Article Text

Abstract
Objective To report the efficacy, patient-reported, radiographic and safety outcomes of 4 years’ certolizumab pegol (CZP) treatment in patients with psoriatic arthritis (PsA).
Methods RAPID-PsA (NCT01087788) was double-blind and placebo-controlled to Week 24, dose-blind to Week 48 and open-label (OL) to Week 216. Patients were randomised 1:1:1 to either placebo or CZP 200 mg every 2 weeks (Q2W) or 400 mg every 4 weeks (Q4W) (following 400 mg at Weeks 0/2/4). Patients randomised to CZP continued their assigned dose in the OL period. Patients randomised to placebo were re-randomised to CZP 200 mg Q2W or 400 mg Q4W (post-loading dose) at Week 16 (early escape) or after the double-blind phase. We present observed and imputed data; missing values were imputed using non-responder imputation (NRI) for categorical and last observation carried forward (LOCF) for continuous measures.
Results 409 patients were randomised; 20% (54/273) of Week 0 patients randomised to CZP had prior anti-tumour necrosis factor (TNF) exposure; 67% (183/273) completed 216 weeks. By Week 48, 60.4% of patients achieved Disease Activity Index for Psoriatic Arthritis low disease activity or remission, which was maintained; 66.3% achieved these outcomes at Week 216 (NRI). At Weeks 48 and 216, 39.2% of patients achieved minimal disease activity (NRI). 75% reduction in Psoriasis Area and Severity Index responses were 65% and 52% at Weeks 48 and 216 (NRI). Total resolution rates for enthesitis, dactylitis and nail psoriasis, at 4 years, were 71%, 81% and 65%, respectively (LOCF). Structural damage progression was low over 4 years’ treatment. No new safety signals were identified after Week 96.
Conclusions CZP efficacy in treating PsA was maintained over 4 years, in patients both with and without prior anti-TNF exposure, with no new safety signals identified.
- anti-tnf
- tnf-alpha
- dmards (biologic)
- psoriatic arthritis
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Key messages
What is already known about this subject?
Previous reports of RAPID-PsA demonstrated the efficacy and safety of certolizumab pegol (CZP) with two CZP dose regimens over 96 weeks for the treatment of psoriatic arthritis (PsA) in patients with and without prior anti-tumour necrosis factor (TNF) exposure.
What does this study add?
CZP efficacy in patients with and without prior anti-TNF exposure and improvements in patient-reported outcomes, psoriasis, nail disease, enthesitis and dactylitis were maintained over 4 years’ treatment.
Patients completing 4 years’ CZP treatment achieved stringent treatment targets: 44% achieved Disease Activity Index for Psoriatic Arthritis (DAPSA) remission, 32% achieved DAPSA low disease activity, 58% achieved minimal disease activity and 29% achieved very low disease activity.
There was little radiographically detectable progression in structural joint damage in patients with PsA treated with CZP throughout the 4-year RAPID-PsA trial.
How might this impact on clinical practice?
The long-term efficacy of CZP in patients with and without prior anti-TNF exposure and the sustained improvements across most PsA disease domains support the use of CZP for the long-term therapeutic management of PsA.
Introduction
Psoriatic arthritis (PsA) is a heterogeneous and multifaceted chronic inflammatory musculoskeletal disease affecting up to 30% of patients with psoriasis.1 2 More than half of patients with PsA have a progressive and erosive disease, which results in functional impairment.3 4 In addition to peripheral joint involvement, patients are also affected by skin and nail psoriasis, enthesitis and dactylitis. Moreover, PsA is associated with numerous extra-articular immune-mediated symptoms, such as uveitis and inflammatory bowel disease, and comorbidities, including cardiovascular disease, obesity, diabetes, osteoporosis, cancer, fatty liver disease, anxiety and depression. The Group for Research and Assessment of Psoriasis and Psoriatic Arthritis (GRAPPA) international guidelines for the treatment of PsA have outlined how an integrated treatment approach should be taken to address the different clinical domains of PsA (peripheral arthritis, axial disease, enthesitis, dactylitis and nail disease) and comorbidities.5
Previous reports of RAPID-PsA (NCT01087788), a phase 3 double-blind, placebo-controlled trial of CZP in patients with PsA, have demonstrated the safety and efficacy of CZP in improving multiple manifestations of the disease, including arthritis, skin disease, nail psoriasis, dactylitis and enthesitis, while also inhibiting progression of structural damage and providing improvements in patient-reported outcomes (PROs)2 6; CZP efficacy was observed from Week 12 (during the double-blind phase) and was maintained to Week 96, in patients both with and without prior antitumour necrosis factor (TNF) exposure.7 Here, we present the final report of long-term efficacy outcomes of CZP treatment and safety data from the 4-year RAPID-PsA trial.
Methods
Patients
Patient eligibility criteria for the RAPID-PsA trial have been reported elsewhere.2 Briefly, eligible patients were ≥18 years, with a diagnosis of active PsA, fulfilling the Classification Criteria for Psoriatic Arthritis,8 of ≥6 months’ duration and had failed treatment with ≥1 disease-modifying antirheumatic drug (DMARD). Up to 40% of patients could have experienced loss of efficacy (secondary failure) or intolerance to one prior anti-TNF.
The study protocol, amendments and subject informed consent were reviewed by a national, regional or Independent Ethics Committee or Institutional Review Board prior to implementation. Patients’ informed consent was obtained and documented, and the study conducted in accordance with local regulations, International Council for Harmonisation Good Clinical Practice requirements and the ethical principles that have their origin in the principles of the Declaration of Helsinki.
Study design
RAPID-PsA (NCT01087788) was a 216-week, phase 3, randomised, multicentre study in patients with PsA. The trial was double-blind and placebo-controlled to Week 24, dose-blind to Week 48 and open-label (OL) to Week 216. The primary clinical (American College of Rheumatology (ACR) 20 at Week 12) and radiographic (change from baseline in van der Heijde modified Total Sharp Score (mTSS) for PsA9 at Week 24) endpoints of RAPID-PsA and interim analyses of the dose-blind period (Weeks 24–48) and the first 48 weeks of the OL period (ie, 96 weeks from the study start) have been reported previously.7 Here, we present data from the combined double-blind, dose-blind and OL phase up to Week 216.
A total of 409 patients were randomised 1:1:1 to placebo or subcutaneous CZP 400 mg at Weeks 0, 2 and 4 (loading dose) followed by either CZP 200 mg every 2 weeks (Q2W) or CZP 400 mg every 4 weeks (Q4W) (figure 1A). Patients randomised to placebo in the dose-blind phase were re-randomised 1:1 to CZP 200 mg Q2W or CZP 400 mg Q4W (following CZP loading dose) either on failing to achieve ≥10% reduction in tender and swollen joint counts at both Weeks 14 and 16 (early escape) or after having completed the 24-week double-blind phase (figure 1A).

(A) RAPID-PsA trial design, (B) patient disposition to Week 216 and (C) Kaplan-Meier plot to time of withdrawal for any reason, or due to lack of efficacy or adverse events, for patients randomised to CZP at Week 0. †Only 121 of the 123 Week 0 CZP 200 mg Q2W patients who completed the dose-blind period of treatment went on to start the open-label period of treatment. ‡One fewer patient went on to start the open-label period of treatment. *Censored patients are those that withdrew due to reasons other than lack of efficacy or adverse event and those lost to follow-up. CZP, certolizumab pegol; Q2W, every 2 weeks; Q4W, every 4 weeks; TJC, tender joint count; SJC, swollen joint count.
Study procedures and evaluations
Efficacy assessments included ACR 20/50/70 responder rates,10 11 Psoriasis Area and Severity Index (PASI) 75/90/100 responder rates,10 mean change from baseline in body surface area (BSA) affected by psoriasis and ≤1% BSA responder rates (skin outcomes reported in patients with baseline skin involvement ≥3% BSA). The Disease Activity Index for Psoriatic Arthritis (DAPSA),12 the proportion of patients achieving DAPSA low disease activity (LDA; DAPSA >4 and ≤14), DAPSA remission (DAPSA ≤4), minimal disease activity (MDA; fulfilling at least 5 of 7 MDA criteria) and very low disease activity (VLDA; achieving all 7 MDA criteria) were also analysed.
Change in nail psoriasis, enthesitis and dactylitis were also assessed. Enthesitis was evaluated by mean change from baseline in the Leeds Enthesitis Index (LEI)13 and total resolution of enthesitis (LEI=0) responder rates for patients with baseline involvement (LEI >0). Dactylitis was evaluated by mean change from baseline in the Leeds Dactylitis Index (LDI)13 and total resolution (LDI=0) responder rates for patients with baseline involvement (defined as having at least 1 digit affected and with a difference in circumference ≥10% compared with the opposite digit and LDI >0). Nail psoriasis was evaluated by mean change from baseline in the modified Nail Psoriasis Severity Index (mNAPSI)13 and total resolution (mNAPSI=0) responder rates for patients with baseline involvement (mNAPSI >0).
PRO measures included pain (0–100 mm visual analogue scale (VAS)),14 fatigue (0–10 VAS),15 function (Health Assessment Questionnaire Disability Index, HAQ-DI; range: 0 (mild limitations of physical function)–3 (very severe limitations of physical function)),13 the Short-Form 36-item health survey (mental component summary (MCS) and physical component summary (PCS); standardised so that the mean and SD of each scale in the USA general population were 50 and 10, with higher scores indicating better health-related quality of life)16 17 and PsA quality of life (PsAQoL; range: 0 (best)–20 (worst)).18 Improvements in these PROs were evaluated by mean change from baseline.
Structural joint damage (measured using mTSS) was evaluated for patients originally randomised to CZP to Week 216 as part of the Week 216 reading campaign, which included radiographs taken at baseline, Week 96, Week 168 and Week 216. Radiographs were also read for patients originally randomised to placebo who switched to CZP treatment at Week 16 or 24. For these patients, mTSS change was assessed from CZP initiation. Radiographic images were scored by two central readers who were blind to patient information and the chronological order of the images. Structural joint damage was evaluated as mean change from baseline mTSS and the proportion of patients with no (or minimal) structural joint damage (non-progression; defined as change from baseline in mTSS ≤0.5 or ≤0) to Week 216. All structural joint damage as described above was also evaluated for patients stratified by their baseline mTSS into two subgroups (either > or ≤ the median baseline mTSS of 4.5).
The Safety Set consisted of patients who received at least one dose of CZP at any point during the 216-week trial. The occurrence of adverse events (AEs) was assessed and recorded at every visit and coded according to the Medical Dictionary for Regulatory Activities (MedRA) criteria, V.14.1. Treatment-emergent adverse events (TEAEs) occurring after the first CZP administration until 70 days after the last CZP administration were recorded.
Statistical analysis
Efficacy results for clinical, functional and structural joint damage outcomes are presented for patients treated with CZP from Week 0 (both doses combined) in this manuscript. Data for patients stratified by the dose they received and data for the ‘All CZP’ group (all patients randomised to CZP at Week 0, combined with patients randomised to placebo at Week 0 who were later re-randomised to CZP) are presented in the online supplementary material.
Supplementary file 1
Enthesitis, dactylitis and nail psoriasis measures (LEI, LDI, mNAPSI) are reported for patients affected by the respective symptoms at baseline. Missing categorical data were imputed by non-responder imputation (NRI), except for total resolution of enthesitis, dactylitis and nail psoriasis, missing values for which were imputed by last observation carried forward (LOCF); missing continuous data were imputed by LOCF for all patients with at least a measurement at baseline. Observed data are also presented.
Structural joint outcomes were evaluated using a mixed-effect model for repeated measures (MMRM),19 with mTSS as the dependent variable, and where dose regimen, visit and their interaction were fixed-effects. An unstructured covariance matrix was used to account for within-subject correlation. MMRM is a model-based approach that was chosen because it allows the use of all available data over the course of the study, where any missing data are assumed to be missing at random. This is done without having to specify a method of imputation. Data are presented as the least squares mean with 95% confidence intervals (CIs) for mTSS and change from baseline in mTSS. The percentage of patients with mTSS non-progression are reported based on the observed data for patients assessed at each visit.
Patient withdrawal due to lack of efficacy or AE was estimated using the Kaplan-Meier statistical analysis. Patients that withdrew for other reasons and were lost to follow-up were censored at the time of withdrawal.
Safety data are presented for the Safety Set. TEAEs are reported as the proportion of the Safety Set who experienced each event, and in terms of event rate (ER) per 100 patient-years (PY) of exposure. Malignancies, including lymphoma, were identified using the Standardised MedDRA Query (SMQ), ‘Malignancies.’ ‘Infections and Infestations’, ‘ Musculoskeletal and Connective Tissue Disorders’ and ‘ Cardiac Disorders’ were each identified using System Organ Classes (SOCs) of the same name.
Results
Patient disposition and baseline characteristics
There were 409 patients randomised in RAPID-PsA; 273 were randomised to receive CZP from Week 0 (baseline) and 136 to placebo. Baseline demographic and disease characteristics of all patients randomised to CZP have been published previously and are summarised in online supplementary table 1. Among patients randomised to placebo, 59 required early escape and were re-randomised to CZP at Week 16; 61 completed the double-blind phase and were re-randomised to receive CZP at Week 24; 16 discontinued study treatment prior to re-randomisation to CZP (figure 1B). Of the 393 patients who received at least one dose of CZP at any time during the RAPID-PsA trial, 75 (19%) had prior anti-TNF exposure, 54 (72%) of whom were randomised to CZP at Week 0. Baseline demographics and disease severity characteristics were similar between all patients in the different dosing arms as has been reported previously.7
Of the 273 patients randomised to CZP at baseline, 248 (90.8%) patients completed to Week 24, 237 (86.8%) patients completed to Week 48 and 183 (67.0%) completed to Week 216 (figure 1B). In the combined double-blind, dose-blind and OL periods, 36/273 (13.2%) and 9/273 (3.3%) patients withdrew from the study due to an AE or lack of efficacy, respectively; 45/273 (16.5%) withdrew for other reasons (figure 1C).
Efficacy outcomes
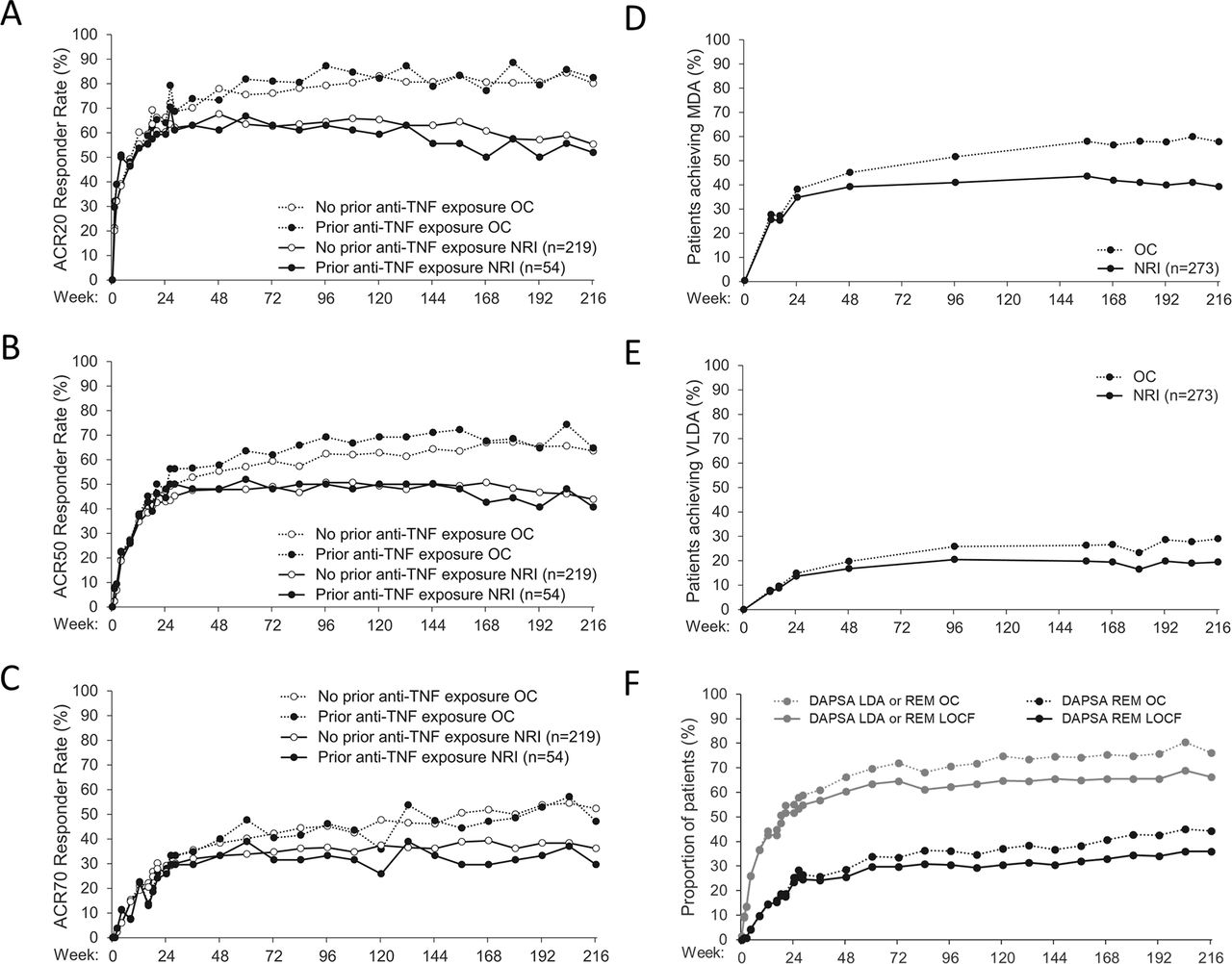
The significant improvements seen in joint disease in patients with PsA, as measured by ACR 20/50/70 after 24 weeks of CZP treatment, were generally maintained throughout the dose-blind and OL phases of the 4-year study and were similar irrespective of prior anti-TNF exposure (online supplementary figure 1, figure 2A–C and table 1).
Clinical disease activity and patient-reported outcomes in patients randomised to CZP treatment at Week 0
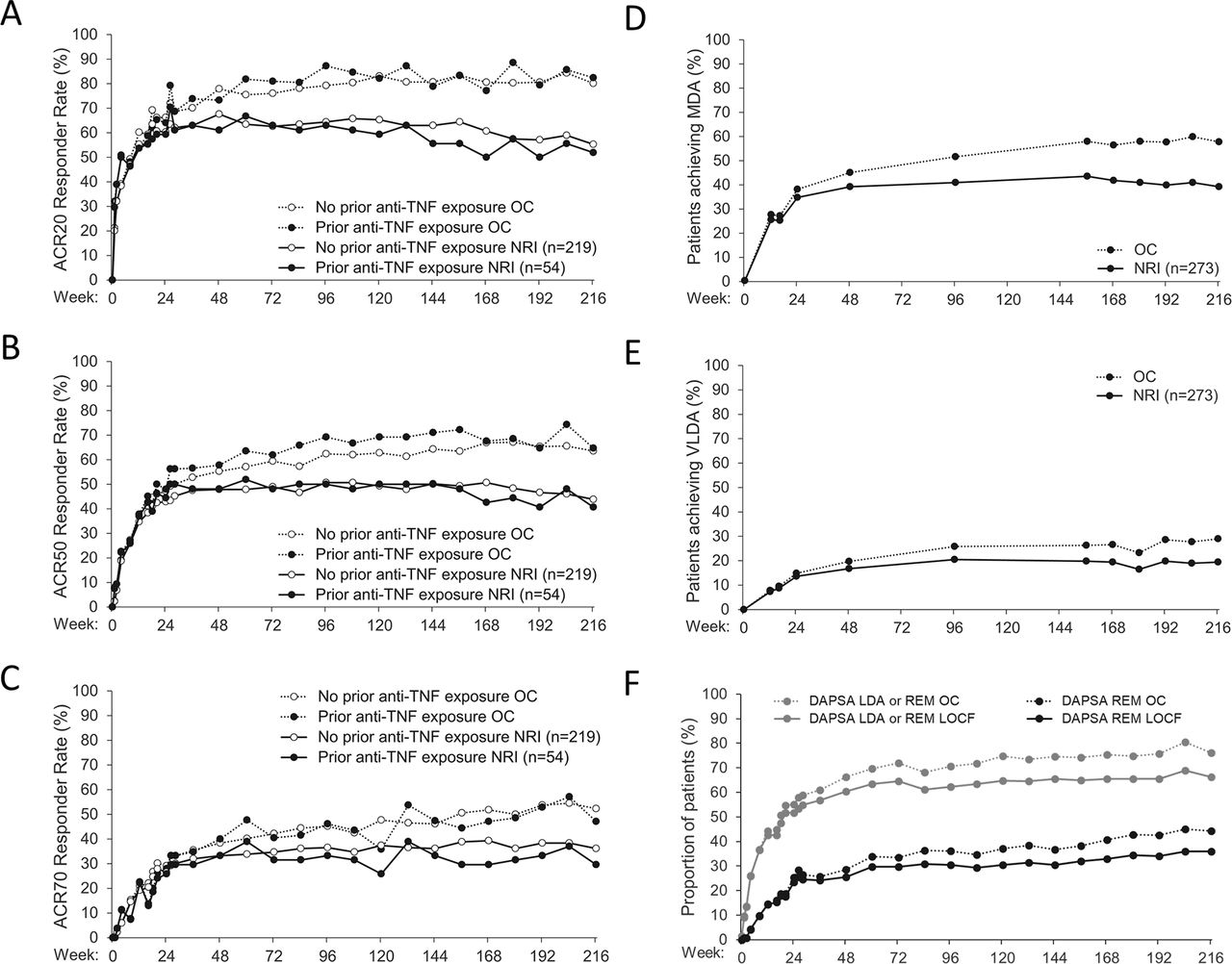
ACR responder rates in patients receiving CZP from Week 0, stratified by prior anti-TNF exposure (A−C) and the proportion of patients receiving CZP from Week 0 achieving MDA (fulfilling ≥5/7 MDA criteria) (D), VLDA (fulfilling 7/7 MDA criteria) (E) and DAPSA LDA (>4 and ≤14) or remission (≤4) (F) over 4 years’ CZP treatment. Data are shown for the Randomised Set. ACR20/50/70: 20%, 50% and 70% or greater improvement in ACR score. ACR, American College of Rheumatology; CZP, certolizumab pegol; DAPSA, Disease Activity Index for Psoriatic Arthritis; LDA, low disease activity; LOCF, last observation carried forward; MDA, minimal disease activity; NRI, non-responder imputation; OC, observed case; REM, remission; TNF, tumour necrosis factor; VLDA, very low disease activity.
Improvements in disease activity in patients initially randomised to CZP, assessed by evaluating the number of patients achieving MDA and VLDA (which include joint and skin disease components and PROs20) and the patients’ DAPSA (a disease activity index based on peripheral joint disease, global activity, pain, and CRP levels12), were maintained from Week 24 to Week 216 (table 1 and figure 2). Of patients completing 4 years’ CZP treatment, 29% achieved VLDA, more than half achieved MDA and more than 75% achieved either DAPSA remission or DAPSA LDA (table 1 and figure 2D–F).
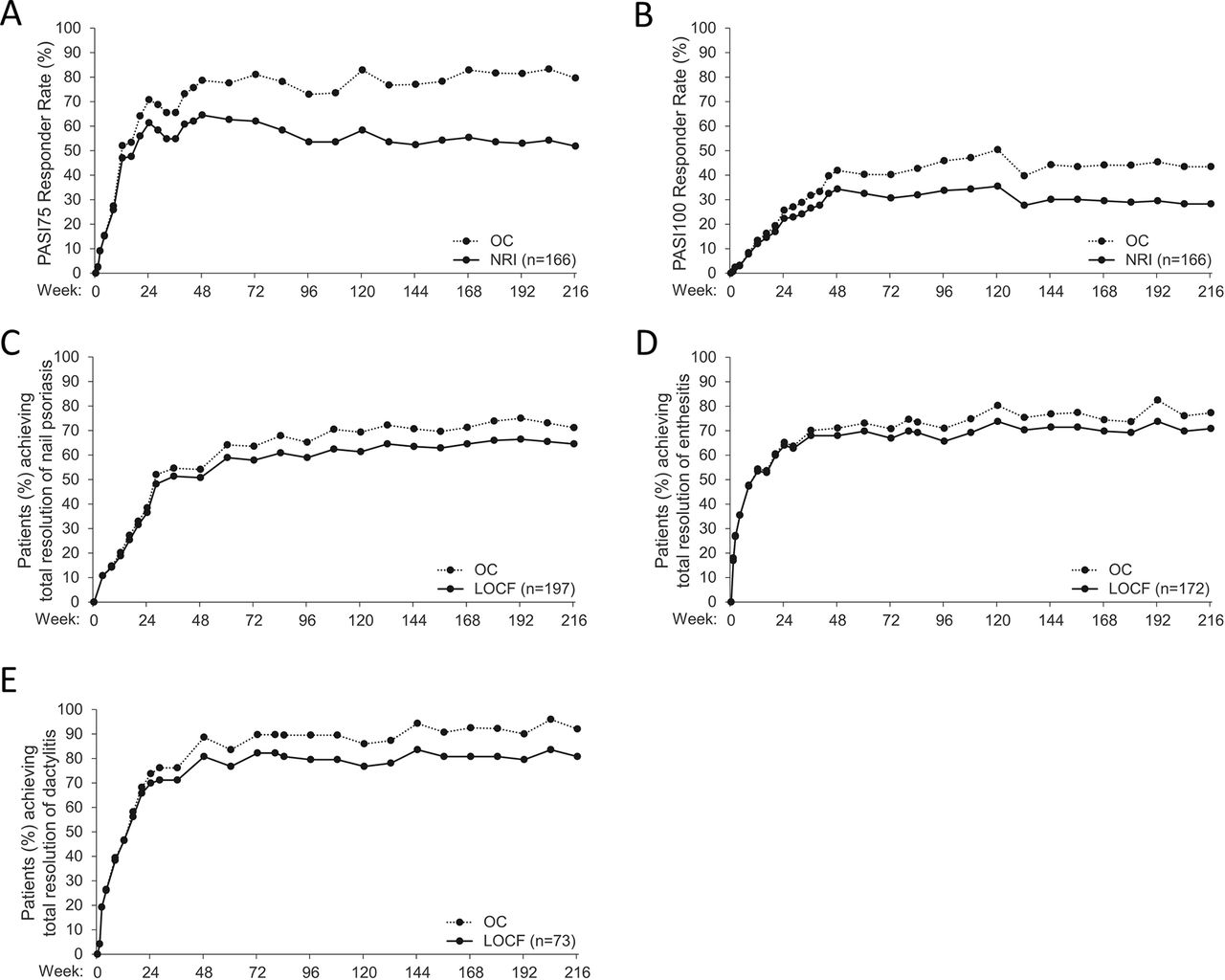
Among patients with skin involvement (≥3% BSA) at baseline, improvements in psoriasis were generally maintained from the end of the double-blind phase at Week 24 to Week 216, with more than half achieving 75% reduction in PASI and BSA ≤1% at 4 years (figure 3A–B and table 1). Improvements in psoriasis were also similar in patients with and without prior anti-TNF exposure (online supplementary figure 2D and online supplementary figure 3D). As expected, greater PASI75 and PASI100 responder rates were observed and sustained in patients with more severe skin involvement at baseline (PASI ≥10 vs PASI <10; online supplementary figure 2E and online supplementary figure 3E).
{kind=link}
{kind=link}
{kind=link}
PASI responder rates (A, B) and total resolution in (C) nail psoriasis, (D) enthesitis and (E) dactylitis in affected patients receiving CZP from Week 0, over 4 years’ treatment. Data are shown for the Randomised Set. PASI responder rates are given for patients with baseline skin involvement (≥3% body surface area affected by psoriasis). Total resolution rates for nail psoriasis, enthesitis and dactylitis are presented for patients affected by the respective conditions at baseline, respectively defined as modified Nail Psoriasis Severity Index >0 for nail psoriasis; Leeds Enthesitis Index >0 for enthesitis and Leeds Dactylitis Index >0, defined as having at least 1 digit affected and with a difference in circumference ≥10% compared with the opposite digit, for dactylitis. CZP, certolizumab pegol; LOCF, last observation carried forward; NRI, non-responder imputation; OC, observed case; PASI, Psoriasis Area and Severity Index.
For patients with enthesitis, dactylitis or nail psoriasis at baseline, previously reported improvements achieved by Week 24 in LEI, LDI and mNAPSI, respectively, were maintained to Week 216 (table 1). More than two-thirds of patients treated with CZP, with baseline involvement of dactylitis, enthesitis and nail psoriasis, went on to achieve total resolution of their respective conditions over 4 years (table 1 and figure 3C–E).
Radiographic assessments showed minimal structural joint damage progression in patients treated with CZP from Week 0 to Week 216 (table 2) and in patients originally randomised to placebo, who were re-randomised to CZP at Week 16 or 24 (online supplementary table 5). Patients with baseline mTSS greater than the median baseline score (with more severe disease than those with a baseline mTSS less than the median) also had slightly higher levels of change in mTSS from baseline to Week 216, though progression in structural joint damage remained low in both subgroups (online supplementary table 6).
Structural joint damage in patients randomised to CZP treatment at Week 0
For all measured PROs – HAQ-DI, pain, fatigue, PsAQoL, SF-36 PCS and SF-36 MCS – early improvements observed at Week 24 were generally maintained or further improved at Week 216 (table 1). The most notable improvement was in pain, which improved by more than 50% by Week 216.
Improvements in the signs and symptoms of PsA in patients treated with CZP over 4 years, by all measures evaluated in this study, were similar irrespective of CZP dose regimen, and when patients randomised to CZP at Week 0 were evaluated together with patients re-randomised from placebo to CZP at Week 16 or 24 (online supplementary figures 1–3 and online supplementary tables 2–6).
Safety
Total exposure to CZP in RAPID-PsA was 1320.8 PY. TEAEs occurred in 367 patients (93.4%, ER=257.9 per 100 PY), the majority of which were mild or moderate. Severe TEAEs as classified by the investigator were reported in 71 patients (18.1%). Serious TEAEs occurred in 100 patients (25.4%, ER=11.9 per 100 PY), and in 27 cases (6.9%), this led to permanent withdrawal. The most common serious TEAEs reported were in the ‘Infections and Infestations’, and ‘Musculoskeletal and Connective Tissue Disorders’ SOCs (table 3). The safety profile of CZP was similar for both dosing regimens.
Treatment-emergent adverse events for all patients treated with CZP during the combined double-blind, dose-blind and open-label periods of RAPID-PsA
Of the 23 infections considered to be serious, the most common was pneumonia, with four cases reported; there were no confirmed cases of active tuberculosis. Fifty-four (13.7%) patients experienced a TEAE leading to withdrawal from the study. During the study, a total of 10 patients (2.5%) had a serious cardiac disorder and 7 patients (1.8%) had a malignancy table 3. There were 3 reports of breast cancer and single reports of lymphoma, metastatic gastrointestinal cancer, ovarian cancer and cervix carcinoma stage 0. No cases of uveitis or suicidality were reported as TEAEs in this study.
Six deaths occurred during the study, two in the double-blind period, one in the dose-blind period and three in the OL period between 48 and 96 weeks, which have all been reported previously (two cardiac disorders, one sudden death, one infection, one case each of breast cancer and lymphoma).7 No further deaths were reported, and no new safety signal was identified from Week 96 to Week 216.
Discussion
Two-thirds of the patients originally randomised to CZP in the RAPID-PsA trial completed the 4-year study. CZP demonstrated long-term efficacy in achieving improvement in disease activity in most of the major disease domains of PsA; for most patients completing the trial, CZP treatment demonstrated sustained efficacy in improving joint disease, skin and nail psoriasis, enthesitis and dactylitis, by all disease activity and PRO measures assessed, which was similar with both 200 mg Q2W and 400 mg Q4W dose regimens. The study has shown CZP to have a safety profile that is expected for this therapeutic class, with the most frequent serious TEAEs being infections; no new safety signals have been identified since the Week 96 report of RAPID-PsA.7
More than 7 in every 10 patients with PsA completing 4 years' CZP treatment (and 6/10 of the intention-to-treat population) achieved DAPSA remission or DAPSA LDA, which relate to improvements in peripheral joint disease and patient reported outcomes. An international taskforce of physicians and patients recently developed recommendations for treatment targets in PsA; they acknowledged that DAPSA remission may be difficult to achieve in patients with long-standing disease, for whom they recommend MDA be used as a treatment target.21 Almost 60% of patients completing 4 years’ CZP treatment had achieved MDA (≥5/7 MDA criteria), and half of those also achieved the most stringent target of VLDA (7/7 MDA criteria) indicating that CZP can deliver low disease activity with respect to articular disease, skin disease, pain, function and PROs, for a substantial proportion of patients.
There is overlap between the DAPSA and MDA/VLDA treatment targets; however, the latter also includes the domain of skin disease. There are diverse opinions regarding whether it is better to assess skin separately (in addition to the DAPSA) or as part of the composite outcome (such as the MDA/VLDA).22 Psoriasis is a cause of frustration and embarrassment in many patients with PsA that adds substantially to their burden of disease and lessens their quality of life.23 24 CZP demonstrated sustained efficacy in improving psoriatic skin disease, with more than half of the intention-to-treat population in RAPID-PsA with BSA ≥3% at baseline having achieved BSA ≤1% at Week 216.
Nail psoriasis, dactylitis and enthesitis also contribute significantly to the impact of disease on patients’ quality of life.25 RAPID-PsA has demonstrated the sustained, long-term efficacy of CZP in improving these symptoms of PsA, with more than 6 in every 10 patients with baseline involvement achieving total resolution of nail psoriasis, dactylitis and enthesitis.
PROs are important components in the evaluation of disease impact and therapy response in patients with PsA. The current study showed that patients treated with CZP reported improvements for all PROs measured. The largest improvement was in pain, which improved by more than 50%. Structural joint damage in PsA has been associated with disease activity and severity26 and often correlates with functional impairment.4 There was minimal progression of structural joint damage in patients with PsA treated with CZP, as measured by mTSS, throughout the 4 years of the RAPID-PsA trial, even in patients with more severe structural joint damage at baseline. The Week 216 radiographic results indicated that the proportion of patients treated with CZP over 4 years with structural joint damage non-progression from CZP baseline remained high. Except for CZP and golimumab, such long-term structural joint damage progression data have not been reported for other anti-TNFs or other biological DMARDs (targeting interleukin-12/17/23) and targeted synthetic DMARDs (phosphodiesterase type 4 inhibitors) approved for the treatment of PsA. Notably, the MMRM analysis used in this study to estimate radiographic progression assumed that the mTSS of patients who withdrew from the study would have been statistically similar to other patients receiving the same dose regimen and who had a similar observed mTSS at baseline, had they remained in the study—an assumption that cannot be verified based on the available data.
In patients who do not respond adequately to their first biological DMARD, the GRAPPA and European League Against Rheumatism treatment guidelines for PsA both recommend switching to a second biological DMARD; including the option to switch between anti-TNFs.5 21 A head-to-head trial of CZP and the anti-TNF adalimumab in patients with rheumatoid arthritis recently demonstrated the efficacy and safety of switching to a second anti-TNF after primary failure to an initial anti-TNF.27 In this study of CZP in patients with PsA, although only around 1 in 5 had previously been treated with an anti-TNF, the efficacy of CZP was similar in patients both with and without prior anti-TNF exposure, indicating that CZP may be effective in patients who do not respond adequately to their first biological DMARD.
The limitations of the RAPID-PsA study include the lack of a placebo control beyond Week 24 and inherent bias in having dose-blind and OL periods, when the patient is aware that they are receiving active treatment, as is their physician. As is true for all clinical trials, patient withdrawal from the study also introduces a risk of bias in the data, and the impact of patient withdrawal is likely to be greater in a long-term study. Imputation of the missing data that results from patient withdrawal helps to conserve the validity of the analyses, but also requires assumptions to be made about the measurements that patients would have had if they had remained in the study. Here, we have reported both observed and imputed data to minimise the risk of bias. Another limitation of clinical trials is that while the long-term clinical efficacy and safety data are relevant to clinical practice, the study participants are not completely representative of all patients treated in the clinical practice. In conclusion, the 4-year data demonstrating the efficacy of CZP across most PsA disease domains in the RAPID-PsA study support CZP treatment for the long-term therapeutic management of PsA.
Acknowledgments
The authors thank the patients and their caregivers in addition to the investigators and their teams who contributed to this study. The authors also acknowledge Alvaro Arjona, UCB Pharma, Brussels, Belgium for critical review of the manuscript and Hinal Tanna from Costello Medical Consulting, Cambridge, UK for medical writing and editorial assistance in preparing this manuscript for publication based on the authors’ input and direction.
References
Footnotes
Contributors Substantial contributions to study conception/design or acquisition/analysis/interpretation of data; drafting of the publication or revising it critically for important intellectual content and final approval of the publication: all authors.
Funding All costs associated with the development of this manuscript were funded by UCB Pharma.
Competing interests DvdH has received consulting fees from AbbVie, Amgen, Astellas, AstraZeneca, Bristol-Myers Squibb, Boehringer Ingelheim, Celgene, Daiichi, Eli Lilly, Galapagos, Gilead, Janssen, Merck, Novartis, Pfizer, Regeneron, Roche, Sanofi and UCB Pharma and is the director of Imaging Rheumatology bv. AD has received grants or research support from AbbVie, Amgen, Eli Lilly, GlaxoSmithKline, Janssen, Novartis, Pfizer and UCB Pharma and consulting fees from Eli Lilly, Janssen, Novartis, Pfizer and UCB Pharma. OFG has received grants or research support from AbbVie, Bristol-Myers Squibb, Janssen and Pfizer and consulting fees from AbbVie, Amgen, Celgene, Eli Lilly, Janssen, Pfizer and UCB Pharma and speaker fees from AbbVie, Celgene Janssen, Novartis, Pfizer and UCB Pharma. RF has received grants or research support from AbbVie, Amgen, AstraZeneca, Bristol-Myers Squibb, Celgene, Eli Lilly, Genentech, Janssen, MSD Pharmaceuticals, Novartis, Pfizer, Roche, Sanofi-Aventis and UCB Pharma and consulting fees from AbbVie, Amgen, Bristol-Myers Squibb, Eli Lilly, GlaxoSmithKline, Janssen, Novartis, Pfizer and Sanofi-Aventis. DG has received grants or research support and consulting fees from Abbott, Amgen, Bristol-Myers Squibb, Celgene, Johnson & Johnson, MSD, Novartis, Pfizer and UCB Pharma. ABG has received consulting fees from Abbott (AbbVie), Aclaris, Actelion, Akros, Allergan, Amgen, Amicus, Astellas, Baxalta, Beiersdorf, Bristol-Myers Squibb, Canfite, Catabasis, Celgene, Centocor (Janssen), Coronado, Crescendo Bioscience, CSL Behring Biotherapies for Life, Dermipsor, Dermira, Eli Lilly, Genentech, GlaxoSmithKline, Incyte, Karyopharm, Kineta One, KPI Therapeutics, Meiji Seika Pharma, Mitsubishi, Novartis, Novo Nordisk, Pfizer, Reddy Labs, Takeda, Tanabe Pharma Development America, TEVA, UCB Pharma, Valeant, Vertex and Xenoport and received grants or research support from Incyte and Janssen. BH, LB, OI-S and LP are employees of UCB Pharma. AT has received grants or research support, consulting fees and speaker fees from Abbvie, Eli Lilly, Janssen, Novartis, Pfizer and UCB Pharma. JW has received grants or research support and consulting fees from UCB Pharma. PJM has received consulting fees from AbbVie, Amgen, Bristol-Myers Squibb, Celgene, Janssen, Eli Lilly, Novartis, Pfizer, Sun and UCB Pharma; grants or research support from AbbVie, Amgen, Bristol-Myers Squibb, Celgene, Janssen, Eli Lilly, Merck, Novartis, Pfizer, Sun, UCB Pharma and Zynerba and speaker fees from AbbVie, Amgen, Bristol-Myers Squibb, Celgene, Genentech, Janssen, Novartis, Pfizer and UCB Pharma.
Patient consent Detail has been removed from this case description/these case descriptions to ensure anonymity. The editors and reviewers have seen the detailed information available and are satisfied that the information backs up the case the authors are making.
Ethics approval The study protocol, amendments and subject informed consent were reviewed by a national, regional or Independent Ethics Committee (IEC) or Institutional Review Board (IRB) prior to implementation.
Provenance and peer review Not commissioned; externally peer reviewed.
Correction notice This article has been corrected since it first published.