Article Text

Abstract
Objectives Imaging studies in patients with cutaneous psoriasis have demonstrated asymptomatic bone and tendon changes, commonly of the foot and ankle. We sought to determine if patients with cutaneous psoriasis have an increased risk of clinically significant foot and ankle tendinopathy or enthesopathy compared with the general population.
Methods Patients with cutaneous psoriasis and a general population cohort were identified in The Health Improvement Network, a general practice medical records database from the UK. All patients with psoriatic arthritis were excluded. Cox proportional-hazards models (α=0.05) estimated the HR for development of foot and ankle tendinopathy or enthesopathy among patients with psoriasis, with adjustment for numerous covariates.
Results In total, 78 630 patients with cutaneous psoriasis and 5 983 338 persons from the general population were identified. In an unadjusted model, patients with cutaneous psoriasis had a 25% increased risk of developing foot and ankle tendinopathy or enthesopathy compared with the general population (HR 1.25, 95% CI 1.20 to 1.30, p<0.0001). The HR remained unchanged and statistically significant after adjusting for covariates, and in sensitivity analyses.
Conclusions These data suggest that patients with psoriasis can have foot and ankle tendinopathy or enthesopathy without having psoriatic arthritis, presenting a diagnostic challenge to physicians. Further research is needed to elucidate mechanisms contributing to this increased risk.
- tendinitis
- psoriatic arthritis
- inflammation
- epidemiology
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Key messages
What is already known about this subject?
Imaging studies suggest that many patients with psoriasis have asymptomatic foot and ankle bone and tendon lesions.
What does this study add?
Patients with cutaneous psoriasis had a 25% increased risk of developing tendinopathy or enthesopathy of the foot and ankle.
How might this impact on clinical practice?
Patients with psoriasis may present with foot and ankle tendinopathy or enthesopathy without necessarily having psoriatic arthritis.
Introduction
Psoriasis is an inflammatory skin disease characterised by pruritic, erythematous, scaling plaques, papules and occasionally pustules.1 2 While originally thought to be a disease limited to the skin, recent evidence suggests that systemic consequences occur in psoriasis, such as increased risk of myocardial infarction,3 chronic kidney disease,4 cancer5 and depression.6
From a musculoskeletal perspective, 8%–30% of patients with psoriasis develop psoriatic arthritis,7 8 a chronic inflammatory arthropathy.8 While joint involvement is the main distinguishing feature between psoriatic arthritis and psoriasis, a recognised extra-articular feature of psoriatic arthritis is inflammation of tendons, usually at their insertions or entheses, termed tendinopathy and enthesopathy respectively.8 9 Most commonly, this manifests at the plantar fascia and Achilles tendons,9 causing significant foot and ankle pain and immobility.
Tendon and entheseal involvement is typically considered a feature exclusive to psoriatic arthritis rather than psoriasis. However, recent studies using high-resolution peripheral quantitative CT scans have shown that psoriasis patients without arthritis had significant enthesophyte formation, signalling enthesopathy, compared with healthy controls.10 Moreover, in an MRI study of patients with psoriasis, it was found that 57% had evidence of asymptomatic Achilles tendinopathy.11 On ultrasound imaging, patients with spondyloarthropathy had more frequent enthesopathy in the absence of clinical symptoms compared with healthy controls.12 Thus, it appears that patients with psoriasis may develop pathology consistent with tendon dysfunction, but since these studies were relatively small and without clinical follow-up, it remains unknown whether patients with psoriasis actually experience clinically significant tendon and entheseal disorders at a greater rate than the general population.
In this study, we used The Health Improvement Network (THIN), a general practice medical records database in the UK, to test the hypothesis that psoriasis patients without psoriatic arthritis are at increased risk of developing clinically significant foot and ankle tendinopathy or enthesopathy compared with the general population, thereby identifying a potential extracutaneous manifestation. We focused exclusively on the foot and ankle (a) as these are the most common sites observed for tendon dysfunction in patients with psoriatic arthritis (ie, Achilles tendon and plantar fascia),9 (b) as previous research has shown imaging evidence of disease at these sites in patients with psoriasis11 and (c) to explore the concept of a ‘deep Koebner’ phenomenon, with selection of a site with high mechanical loading offering pathophysiological insight.
Methods
Data source
THIN is an electronic database that contains general practice medical records from the UK with up to 25 years of follow-up.13 Additionally, data from specialists are provided to general practitioners and subsequently recorded in THIN. Given the longitudinal follow-up and detailed medical history data, THIN is ideal for studying potentially low-incidence outcomes such as tendinopathy and enthesopathy among a cohort with psoriasis.
Study population and exposure
THIN was used to identify individuals between the ages of 10–90 years diagnosed with psoriasis (exposure cohort) and those without psoriasis (referent cohort). Diagnosis of psoriasis was based on the presence of one or more validated Read diagnostic codes (linked to International Classification of Diseases codes) for psoriasis.14 Any patient with a psoriasis code within 1 year of registering in THIN was excluded from this study, to ensure that all cases of psoriasis were incident, as done previously.15 Additionally, to ensure focus on cutaneous psoriasis patients without arthritis, any patient with a validated Read code for psoriatic arthritis at any time in their record was excluded from this study.16 Finally, any patients with a Read code for foot and ankle tendinopathy or enthesopathy (main outcome) prior to psoriasis diagnosis were excluded.
The referent cohort (general population) also had a 1-year washout period, and any patient who had a prevalent code for foot and ankle tendinopathy or enthesopathy within this period was excluded from analysis.
Outcomes
All patients were followed until the earliest of (a) development of foot and ankle tendinopathy or enthesopathy (main outcome), (b) transfer out of practice, (c) death or (d) end of data collection period. Patients who did not have a record of tendinopathy or enthesopathy during this follow-up period were censored. Development of foot and ankle tendinopathy or enthesopathy was defined based on the presence of any Read code relating to tendinopathy or enthesopathy of the foot and ankle. Read codes that were determined to relate to foot and ankle tendinopathy and enthesopathy were identified as follows: first, all Read codes relating to tendinopathy or enthesopathy were identified. This list was then reviewed independently by a rheumatologist and orthopaedic surgeon, where consensus was established on which codes would properly capture tendinopathy or enthesopathy specific to the foot and ankle. While enthesitis is the more common outcome for patients with psoriatic arthritis, tendinopathy was included to broaden our definition since this also occurs in psoriatic arthritis.17 Additionally, since clinically defining tendon injury as tendinopathy versus enthesopathy is dependent only on the point along the tendon at which the injury occurs, we considered both terms in our analysis in hopes of improved sensitivity, given not all patients with tendon pain may have imaging to confirm where along the tendon the injury was to classify them as enthesopathy or tendinopathy. Read codes used in our analysis for foot and ankle tendinopathy or enthesopathy can be found in table 1.
Read codes used to define foot and ankle tendinopathy or enthesopathy in this study
Covariates
Age, sex, obesity status (body mass index ≥30 kg/m2), alcohol use (yes or no), smoking status (current, past or never) and socioeconomic status (based on Townsend deprivation index) were determined for all patients in both the psoriasis and referent cohorts. These were taken in closest proximity to the date of diagnosis in the psoriasis cohort and closest to the start date in THIN for the referent cohort, as done previously.15 We also assessed comorbidity burden using Read codes to compute the Charlson comorbidity index within the first three years of the study start date.15
As patients with moderate–severe psoriasis are likely to receive systemic therapy which may mask or treat tendinopathy or enthesopathy, we also recorded use of systemic therapy as a covariate defined based on the presence of any of the following codes, as done previously3 15: acitretin, azathioprine, cyclosporine, etretinate, hydroxycarbamide, methotrexate, mycophenolic acid and phototherapy with or without psoralen. Biologics were not considered as they are poorly recorded in THIN15 16; however, since UK treatment guidelines indicate patients with psoriasis should be started on a disease-modifying antirheumatic drugs prior to any biologic,18 likely these patients would still be captured within our systemic therapy covariate.
Lastly, we included use of systemic steroid medications and use of fluoroquinolones at any point during the study period as covariates as these medications are known to predispose to tendon injury.19–21
Statistical analysis and data presentation
This manuscript was prepared in accordance with the Strengthening the Reporting of Observational Studies in Epidemiology statement.22 Analyses were performed using STATA/MP V.13.1 (α=0.05). Baseline data were compared between the psoriasis and referent cohort using χ2 tests. Cox proportional-hazards models were used to evaluate the risk of foot and ankle tendinopathy or enthesopathy among psoriasis patients compared with the referent cohort, where risk was estimated as an HR with 95% CIs. An omnibus likelihood ratio test was used to assess for statistical interactions between all covariates found to have a significant difference between groups at baseline,15 and no interactions were identified (p=0.189). A backward elimination procedure was then used to evaluate each covariate for possible confounding starting with a fully adjusted model. Ultimately, no variables were found to induce an important change to the HR (ie,>10%) to suggest confounding.15 Data were then presented in both an unadjusted and fully adjusted model. The proportional-hazards assumption was evaluated by testing the Schoenfeld residuals and constructing a log–log plot, and no evidence against this assumption was found.
To further ensure that the psoriasis cohort did not contain individuals likely to develop psoriatic arthritis, a sensitivity analysis was performed that excluded patients who had a code for uveitis, which is known to be a substantial risk factor for psoriatic arthritis in patients with psoriasis.23 In addition, all patients with codes for inflammatory bowel disease or ankylosing spondylitis were removed from consideration to ensure enthesopathy or tendinopathy were not due to these conditions.24 25 To confirm only incident psoriasis cases were included, a sensitivity analysis was performed where patients had to be registered in THIN for at least 5 years before psoriasis diagnosis. Finally, to ensure adequate time was available to develop the outcome of interest, an additional sensitivity analysis was performed that restricted to only patients with at least 5 years of follow-up from their start date in THIN.
Data availability
The data that support the findings of this study are available from IMS Health (UK) but restrictions apply to the availability of these data, which were used under licence for the current study, and so are not publicly available. Data are however available from the authors on reasonable request and with permission of IMS Health.
Results
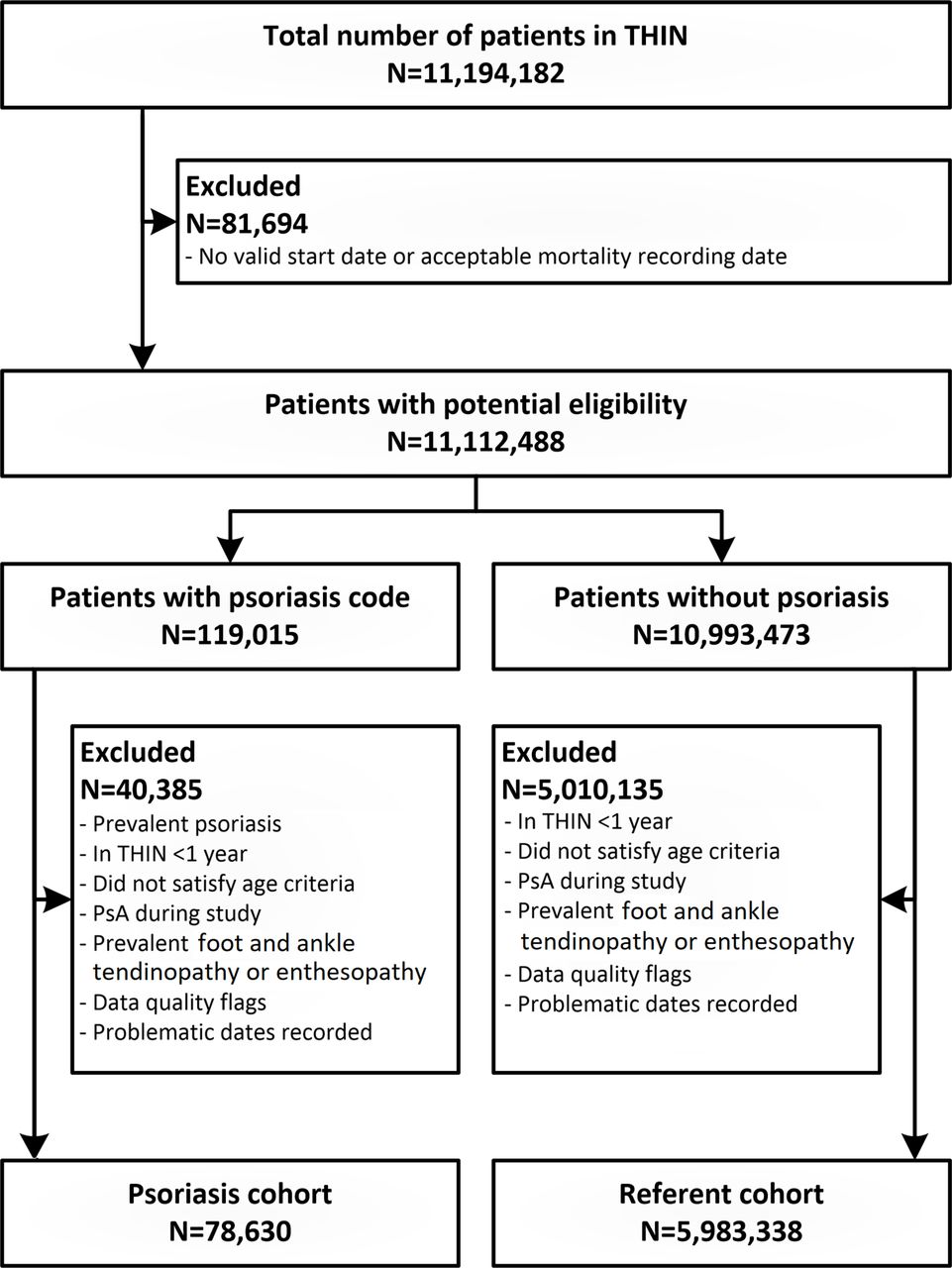
Using THIN, and after ensuring all patients with a code for psoriatic arthritis were removed from consideration, we identified 78 630 patients with cutaneous psoriasis, and a referent cohort comprising 5 983 338 patients (figure 1). At baseline (table 2), the following covariates were found in a greater proportion among the psoriasis cohort: age >40 years, presence of obesity, current smoking, comorbidities, systemic therapy use, systemic steroid use and fluoroquinolone use (all p<0.0001). Conversely, the psoriasis cohort had a lower proportion of individuals who were socioeconomically deprived or alcohol users. Sex distributions were similar between the psoriasis and referent cohorts (p=0.529).
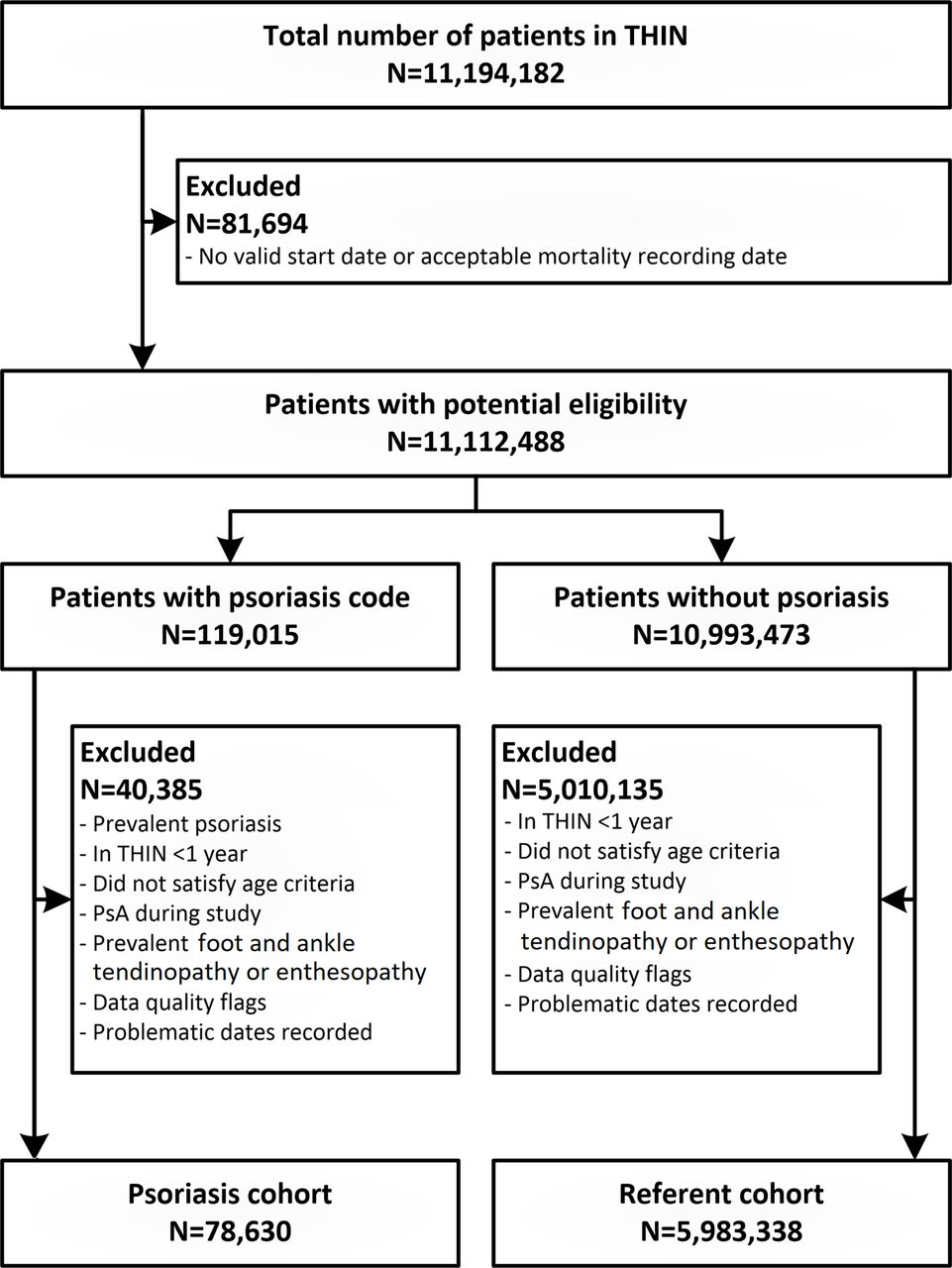
Flow chart showing selection of patients in the psoriasis and general population referent cohort. PsA, psoriatic arthritis; THIN, The Health Improvement Network.
Baseline characteristics of patients with psoriasis and the general population
Follow-up times were up to 26 years, with a median follow-up of 5.1 years (IQR 6.9 years) in the psoriasis cohort and 5.6 years (IQR 7.0 years) in the general population. In total, 2631 patients with psoriasis (3.3%) developed foot and ankle tendinopathy or enthesopathy while 147 919 patients (2.5%) developed foot and ankle tendinopathy or enthesopathy in the general population. The median time to development of foot and ankle tendinopathy or enthesopathy from psoriasis diagnosis was 4.4 years (IQR 5.8 years). Overall, the median age at diagnosis of foot and ankle tendinopathy or enthesopathy was 53.2 years (IQR 21.6 years).
An unadjusted cox proportional-hazards model revealed that patients with psoriasis were at a 25% increased risk of developing foot and ankle tendinopathy or enthesopathy compared with the general population (HR 1.25, 95% CI 1.20 to 1.30, p<0.0001). All covariates that were significantly different between groups at baseline were included in a fully adjusted model, and patients with psoriasis remained at significantly increased risk of foot and ankle tendinopathy or enthesopathy (HR 1.25, 95% CI 1.17 to 1.33, p<0.0001). These models are shown in table 3. Kaplan-Meier failure curves for development of foot and ankle tendinopathy or enthesopathy can be seen in figure 2.

{kind=link}
{kind=link}
Kaplan-Meier failure curve for development of foot and ankle tendinopathy or enthesopathy. Patients with psoriasis (orange) were at a 25% increased risk of foot and ankle tendinopathy or enthesopathy compared with the general population (blue).
HRs for the risk of foot and ankle tendinopathy and enthesopathy
To further ensure we excluded patients with a predisposition to tendinopathy or enthesopathy through other autoimmune processes,23 we performed sensitivity analyses to exclude 42 215 patients with uveitis, inflammatory bowel disease or ankylosing spondylitis. This resulted in 77 326 patients with psoriasis and 5 942 427 patients from the general population analysed. Here, in the fully adjusted model, psoriasis remained a significant risk factor for development of foot and ankle tendinopathy or enthesopathy (HR 1.25, 95% CI 1.17 to 1.34, p<0.0001). Similarly, results remained unchanged when restricting to only those patients with at least 5 years in THIN before psoriasis diagnosis (HR 1.30, 95% CI 1.18 to 1.43, p<0.0001) or when restricting to only those patients who had at least 5 years of follow-up in THIN (HR 1.25, 1.16 to 1.34, p<0.0001).
Discussion
The absolute risk of foot and ankle tendinopathy or enthesopathy was low in both the psoriasis and referent cohorts. Thus, clinically it is important to acknowledge that foot and ankle tendinopathy or enthesopathy is not experienced by a large proportion of patients with psoriasis; however, our finding of a 25% increased risk of foot and ankle tendinopathy or enthesopathy among those with psoriasis may provide important information on the underlying pathophysiology of psoriasis, and add to the growing body of evidence suggestive of systemic pathophysiology in the development and course of psoriasis.
Previous research has shown that patients with psoriasis have imaging findings consistent with tendon dysfunction more frequently than healthy controls.11 Similarly, subclinical enthesitis has been documented in patients with psoriatic arthritis.26 Although some overlap exists in genetic architecture between psoriasis and psoriatic arthritis, each condition and specific disease phenotypes have unique genetic signatures, perhaps accounting for why not all patients with psoriasis develop psoriatic arthritis, or why some patients develop arthritis before psoriasis.27 28 Our study adds to this complex relationship by identifying that patients with psoriasis are at 25% increased risk of being diagnosed with foot and ankle tendinopathy or enthesopathy by a physician compared with the general population. Clinically, this indicates that foot and ankle tendinopathy or enthesopathy is associated with psoriasis and not only psoriatic arthritis. Just as some patients with psoriasis show susceptibility to development of articular or nail symptoms,28 it might also be possible that some patients with psoriasis are at higher susceptibility to tendon or enthesis symptoms, but without joint symptoms to diagnose them as having psoriatic arthritis. Since we excluded all patients with psoriatic arthritis codes in our study, and further excluded those with uveitis, inflammatory bowel disease and ankylosing spondylitis, this poses a clinical challenge to physicians as patients may experience foot and ankle tendinopathy or enthesopathy without necessarily having psoriatic arthritis, leading to uncertainty on the diagnosis or the need for rheumatology consultation.
The diagnosis of psoriatic arthritis is largely clinical since there are no specific genetic, tissue biopsy or serological markers. While many different clinical classification criteria exist for psoriatic arthritis, it should be emphasised that these are simply a means to classify disease phenotypes rather than diagnostic criteria for psoriatic arthritis. On the assumption of patients exclusively having psoriasis without arthritis but with findings of tendinopathy or enthesopathy, many clinical criteria would not classify these patients as having psoriatic arthritis. While it remains possible that a subset of the patients considered in this study had additional features that would classify them as psoriatic arthritis by some criteria, these patients would be expected to evolve over time and eventually be captured and recoded as having psoriatic arthritis in THIN, which we excluded from analysis. Moreover, by exclusion of patients with codes for uveitis, which has been documented as a strong risk factor for future development of psoriatic arthritis,23 by eliminating all patients with inflammatory bowel disease or ankylosing spondylitis from consideration and by restricting to only patients with a long follow-up time in sensitivity analyses, the possibility that remaining patients would subsequently develop joint involvement and psoriatic arthritis is low. Thus, our results more likely represent foot and ankle tendinopathy or enthesopathy in the setting of cutaneous psoriasis rather than psoriatic arthritis. The alternative to this possibility, depending on the classification system chosen, is that these patients simply represent unrecognised cases of psoriatic arthritis; however, this is perhaps less likely based on the sensitivity analyses performed, and on the basis that any misclassification bias would be expected to occur non-differentially between the psoriasis and referent cohorts.
Given that the Achilles tendon and plantar fascia are typically sites of repetitive mechanical loading, the possibility of a biomechanical aetiology in foot and ankle tendinopathy or enthesopathy is strong. It is well documented that repetitive mechanical stress in the Achilles tendon and plantar fascia can alter gene expression, induce local inflammation and tendon degradation,29–31 giving support to the proposed concept of a ‘deep Koebner phenomenon’ in psoriatic disease.10 32 Indeed, it has recently been proposed that mechanical stress may be an important factor contributing to the onset of inflammation and development of spondyloarthritis.33 Moreover, tendon degradation may persist following chronic under loading,29 and interestingly one study involving patients with psoriatic arthritis with active enthesitis did demonstrate reduced Achilles tendon force during gait.34 While it has been suggested that the biomechanical environment of the Achilles tendon and plantar fascia may be dependent on underlying muscle physiology,35–37 musculoskeletal anatomy,35 38 obesity,39 gait abnormalities38 and even footwear,40 41 none of these factors have been assessed in the context of foot and ankle pathology in patients with psoriasis. Therefore, additional research in this area is warranted to understand the potential mechanisms by which patients with psoriasis develop foot and ankle tendinopathy or enthesopathy.
This study has a number of strengths and limitations to consider. First, our use of a large, nationally representative database allowed us to study very large sample sizes over a long period of time. While this gave substantial statistical power, this also led to small differences being statistically significant, and these should be interpreted from a frame of clinical relevance. Second, by using a medical database there is also a risk of misclassification of cases. However, previous work has validated codes for psoriasis and psoriatic arthritis,14 16 and our results remained robust in sensitivity analyses, so this risk is expected to be small. Nonetheless, it is possible that some patients had psoriatic arthritis prior to beginning in THIN and were subsequently not captured and removed from this study. Lastly, while this study shows an association between psoriasis and foot and ankle tendinopathy or enthesopathy, it was not possible to include imaging findings, genetics or serum inflammatory markers, which may provide further information.
In summary, this study suggests that cutaneous psoriasis without joint involvement increases the risk of developing foot and ankle tendinopathy or enthesopathy by approximately 25%. While the absolute risk of developing foot and ankle tendinopathy or enthesopathy among patients with psoriasis was relatively low, the increased risk relative to the general population is important in considering the potential systemic nature of psoriasis. Future research should explore the mechanisms by which patients with psoriasis are at increased risk of foot and ankle tendinopathy or enthesopathy. Clinically, physicians should be aware that patients with psoriasis may present with foot and ankle tendinopathy or enthesopathy without necessarily having psoriatic arthritis.
References
Footnotes
Contributors RTL, IAV and CB developed the study topic. LMP, JML and CB contributed expert advice on psoriasis, psoriatic arthritis and tendinopathy/enthesopathy. RTL, LMP, JML and CB reviewed Read codes corresponding to the present study. IAV, ADF and MWL contributed to data systems development and extraction. GGK, SBP and CB provided methodological expertise. Statistical analyses were performed by IAV with critical review by RTL, GGK, SBP and CB. RTL drafted the manuscript, tables and figures, with all authors providing critical review. All authors approved the final version of this manuscript.
Funding This study was funded by a studentship from the Canadian Association of Psoriasis Patients and the Canadian Institutes of Health Research.
Competing interests None declared.
Patient consent Not required.
Ethics approval Approved by the University of Calgary Conjoint Health Research Ethics Board and the UK IMS Health Scientific Review Committee.
Provenance and peer review Not commissioned; externally peer reviewed.
Correction notice This article has been corrected since it first published. Figures 1 and 2 have been transposed so that they are with the correct figure legend.