Article Text

Abstract
Objectives Verinurad (RDEA3170) is a high affinity, selective uric acid transporter (URAT1) inhibitor indevelopment for treating gout and asymptomatic hyperuricaemia. This phase IIa study evaluated the pharmacodynamics, pharmacokinetics and safety of verinurad combined with allopurinol versus allopurinol alone in adults with gout.
Methods Forty-one subjects were randomised into two cohorts of verinurad (2.5–20 mg) plus allopurinol (300 mg once daily) versus allopurinol 300 mg once daily, 600 mg once daily or 300 mg twice daily alone. Each treatment period was 7 days. Serial plasma/serum and urine samples were assayed for verinurad, allopurinol, oxypurinol and uric acid.
Results Serum pharmacodynamic data pooled across cohorts demonstrated maximum per cent decreases in serum urate (sUA) from baseline (Emax) at 7–12 hours after verinurad plus allopurinol treatment. Combination treatment decreased sUA in dose-dependent manner: least-squares means Emax was 47%, 59%, 60%, 67%, 68% and 74% for verinurad doses 2.5, 5, 7.5, 10, 15 and 20 mg plus allopurinol 300 mg once daily, versus 40%, 54% and 54% for allopurinol 300 mg once daily, 600 mg once daily and 300 mg twice daily. Verinurad had no effect on allopurinol plasma pharmacokinetics, but decreased oxypurinol Cmax by 19.0%–32.4% and area under the plasma concentration–time curve from time zero to the last measurable time point by 20.8%–39.2%. Verinurad plus allopurinol was well tolerated with no serious adverse events (AEs), AE-related withdrawals or renal-related events. Laboratory values showed no clinically meaningful changes.
Conclusion Verinurad coadministered with allopurinol produced dose-dependent decreases in sUA. All dose combinations of verinurad and allopurinol were generally well tolerated. These data support continued investigation of oral verinurad in patients with gout.
Trial registration number NCT02498652.
- gout
- pharmacokinetics
- treatment
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Key messages
What is already known about this subject?
Many patients with gout do not achieve their serum urate (sUA)-lowering targets during treatment with a xanthine oxidase inhibitor (XOI), for example, allopurinol or febuxostat, alone.
The pharmacodynamics, pharmacokinetics and safety of verinurad in combination with allopurinol 300 mg once daily have not previously been investigated in subjects with gout in comparison with allopurinol 300 mg once daily, 600 mg once daily or 300 mg twice daily alone.
What does this study add?
Verinurad at doses of 2.5–20 mg in combination with allopurinol 300 mg once daily produced dose-dependent lowering of sUA levels. Verinurad at doses ≥5 mg in combination with allopurinol 300 mg once daily produced greater sUA lowering than allopurinol 600 mg once daily or 300 mg twice daily alone.
Allopurinol 600 mg produced equivalent sUA lowering when administered once or twice daily.
How might this impact on clinical practice?
If approved, verinurad in combination with an XOI may represent an effective treatment option in patients with gout who have an incomplete response to an XOI alone, providing a greater sUA lowering than dose escalation of XOI.
Introduction
Gout is characterised by the deposition of monosodium urate crystals in the joints, tendons and other connective tissues, secondary to long-standing hyperuricaemia.1–3 Reducing the concentration of serum urate (sUA) below its saturation point leads, over time, to the dissolution of crystals and the alleviation of gout symptoms.4 5 To achieve this goal, patients typically require long-term urate-lowering therapy (ULT) in addition to lifestyle and dietary changes.
Current ULTs can be grouped by their mechanism of sUA reduction: the xanthine oxidase inhibitors (XOIs) allopurinol and febuxostat reduce urate production, while the uricosuric agents probenecid, benzbromarone, sulfinpyrazone and lesinurad increase renal excretion of uric acid by inhibiting its reabsorption.3 Finally, the injectable uricases—for use in patients with severe tophaceous gout— enzymatically degrade uric acid to allantoin.6
Allopurinol is the most widely prescribed first-line ULT for gout. Dosing recommendations for allopurinol are to start at ≤100 mg/day to reduce the risk of allopurinol hypersensitivity syndrome and to titrate in 100 mg/day increments every 2–4 weeks while monitoring sUA to achieve and maintain a target sUA of <6 mg/dL (or <5 mg/dL in patients with severe gout symptoms).7 8 Allopurinol is approved at a daily dose up to 800 mg (USA) or 900 mg (Europe), although in practice few patients receive more than 300 mg,9 in part due to physicians’ concerns over the safety of higher doses.10 The majority of patients fail to achieve their target sUA on allopurinol monotherapy.9 10 For these patients, guidelines recommend switching to febuxostat monotherapy or combining treatments with complementary mechanisms of action, such as an XOI with a uricosuric agent.5 7
Lesinurad is a uricosuric agent approved in combination with allopurinol or febuxostat for the treatment of hyperuricaemia associated with gout in patients failing to achieve target sUA on an XOI alone.11–13 In the phase III clinical development programme, treatment with lesinurad at 200 mg and 400 mg doses in combination with febuxostat resulted in more patients achieving target sUA and experiencing reduction in overall tophus area compared with febuxostat alone.12 Neither the lesinurad 200 mg nor 400 mg dose combinations significantly reduced gout flares versus febuxostat alone at 12 months; however, the 400 mg combination did trend lower. The 400 mg lesinurad dose was associated with increased renal adverse effects (compared with lesinurad 200 mg plus febuxostat or febuxostat alone) and was neither submitted to, nor approved by, US and European regulatory agencies.
The clinical trial experience with ULTs demonstrates that more precipitous and increased lowering of sUA below target levels may lead to improved outcomes (eg, lower gout flare incidence, more rapid tophus area reduction).14–18
Verinurad, a next-generation uric acid transporter (URAT1) inhibitor, demonstrates high potency in inhibiting URAT1.19 Verinurad at doses as low as 2.5 mg produces significant sUA lowering in humans,20–22 and this significant dose-dependent reduction in sUA may lead to improved outcomes and medical benefits for patients with gout. As observed for other uricosurics, verinurad monotherapy has been associated with elevated concentrations of urinary uric acid and instances of serum creatinine (sCr) elevation.20 ,22 XOIs, by contrast, are known to reduce urinary uric acid excretion by inhibiting urate production23 and the combination of an XOI with verinurad has been shown to maintain pretreatment levels of urinary uric acid excretion.24 Coadministration of an XOI with verinurad may therefore mitigate the renal effects of verinurad monotherapy, while lowering sUA to a greater extent than with either agent alone at the same dose.
Verinurad studies in healthy volunteers show that ~64% of a single oral 10 mg dose is absorbed, with a median time to maximum observed plasma concentration (Tmax) of 0.5 hours and a terminal half-life of 15 hours.25
The current study evaluated the pharmacodynamics (PD), pharmacokinetics (PK) and safety of multiple doses of verinurad in combination with allopurinol compared with allopurinol monotherapy in adults with gout (NCT02498652). The doses of allopurinol monotherapy investigated included 300 mg once daily, 600 mg once daily and 300 mg twice a day. In addition to investigating dose combinations of verinurad with allopurinol, this study therefore provides a direct comparison of the PD of allopurinol 600 mg when administered once or twice daily.
Methods
Subjects
This phase IIa, randomised, open label, multicentre study investigated subjects with a diagnosis of gout according to American Rheumatism Association Criteria.26 Subjects were required to be aged ≥18 and ≤75 years with a body weight ≥50 kg, body mass index (BMI) ≥18 to ≤45 kg/m2, sUA ≥8 mg/dL and estimated sCr clearance ≥60 mL/min calculated by the Cockcroft-Gault formula using ideal body weight.
The study was conducted in compliance with Good Clinical Practice and the Declaration of Helsinki. Subjects provided informed consent to participate in the study. The study was performed from July to November 2015.
Study design
Two cohorts of subjects were randomised by incomplete block design to one of eight treatment sequences that included allopurinol (300 mg once daily) in combination with varying verinurad doses (Cohort 1: 2.5–15 mg, Cohort 2: 5–20 mg) or allopurinol 300 mg once daily, 600 mg once daily or 300 twice daily alone. Randomisation used a centralised Interactive Web Response System that generated a unique randomisation number for each subject. Treatment sequences were randomised to avoid a ‘sequence effect’ (figure 1). Each treatment period was 7 days, which combined a period for washing out the previous treatment and for stabilising the new treatment.
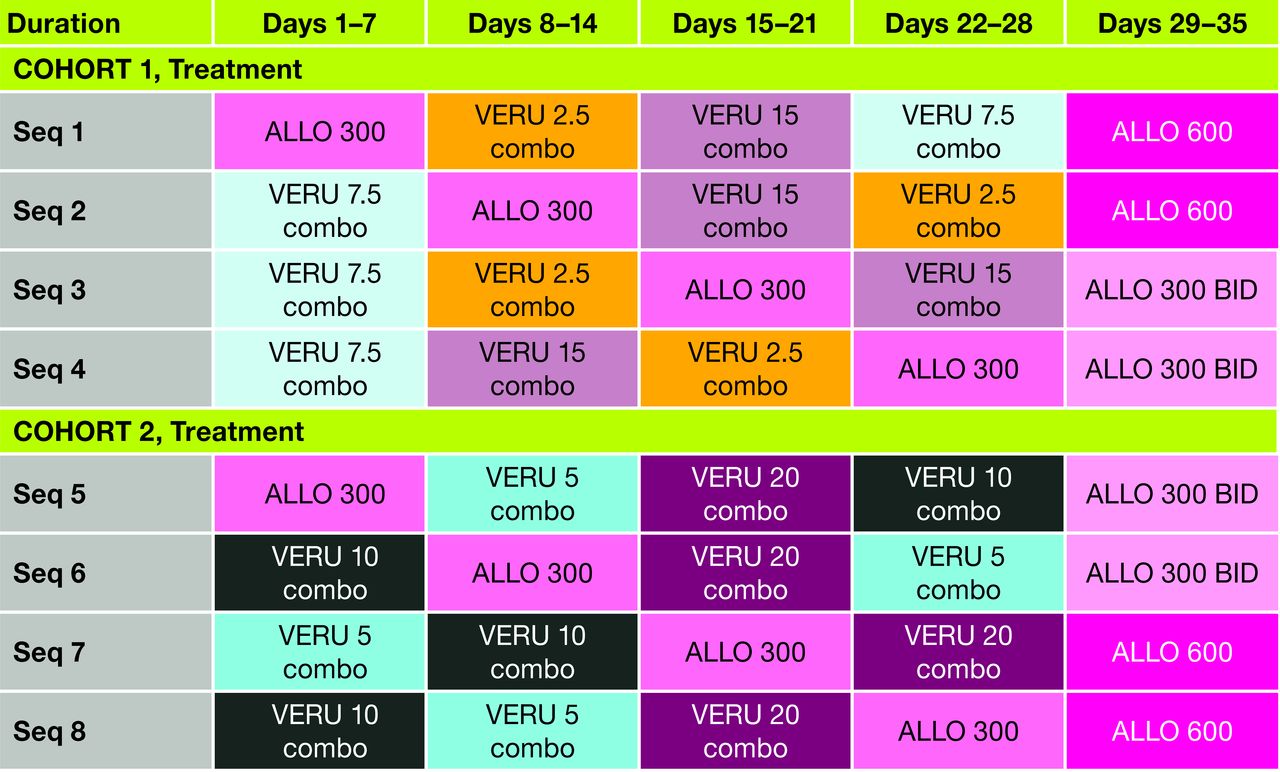
Study design. ALLO 300, allopurinol 300 mg once daily; VERU×combo, verinurad×mg combination with ALLO 300 mg once daily; ALLO 600, allopurinol 600 mg once daily; ALLO 300 BID, allopurinol 300 mg twice daily.
Subjects on prior ULT were started on colchicine 0.6 mg for gout flare prophylaxis at the beginning of ULT washout on approximately day −14. Subjects not on ULT started colchicine on approximately day −7. Verinurad and allopurinol 300 mg once daily or 600 mg once daily were administered approximately 30 min after a standardised breakfast (approximately 650 kcal and 35% fat). For allopurinol 300 mg BID, the second allopurinol dose was given in the evening after a meal, approximately 10 hours after the first dose.
Blood and urine sampling
Serum samples for PD analyses were collected at screening and at frequent preset intervals on baseline (day −1) and days 7, 14, 21, 28 and 35. Serial blood samples for PK analyses were collected on days 7, 14, 21, 28 and 35. Plasma was isolated from the blood by centrifugation. Urine samples (total catch) for PD and PK analyses were collected at 1 hour intervals rising to 2-hour or 10-hour intervals. Baseline sUA and sCr concentrations were assessed on day −2.
On PD/PK urine collection days, subjects were instructed to drink 240 mL of water immediately on waking (within 2 hours predose) to maintain their urine output. Study medication was administered with another 240 mL of water. After dosing, subjects were instructed to drink ~160 mL of water per hour for the next 12 hours with an additional 240 mL at 22 hours.
Analytical methods
Verinurad, allopurinol and oxypurinol concentrations in plasma and urine were measured by Ardea Biosciences (San Diego, California, USA). Plasma samples were extracted by protein precipitation and analytes quantified by high-performance liquid chromatography–mass spectrometry/mass spectrometry (LC-MS/MS) detection, while urine samples were prepared by dilution with water and quantified by high-performance LC-MS/MS.22 24
Assay performance information is included in the online Supplementary file 1.
Supplementary file 1
End points and determinations
All subjects who received at least one dose of verinurad or allopurinol with evaluable PD or PK data were included in the PD and PK populations. All subjects who received at least one dose of verinurad or allopurinol made up the safety population.
The primary study objective was an assessment of the multiple-dose PD of verinurad in combination with allopurinol compared with allopurinol alone. The PD of allopurinol 600 mg once daily versus 300 mg twice daily was additionally compared. Planned PD parameters included maximum per cent change in sUA from baseline (Emax), mean time-matched per cent change in sUA from baseline (day −1), rate of urinary uric acid excretion, renal clearance of uric acid and fractional excretion of uric acid for each 24-hour collection period.
For PD analyses, a mixed-effects model was used on Emax, with sequence and treatment as fixed effects, subject as a random effect and baseline value as a covariate. The least-squares means for each treatment group and between-treatment differences, along with 95% CIs and P values were estimated for each cohort. All statistical testing was conducted at an alpha level of 0.05. No adjustments were made for multiple comparisons. For summary statistics, data were pooled across cohorts according to allopurinol treatment. PD data were collected by Covance Central Laboratory Services (Indianapolis, Indiana, USA) and analyses were performed using SAS V.9.3 or later.
PK assessments investigated the dose proportionality of verinurad 2.5–20 mg in the presence of allopurinol 300 mg and the comparative PK of allopurinol 300 mg twice daily versus 600 mg once daily, using a power model in Phoenix WinNonlin software V.6.3 (Pharsight Corporation, Mountain View, California, USA). PK parameters for verinurad, allopurinol and oxypurinol (the main metabolite of allopurinol) included maximum observed plasma concentration (Cmax), Tmax, area under the plasma concentration–time curve from time zero to 24 hours postdose (AUC0–24) and from time zero to the last measurable time point (AUClast), plasma terminal half-life (t½), amount excreted in urine (Ae0–24), fraction excreted in urine as unchanged drug or metabolite (fe0–24) and renal clearance from time zero to 24 hours postdose (CLR0–24).
For PK analyses, a mixed-effects model was used on AUClast or AUC0–24, Cmax and CLR0–24, with treatment (allopurinol in the presence of verinurad vs allopurinol alone) as a fixed effect and subject as a random effect. Geometric mean (90% CI) PK parameters of allopurinol and oxypurinol are presented in the presence of varying verinurad doses versus allopurinol 300 mg once daily alone. Additionally, a fixed-effect analysis of variance model was used to compare the Cmax and AUC0–24 of allopurinol and oxypurinol between the two parallel allopurinol dose groups (allopurinol 600 mg once daily vs 300 mg twice daily). In the twice daily regimen, AUC0–24 values for allopurinol or oxypurinol were extrapolated based on concentration profiles following the morning dose (estimated as 2×AUC0–12). PK analyses were conducted by Ardea Biosciences, using Phoenix WinNonlin V.6.3.
Subjects were monitored for safety throughout the study and at follow-up on day 49 (±2). Safety assessments included adverse events (AEs) coded according to the Medical Dictionary for Regulatory Activities (V.17.0), clinical laboratory evaluations, vital signs, electrocardiograms and physical examinations. AEs were defined as serious if they resulted in death, were life threatening, required hospitalisation or prolongation of existing hospitalisation or caused persistent or significant disability/incapacity. Any renal serious AEs were to be reviewed by a Renal Events Adjudication Committee appointed by the study sponsor during conduct of the verinurad clinical studies. Any haematology, chemistry or urinalysis abnormalities considered clinically relevant were to be assigned a severity rating by the investigator, based on Rheumatology Common Toxicity Criteria V.2.0, 2007.27 Safety data are summarised by descriptive statistics using SAS V.9.3 or later.
Results
Subjects
A total of 41 subjects were randomised to treatment in one of the two cohorts (n=20, Cohort 1; n=21, Cohort 2). Forty subjects completed the study as per protocol. One randomised subject in Cohort 2 was withdrawn because of non-compliance/protocol violation.
The demographic and baseline characteristics of the subjects are summarised in table 1. Forty subjects were male and the majority (75.6%) were white. Mean age, weight and body mass index (BMI) were similar between the cohorts. The overall mean (SD) sUA at baseline was 9.1 (1.17) mg/dL.
Demographic characteristics and serum urate levels
Pharmacodynamics
The time course of mean per cent change in sUA from baseline (time matched) is shown in figure 2. The mean time to Emax ranged from 7 to 12 hours postdose for each treatment. Verinurad (2.5–20 mg) combined with allopurinol 300 mg once daily decreased Emax in a dose-dependent manner (figure 3). Least-squares mean Emax was 47%, 59%, 60%, 67%, 68% and 74%, respectively, for verinurad doses of 2.5, 5, 7.5, 10, 15 and 20 mg in combination with allopurinol 300 mg once daily, versus 40%, 54% and 54% for allopurinol 300 mg once daily, allopurinol 600 mg once daily and allopurinol 300 mg twice daily alone. Verinurad at all doses combined with allopurinol 300 mg once daily produced significantly greater Emax than allopurinol 300 mg alone, while verinurad doses ≥5 mg combined with allopurinol 300 mg once daily produced greater Emax than allopurinol 600 mg once daily or 300 mg twice daily alone (P<0.05, all comparisons within each cohort). Allopurinol 600 mg once daily was equivalent to allopurinol 300 twice daily in Emax (figure 3).
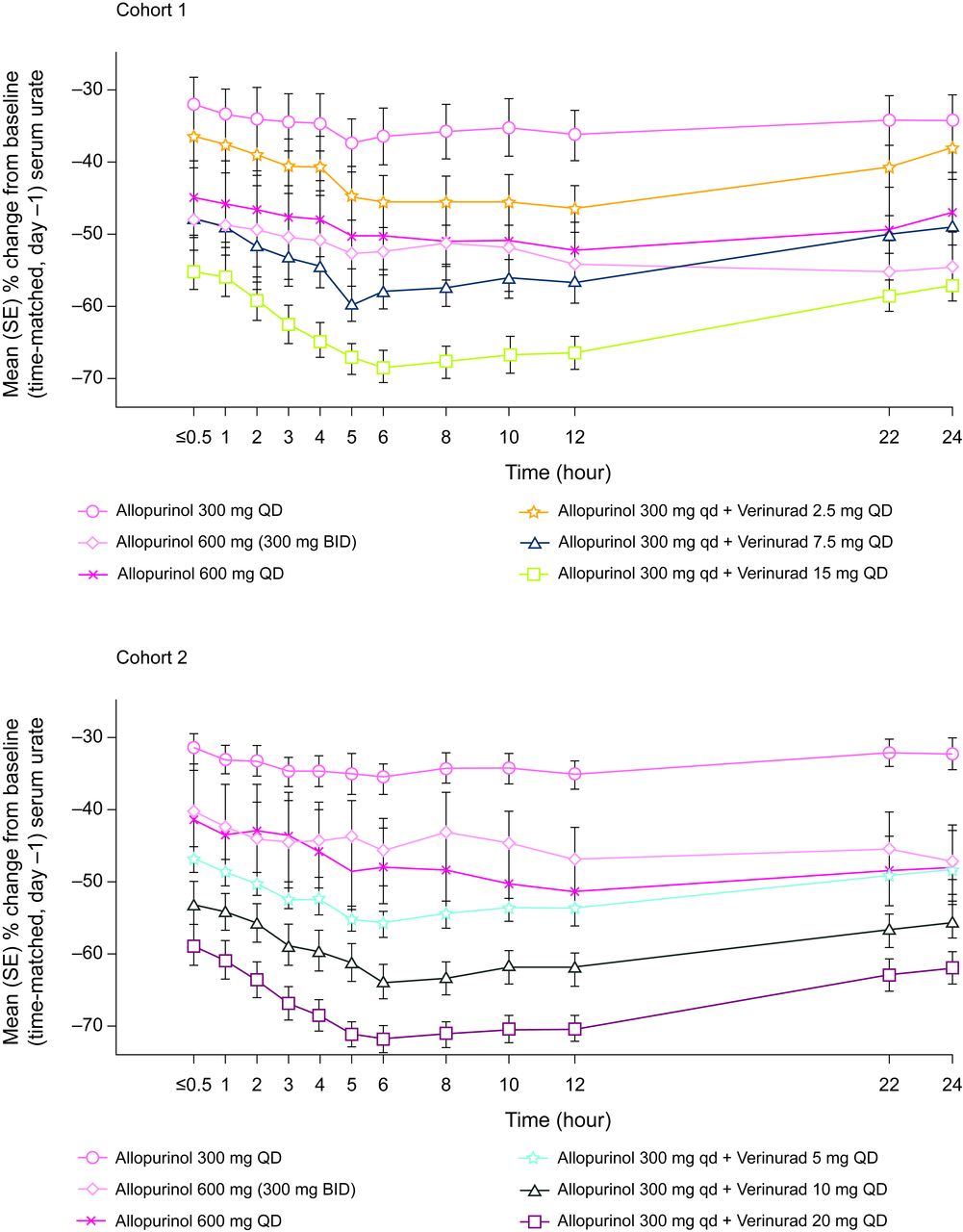
Mean (SE) per cent change from baseline in serum urate (mg/dL) following once-daily oral administration of varying verinurad doses in combination with allopurinol 300 mg once daily versus allopurinol 300 mg once daily, 300 mg twice daily or 600 mg once daily alone.

{kind=link}
{kind=link}
{kind=link}
Maximum mean (SE) per cent change in serum urate from baseline (Emax) following once-daily oral administration of varying verinurad doses in combination with allopurinol 300 mg versus allopurinol 300 mg once daily, 600 mg once daily or 300 mg twice daily alone (allopurinol data pooled across cohorts).
Because of difficulty with the storage conditions of the urinary PD samples, urinary uric acid PD parameters could not be determined accurately and are therefore not reported.
Pharmacokinetics
Mean plasma concentration profiles of verinurad in combination with allopurinol are shown in figure 1 in the online Supplementary file 2. The median Tmax of verinurad ranged from 3.00 to 3.97 hours and the mean t½ ranged from 9.4 to 20.0 hours postdose for varying doses of verinurad in combination with allopurinol 300 mg once daily (table 2). Increases in verinurad Cmax and AUC were dose dependent (table 2; figure 1 in the online Supplementary file 2).
Supplementary file 2
![[rmdopen-2017-000584-SP2.jpg]](https://rmdopen.bmj.com/content/rmdopen/4/1/e000584/DC2/embed/inline-supplementary-material-2.jpg?download=true){kind=link}
Plasma and urine pharmacokinetics of verinurad following once-daily oral administration of varying verinurad doses in combination with allopurinol 300 mg once daily (geometric means, 95% CIs)
Verinurad did not affect the plasma PK of allopurinol, but dose dependently reduced oxypurinol Cmax by 19.0%–32.4% and AUClast by 20.8%–39.2% (table 3). Allopurinol administered as a single 600 mg dose produced comparable AUCs to divided 300 mg doses for allopurinol (least-squares geometric mean ratios (90% CIs): 204 (162 to 257) for Cmax and 128 (101 to 162) for AUC0–24) and oxypurinol (122 (103 to 146) and 115 (93.0 to 143), respectively).
Plasma and urine pharmacokinetics of allopurinol and oxypurinol following once-daily oral administration of varying verinurad doses in combination with allopurinol 300 mg once daily (geometric means and geometric least-squares mean ratios, 95% CIs)
Urinary drug concentration measurements were not affected by the storage conditions. Verinurad Ae0–24 increased with verinurad dose in combination with allopurinol 300 mg once daily, from 17.8 µg at 2.5 mg verinurad to 165 µg at 20 mg verinurad. Verinurad fe0–24 ranged from 0.63% to 0.87% (table 2) and CLR0–24 from 8 to 11 mL/min.
Allopurinol Ae0–24 and CLR0–24 were generally unchanged by verinurad at any dose, while oxypurinol Ae increased by 5%–29% and CLR by 32%–101% with increasing verinurad doses relative to allopurinol 300 mg once daily alone (table 3).
Safety
Twelve subjects reported 23 treatment-emergent AEs (TEAEs). The most common individual TEAEs (in >5% of subjects) in the combined cohorts were upper respiratory tract infection (n=4 subjects, 9.8%) and headache (n=3, 7.3%).
No TEAEs led to study withdrawal. During follow-up, one subject experienced a serious AE of aspiration pneumonia and acute renal failure that was attributed to dehydration following alcohol inebriation and vomiting.
No clinically meaningful changes in laboratory values or vital signs were observed, including no cases of sCr elevation ≥1.5×baseline.
Discussion
Verinurad is a potent, selective inhibitor of the URAT1 transporter in clinical development for the treatment of gout and asymptomatic hyperuricaemia. In this phase IIa study of 41 subjects with gout and baseline sUA ≥8 mg/dL, verinurad (2.5–20 mg) in combination with allopurinol 300 mg reduced sUA in a dose-dependent manner. Verinurad at doses ≥2.5 mg in combination with allopurinol 300 mg once daily produced greater sUA lowering than allopurinol 300 mg once daily alone, while verinurad ≥5 mg in combination with allopurinol 300 mg once daily lowered sUA more than allopurinol 600 mg alone (once daily or twice daily), thereby demonstrating a greater PD effect for combination therapy than allopurinol dose escalation. These observations are consistent with phase Ib studies of lesinurad (another URAT1 inhibitor) in combination with an XOI in patients with gout, where combination therapy also produced greater sUA lowering than an increased dose of XOI.28
The current study also compared the plasma PD and PK of allopurinol 600 mg when given once daily or twice daily. The AUC and sUA-lowering efficacy of allopurinol were comparable for once daily and twice daily administration, suggesting that the extent of sUA lowering is attributable to AUC rather than Cmax. This short-term study adds to the limited data on allopurinol dosing and indicates that, based on PD effects, it may not be necessary to divide daily doses above 300 mg, as currently recommended in the prescribing information for allopurinol.
Urinary PD parameters were not assessed in this study due to improper storage conditions for urinary uric acid. However, the effects of verinurad on urinary excretion of uric acid have been characterised elsewhere: in a phase I, drug–drug interaction study in human volunteers and in a phase IIa, open-label study of verinurad combined with febuxostat in subjects with gout, the verinurad and XOI combination was associated with urinary uric acid excretion levels at or below baseline levels,21 29 in support of the contention that XOI-mediated reductions in urinary uric acid will offset elevations in urinary uric acid associated with uricosuric agents.
Verinurad plasma exposures increased dose proportionally with increasing doses. Verinurad did not influence the PK of allopurinol (in contrast with Hall et al24), but did lower oxypurinol plasma exposure, most likely via inhibition of URAT1 and increased urinary oxypurinol excretion.30 It is notable that lesinurad and benzbromarone (other URAT inhibitors) in combination with allopurinol also lower oxypurinol plasma exposure.31 32 Despite the effect of verinurad on oxypurinol PK, it should be emphasised that the verinurad and allopurinol combination produced significantly greater sUA lowering than allopurinol alone.
All dose combinations of verinurad and allopurinol were generally well tolerated, with no serious AEs or renal-related events and no clinically meaningful changes in laboratory evaluations during treatment.
Limitations of the study include the short study duration, the inclusion of subjects with high mean sUA levels (>9 mg/dL) at baseline and the failure to obtain urinary uric acid data. Strengths of the study include the frequent blood samplings that increased the reliability of the PD and PK analyses, the inclusion of subjects with gout to ensure clinical relevance and the randomisation design that eliminated sequence effects.
In conclusion, oral verinurad at the doses studied (2.5–20 mg) in combination with allopurinol 300 mg once daily produced significantly greater sUA lowering than allopurinol 300 mg once daily alone in subjects with gout. Verinurad at doses ≥5 mg combined with allopurinol 300 mg once daily also produced significantly greater sUA lowering than allopurinol 600 mg alone, indicative of greater efficacy for this combination than for allopurinol dose escalation. All dose combinations of verinurad and allopurinol were generally safe and well tolerated, with no instances of sCr elevation. These data support continued investigation of oral verinurad in a dual-mechanism approach to lowering sUA.
Acknowledgments
Editorial support for this manuscript was provided by Bill Wolvey of PAREXEL, which was funded by AstraZeneca.
References
Footnotes
Contributors All the authors contributed to the acquisition, analysis, interpretation of data for the work, drafting the work or revising it critically for important intellectual content and final approval of the version to be published. JNM, JH and MG were involved in the conception and design of the work
Funding Funding for this study was provided by Ardea Biosciences/AstraZeneca.
Competing interests RF received a clinical study grant from Ardea Biosciences. PW is a full-time employee of Anaheim Clinical Trials. JNM, XY, LH, SV, JH, SL and ZS are/were full-time employees of Ardea Biosciences, a member of the AstraZeneca Group. MG is a full-time employee of AstraZeneca. MHI reports no conflict of interest.
Patient consent Obtained.
Ethics approval Schulman Associates IRB, Cincinnati, Ohio, USA.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement De-identified patient data from this study are made available for scientific research on a case by case basis through AstraZeneca’s Data Request Portal: https://astrazenecagroup-dt.pharmacm.com//DT/Home/Index/