is a predictor for RA development, when measured in small hand and feet joints, but not in knee joints (which may not be the location where synovitis begins in RA). As with US, age-matched symptom-free controls to define thresholds at which MRI features should be viewed as abnormal are lacking in most MRI-based studies. This may have affected the results as it has been recently shown that the predictive accuracy and specificity of a positive MRI increased when this was taken into account.48 Finally only one MRI study provided PPVs and observed that an abnormal MRI result (in patients with CSA) was associated with a risk for arthritis development during the next year of 31%.24
In conclusion, imaging studies in arthralgia have been conducted in different patient populations, evaluating different joints and different inflammatory features. None of the studies were independently replicated and none compared MRI and US in the same patients with arthralgia. Further studies using similar protocols in homogeneous patient groups are warranted.
Markers characterising immune cell dysfunction
It has been suggested that immune system dysregulation is an early feature of RA frequently preceding the onset of arthritis. Several markers have been studied. The number of regulatory T cells (Tregs) in the peripheral blood appeared not to be indicative of RA development in patients with seropositive arthralgia.30 In contrast, others showed that reduced naïve T cells and Tregs and increased inflammation-related cells were predictive of progression to arthritis in ACPA-positive persons with non-specific MSK symptoms.49 Seropositive patients who developed arthritis had a significantly decreased number of peripheral CD8+ T cells and memory B cells compared with non-converters.50 B cell subtypes have been studied; patients with seropositive arthralgia with a low B cell score, measured as expression of CD19, CD20, CD79α and CD79β, had an increased risk of arthritis if there was also a high type I interferon signature.51 B cell receptor (BCR) clones, defined as BCR clones expanded beyond 0.5% of the total repertoire, have also been studied in the peripheral blood of 71 seropositive individuals at risk of RA and were associated with an enhanced risk of arthritis.52
Unfortunately, most of the abovementioned studies did not address whether the novel markers added to the predictive utility of regularly used biomarkers and validation was lacking. In addition, most of the studied markers are not high-throughput available in daily clinical practice.
Conclusion
The processes causing arthralgia to progress to clinically evident RA are insufficiently understood. Most studied predictors are not pathognomonic for this transition or for RA, and the predictive accuracy of most markers has not been validated in different studies. Only ACPA positivity has been observed to associate with RA development across multiple studies. In addition none of the predictors studied, including ACPA, was sufficiently predictive on its own, and the vast majority of studies did not combine different types of predictors. The few studies that did combine different markers (eg, imaging and ACPA) revealed that combinations were also insufficient for adequate risk stratification in many patients (as PPVs were <80%).24 Therefore more research is needed to obtain adequate risk stratification in patients with arthralgia.
Ideally, future studies should be performed in homogeneous patient groups, for example, patients fulfilling the EULAR definition of arthralgia at risk for RA. In this way, patients with comparable prior risks for RA will be selected, and validation of findings in different cohorts will be possible. Results of these future studies should provide data to support the development of robust algorithms to differentiate patients with arthralgia likely to progress to RA from those unlikely to do so. Importantly the variables within these algorithms and their weightings may well be different for algorithms designed for use in different contexts, for example, primary and secondary care.
Acknowledgments
The authors like to thank JW Schoones, medical librarian of the Leiden University Medical Center, for his help with the literature search.
References
Footnotes
Contributors All authors contributed equally to the content of the paper.
Funding This work was supported by a Vidi grant from the Netherlands Organisation for Scientific Research and European Research Council (ERC Starting Grant) and the Arthritis Research UK Rheumatoid Arthritis Pathogenesis Centre of Excellence. The funding sources had no role in the writing of the manuscript.
Competing interests None declared.
Provenance and peer review Commissioned; externally peer reviewed.
Data sharing statement No additional data ara available.