Article Text

Abstract
Background Osteopontin (OPN) is a glycoprotein involved in Th1 and Th17 differentiation, tissue inflammation and remodelling. We explored the role of serum OPN (sOPN) as a biomarker in patients with giant cell arteritis (GCA).
Methods sOPN was measured by immunoassay in 76 treatment-naïve patients with GCA and 25 age-matched and sex-matched controls. In 36 patients, a second measurement was performed after 1 year of glucocorticoid treatment. Baseline clinical and laboratory findings, as well as relapses and glucocorticoid requirements during follow-up, were prospectively recorded. sOPN and C reactive protein (CRP) were measured in 32 additional patients in remission treated with glucocorticoids or tocilizumab (interleukin 6 (IL-6) receptor antagonist). In cultured temporal arteries exposed and unexposed to tocilizumab, OPN mRNA expression and protein production were measured by reverse transcription polymerase chain reaction (RT-PCR) and immunoassay, respectively.
Results sOPN concentration (ng/mL; mean±SD) was significantly elevated in patients with active disease (116.75±65.61) compared with controls (41.10±22.65; p<0.001). A significant decline in sOPN was observed in paired samples as patients entered disease remission (active disease 102.45±57.72, remission 46.47±23.49; p<0.001). sOPN correlated with serum IL-6 (r=0.55; p<0.001). Baseline sOPN concentrations were significantly higher in relapsing versus non-relapsing patients (relapsers 129.08±74.24, non-relapsers 90.63±41.02; p=0.03). OPN mRNA expression and protein production in cultured arteries were not significantly modified by tocilizumab. In tocilizumab-treated patients, CRP became undetectable, whereas sOPN was similar in patients in tocilizumab-maintained (51.91±36.25) or glucocorticoid-maintained remission (50.65±23.59; p=0.49).
Conclusions sOPN is a marker of disease activity and a predictor of relapse in GCA. Since OPN is not exclusively IL-6-dependent, sOPN might be a suitable disease activity biomarker in tocilizumab-treated patients.
- giant cell arteritis
- corticosteroids
- cytokines
- systemic vasculitis
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Key messages
To date, serum osteopontin (OPN) concentrations have not been explored in patients with giant cell arteritis (GCA).
Baseline serum OPN concentration is significantly elevated in patients with active GCA compared with controls and patients in remission, and significantly higher in relapsing versus non-relapsing patients.
In cultured GCA arteries, OPN mRNA expression and protein production are not significantly modified by short-term exposure to tocilizumab.
While in tocilizumab-treated patients C reactive protein becomes undetectable, serum OPN is similar in patients in tocilizumab-maintained or glucocorticoid-maintained remission.
Serum OPN might be a suitable disease activity biomarker in tocilizumab-treated patients with GCA. This needs to be explored in larger studies.
Introduction
Giant cell arteritis (GCA) is an inflammatory disease of large-sized and medium-sized arteries with a chronic and relapsing course.1 2 About 43%–64% of patients experience recurrences3–5 and require long-term glucocorticoid treatment with substantial toxicity.4 6 7 For years, attempts to identify glucocorticoid-sparing agents have not been clearly successful,8–10 but a new treatment paradigm based on the inhibition of interleukin 6 (IL-6) signalling is emerging in the field of GCA, supported by two recent randomised controlled trials with the IL-6 receptor neutralising antibody tocilizumab.11 12
The inflammatory markers erythrocyte sedimentation rate (ESR) and C reactive protein (CRP) are widely used in clinical practice to monitor disease activity in patients with GCA.3–5 8–10 However, IL-6 receptor blockade with tocilizumab abrogates the hepatic synthesis of acute-phase reactants and renders CRP and ESR measurement unreliable for the purpose of monitoring disease activity.11 12 For these reasons, there is an urgent need for novel biomarkers that reflect overall disease activity in the era of tocilizumab treatment for GCA.
Osteopontin (OPN) is a multifunctional intracellular and secreted glycoprotein that functions as a matrix protein or as a soluble mediator.13 14 It is expressed by a variety of cells involved in immune and inflammatory responses, including dendritic cells, T and B lymphocytes, macrophages, neutrophils and eosinophils. OPN participates in innate and adaptive immune responses.13–15 It is highly induced after T lymphocyte activation, stimulates Th1 and Th17 differentiation and inhibits Th2-mediated responses. It also promotes B cell differentiation and immunoglobulin production. OPN is not expressed by circulating monocytes, but it is highly upregulated during macrophage differentiation.16 OPN has integrin and CD44 binding sequences and supports lymphocyte and monocyte migration and survival.14–16 In addition, OPN enhances endothelial and vascular smooth muscle cell (VSMC) migration, contributing to angiogenesis and vascular remodelling.17 According to these functions, OPN is highly expressed at the sites of inflammation and tissue injury and reflects concomitant activation of different pathways relevant to immune and inflammatory responses that participate in the pathogenesis of GCA.18 19
Based on its production by activated macrophages, OPN expression was investigated by immunohistochemistry in a variety of granulomatous diseases. In this survey, increased tissue expression of OPN was observed in two temporal artery biopsies from patients with GCA.20 Moreover, increased circulating soluble OPN has been shown in several inflammatory diseases of blood vessels, including Behçet’s disease and anti-neutrophil cytoplasmic antibodies (ANCA)-associated vasculitis.21 22 Elevated tissue and serum concentrations of OPN have been demonstrated in patients with other vascular conditions, such as non-vasculitic thoracic or abdominal aortic aneurysms.23 24 To date, serum OPN (sOPN) concentrations have not been explored in patients with GCA.
In this study, we investigated the value of sOPN as biomarker of disease activity and risk of disease relapse in patients with GCA. In addition, we explored the temporal artery expression of OPN in the context of IL-6 receptor blockade. Finally, we compared the serum concentrations of OPN and CRP in patients in remission receiving tocilizumab (with or without low-dose glucocorticoids) or glucocorticoids alone.
Materials and methods
Patients
The study group consisted of 76 biopsy-proven patients with GCA, selected from two reported cohorts.25–27 The first cohort consisted of patients with GCA prospectively imaged in order to detect large vessel involvement at diagnosis (cohort 1).25 The second cohort incorporated patients who were cross-sectionally evaluated to detect aortic dilatation during follow-up (cohort 2).26 27 Patient inclusion in the present study was based on the availability of serum samples collected at the time of diagnosis, before the initiation of glucocorticoid treatment. Cohort 1 included 42 patients and cohort 2 included 34.
Cranial symptoms (headache, jaw claudication, scalp tenderness), systemic manifestations (weight loss, fever), polymyalgia rheumatica and disease-related cranial ischaemic complications were recorded at the time of diagnosis. CRP, haemoglobin concentration and ESR were determined by laboratory standardised systems.
Patients were followed for at least 2 years (mean 187 weeks, range 114–360), and time to first disease relapse, number of disease relapses, time to reach a stable (at least for 3 months) prednisone maintenance dosage <10 mg/day or <5 mg /day, as well as time to prednisone discontinuation and cumulative prednisone dose were recorded. We used a consensus definition of relapse established in the context of international multicentre clinical trials.9 10 Relapses were defined as reappearance of GCA manifestations, usually accompanied by elevation of acute-phase reactants, that required treatment adjustment. Disease-related symptoms considered were polymyalgia rheumatica, cranial symptoms (headache, scalp tenderness, jaw claudication, cranial ischaemic complications), systemic manifestations (anaemia, fever and/or weight loss) or symptomatic large vessel involvement (extremity claudication). Cranial ischaemic manifestations included amaurosis fugax, GCA-related visual loss, diplopia, transient ischaemic attacks or stroke. Isolated increases in ESR or CRP were not considered relapses unless the above symptoms occurred after close follow-up.
In 36 patients from the discovery cohort, a second sample was obtained after approximately 1 year (402±48 days) of glucocorticoid treatment following a uniform, previously reported tapering protocol.4 28 At the time of the second sample collection, patients were receiving a median daily prednisone dose of 5 mg/day (range 2.5–10 mg/day), and all patients were in clinical remission defined by the absence of disease-related manifestations and the presence of ESR and CRP levels within the normal range.
The control group consisted of two sets of 13 (A) and 12 (B) healthy individuals with no chronic inflammatory diseases and matched for age and gender. sOPN was measured in 17 additional patients with GCA in prednisone-maintained remission. Seven patients were receiving ≥20 mg/day (high dose) and 10 were receiving ≤10 mg/day (low-dose). sOPN was subjected to cross-sectional comparison with that from 15 patients in remission treated with tocilizumab (4–8 mg/kg/month) (as monotherapy or together with low-dose prednisone) to explore the effect of tocilizumab on sOPN concentration. CRP was simultaneously measured in the same samples for comparison purposes. The clinical characteristics of these additional 32 patients have been previously described.29
sOPN, CRP and IL-6 measurement
Serum samples were stored at −80°C until use. sOPN, IL-6 and CRP in sera were determined by immunoassay (Quantikine R&D Systems, Minneapolis, Minnesota, USA). OPN was also detected in the supernatant fluid from cultured temporal arteries.
Culture of temporal arteries from patients with GCA and controls
Temporal artery fragments from 16 patients with GCA and normal temporal arteries from 15 controls (patients with suspected GCA who eventually were diagnosed with other conditions) were cut into 0.8–1 mm sections and were embedded in Matrigel (Corning Matrigel Basement Membrane Matrix, Life Sciences, Tewksbury, Massachusetts, USA) to ensure prolonged survival as described30 31 with or without tocilizumab (RoActemra, purchased from Hoffman-La Roche, Basel, Switzerland) or an IgG isotype control (Sigma, Ayrshire, UK) both at 10 µg/mL. Each condition was tested in two to three replicate wells. Temporal artery biopsies were obtained for diagnostic purposes and, since appropriate diagnosis was the first priority, all conditions could not be tested in all samples due to the small size of tissue spared for research. After 5-day culture, sections were homogenised and frozen in TRIzol reagent (Life Technologies, Carlsbad, California, USA) for RNA extraction.
RNA extraction and real-time reverse transcription polymerase chain reaction (RT-PCR)
Total RNA was obtained from 11 cultured arteries from six patients with GCA and five controls, following the instructions of the manufacturer, and reverse-transcribed to cDNA using Archive Kit (Applied Biosystems, Life Technologies) in a final volume of 100 µL, employing random hexamer priming. OPN and signal transducer and activator of transcription 3 (STAT3) expression, as well as expression of the housekeeping gene GUSb, was investigated using specific predeveloped TaqMan probes (Hs00959010_m1, Hs00374280_m1 and Hs99999908_m1, respectively) from Applied Biosystems (TaqMan Gene Expression Assays). Fluorescence was detected using ViiA 7 Real-Time PCR System and results were analysed with the QuantStudio Real-Time PCR V.1.1 software (both from Applied Biosystems). Gene expression was normalised to the expression of the endogenous control GUSb using comparative threshold cicles (ΔCt) method. mRNA concentration was expressed in relative units with respect to GUSb.
Statistical analysis
Mann-Whitney U test and Student’s t-test, when applicable, were used for quantitative independent or paired data. Correlations were calculated using Spearman’s test. Receiver-operator characteristic (ROC) curves were applied to sOPN concentrations to calculate cut-offs with best sensitivity and specificity. Time (weeks) to first relapse and time required to achieving a maintenance prednisone dose <10 mg/day or <5 mg/day were determined by Kaplan-Meier survival method and compared using the log-rank test. Statistical significance was defined as P<0.05. Calculations were performed with the IBM SPSS Statistics V.20.0.
Results
sOPN concentrations are increased in patients with active GCA
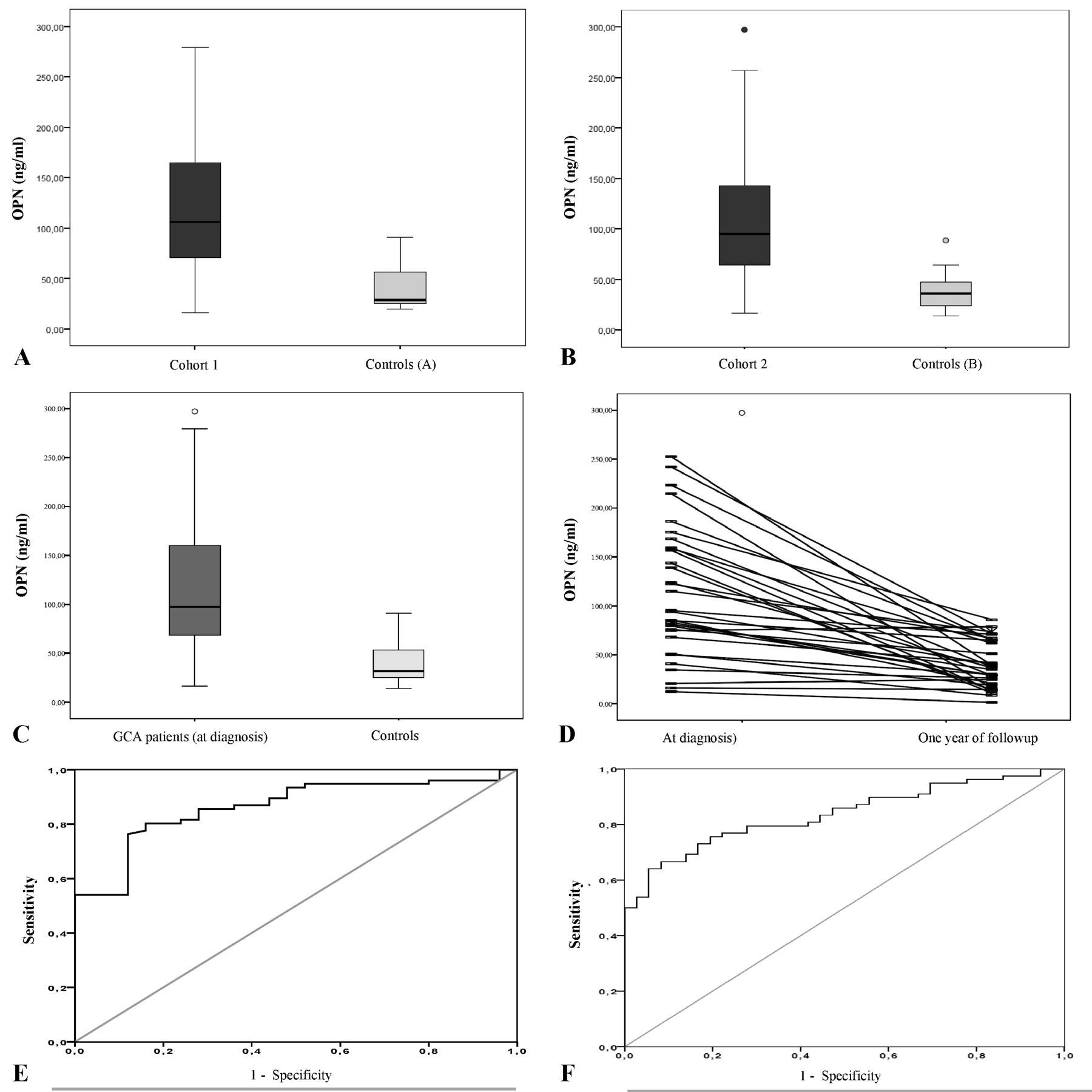
Table 1 summarises clinical and laboratory data from cohort 1 and cohort 2 of patients with GCA. sOPN concentrations (ng/mL; mean±SD) were significantly elevated in patients with active GCA compared with controls in both cohorts: GCA 119.59±70.36 vs controls 42.82±24.58 (p<0.001) in cohort 1, and GCA 113.21±69.56 vs controls 39.24±21.28 (p<0.001) in cohort 2 (figure 1A,B); as well as in the pooled cohorts of patients with active GCA (116.75±69.61) compared with pooled healthy controls (41.10±22.65; p<0.001) (figure 1C). In the 36 patients who underwent a second sample collection at the time of disease remission, a significant decline in sOPN concentrations was observed (active disease at baseline 102.45±57.72 vs remission 46.47±23.49; p<0.001) (figure 1D). Using ROC analysis, an sOPN cut-off of 59.79 ng/dL resulted in a sensitivity and specificity of 80% and 84%, respectively, for patients with active GCA compared with healthy controls (area under the curve (AUC) 0.862, 95% CI 0.788 to 0.937; p<0.001) (figure 1E). Moreover, a sOPN cut-off of 67.28 ng/dL resulted in a sensitivity and specificity of 77% and 78%, respectively, to detect disease activity when analysing active patients and those in remission (AUC 0.836, 95% CI 0.764 to 0.907; p<0.001) (figure 1F). No significant differences in sOPN concentrations were found between patients in remission (48.78±23.97) and healthy controls (41.10±22.65; p=0.213).
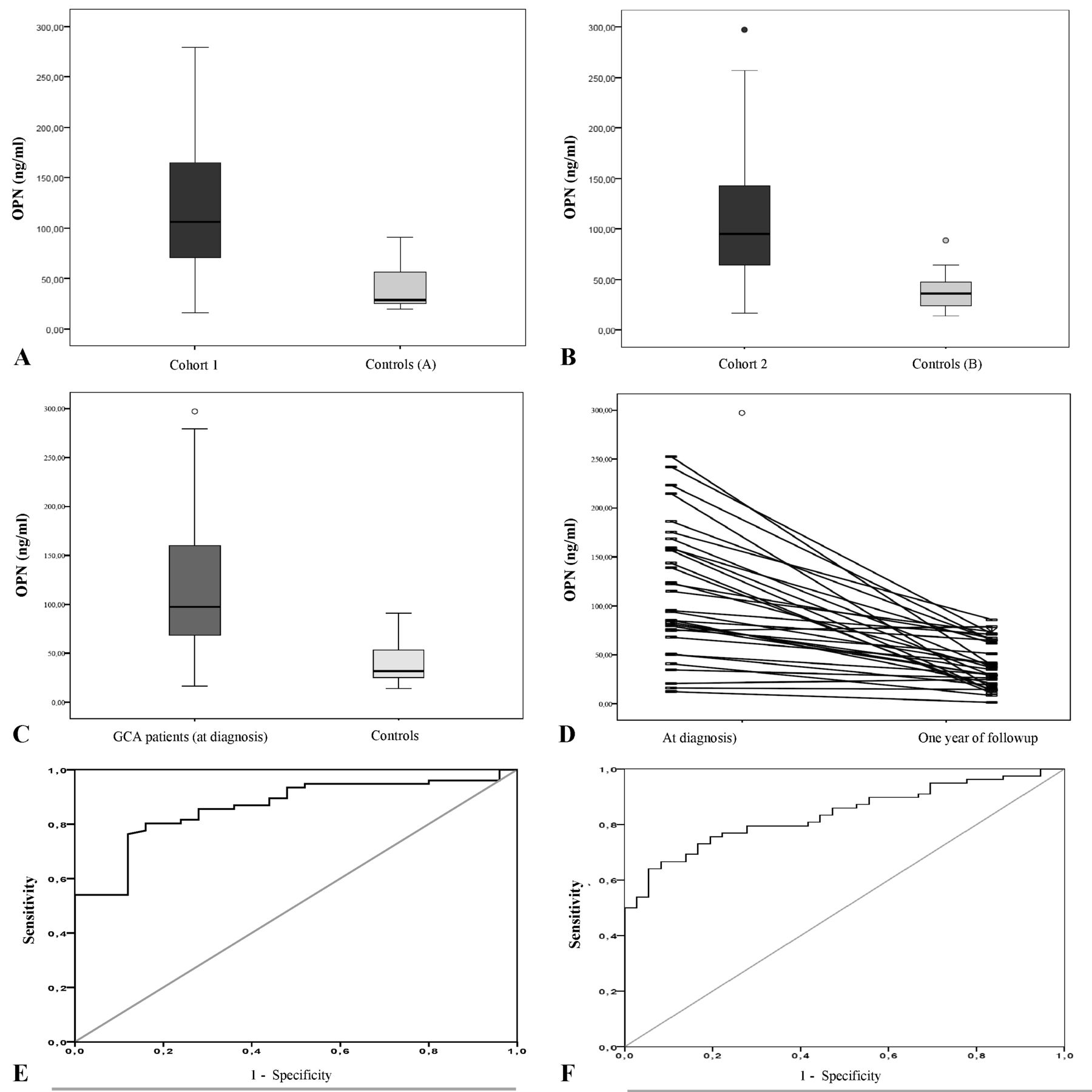
Serum osteopontin (sOPN) concentrations in patients with giant cell arteritis and healthy controls. (A) sOPN concentrations in active patients with giant cell arteritis (GCA) from the cohort 1 and in controls (subgroup A). (B) sOPN concentrations in active patients with GCA from the cohort 2 and controls (subgroup B). (C) sOPN concentrations in the pooled cohorts of patients with active GCA and controls. Box-plot in (A), (B) and (C) represent median, 25%–75% percentile and range. (D) sOPN concentrations in patients with GCA at diagnosis and when in remission by paired comparison. (E) Receiver-operator characteristic (ROC) analysis of sOPN concentrations in patients with active GCA versus controls. (F) ROC curve of patients with active GCA versus patients in remission.
Baseline clinical, laboratory and follow-up data of patients with giant cell arteritis
Patients with GCA with active disease and systemic symptoms demonstrated significantly higher sOPN concentrations than those with no systemic symptoms (118.45±61.70 vs 82.70±57.50; p=0.028) (table 2). Contrarily, and as previously described for serum IL-6,32 sOPN concentrations were significantly lower in patients with cranial ischaemic complications compared with patients without these complications (79.91±57.90 vs 117.29±61.32; p=0.028) (table 2). There were no differences in baseline sOPN levels between patients with or without vascular imaging compatible with large vessel inflammation (table 2). In addition, there was no correlation between baseline sOPN concentrations and subsequent aortic dilatation (table 2).
Serum OPN concentrations according to clinical/imaging data in the pooled cohort of patients with giant cell arteritis
sOPN correlates with acute-phase reactants and circulating IL-6
At the time of GCA diagnosis, sOPN showed a positive correlation with serum IL-6 (r=0.55; p<0.001) and with the IL-6-dependent acute-phase reactants ESR (r=0.32; p=0.009) and CRP (r=0.42; p<0.001). In addition, baseline sOPN negatively correlated with haemoglobin concentrations (r=−0.34; p=0.005).
Baseline sOPN concentration predicts disease relapse and glucocorticoid use
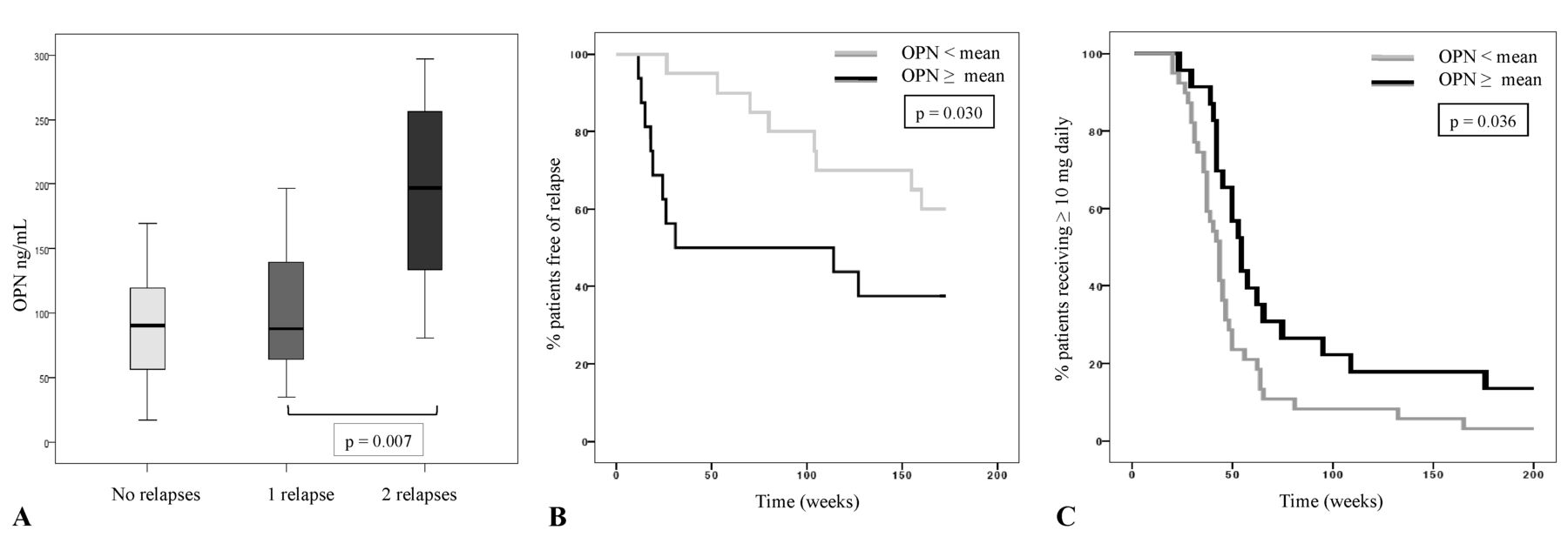
Baseline sOPN was significantly higher in patients who developed disease relapses during follow-up (relapsers 129.08±74.24 vs non-relapsers 90.63±41.02 ng/mL; p=0.03). Within the group of relapsers, patients with more than one disease relapse demonstrated significantly higher sOPN levels (194.00±77.02) than those with only one relapse (98.52±50.72; p=0.007) (figure 2A).

Baseline serum osteopontin in patients with giant cell arteritis as predictor of relapses and duration of glucocorticosteroid treatment. (A) Baseline sOPN concentrations in patients with no subsequent relapses, with 1 relapse and with ≥2 relapses. (B) Percentage of patients in remission over time according to baseline sOPN (≥mean sOPN vs <mean sOPN). (C) Percentage of patients requiring a daily maintenance prednisone dose ≥ 10 mg over time according to baseline sOPN (≥ mean sOPN v s < mean sOPN).
Furthermore, the percentage of patients in remission over time was significantly lower in patients with baseline sOPN concentrations superior to the mean value (p=0.03) (figure 2B).
The proportion of patients requiring a prednisone maintenance dose ≥10 mg/day over time was significantly higher among patients with sOPN levels above the mean sOPN concentration at the time of diagnosis (p=0.036) (figure 2C).
Moreover, there was a positive correlation between the baseline sOPN and the time to achieve a stable glucocorticoid dose <10 mg/day (r=0.43, p=0.02) or <5 mg/day (r=0.48, p=0.03), and between baseline sOPN and the cumulated prednisone dose at the time of prednisone discontinuation (r=0.37; p=0.01).
In contrast to the sOPN findings, no significant differences were found in baseline IL-6 (49.76±41.52 vs 28.00±30.86 pg/mL; p=0.237), ESR (83.88±31.10 vs 95.28±20.38 mm/1 hour; p=0.188), CRP (9.77±8.37 vs 6.70±3.91 mg/dL; p=0.117) or haemoglobin (116.56±14.33 vs 113.11±12.15 mg/dL; p=0.412) concentrations between relapsing patients and patients who achieved sustained clinical remission (online supplementary table S1). As with sOPN, the proportion of patients who relapsed over time was significantly higher in patients with CRP concentrations above the mean level than in patients with lower concentrations (p=0.022), but no differences were found according to IL-6, ESR or haemoglobin values (online supplementary figure S1). Together, these data underline the predictive value of baseline sOPN in terms of disease relapse and long-term glucocorticoid requirements in patients receiving glucocorticoid monotherapy.
Supplementary Table 1
Supplementary file 2
OPN expression and secretion in cultured GCA arteries are not suppressed by short-term IL-6 receptor blockade
IL-6 receptor signalling results in activation and expression of transcription factor STAT-3.32 We have previously shown that cultured temporal arteries have constitutive IL-6 and STAT3 expression and activation.30 31 As previously shown, STAT3 expression was higher in cultured control arteries than in cultured GCA involved arteries, possibly reflecting loss of STAT-3 producing VSMCs31 (figure 3A). Short-term treatment with the anti-IL-6 receptor monoclonal antibody tocilizumab for 5 days, at concentrations able to reduce STAT3 expression (figure 3A), did not modify OPN mRNA expression or protein secretion in cultured GCA arteries (figure 3B,C). These findings support that, in spite of the correlation between serum IL-6 and sOPN, OPN production in GCA arteries is not exclusively dependent on IL-6 signalling.

Effect of tocilizumab (TCZ) on osteopontin (OPN) and STAT3 expression in cultured temporal arteries from patients with giant cell arteritis (GCA) and controls. (A) STAT3 mRNA expression in relative units (RU) by cultured temporal arteries from negative controls (n=5) and from patients with GCA untreated (n=6), treated with TCZ at 10 µg/mL (n=6) or treated with non-immune human control IgG at 10 µg/mL (n=4). *p=0.030 vs negative biopsies, #p=0.046 vs untreated GCA biopsies (paired comparison). (B) OPN mRNA expression in RU by cultured temporal arteries from negative controls and from patients with GCA untreated, treated with TCZ at 10 µg/mL or treated with non-immune human control IgG at 10 µg/mL as in (A). (C) OPN concentrations in the supernatants of cultured temporal arteries from negative controls (n=15) and from patients with GCA untreated (n=14), treated with TCZ at 10 µg/mL (n=15) or treated with non-immune human control IgG at 10 µg/mL (n=16). **p<0.001 vs negative control samples. Sensitivity of the immunoassay (minimal detectable concentration) was 0.011 ng/mL.
sOPN is reduced but not abrogated in patients with GCA in remission treated with tocilizumab
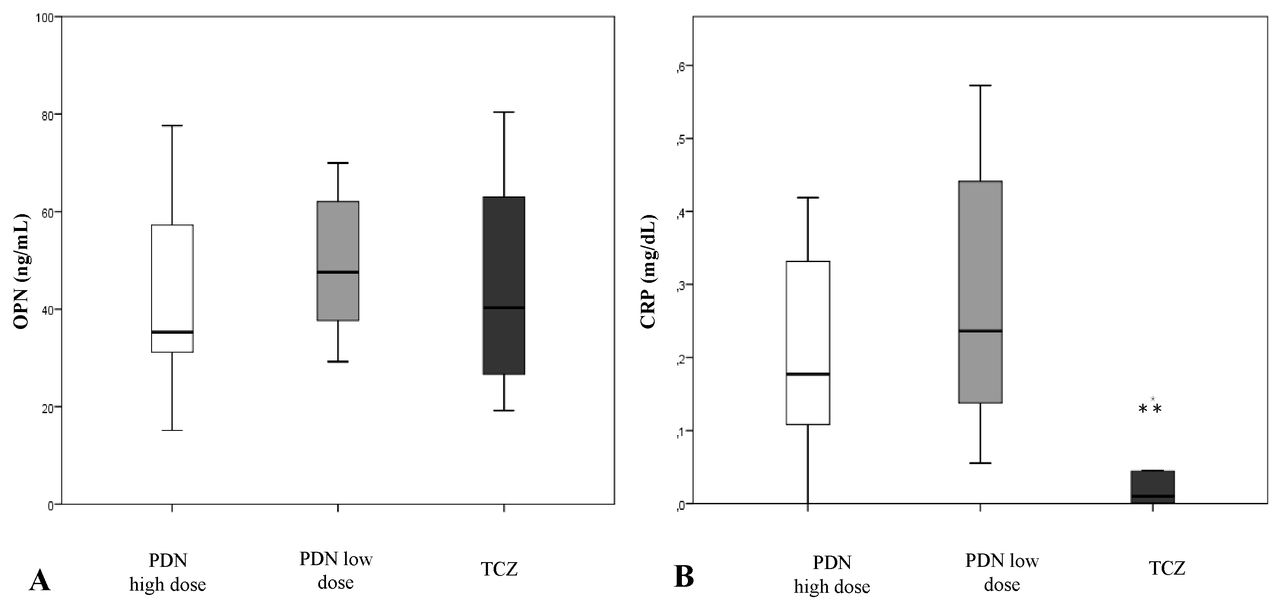
Based on our results on cultured arteries, we measured sOPN and serum CRP concentrations in a subset of patients with GCA who were in remission maintained with glucocorticoids or tocilizumab (alone or in combination with low-dose prednisone) to see whether sOPN could be a useful biomarker in patients receiving IL-6 blockade therapy. As shown in figure 4, serum CRP was significantly lower and sometimes undetectable in tocilizumab-treated patients (0.06±0.16 mg/dL) compared with prednisone only-treated patients at high dose (0.25±0.24 mg/dL; p=0.017) or low dose (0.28±0.19 mg/dL; p<0.001). In contrast, sOPN was detected in all cases without significant differences between patients under tocilizumab (51.91±36.25) or glucocorticoid only treatment either at high dose (43.55±21.36; p=0.861) or low dose (55.62±24.87; p=0.24). These results suggest that, unlike CRP, sOPN might be an interesting disease activity biomarker to be explored in tocilizumab-treated patients.
{kind=link}
{kind=link}
![[SP2.jpg]](https://rmdopen.bmj.com/content/rmdopen/3/2/e000570/DC2/embed/inline-supplementary-material-2.jpg?download=true){kind=link}
{kind=link}
{kind=link}
Serum osteopontin (sOPN) and C reactive protein (CRP) in patients with giant cell arteritis (GCA) in remission according to treatment. (A) sOPN in patients with GCA in remission with high-dose prednisone (PDN) (≥20 mg/day), low-dose prednisone (≤10 mg/day) or with tocilizumab (TCZ). (B) Serum CRP concentration in patients with GCA in remission with high-dose prednisone (≥20 mg/day), low-dose prednisone (≤10 mg/day) or with TCZ. **p=0.017 vs high-dose prednisone group and p<0.001 vs low-dose prednisone group. Sensitivities (minimal detectable concentration) of OPN and CRP immunoassay are 0.011 ng/mL and 0.010 ng/mL, respectively.
Discussion
In this study, we demonstrated that sOPN was significantly elevated in patients with active GCA compared with age-matched and sex-matched healthy individuals but returned to normal when patients achieved remission with glucocorticoid treatment. In addition, patients with the highest sOPN concentrations at diagnosis experienced more relapses and cumulated higher glucocorticoid doses. Previous studies have indicated that an intense systemic inflammatory response assessed by a composite combination of clinical and biological data is associated with recurrent disease.4 5 33 Accordingly, in the present study, sOPN was significantly higher in patients with strong systemic inflammatory response than in patients with weak acute-phase reaction. Interestingly, although sOPN at baseline correlated with ESR, CRP and IL-6, and negatively with haemoglobin concentration, sOPN performed better than individual detection of ESR, CRP, haemoglobin or IL-6 as predictor of relapsing course. sOPN is increased in a variety of conditions conveying tissue injury and remodelling, including malignancies, infection and other systemic vasculitis.21 22 34 Therefore, sOPN may not be a suitable diagnostic biomarker. However, if confirmed in larger studies, our data indicate that sOPN may be a useful biomarker of disease activity and predictor of relapsing disease and glucocorticoid requirements.
Regarding additional clinical data, patients with cranial ischaemic complications had significantly lower sOPN concentrations. A similar pattern has been previously shown for serum IL-6,35 and, in fact, in the present study sOPN and sIL-6 concentrations significantly correlated, suggesting coordinated regulation. As hypothesised for IL-6, angiogenic activity of OPN might compensate for ischaemia at distal sites.35 36
Although glucocorticoids are very efficient in inducing remission in the majority of patients, glucocorticoid tapering results in relapse in a substantial number of individuals. No clear alternatives to prolonged use of glucocorticoids were available to treat patients with GCA until very recently.8–12 37 A phase II and a phase III trial have demonstrated the efficacy and safety of blocking IL-6 receptor with tocilizumab in maintaining remission and sparing glucocorticoid in GCA.11 12 However, neutralising IL-6 receptor blocks the synthesis of acute-phase response and leads to a transient rebound in serum IL-6, making difficult the assessment of disease activity in individuals treated with tocilizumab.38 OPN synthesis is activated through different pathways. Its promoter region has binding sites for transcription factors relevant to immune and inflammatory responses such as nuclear factor kB (NFkB), activator protein 1 (AP-1) and STAT3, which also regulate IL-6 expression.39 Although OPN can be induced by IL-6, it is not exclusively IL-6-dependent. It can be also induced by IL-1β, tumour necrosis factor-α and interferon-γ, among others.16 Our preliminary results indicate that short-term treatment exposure of ex vivo cultured GCA arteries to tocilizumab does not have a selective impact on OPN expression in GCA lesions. Consistently, while tocilizumab virtually abolished serum CRP, sOPN was similar in patients in glucocorticoid-maintained or tocilizumab-maintained remission. All together, these data suggest that sOPN could be a useful biomarker of disease activity for tocilizumab-treated patients.
Our data on baseline sOPN were obtained from two patient cohorts subjected to imaging.25–27 As with serum IL-6, sOPN did not seem to be associated with anatomical disease extension in these patients since there was no relationship between sOPN and computed tomography angiography (CTA) detection or extension of large-vessel inflammation at diagnosis. Moreover, as shown for serum IL-6,26 27 sOPN at diagnosis did not predict subsequent development of aortic dilatation in our patients.
Our study has important strengths: it is performed in a sizeable and unique cohort of patients with treatment-naïve, biopsy-proven GCA, subjected to standardised clinical evaluation, imaging and treatment. However, detection of sOPN in patients in tocilizumab-induced vs glucocorticoid only-induced remission was cross-sectional, and the performance of sOPN as a marker of disease activity in these patients could not be specifically assessed, since no baseline samples or samples during relapse were available. The absence of baseline samples from patients treated with tocilizumab also prevents assessment of sOPN as predictor of response to tocilizumab as demonstrated in rheumatoid arthritis.40 This would be an interesting point to be investigated in future studies.
In summary, our data suggest that OPN might be a biomarker of disease activity in patients with GCA, and our preliminary data suggest that it might be particularly useful for patients treated with tocilizumab. Its performance in this setting deserves to be explored in larger prospective, longitudinal cohorts or in sera collected during clinical trials.
Acknowledgments
The authors thank Anna Jordán and Carmen Ligero for their valuable help in getting blood samples from the patients.
References
Footnotes
SP-G and NT-G contributed equally.
Contributors MCC had full access to all of the data in the study and takes responsibility for the integrity of the data and the accuracy of the data analysis. Study design: SP-G, NT-G, MCC. Acquisition of data: SP-G, NT-G, MC-B, CM, EP-R, AG-M, GE-F, IT-B, AP, JM-H, MAA, JH-R, SHU, MCC. Analysis and interpretation of data: SP-G, GE-F, MAA, MC-B, EP-R, JH-R, SHU, MCC. Manuscript preparation: SP-G, NT-G, SHU, MCC. Statistical analysis: SP-G, MAA, NT-G, MCC. All authors read, made improvements and approved the manuscript.
Funding Supported by Ministerio de Economía y Competitividad (SAF 14/57708-R and SAF17/82275-R), Marató TV3 (201507), Instituto de Salud Carlos III (PIE13/00033) and Fondo Europeo de Desarrollo Regional (FEDER, una manera de hacer Europa). SP-G and IT-B were supported by a research award from Hospital Clínic, GE-F by Instituto de Salud Carlos III (PI 15/00092), and MAA by Consejo Nacional de Ciencia y Tecnología (CONACyT), Mexico, and by Agencia de Gestió d’Ajuts Universitaris i de Recerca (AGAUR), Generalitat de Catalunya.
Competing interests GE-F, SP-G, JH-R, SHU and MCC have participated in the GiACTA trial sponsored by Hoffmann-La Roche. MCC has received consultation fees from Hoffman-La Roche.
Ethics approval The study was approved by the ethics committee of Hospital Clínic (Barcelona, Spain) and the Massachusetts General Hospital (Boston, Massachussets, USA).
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement No additional data are available.