Article Text

Abstract
Background Rheumatoid arthritis (RA) treatment includes the use of the anti-CD20 monoclonal antibody rituximab (RTX). RTX acts through Fcγ-receptors (FCGR) on effector natural killer cells and macrophages and it can be administered effectively in RA and in lymphomas. Based on the results of in vitro experiments, its efficacy may depend of FCGR gene polymorphisms in both diseases.
Aim As genetic background of diseases and therapeutic efficacy (pharmacogenetics) may vary among different geographical regions, we wished to assess possible relationships between FCGR3A polymorphism and the therapeutic outcome of RTX therapy in a Hungarian RA cohort.
Patients and methods Altogether, 52 patients, 6 men and 46 women, were included in the study. Peripheral blood samples were used to determine FCGR3A polymorphism by genotyping using real-time PCR method.
Results The distribution of FCGR3A genotypes was 8 VV, 34 VF and 10 FF. Disease activity score 28 (DAS28) reductions in patients with VV, VF and FF genotypes were 1.98±0.54 (p=0.008 between DAS28 before and after treatment), 2.07±0.23 (p<0.001) and 1.59±0.52 (p=0.014), respectively. Significant differences in DAS28 reductions on treatment were found between VF heterozygotes and FF homozygotes (p=0.032), as well as between heterozygotes and all (VV+FF) homozygotes (p=0.017). Furthermore, significantly more VV (62.5%; p=0.030) and VF (64.7%; p=0.015) patients achieved low disease activity compared with FF subjects (30.0%).
Conclusion Our results suggest that FCGR3A polymorphism may predict more effective disease activity reduction by RTX. Furthermore, carrying the V allele may also be associated with better therapeutic response in Hungarian patients with RA.
- rheumatoid arthritis
- dmards (biologic)
- pharmacogenetics
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Key messages
FCGR3A polymorphism has been associated with response to rituximab therapy in rheumatoid arthritis (RA) and in non-Hodgkin’s lymphomas.
Significant differences in disease activity score 28 reductions on treatment were found between VF heterozygotes and FF homozygotes, as well as between heterozygotes and all (VV+FF) homozygotes.
Carrying V allele leads to more effective therapy also in Hungarian patients with RA.
Determination of FCGR3A polymorphism in the future can help to select an effective therapy in RA.
Introduction
Rheumatoid arthritis (RA) is an autoimmune-inflammatory rheumatic disease, which primarily affects the joints causing erosive or non-erosive arthritis. Genetic factors including human leucocyte antigen (HLA) and non-HLA genes have been implicated in both the pathogenesis and outcome of the disease. Early diagnosis and adequate treatment is necessary to prevent joint destruction and disability. Because of differences in pharmacogenetics and other outcome markers, patients respond to conventional and biologic disease-modifying antirheumatic drugs (DMARDs) in different ways. Biologics used in the treatment of RA include tumour necrosis factor (TNF)-α, interleukin (IL)-1 and IL-6 receptor antagonists, B-cell depleting anti-CD20 antibody (rituximab (RTX)) and T-cell costimulation inhibitor.1–4 Due to genetic heterogeneity, personalised treatment may be necessary.
Pharmacogenetics and pharmacogenomics deal with the associations of single nucleotide polymorphisms (SNP) and genomic signatures with the therapeutic efficacy of antirheumatic drugs, respectively. Therapeutic response may depend on genetic, as well as clinical, immunological and environmental factors.1 5–9
RTX is a commonly used chimeric anti-CD20 monoclonal antibody, which is highly effective in RA, as well as haematological malignancies. RTX acts on Fc-γ receptors (FcγR) expressed by mononuclear cells. After RTX binding, B-cells are eliminated through several mechanisms, such as complement-dependent or antibody-dependent cytotoxicity, as well as phagocytosis. A SNP in the FcγRIIIA gene (FCGR3A) can modify the structure of this receptor influencing the binding of antibody to the receptor. Because of structural changes, the effect of RTX may be altered.10–14 This SNP in the FCGR3A gene encoding FcγRIIIA at position 158 leads to an amino acid change from Val to Phe resulting in weaker binding of biological drugs. Carrying one or two copies of V allele can result in better response to RTX therapy in RA and non-Hodgkin’s lymphomas.15 16 As pharmacogenetics may exert geographical differences, we wished to assess possible associations between FCGR3A genotypes and responses to RTX in the first Hungarian RA cohort.
Patients and methods
Patient clinical data
Clinical data of patients with RA were reviewed with reference to sex, reduction of disease activity score 28 (DAS28), therapeutic response and remission. Altogether, 52 patients (6 men and 46 women) were involved in the study. All patients were treated with RTX according to standard protocol (2×1000 mg RTX intravenous 2 weeks apart). Therapeutic response was assessed by the European League Against Rheumatism (EULAR) response criteria after 6 months of the first RTX infusion. Low disease activity (LDA) and remission were defined as DAS28 <3.2 and DAS28 <2.6, respectively.
Altogether, 46 female and 6 male patients were included in the study. The mean age at the time of diagnosis was 57.46±9.72 years. The mean disease duration was 18.76±14.03 years. We administered two or more different DMARDs including one TNF inhibitor before RTX. Corticosteroids were administered to 82% of patients. RTX was combined with methotrexate (MTX) or other traditional DMARDs in all patients. Thirty-four patients (65%) were anti-citrullinated protein antibodies (ACPA) and 36 patients (70%) were rheumatoid factor (RF) seropositive (table 1).
Baseline characteristics of patients with rheumatoid arthritis
Informed consent was obtained from all patients according to the Declaration of Helsinki.
Determination of FCGR3A polymorphisms
High molecular weight DNA for genotyping was extracted from peripheral blood samples using a QiaAmp DNA Blood Mini Kit (Qiagen GmbH, Germany). DNA was quantitated by UV absorption at 260 and 280 nm. Genotyping was employed using a real-time PCR method. Genotyping of the single nucleotide substitutions were carried out using the allelic discrimination assay. PCR primers and TaqMan probe specific for the polymorphisms (rs 396991) were purchased from Applied Biosystems (Foster City, California, USA). Real-time PCR was performed in a Corbett Rotor-Gene RG-3000 equipment, which was set to detect FAM and VIC reporter dye simultaneously. The PCR reaction was carried out in a 20 µL reaction volume containing TaqMan Universal Master Mix, TaqMan genotyping Assay and optimised quantities of genomic DNA. The Universal Master Mix contained AmpliTaq Gold DNA Polymerase, AmpErase UNG, dNTPs with dUTP, passive reference and optimised buffer components. Reactions were set up in duplicate. Thermal cycling was initiated by incubation at 95°C for 10 mins for optimal AmpErase UNG activity and activation of AmpliTaq Gold DNA polymerase. After this initial step, 40 cycles of PCR were performed. Each PCR cycle consisted of heating to 92°C for 15 s for melting, and to 60°C for 1 min for annealing and extension.
Statistical analysis
The statistical analysis was processed with IBM SPSS V.22 software. Descriptive statistical analysis was used to characterise the patient populations. Normality of the parameters were determined applying the Kolmogorov-Smirnov test. Differences between DAS28 levels before and after treatment were examined using paired t-test. The relationship between therapy and genetics was measured by Fisher’s exact test. The strength of associations between genotype and effect of therapy were measured by OR with 95% CI. Differences were significant if probability level was <5% (p<0.05). Genotypes were in Hardy-Weinberg equilibrium.
Results
Out of the 52 RTX-treated patients, 36 (69.2%) were EULAR responders, 17 (32.7%) reached remission and 29 (55.8%) reached at least LDA. The mean DAS28 at baseline was 5.16±1.22, after treatment 3.23±1.29. The mean DAS28 reduction was 1.93±1.42.
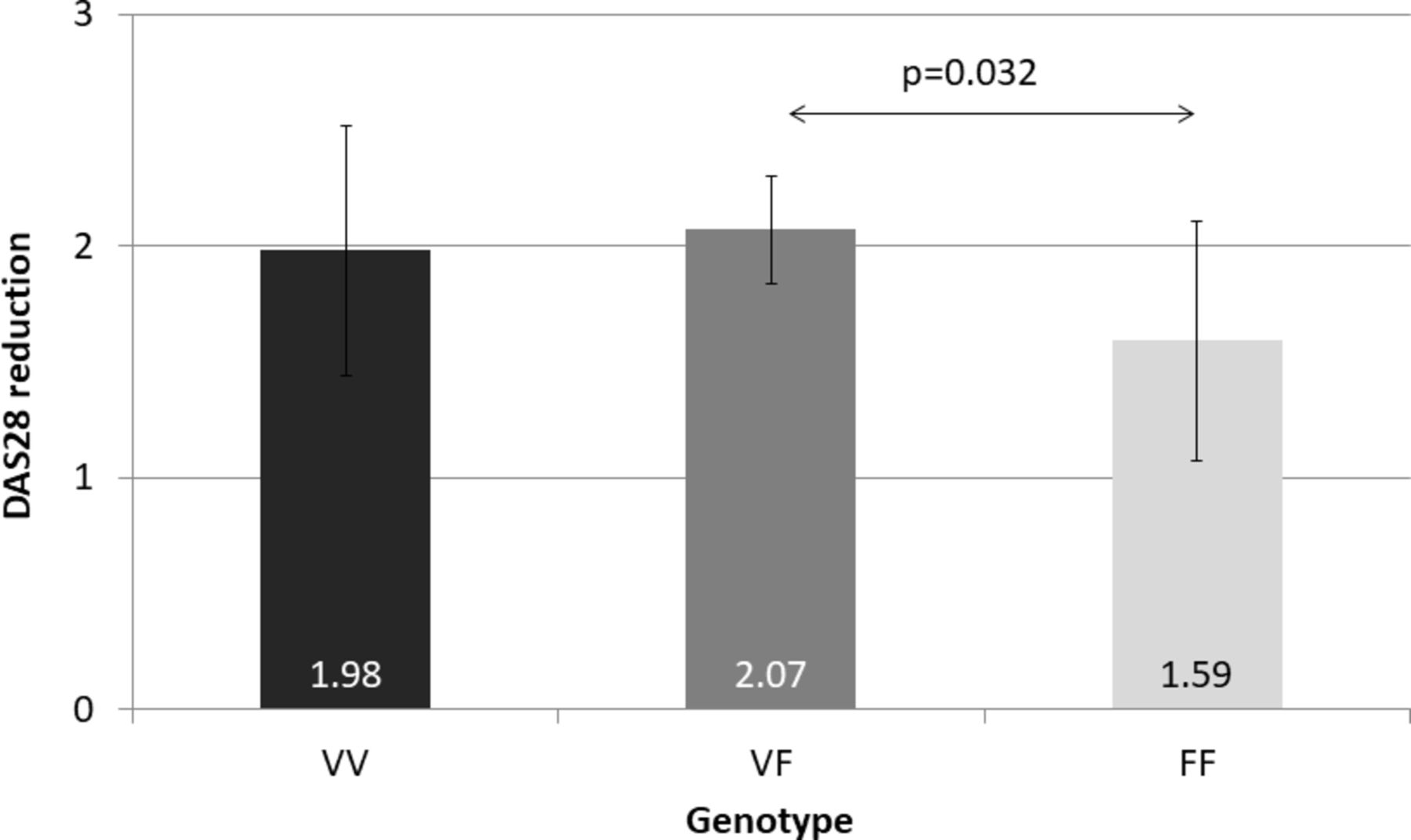
The distribution of FCGR3A genotypes was as follows: 8 (15.4%) patients had VV, 34 (65.4%) had VF and 10 had (19.2%) FF genotype (table 2). Patients with all three genotypes had significant reduction in DAS28. DAS reductions in patients with VV, VF and FF genotypes were 1.98±0.54 (p=0.008 between DAS28 before and after treatment), 2.07±0.23 (p<0.001) and 1.59±0.52 (p=0.014), respectively. At baseline, there was no significant difference in the mean DAS28 in the VV, VF and FF subsets. With respect to changes in DAS28 on RTX treatment, significant difference was found between the VF and FF group (p=0.032). There was no difference in DAS28 reduction between VV versus VF or VV versus FF. Patients carrying at least one V (VV+VF) or F (VF+FF) allele did not differ from each other. On the other hand, there were significant differences in DAS28 reductions on treatment between VF heterozygotes and FF homozygotes (p=0.032) (figure 1), as well as between heterozygotes and all (VV+FF) homozygotes (p=0.017). We did not find any significant differences in DAS28 reduction between VV homozygotes and VF heterozygotes and between VV and FF homozygotes.
The effect of FCGR3A genotypes on EULAR response, low disease activity and complete remission
{kind=link}
Disease activity score 28 (DAS28) reduction in different genotypical groups before and after therapy.
With respect to clinical responses (EULAR response, LDA, remission), patients in the VV, VF and FF subset exerted similar EULAR responses (60%–73%) and remission rates (30%–37.5%) without major differences. In contrast, significantly higher proportion of VV (62.5%; p=0.030) and VF patients (64.7%; p=0.015) achieved LDA compared with FF patients (30.0%) (table 1).
Discussion
Biological DMARDs mean a therapeutic milestone in the treatment of RA. RTX, an anti-CD20 monoclonal antibody, acts through Fcγ receptors. FCGR3A polymorphism has been associated with response to RTX therapy in RA and in non-Hodgkin’s lymphomas. Carrying one or two V alleles would lead to better treatment response.13 15 16 A meta-analysis showed that the association of FCGRA3A-158VV homozygosity with RA is sex-dependent.13
In our study, significant differences in DAS28 reductions on treatment were found between VF heterozygotes and FF homozygotes, as well as between heterozygotes and all (VV+FF) homozygotes. In another study, FCGR3A-F158V heterozygosity also indicated a better response rate to RTX therapy.13 In addition, significantly higher proportion of patients with RA with VV or VF genotype achieved LDA than did FF homozygotes. In terms of therapeutic response and low disease activity, heterozygous patients could achieve better responses. Altogether, 37.5% of VV homozygous patients, 32.4% of VF heterozygous patients and 30% of FF homozygous patients achieved complete remission, but the differences were not significant. In another study, RTX and TNF-α inhibitors were assessed in relation to FCGR3A polymorphism and they could not found significant differences in treatment responses to RTX compared with TNF inhibitors.17 In contrast to our results, Italian investigators reported better response rates to RTX in VV homozygous patients.18 VV homozygous patients showed better response rates to RTX in RA and in hepatitis C virus (HCV)-related cryoglobulinemia.19
Thus, our data suggest that indeed, carrying one or two V alleles may lead to better treatment response. Gender did not influence the efficacy of therapy as we could not find any significant difference in the effect of VV and VF genotypes between females and males. The reason for the difference between the different genotypical subsets is mostly functional. The V158 isoform can bind IgG with higher affinity than F158 isoform.16 Thus, the presence of the V allele can confirm capture of IgG-opsonised pathogens or immune complexes and lead to more effective antigen presentation in comparison to the F allele.16 20 Furthermore, carrying V allele leads to more effective peripheral B-cell depletion.16 20 The variability of response rates may also be the consequence of different expression levels of FcyRIIIa.20 21 However, we have not studied protein expression. Low expression level of FcyRIIIa results in diminished RTX efficacy.21 All the above-mentioned mechanisms may be associated with the efficacy of RTX in Hungarian, as well as other patients with RA. The major limitation of the study is the low patients number, which results in lack of statistical power to show any association between response to RTX and VV homozygosity.
Acknowledgments
None
References
Footnotes
Contributors IP performed the experiments and drafted the manuscript. SS and ZS performed data analysis, revised manuscript. KH performed data analysis and statistics. LV supervised the work, drafted the protocol and read the manuscript.
Funding The work was supported by the European Union and the State of Hungary co-financed by the European Social Fund in the framework of TAMOP-4.2.4.A/2-11/1-2012-0001 ‘National Excellence Program’ (ZS); also by the European Union grant GINOP-2.3.2-15-2016-00015 (ZS).
Competing interests None declared.
Patient consent Obtained.
Ethics approval The study protocol was approved by the Institutional Review Board of University of Debrecen.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement The corresponding author can be contacted regarding additional data.