Article Text

Abstract
Objective This study was designed to evaluate the determinants of patient and physician global assessments (PtGA and MDGA, respectively) of disease activity, their discordance and change over 2 years in Hispanics with rheumatoid arthritis (RA). We further examined the impact of discordance and its persistence on health-related quality of life (HRQOL) and work productivity on final visit.
Methods We studied 536 Hispanics with established RA from a single centre. PtGA and MDGA were measured annually on 10 cm visual analogue scales and discordance was defined as absolute difference between them ≥3 cm. Associations between predictors and outcomes of interest were evaluated using multivariable regression and analysis of covariance for cross-sectional and longitudinal data, respectively.
Results Independent predictors of baseline PtGA were pain, fatigue, depression, general health perceptions and tender joint count. MDGA was predicted by swollen joint count, tender joint count, erythrocyte sedimentation rate, fatigue and depression. Both PtGA and MDGA improved over time (all p<0.001). Discordance was observed in 43% at baseline, with fair stability over 2 years. Higher (worse) patient ratings were most prevalent; their presence at any time and increasing persistence predicted lower physical and mental HRQOL, decreased work productivity and more activity impairment at 2-year follow-up (all p<0.001).
Conclusions Determinants of PtGA, MDGA and changes over 2 years were disparate in Hispanics with RA yielding significant discordance. Higher patient ratings at any time contributed to worse HRQOL, work productivity and activity impairment on final visit.
- rheumatoid arthritis
- disease activity
- patient rerspective
- outcomes research
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Key messages
What is already known about this subject?
Changes in patient and physician global assessments, discordance over time and predictors thereof are of significant interest yet underexplored. The impact of discordance on health-related quality of life (HRQOL) outcomes is unknown, especially for racial and ethnic minority populations.
What does this study add?
Determinants of patient and physician assessments of rheumatoid arthritis activity and their change are disparate in Hispanics in the USA, yielding significant discordance.
Worse patient ratings (positive discordance (PD)) at any time, and their persistence, yielded worse physical and mental HRQoL, inferior work productivity and greater activity impairment at final visit.
PD may be a patient-specific rather than a visit-related characteristic; patients with PD are more likely to have fibromyalgia and articular destruction.
How might this impact on clinical practice?
Physicians should promptly reconsider the patient perspective in individuals with PD; interventions aiming at reducing such discordance might improve outcomes.
Introduction
The primary goal of treatment in rheumatoid arthritis (RA) is to maximise long-term health-related quality of life (HRQOL). This objective is best achieved by treating to a target of disease remission.1 Both patient and physician global assessments (PtGA and MDGA, respectively) of disease activity constitute integral components of remission definitions.2 Patients report higher disease activity more frequently than physicians.3 4 Higher PtGA scores may preclude patients from being classified in remission5; moreover, they contribute to dissatisfaction, decreased adherence with treatment and impaired work productivity.6–8
Changes in PtGA and MDGA,9 10 discordance over time8 9 11 and predictors thereof are of significant interest yet underexplored. Importantly, the impact of discordance on HRQOL outcomes is unknown.12 This is especially true for racial and ethnic minority populations, immigrants and socioeconomically disadvantaged patients. In the USA, Hispanics represent the most rapidly expanding sector of the population.13 Arthritis-attributable burden appears higher in Hispanics compared with non-Hispanic whites,14 and Hispanics with RA score worse in all self-report measures compared with non-Hispanic whites or African Americans despite similar physician assessments,15–17 and regardless of achieving therapeutic targets.18 Hispanics with limited English proficiency, in particular, report worse self-rated health compared with patients from other ethnic backgrounds.19
Treatment goals and the therapeutic landscape in RA have significantly evolved over the past two decades, and patients are acknowledged as equal partners in therapeutic decision making. It is, therefore, important to identify the prevalence and predictors of discrepant disease assessments over time, as well as their effects on HRQOL and work productivity in a large contemporary cohort of Hispanics with RA.
The present research was conducted in Los Angeles, California, where 48% of residents are Hispanic, with a 28% increase between 2000 and 2010 compared with 1.5% in non-Hispanics.13 Our study had two main objectives: (1) to identify determinants of PtGA, MDGA, discordance and changes over 2 years in Hispanics with RA; and (2) to explore associations among discordance and measures of HRQOL, work productivity and activity impairment after 2 years of follow-up.
Methods
Participants and procedures
The sample included participants enrolled in the Harbor-UCLA prospective observational RA cohort16 between 2012 and 2016. Harbor-UCLA Medical Centre is a large county hospital that provides comprehensive healthcare primarily to Latino patients, the majority of whom are monolingual Spanish-speaking, first-generation immigrants from Mexico and Central America. Patients were included in the study if they self-identified as ‘Hispanic’ or ‘Latino’ in a hospital registration form, were ≥18 years old and fulfilled 2010 American College of Rheumatology (ACR) criteria for RA.20 Patients with overlapping autoimmune syndromes or comorbid conditions that could confound RA treatments (including chronic infections, advanced or decompensated heart failure, class II chronic kidney disease or above, cancer within 5 years) or at risk for suicide were excluded. Patients were recruited consecutively during routine clinic visits (<1% of eligible patients declined participation) and followed-up annually according to a standard protocol. The first visit with complete data available on all predictors and outcomes of interest in this study was selected as baseline visit. In the vast majority of patients, the designated baseline visit was not the initial disease-associated visit.
At each visit, participants completed self-report questionnaires in Spanish administered by a native proficiency Spanish-speaking study coordinator and then received a physical examination by a board-certified rheumatologist with professional working proficiency in Spanish and laboratory evaluation. All participants provided written informed consent in compliance with the Helsinki Declaration and this research has been approved by the Harbor-UCLA Institutional Review Board.
Predictor variables
Demographics, rheumatoid factor and anticyclic citrullinated peptide antibody status were obtained via chart review. Use of prednisone, synthetic disease-modifying antirheumatic drugs (DMARDs) and biologic DMARDs were assessed at each visit. Presence of erosions, irreversible articular damage (IAD; defined as subluxation, fusion/fixed deformities, arthrodesis or prosthesis) and fibromyalgia21 were also recorded. Disease activity assessment was based on 28 joint counts for tenderness (TJC) and swelling (SJC) and erythrocyte sedimentation rate (ESR).
Physical impairment was evaluated using the Health Assessment Questionnaire Disability Index (HAQ-DI).22 The nine-item Patient Health Questionnaire (PHQ-9)23 24 assessed depressive symptoms (range 0–27). Pain and fatigue were both measured using 10 cm visual analogue scales (VAS) spanning from 0 (best status) to 10 (worst status). The Short-Form Health Survey25 general health (GH) domain assessed self-evaluated health status (range 0–100, higher scores indicate greater perceived health).
Outcomes
Our primary outcomes were PtGA and MDGA. Both were assessed on separate 10 cm VAS anchored by ‘very good’ or ‘no activity’ on the left and ‘very bad’ or ‘high activity’ on the right, respectively. Prior to their visit, patients were asked ‘Considering all of the ways your arthritis has affected you, how do you feel your arthritis is today?’ After the visit, the examining physician (blinded to the patient’s rating) recorded their MDGA based on history, physical examination and available laboratory tests. Participants were classified into one of three groups based on subtracting MDGA from PtGA (PtGA−MDGA)3: patients with concordant ratings (PtGA and MDGA within ±3 cm); those with higher patient ratings or positive discordance (PD; PtGA−MDGA ≥3 cm); and those with higher physician ratings or negative discordance (ND; PtGA−MDGA ≤−3 cm).
Secondary outcomes included HRQOL measured using the 12-item Short-Form Health Survey (SF-12) physical and mental component summary (PCS and MCS, respectively) scores (each standardised to a mean of 50; higher scores indicate better HRQOL).26 In addition, the Work Productivity and Activity Impairment Questionnaire27 evaluated activity impairment due to RA, as well as percentage of work productivity loss, reduced productivity at work (presenteeism) and work time missed (absenteeism).
Statistical analysis
Descriptive statistics are presented as frequencies and percentages for categorical variables and means and SD for continuous variables. Analysis of variance (ANOVA) or χ2 analyses assessed baseline differences between discordance groups. To examine predictors of baseline PtGA and MDGA, correlation analyses identified the best set of candidate variables for each outcome and significant bivariate predictors were entered in separate backward linear regression models. Predictor importance was determined using relative weight (RW) analysis.28 RWs indicate the contribution of each predictor in a model to the total variance explained (sum to R2) after accounting for the effects of intercorrelations among variables.29 Predictors of baseline discordance were also assessed. Variables significantly discriminating between discordance groups were evaluated in a multinomial logistic regression model to identify predictors independently associated with classification in the PD or ND groups (compared with the concordant).
Repeated-measures ANOVA assessed change in PtGA, MDGA and discordance over time. Linear mixed models explored longitudinal associations between predictors of interest and PtGA and MDGA. Initial models contained fixed-effects terms for SJC, TJC, ESR, pain, fatigue, PHQ-9, HAQ-DI and GH domain score. Parameter estimates were derived from the solution for fixed effects in the final reduced model. Impact of the presence of PD and its increasing persistence (at zero, one, two or all three study time points) on HRQOL, activity impairment and employment-related outcomes at 2 years was assessed using analysis of covariance, adjusting for baseline values of those outcomes. Given the potential bias introduced by baseline adjustment in observational studies,30 we performed sensitivity analyses and found no inflation of parameter estimates compared with models without baseline adjustment. Analyses were performed using SPSS V.21 (IBM Corp, USA). Global level of significance was p<0.05 for all analyses, with Benjamini-Hochberg adjusted p values for multiple comparisons.31
Results
Of the 653 patients with at least one visit during the study time frame, these analyses include data from 536 patients with complete data for all variables of interest (table 1).
Baseline characteristics of patients according to concordant/discordant groups*
The sample was primarily female with established, seropositive, erosive disease. Concordant assessments were seen in 308 (57%) cases at baseline; PD was observed in 168 (31.3%), whereas ND was reported in 63 (11.7%).
Determinants of PtGA, MDGA and concordance/discordance at baseline
Mean scores were 4.34±2.81 for PtGA and 3.07±3.14 for MDGA at baseline. Lin’s concordance coefficient was 0.31 (95% CI 0.24 to 0.38), indicating low–moderate agreement. Significant predictors of PtGA and MDGA are shown in table 2.
Multivariable predictors of baseline PtGA and MDGA
Our models explained 71% and 87% of variance in PtGA and MDGA, respectively. The most important predictor of PtGA was pain (27%), followed by fatigue (15%), PHQ-9 (9%), HAQ-DI (8%), GH (7%) and TJC (6%). MDGA was primarily predicted by SJC (44%) and TJC (31%); additional determinants were ESR (6%), fatigue, PHQ-9 and age.
Baseline SJC, TJC and ESR were lowest for patients with PD and highest among those with ND (table 1). In contrast, the PD group reported the highest average scores for HAQ-DI, pain, PHQ-9, fatigue and worst (lowest) GH. In a multinomial logistic regression model (with the concordant group as referent), higher pain, fatigue, HAQ-DI, worse GH and lower TJC and SJC independently predicted classification in the PD group (table 3). Patients with higher TJC and SJC and lower pain and PHQ-9 were more likely to have ND.
Multivariable predictors of baseline discordance*
Change in PtGA, MDGA and discordance over time
Complete data for three visits (baseline, 1 year and 2 years later) were available for 308 patients and used in longitudinal analyses. As shown in figure 1, PtGA improved across three visits, F(1.96, 602.34)=9.54, p<0.001; improvement was associated with commensurate declines in pain, physical impairment, fatigue, depression, TJC and recovery in GH (table 4). MDGA also improved over time, F(1.88, 577.16)=19.55, p<0.001 (figure 1). Its improvement reflected decreases in SJC, TJC, fatigue and ESR.
Mixed model of predictors of PtGA and MDGA over three visits
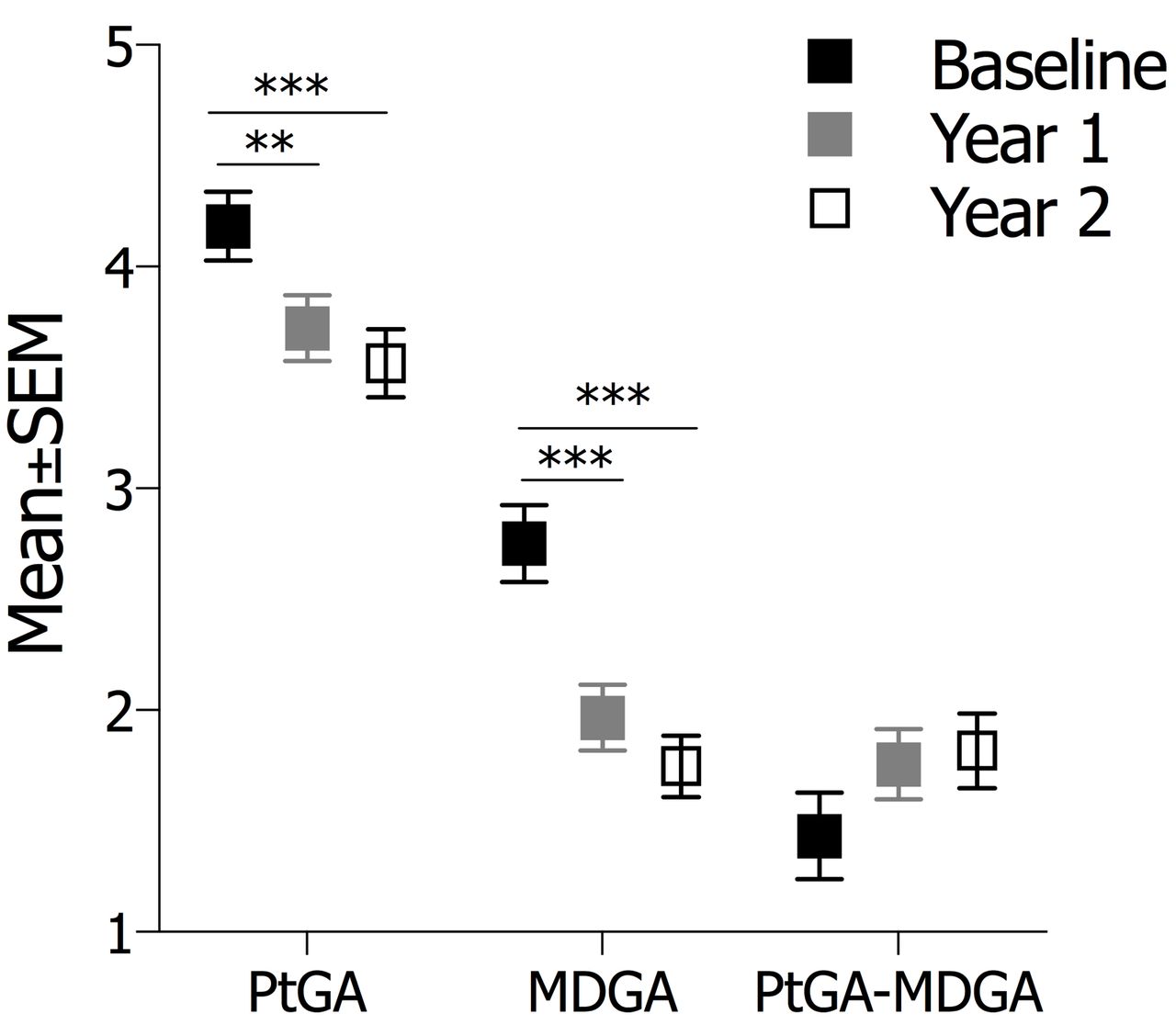
PtGA, MDGA and PtGA–MDGA discordance trends over time. p Values for pairwise comparisons are Benjamini-Hochberg adjusted. **p<0.01, ***p<0.001. PtGA, patient global assessment; MDGA, physician global assessment.
While both PtGA and MDGA decreased over time, mean discordance tended to increase: F(1.97, 605.17)=2.48, p=0.086 (figure 1). Agreement status in patient–physician evaluations longitudinally is shown in online supplementary figure S1. Weighted kappa (κ) coefficients for congruence of discordance category (negative, concordant, positive) across two consecutive visits indicated fair stability over time (κ range 0.26 to 0.31). PD was most prevalent and more stable over time; 85 (27.6%) subjects had PD once, 49 (15.9%) had PD twice and 45 (14.6%) at all three time points. ND was far less stable; 45 (14.6%) patients had ND once, 10 (3.3%) twice and one (0.3%) at all three time points.
Supplementary file 1
Clinical significance of PD and its persistence over time
Presence of any PD throughout the study adversely impacted HRQOL on last visit. Persistence of PD over several time points yielded progressively lower SF-12 PCS scores (figure 2A, p<0.001) and SF-12 MCS scores were lower among patients with any PD compared with those without (figure 2B, p<0.001). Increasing persistence of PD contributed to greater activity impairment at final visit (figure 2C, p<0.001). Furthermore, PD was negatively associated with employment status (p=0.025) (figure 2D). Among patients employed at baseline and 2-year follow-up (n=63), those with PD at one or more time points were significantly more impaired by arthritis in their overall work (p=0.014) (figure 2D) due to reduced productivity while at work (p=0.001); time away from work was not different (p=0.784).

{kind=link}
![[SP1.jpg]](https://rmdopen.bmj.com/content/rmdopen/3/2/e000551/DC1/embed/inline-supplementary-material-1.jpg?download=true){kind=link}
{kind=link}
Impact of positive discordance (PD) and its persistence on final visit outcomes. Effect of number of time points with PD (PtGA-MDGA ≥3) on (A) 12-item Short-Form Health Survey Physical Component Summary (SF-12 PCS), (B) 12-item Short-Form Health Survey Mental Component Summary (SF-12 MCS), (C) percent activity impairment and (D) predicted probability of employment and percent work productivity loss on final visit (2-year follow-up). Analysis of covariance models are adjusted for relevant covariates and baseline values of respective outcomes; p Values of pairwise contrasts are Benjamini-Hochberg adjusted. +p<0.1, *p<0.05, **p<0.01, ***p<0.001. PtGA, patient global assessment; MDGA, physician global assessment.
Discussion
This is the first study to evaluate determinants of PtGA, MDGA, their discordance and change over a span of 2 years in a large, well-characterised cohort of Hispanics with RA in the USA. It is also the first, to our knowledge, to highlight the adverse effects of presence and persistence of patient–physician discordance on HRQOL outcomes in patients with RA.
Our models explained 71% of baseline PtGA variance. Self-reported pain had the largest contribution (27%), although significantly lower compared with prior reports9 12 32; this disparity may be explained by differences in approaches to determine the relative importance of predictors. Those reports largely used stepwise regression (incremental increase R2), which attributes all variance shared by correlated predictors to whichever is first entered in the hierarchical model. A caveat with this approach is that it may conceal the true contribution of a new predictor towards the R2 if that predictor is correlated with other predictors in the model. Had we used this approach, pain would be accounting for 60.4% of PtGA variance, followed by PHQ-9 (5.8%), with fatigue accounting a mere 2% additional PtGA variance. By contrast, we calculated the impact of independent determinants to the PtGA and MDGA constructs using RWs; those represent the contribution of each predictor in a model to the total variance explained (sum to R2) after accounting for the effects of intercorrelations among variables.29 Therefore, this is the indicated approach in order to provide a meaningful decomposition of the R2.33
The combined effects of fatigue, depression and GH perceptions were uniquely addressed in our study and, along with physical impairment, explained a collective 40% of PtGA variance. Their sizeable impact may reflect higher prevalence,15–18 differences in illness beliefs, experiencing or coping with a chronic ailment and disease literacy.34–36 We further showed that TJC independently accounted for 4% of PtGA variance. Supplementary analyses indicated that pain partially mediated the effect of TJC on PtGA. This suggests that, from a patient perspective, pain represents a broader construct in RA, one not limited to TJC, as sole indicator of articular inflammation.9 12
Our models explained 87% of baseline MDGA variance, consistent with prior reports SJC contributed the most, followed by TJC, ESR and fatigue. Although TJC robustly contributed to MDGA, self-reported pain—the most important predictor of the PtGA estimate—was strikingly under-represented in both ours and other reports.9 12 In our study, this was because TJC fully mediated the effect of pain on MDGA, suggesting that physicians interpret joint tenderness on examination as the primary form or experience of disease-related pain. Interestingly, higher depression scores and older age were associated with lower MDGA, indicating that physicians may underestimate disease activity in these individuals.12 37
While both PtGA and MDGA significantly improved over time, mean discordance tended to increase. This is contrary to what might be expected given that patients and physicians interact with each other across multiple visits, and during that time, they develop a relationship. In addition, MDGA displayed greater improvements over time than PtGA. This was particularly true in subjects with ND. Physicians predicate their ratings and overall treatment efforts on the number of swollen and tender joints and inflammatory markers; fatigue contributes relatively little to their MDGA, while additional parameters such as pain, depression, functional limitation or GH perception that shape patients’ experience of disease activity are not considered at all. Hence, as physicians appreciate significant changes in the aforementioned metrics they mostly care about, they are likely to lower their MDGA score more aggressively compared with patients who still experience—and highly regard—residual fatigue, untreated depression or unaddressed functional limitations.
Despite limited reports on longitudinal trends,8–11 our study is the first to evaluate independent determinants of changes in PtGA and MDGA on multiple visits within a 2-year span, specifically in Hispanics with RA. Similar to baseline determinants, improvements in PtGA were associated with commensurate recovery in pain, physical function, fatigue, depression, TJC and GH. Likewise, improvement in MDGA reflected recovery in SJC, TJC, fatigue and ESR.
The disparity in nature and effect size of the parameters shaping patient and physician perceptions of disease activity led to discordance in 43% of subjects at baseline; this is higher than prior reports using a similarly stringent threshold of ±3 cm (25% for Choi38 and 32.5% for Nicolau39). One possibility may be the low RA activity present in our cohort. At baseline, 157 (29.3%) subjects had MDGA <1; of those, only 42 (27%) had PtGA <1, while 69 (44%) had PD. Alternatively, lower acculturation levels, weaker social support systems and underutilisation of available health services in a primarily immigrant, monolingual sample may further adversely impact PtGA40 and therefore discordance.
In our study, PD is common with fair stability. This raises the question whether PD may in fact represent a patient-related characteristic rather than a visit-specific feature. Supplementary analyses indicated that PD at baseline increased the likelihood of PD at subsequent visits (OR 4.91, 95% CI 2.91 to 8.27). Additionally, patients with persistent PD were more likely to have fibromyalgia and IAD (p<0.001 and p=0.01, respectively). This contrasts a prior report in ankylosing spondylitis of PD being a visit-specific characteristic, and bearing no relation to fibromyalgia.41 ND was far less stable over time than PD. This was attributed to a significant improvement in MDGA without corresponding changes in PtGA post baseline visit. Notably, discordance showed a marginal increase over time despite improvement in both PtGA and MDGA, reflecting a greater appreciation by physicians than patients of decreases in disease activity.
Prior reports addressed discordance cross-sectionally at various thresholds and in diverse cohorts.12 35 42 Longitudinal evaluation of PtGA-MDGA discordance was recently reported in non-Hispanic white8 9 and Japanese patients.11 In the PRESERVE trial, discordance (±2 cm) was negatively associated with work productivity.8 In the SAKURA cohort of newly diagnosed RA patients, PD ≥1 cm predicted lower structural remission and rapid radiographic progression.11 We uniquely demonstrated that patients with PD at any time displayed lower physical and mental HRQOL, decreased work productivity and greater activity impairment at final visit; moreover, physical HRQOL and activity impairment were significantly worse in patients with higher numbers of discordant points. These observations collectively indicate that patient adjustment to RA is individualised in nature and may not be adequately predicted by metrics of disease activity alone. Psychosocial variables may be more influential than objective measures of disease activity in accounting for health outcomes in patients with RA.43 This suggests that an exclusively biomedical approach would not be sufficient for some patients, such as those with PD, since issues like depression, generalised pain and fatigue may be treated more effectively with psychological and/or behavioural interventions rather than pharmacological treatment aimed at the RA disease process. Taken together, this implies that physicians should promptly reconsider the patient perspective in individuals with PD and a multidisciplinary approach to care poised to reduce such discordance is necessary for the treatment of RA.
A particular strength of our study was that physicians were blinded to PtGA scores and all patient-reported outcomes at the time of their MDGA assessment, allowing for an impartial rating. Several limitations should be noted. We had no data on disease literacy, illness beliefs or cultural factors with potential impact on PtGA ratings. This study used the 28-joint count examination which may have underestimated disease activity compared with a 68/66 count for TJC and SJC, respectively. We did not systematically evaluate the impact of comorbidities with a formal index (eg, Charlson Comorbidity Index). However, a priori, we excluded patients from our study with conditions that potentially confound RA treatments such as chronic infections, history of heart failure, chronic kidney disease or cancer, included in such indices. Finally, our sample primarily included monolingual Spanish-speaking first-generation immigrants from Mexico and Central America. Although representative of our general referral base, study findings may not generalise to Hispanics of diverse national origin, levels of acculturation or socioeconomic status.
Conclusions
Determinants of patient and physician assessments of RA activity and their change are disparate in Hispanics yielding significant discordance. Higher patient assessments represent the majority of such discordance and PD at any time adversely impacts HRQOL outcomes, work productivity and activity impairment on final visit. An ideological and structural overhaul of the traditional care model is therefore needed; this would ideally entail a patient-centred approach that empowers patients to articulate their concerns and expectations about their disease state, while allowing physicians a better appreciation of the ‘patient experience’ of RA.
Acknowledgments
The authors would like to thank all patients who participated in this research and acknowledge the contributions of Harbor-UCLA Medical Center rheumatologists Benedict Chou,
Gopika Miller and Rosalinda Moran who contributed to the clinical evaluation and assessment of participants in the study. The authors also acknowledge that the present manuscript is based on work previously presented at the ACR Conference and published as conference abstract in 2016.
References
Footnotes
Contributors GAK conceived and designed the study, collected, analysed and interpreted the data and wrote the draft of the manuscript. SR, CEC, TLD and EH made substantial contributions to data acquisition. VS advised on interpreting health-related quality of life outcomes and contributed to drafting the manuscript. SRO participated in the design of the study, conducted statistical analyses and contributed to drafting the manuscript. Additionally, all authors contributed to the interpretation of the results, critically revised the manuscript for important intellectual content and reviewed and approved the final manuscript. GAK drafted this article and is the guarantor.
Competing interests None declared.
Patient consent Obtained.
Ethics approval John F. Wolfe Human Subjects Committee of the Los Angeles Biomedical Research Institute at Harbor-UCLA Medical Center.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement The dataset used in this study is available from the corresponding author on reasonable request.