Article Text

Abstract
Objectives To compare outcomes of targeted treatment aimed at either low disease activity or remission in patients with early active rheumatoid arthritis (RA).
Methods Five-year outcomes were compared in 133 patients with early active RA (1987), starting with methotrexate, sulfasalazine and tapered high dose of prednisone (arm 3 of the BehandelStrategieën (Treatment Strategies for Rheumatoid Arthritis) (BeSt) study), targeted at Disease Activity Score (DAS) ≤2.4 (low disease activity), and 175 patients with early RA, starting methotrexate and tapered high dose of prednisone, targeted at DAS <1.6 (selected from IMPROVED study who would have fulfilled inclusion criteria of the BeSt study). Association of treatment target with outcomes DAS <1.6, Boolean remission at year 1 and drug-free DAS remission (DFR) at year 5 were analysed by logistic regression analysis.
Results At baseline, DAS <1.6 steered patients had a milder disease than DAS ≤2.4 steered patients (mean DAS 4.1±SD 0.7vs4.4±0.9, p=0.012) and less radiological damage. DAS decrease, functional ability and radiological damage progression over time were similar in both patient groups. DAS ≤2.4 was achieved in similar percentages in both patient groups, but more DAS <1.6 steered patients achieved DAS <1.6 and DFR. DAS <1.6 steered treatment was associated with achieving DAS <1.6 (OR 3.04 (95% CI 1.64 to 5.62)) and Boolean remission (3.03 (1.45 to 6.33)) at year 1 and DFR at year 5 (3.77 (1.51 to 9.43)).
Conclusions In patients with early active RA who start with comparable disease-modifying antirheumatic drug+prednisone combination therapy, subsequent DAS <1.6 steered treatment is associated with similar clinical and radiological outcomes over time as DAS ≤2.4 steered treatment; however, in the DAS <1.6 steered group, more patients achieved remission and drug-free remission.
- rheumatoid arthritis
- treatment
- remission
- disease activity score
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Key messages
What is already known about this subject?
The optimal treatment strategy to suppress disease activity in early arthritis patients is initial combination therapy followed by targeted treatment.
It is recommended to set the treatment target at Disease Activity Score (DAS) remission or at least at low disease activity, but which is the best target is unknown.
What does this study add?
Compared with a target of low disease activity, a target of DAS remission results in more remission and drug-free remission but not significantly better function.
How might this impact on clinical practice?
Aiming at a target of DAS remission in patients with early active RA may be the preferred treatment target, which offers more patients the option to successfully taper and stop antirheumatic medication.
Introduction
Initial combination therapy followed by targeted treatment is the optimal treatment strategy to suppress disease activity in early arthritis patients.1–6 Treat-to-target therapy has been introduced in clinical trials and implemented in daily practice; however, the optimal treatment target is under discussion, and head-to-head comparisons are lacking. International recommendations state that treatment should be steered at achieving remission (Disease Activity Score (DAS) <1.6) or at least low disease activity (DAS <2.4).7 Instinctively, remission appears the optimal treatment target, as this is associated with better functional ability and less damage progression.4 6 However, this association may be a coinciding, not a causal relationship. To proceed with further treatment adjustments aiming at remission when low disease activity is achieved may not bring additional clinical benefits but additional costs and risks for side effects. This may explain an earlier observation that adherence to a protocol where the treatment target is DAS remission is less compared with a protocol where the treatment target is low disease activity.8
We aimed to investigate whether targeted treatment aimed at DAS remission results in better outcomes than targeted treatment aimed at low disease activity in patients with early rheumatoid arthritis (RA). Therefore, we compared two treat-to-target studies: the Behandel Strategieën (Treatment Strategies for Rheumatoid Arthritis) (BeSt) study with treatment target DAS ≤2.4, selecting patients in arm 3 who started on a high tapered dose of prednisone with methotrexate and sulfasalazine (SSZ), and the Induction therapy with methotrexate and Prednisone in Rheumatoid Or Very Early arthritic Disease (IMPROVED) study, with treatment target DAS <1.6, where patients started on a high tapered dose of prednisone with methotrexate, selecting patients who would have fulfilled the inclusion criteria of the BeSt study.
Patients and methods
BeSt study
The BeSt study (NTR262, NTR 265 (Dutch trial registry)) was a multicentre, randomised clinical trial and introduced treat-to-target therapy in 20 hospitals in the Netherlands in the year 2000. Five hundred and eight patients with early (≤2 years symptom duration) active (≥6 of 66 swollen joints, ≥6 of 68 tender joints and either erythrocyte sedimentation rate (ESR) ≥28 mm/hour or a visual analogue scale (VAS) global health score ≥20 mm)3 RA according to the American College of Rheumatology (ACR) 1987 classification criteria9 were randomised to four treatment strategies. Patients were treated to target every 3 months aiming at low disease activity (DAS ≤2.4). Treatment was intensified (supplementary figure 1) as long as DAS >2.4 but tapered when DAS was ≤2.4 for at least six consecutive months. From year 3, patients who had tapered to low dose single disease-modifying antirheumatic drug (DMARD) and were in DAS remission (DAS <1.6) for at least six consecutive months stopped treatment to achieve drug-free DAS remission (DFR).
Supplementary file 2
IMPROVED study
The IMPROVED study (ISRCTN Register number 11916566 and EudraCT number 2006 06186-16) was a multicentre, randomised clinical trial that started in 2007 in most of the hospitals that also participated in the BeSt study. Six hundred and ten patients with early (≤2 years symptom duration) RA according to the 2010 ACR and European League Against Rheumatism (EULAR) classification criteria10 or with undifferentiated arthritis were included. All received initial treatment with methotrexate (MTX) 25 mg/week and a tapered high dose of prednisone (tapered from 60 mg/day to 7.5 mg/day in 7 weeks) for 4 months.6 Patients were treated to target every 4 months aiming at DAS remission (<1.6).11 Patients who achieved early DAS remission at 4 months tapered and stopped prednisone, followed by MTX if DAS remission persisted at 8 months (supplementary figure 2). DFR could be achieved no sooner than at year 1. Patients who did not achieve DAS remission at 4 months were randomised to arm 1 (MTX 25 mg/week, prednisone 7.5 mg/day, SSZ 2000 mg/day and hydroxychloroquine 400 mg/day) or arm 2 (MTX 25 mg/week and adalimumab 40 mg/2 weeks).4
Current study design
To be able to compare the treatment targets in these studies, we selected patients from both studies who had comparable initial treatment and comparable baseline disease characteristics. Thus, for the current intention-to-treat analysis, we selected 133 patients from the BeSt study who were randomised to arm 3, initially treated with prednisone (tapered in 7 weeks from 60 mg/day to 7.5 mg/day) and MTX 7.5 mg/week (increased to 25 mg/week if DAS after 3 months was >2.4) and SSZ 2000mg/day. These patients will be called the ‘DAS ≤2.4 steered group’. From the IMPROVED study, 175 RA (1987) patients who fulfilled the inclusion criteria of the BeSt study were selected. These patients will be called the ‘DAS <1.6 steered group’.
All patients gave written informed consent. More details of the BeSt study and the IMPROVED study were published elsewhere.3–6
Outcomes
Outcomes were DAS, change in DAS, functional ability assessed by the Dutch Health Assessment Questionnaire (HAQ (13)), low disease activity percentages, DAS remission percentages and DFR percentages, compared at year 1 and year 5. In addition, ACR/EULAR (Boolean) remission12 (tender joint count (TJC) ≤1, swollen joint count (SJC) ≤1, C reactive protein (mg/dL) ≤1 and VAS global health (0–10 scale) ≤1) and radiological damage progression (based on baseline and annual radiographs of hands and feet), scored using the Sharp/van der Heijde score (SHS)13 were compared. The BeSt study was scored in random order, and the IMPROVED study in chronological order by two independent readers blinded for patient identity and allocation. For the analysis, the means of the two readers for each study (IMM and GA for the BeSt study and GA and SAB for the IMPROVED study) were calculated. Damage progression after 1 and 5 years was defined by ≥0.5-point increase from baseline.
Statistical analyses
Between-group differences were analysed by Student’s t-tests, Mann-Whitney U tests and χ2 tests. Associations of treatment target (DAS ≤2.4 or DAS <1.6) with DAS <1.6, Boolean remission at year 1 and DFR at year 5 were analysed by logistic regression analysis. The multivariable model was corrected for baseline differences (DAS, symptom duration and total SHS) between the studies, time on antitumour necrosis factor (anti-TNF) inhibitor and other variables with a p value of <0.2. Statistical analyses were performed with SPSS for Windows V.23.0.
Results
Baseline characteristics
At baseline, all selected patients fulfilled the inclusion criteria of the BeSt study. Patients in the DAS <1.6 steered group had a significantly shorter symptom duration (median 17 (IQR 8–28) weeks vs 23 (15–53) (DAS ≤2.4), p<0.001) and lower DAS (mean 4.1±SD 0.7 vs 4.4±0.9, p=0.012) compared with the DAS ≤2.4 steered group (table 1). This was due to a lower TJC and lower SJC in the DAS <1.6 steered group, whereas ESR were comparable. VAS global health was statistically higher in the DAS <1.6 steered group. Furthermore, SHS at baseline was significantly higher in the DAS ≤2.4 steered group compared with the DAS <1.6 steered group (median (IQR)/mean±SD 1.5 (0–3)/2.8±3.8 vs 0 (0–3)/1.8±2.9, p=0.004). Other baseline characteristics were comparable between the two groups.
Baseline characteristics in DAS ≤2.4 steered (BeSt) and DAS <1.6 steered (IMPROVED) patients
Early response
After 3 months in the DAS≤2.4 steered group, the DAS was decreased by two points to mean (SD) 2.4±1.0 and HAQ was decreased by 0.8 point to 0.6±0.6 (table 2 and figure 1A,B). The target of DAS ≤2.4 was achieved by 75/133 (56%) of the patients and 27/133 (20%) of the patients were in DAS remission (table 2 and figure 1C). In the DAS <1.6 steered group at 4 months, DAS had decreased by (mean) 2.4 to 1.8±SD 1.0 and HAQ by 1 point to 0.5±0.6 (table 2 and figure 1A,B). The target of DAS remission was achieved by 92/175 (53%) of the patients (table 2 and figure 1C). Patients in DAS remission started tapering medication, while 64 patients (37%) not in DAS remission at 4 months were randomised: 30 patients to arm 1 and 34 patients to arm 2. Of these, 25/64 (39%) had DAS ≤2.4. Seventeen patients (10%) who did not achieve early DAS remission were not randomised and were treated outside of protocol. At 4 months, 126/175 (72%) had DAS ≤2.4. There were two patients who left the study before the evaluation at 4 months.
Clinical outcomes in DAS ≤2.4 steered (BeSt) and DAS <1.6 steered (IMPROVED) patients
![[rmdopen-2018-000649-SP2.jpg]](https://rmdopen.bmj.com/content/rmdopen/4/1/e000649/DC1/embed/inline-supplementary-material-1.jpg?download=true){kind=link}
{kind=link}
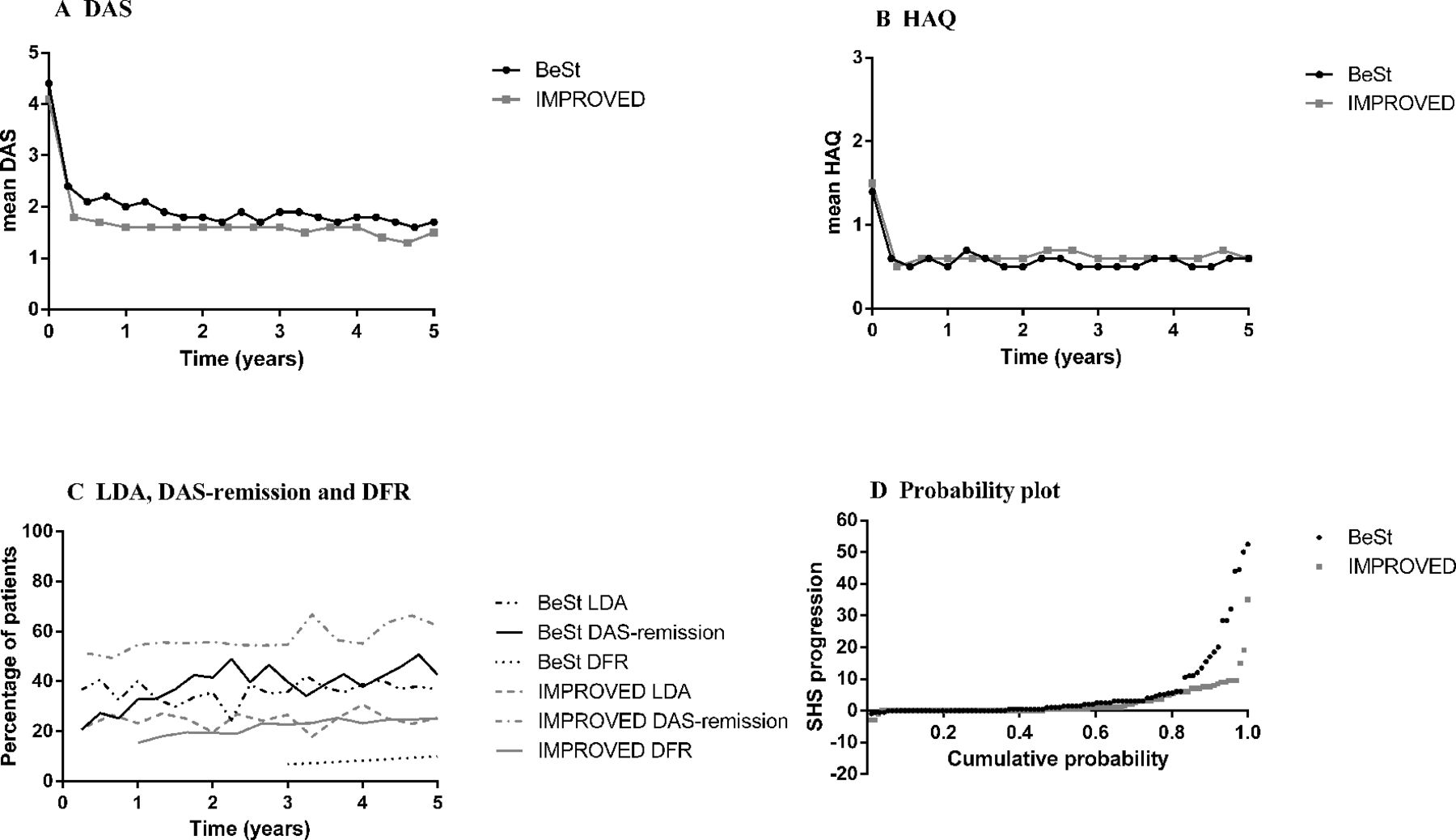
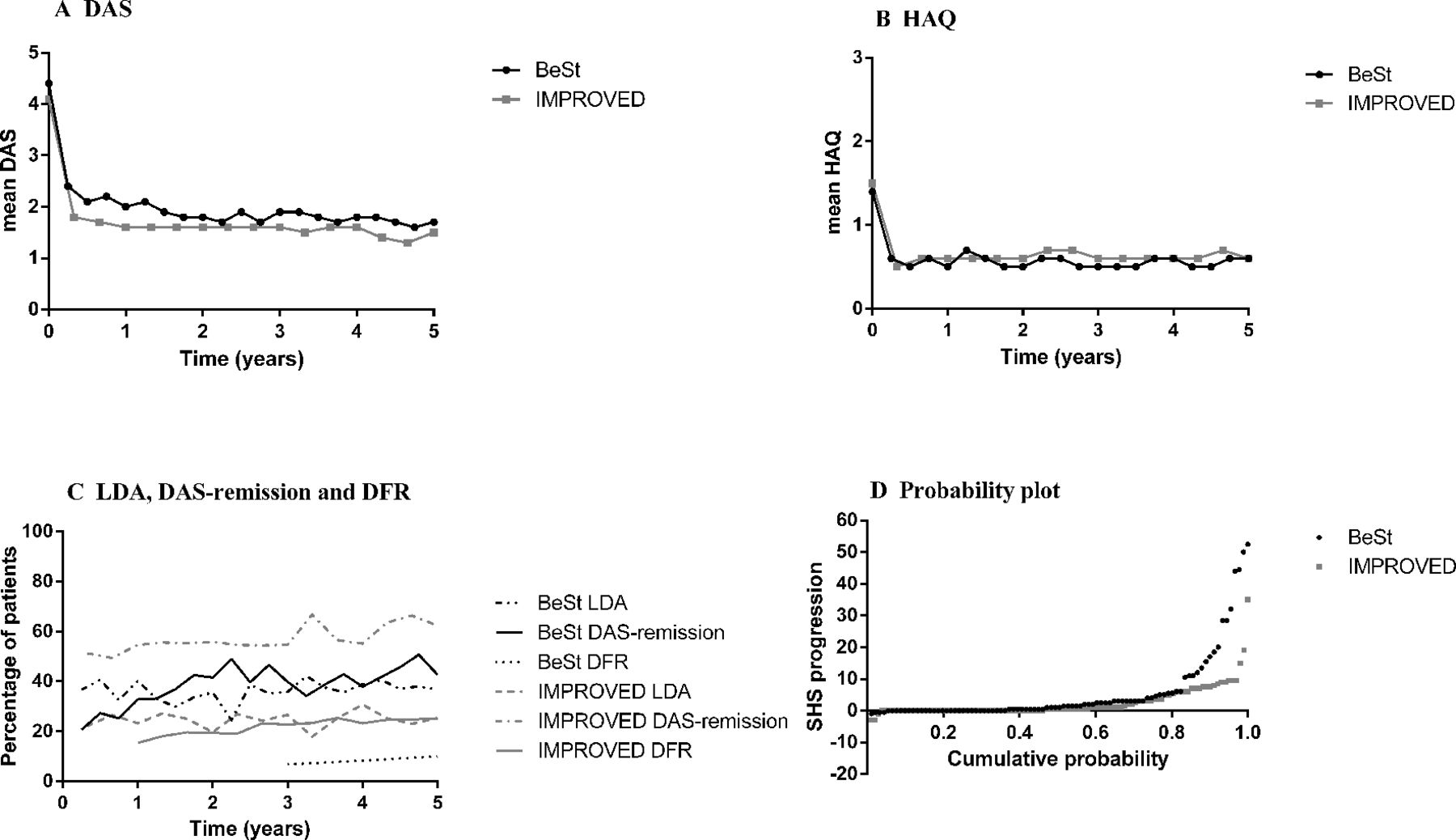
Mean DAS (A), HAQ (B) and percentages in low disease activity, DAS remission and drug-free DAS remission (C) during 5 years in the DAS ≤2.4 steered (BeSt) patients and the DAS <1.6 steered (IMPROVED) patients and probability plot with radiological damage progression after 5 years (D). (D) Each patient depicted by a dot, ordered along the x-axis from low to high progression scores with individual scores on the y-axis. BeSt, Behandel Strategieën (Treatment Strategies for Rheumatoid Arthritis); DAS, Disease Activity Score; DAS remission, DAS <1.6; DFR, drug-free DAS remission; HAQ, Health Assessment Questionnaire; IMPROVED, Induction therapy with methotrexate and Prednisone in Rheumatoid Or Very Early arthritic Disease; LDA, low disease activity DAS ≥1.6–≤2.4; SHS, Sharp/van der Heijde Score; SHS progression, ≥0.5 points increase after 5 years.
At year 1, DAS had decreased similarly in both studies: from baseline by 2.4 in the DAS ≤2.4 steered group to 2.0±0.9 and from baseline by 2.5 (p=0.445) in the DAS <1.6 steered group to 1.6±1.0 (p=0.004) (table 2 and figure 1A). Functional ability at year 1 was comparable in both groups (0.5±0.5 (DAS ≤2.4) and 0.6±0.6 (DAS <1.6), p=0.148) (table 2 and figure 1B). Similar percentages of patients in both studies achieved DAS ≤2.4, but more patients in the DAS <1.6 steered group than patients in the DAS ≤2.4 steered group had achieved DAS remission (51% vs 30%, p<0.001) (table 2 and figure 1C) and Boolean remission (26% vs 16%, p=0.004), and 15% in the DAS <1.6 steered group by year 1 were in DFR. By protocol, patients in the DAS ≤2.4 steered group could not achieve DFR at year 1. Ninety-three of 133 (70%) patients in the DAS ≤2.4 steered group were still on the initial treatment step due to achieving the treatment target. At year 1, SHS progression was similar in both groups (median (IQR) 0 (0–1), mean (SD) 0.9±2.3 in the DAS ≤2.4 steered group and 0 (0–0)/0.4±1.6 in the DAS <1.6 steered group, p=0.164).
In the univariable regression analysis treatment target (DAS ≤2.4 or DAS <1.6) was associated with DAS remission after 1 year (DAS <1.6 steered group OR 2.47 (95% CI 1.51 to 4.02)) and with Boolean remission after 1 year OR 2.31 (1.30–4.14)) (supplementary table 1). In the multivariable model, after correction for potential confounders, treatment target group remained an independent predictor of DAS remission and Boolean remission, along with time on anti-TNF and (for DAS remission) male gender (table 3).
Supplementary file 1
Multivariable logistic regression analysis with DAS remission at year 1, ACR/EULAR (Boolean) remission at year 1 and drug-free DAS remission at year 5 as binomial outcome variable
Long-term response
At year 5, DAS decreased similarly from baseline in both studies: in the DAS ≤2.4 steered group by 2.6 points to 1.7±0.8 and by 2.7 points (p=0.849) in the DAS <1.6 steered group to 1.5±0.8 (p=0.014). Functional ability was comparable in both groups (table 2). DAS ≤2.4 was achieved in 61% in both groups (p=0.092), but DAS <1.6 was achieved in 32% of the DAS ≤2.4 steered group compared with 43% of the DAS <1.6 steered group (p=0.003), and DFR in 8% versus 18% (p=0.003). Boolean remission was achieved by 11% in the DAS ≤2.4 steered group and 19% in the DAS <1.6 steered group (p=0.069). Sixty of 133 (45%) patients of the DAS ≤2.4 steered group were still on the initial treatment step. Possibly, as a result of the treatment protocol and the stricter treatment target, more patients in the DAS <1.6 steered group used anti-TNF during 5 years compared with the DAS ≤2.4 steered group (82/175 (47%) patients vs 29/133 (22%) patients, respectively, p<0.001), but the median (IQR) time on anti-TNF was shorter in the DAS <1.6 steered group (16 (8–20) months) compared with the DAS ≤2.4 steered group (18 (9–45) months, p=0.011). There was no difference between both studies in rates of SHS progression ≥0.5, but in the BeSt study, higher progression scores were observed. Figure 1D shows the probability plot after 5 years. (Serious) adverse events ((S)AEs) were similar in the DAS <1.6 steered group and DAS ≤2.4 steered group (data not shown).
Treatment target was also associated with DFR after 5 years (DAS <1.6 steered group OR 3.13 (95% CI 1.45 to 6.77)) (supplementary table 1). In the multivariable model treatment target was independently associated with DFR (DAS <1.6 steered group OR 4.50 (1.84–11.03)) after correction for symptom duration, baseline DAS, baseline total SHS and time on TNF inhibitor (table 3).
Discussion
Treat-to-target therapy is effective in patients with RA. It is recommended to set the treatment target at DAS remission or at least at low disease activity. Previous studies4 6 showed that patients who achieved remission had better disease outcomes than patients who achieved low disease activity. However, this association may be multifactorial rather than purely causal. A head-to-head comparison trial might show which is the optimal treatment target. Alternatively, we tried to compare two treat-to-target trials with DAS ≤2.4 or DAS <1.6 as treatment target. We found that treatment target indeed appears to be an independent predictor for short-term (DAS remission) as well as long-term (DFR) disease outcomes. However, functional ability and radiological damage progression rates were similar in both target groups.
Instinctively, we expect treatment-to-target results in more patients achieving the target regardless of its height. However, a target of remission may be more difficult to achieve than low disease activity, and indeed this was seen in this comparison. At the first evaluation of treatment efficacy, similar percentages of patients in both groups had achieved the target (56% of the DAS ≤2.4 targeted group and 53% of the DAS <1.6 targeted group). However, as no treatment adjustments before that time had occurred, this seems coincidental and likely to reflect differences in patient and disease characteristics despite our attempt to select similar patients. At the end of the first year, despite treatment adjustments, in the DAS ≤2.4 steered study, the target was achieved in 67% and in the DAS <1.6 steered study in only 51%. After 5 years, these percentages were 61% and 43%, respectively.
Whether a treatment target is achieved also depends on the therapies used and on patient and disease characteristics. We tried to maximise similarities between the patient groups as well as therapies by comparing patients from the IMPROVED study who could have been included in the BeSt study, with patients from the BeSt study who received treatment comparable with treatment in the IMPROVED study. In addition, differences in baseline DAS and SHS, symptom duration, gender and time on TNF inhibitor were corrected for in the multivariable analysis. In the DAS <1.6 targeted group, baseline DAS (SJC, TJC, but not ESR and VAS global health) was lower than in the DAS ≤2.4 targeted group, symptom duration was shorter and baseline radiological damage was less often present. There were also some differences in initial and subsequent therapy: the DAS <1.6 targeted group started with a higher MTX dose, which was only prescribed to the DAS ≤2.4 targeted group if after 3 months the DAS remained >2.4; however, the DAS <1.6 targeted group did not receive cotreatment with SSZ. We do not expect, but cannot rule out, that these differences in medications have affected the differences in (long-term) disease outcomes. A recent head-to-head comparison study14 has shown that extended combination of prednisolone and MTX with SSZ is not superior to only prednisolone with MTX. Over time, there were also slight differences between both groups: patients who did not achieve the target DAS ≤2.4 were treated with a combination of MTX with ciclosporin-A followed by, if necessary, MTX with infliximab, whereas patients who did not achieve the target DAS <1.6 were randomised to DMARD combination and low dose prednisone, or to MTX with a TNF blocker (adalimumab). After failure on the TNF blocker, a second biological DMARD was allowed in the DAS <1.6 steered patient group but not in the DAS ≤2.4 steered patient group. We found that more patients in the DAS <1.6 steered patient group used a TNF blocker.15 16 Tapering of medication was required in the DAS <1.6 steered patient group more rapidly than in the DAS ≤2.4 steered patient group. Probably as a result, median time on a TNF blocker was shorter in the DAS <1.6 steered patient group. We tried to correct for time on TNF inhibitors in the multivariable regression analysis.
After 1 year, we found that DAS remission was more often achieved in the DAS <1.6 steered group (51%) than in the DAS ≤2.4 steered group (30%). Similar proportions of patients had achieved DAS ≤2.4 (67% in the DAS ≤2.4 steered group and 73% in the DAS <1.6 steered group). Decrease in DAS over time compared with baseline was similar in both groups. Also, functional ability over time was not different between the groups. Furthermore, in both groups, radiological progression after 1 and 5 years was similar. After 5 years, DFR was achieved more often in the DAS <1.6 steered group. The multivariable regression analysis shows that the study origin, as proxy for treatment target, was independently associated with DAS remission, Boolean remission and DFR. It also shows that male patients are more likely to have a favourable disease outcome, as reported before.6 There were no differences in (S)AEs in the DAS <1.6 and DAS ≤2.4 steered groups.
There are several limitations to our study. It is clear that despite similarities between the patient groups, they are from two studies with differences in recruitment period, inclusion criteria, treatment strategies and therapies and evaluation frequencies, all of which may have influenced our outcomes beyond the effect of steering at different treatment targets. We looked only at patients with high disease activity at baseline. For patients with low disease activity, the outcomes might have been different. Another limitation is that these results are only generalisable to tapering schemes and not to step-up schemes that were followed in both studies. Also, ‘study group’ that was used as proxy for treatment strategy may represent more than the treatment targets. We have insufficient details on use of various medications over time in our patient groups and can only speculate that the DAS <1.6 steered group may have tapered medication more often than the DAS ≤2.4 steered group. How this influences our results is unclear. Rapid drug tapering may have resulted in more disease flares; however, it may also have inflated the number of patients in (non-sustained) DFR at various time points. In observational situations, patients who are in (DAS or clinical) remission have less radiological damage progression than patients in low disease activity. However, this may be a coincidental rather than a causal association. Radiological data after 1 year were based on scores by two different teams of independent scorers, although the latter were trained by the former. Also, the scoring method was different in both studies. The BeSt study was scored in random order, and the IMPROVED study was scored chronologically. Patients in the IMPROVED study already started with a milder disease at baseline compared with the BeSt study with lower DAS, shorter symptom duration and less radiological damage at baseline resulting in favourable outcomes at 1 and 5 years. We also have not looked at patient-reported outcomes that may be more relevant to patients in daily life than DAS and HAQ. Finally, we chose DAS remission after 1 year as outcome for the regression analysis, the stricter remission definition Boolean remission at year 1 and DFR as long-term outcome, because it most strongly resembles reversal of disease or ‘cure’. However, DAS remission and Boolean remission at 1 year outcome are inter-related with the treatment strategy in at least one of the groups, and through rules of tapering in both protocols, also DFR is interrelated with the treatment targets.
In conclusion, our comparison between two treat-to-target cohorts suggests that indeed DAS remission may be the better treatment target, as this results in favourable disease outcomes in patients with early active RA and is associated with DAS <1.6 and Boolean remission at year 1 and DFR at year 5. The DAS <1.6 steered patients also had lower DAS over time, but their functional ability (HAQ) over time and radiological progression were similar to that measured in the DAS ≤2.4 steered patients. However, aiming at DAS remission may be more challenging than aiming at low disease activity. Also, the potentially higher costs of continued DAS <1.6 steered treatment may be a factor that needs to be considered when deciding which is the optimal treatment target for each patient.
Supplementary file 3
![[rmdopen-2018-000649-SP3.jpg]](https://rmdopen.bmj.com/content/rmdopen/4/1/e000649/DC3/embed/inline-supplementary-material-3.jpg?download=true){kind=link}
Acknowledgments
We would like to thank all patients for their contribution as well as the following rheumatologists who participated in the BeSt study group and in the IMPROVED-study group: J van Aken (Spaarne Hospital, Hoofddorp); WM de Beus (retired); C Bijkerk (Reinier de Graaf Gasthuis, Delft); MHW de Bois (Medical Center Haaglanden, Leidschendam); H Boom (Spaarne Hospital, Hoofddorp); PDM de Buck (Medical Center Haaglanden, Leidschendam); G Collée (Medical Center Haaglanden, Leidschendam); BAC Dijkmans (retired); JAPM Ewals (retired); F Fodili (Fransiscus Hospital, Roosendaal); AH Gerards (Vlietland Hospital, Schiedam); YPM Goekoop-Ruiterman (Haga Hospital, The Hague); BAM Grillet (Zorgsaam, Terneuzen); KH Han (MCRZ Hospital, Rotterdam); JB Harbers (Franciscus Hospital, Roosendaal); A L Huidekoper (Bronovo Hospital, The Hague); SM van der Kooij (Haga Hospital, The Hague); MV van Krugten (Admiraal de Ruyter Hospital, Vlissingen); LR Lard (Medical Center Haaglanden, Leidschendam); H van der Leeden (retired); MF van Lieshout-Zuidema (Spaarne Hospital, Hoofddorp); A Linssen (retired); MC Lodder (Kennemer Gasthuis, Haarlem); PAHM van der Lubbe (Vlietland Hospital, Schiedam); C Mallée (Kennemer Gasthuis, Haarlem); M van Oosterhout (Groene Hart Hospital, Gouda); AJ Peeters (Reinier de Graaf Gasthuis, Delft); N Riyazi (Haga hospital, The Hague); H K Ronday (Haga Hospital, The Hague); D van Schaardenburg (VU Medical Center, Amsterdam); AA Schouffoer (Haga Hospital, The Hague); PEH Seys (retired); G M Steup – Beekman (Bronovo Hospital, The Hague); PBJ de Sonnaville (Admiraal de Ruyter Hospital, Goes); I Speyer (Bronovo Hospital, The Hague); KSS Steen (Kennemer Gasthuis, Haarlem); JPh Terwiel (retired); AE Voskuyl (VU Medical Center, Amsterdam); ML Westedt (retired); S ten Wolde (Kennemer Gasthuis, Haarlem); D van Zeben (Sint Franciscus Gasthuis, Rotterdam). We would also like to thank all other rheumatologists and trainee rheumatologists who enrolled patients in these studies, and all research nurses for their contributions.
References
Footnotes
Contributors GA performed the statistical analysis, interpreted the data and drafted the manuscript. IMM, SAB, RJG, ETM and JHLMvG contributed in the acquisition of the data and revised the manuscript. PJSMK, WFL and TWJH participated in the study design, contributed in the acquisition of the data and were involved in revising the manuscript. CFA participated in the study design, contributed in the acquisition of the data and was involved in analysing and interpreting the data and helped to draft the manuscript. All authors read and approved the final version of the manuscript.
Funding This work was supported by a government grant from the Dutch Insurance Companies, with additional funding from Schering-Plough B.V. and Janssen B.V for the BeSt-study. The study was designed by the investigators. Data collection, trial management, data analysis and preparation of the manuscript were performed by the authors. The IMPROVED study was designed by the investigators and financially supported by AbbVie in the first year. Trial management, data collection, data analysis and preparation of the manuscript were performed by the authors.
Competing interests None declared.
Patient consent Obtained.
Ethics approval Approval for the BeSt study and the IMPROVED study was given by the Medical Ethics Committees of each participating centre.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement GA had full access to all the data in the study and takes responsibility for the integrity of the data and the accuracy of the data analysis. There is no additional unpublished data from this study.