Article Text

Abstract
Objectives To update the knowledge on employment and the role of mastery, a personal factor reflecting the level of control over life and disease, among Dutch patients with ankylosing spondylitis (AS) compared to general population subjects.
Methods Data of persons ≤65 years participating in a Dutch cross-sectional multicentre study on social participation in AS were used. Being employed was the main outcome. Standardised employment ratios (SERs) were calculated using indirect standardisation after adjusting for age, gender and education and repeated after stratification by symptom duration tertiles. Modified Poisson regressions were performed to understand the role of mastery (Pearlin’s scale) independent of sociodemographic and health-related factors.
Results 214 patients and 470 controls (127 (59.3%) and 323 (68.7%) males; mean age 48.3 (SD 10.4) and 39.3 (SD 12.7) years, respectively) completed an online questionnaire. SER (95%CI) in patients was 0.83 (0.69–0.98); 0.84 (0.67–1.04) in males; 0.83 (0.59–1.07) in females. Adjusted absolute employment of patients compared to controls was 69% versus 84%; 73% versus 86% for males; 62% versus 78% for females. In multivariable analyses stratified for patients and controls, mastery was associated with being employed in patients, but only in those with low education. In controls, not mastery but higher education was associated with being employed.
Conclusion Our study reveals that patients suffering from AS compared to population controls are less likely to be employed. Mastery is an important personal factor associated with employment in patients but not in controls. Interventions aimed at improving employment of patients with AS should likely account for mastery.
- ankylosing spondylitis
- spondyloarthritis
- epidemiology
- employment
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Key messages
What is already known about this subject?
In the pre-bDMARD (biological disease-modifying antirheumatic drug) era, employment of patients with ankylosing spondylitis (AS) was reduced compared with the general population.
Personal attitudes or beliefs, such as passive coping or helplessness among patients with AS, have been associated with adverse work outcome.
What does this study add?
This study demonstrates that employment of patients with AS in the Netherlands in the bDMARD era remains reduced compared with the general population.
Mastery, an indicator of control over stressors of life, is associated with being employed in patients but not in controls.
How might this impact on clinical practice?
Also in the 21st century, employment in patients with AS deserves attention, and programmes aimed at work participation might need to focus on self-management skills.
Introduction
For patients with ankylosing spondylitis (AS), employment ranks among the three most important social roles.1 Preceding studies showed that patients with AS encounter difficulties to remain employed.2 When compared with population controls, a Dutch study from 2001 revealed that age-adjusted and gender-adjusted employment in patients with established AS was 11% lower.3 Moreover, a decrease in employment was already seen early in the disease.4 In the same period, other European studies confirmed reduced employment of patients compared with the general population.5, 6 Since then, efforts have been made to improve timely diagnosis and treatment of AS. Importantly, biological disease-modifying antirheumatic drugs (bDMARDs) have been introduced, which had overall beneficial effect on presenteeism and sick leave in patients with higher disease activity.7 Given this progress, it would be expected that employment rates in AS are improving and possibly even become similar to those of the general population. This would be especially expected in patients with short symptom duration, as the effects of improvement in care over the last decade would be expected to be most pronounced in this subgroup.
Participation in labour force of patients with a chronic disease is a complex outcome, and several theoretical frameworks are available to help understand the complex interplay between biomedical and different personal and environmental factors.8, 9 Disease-related determinants, such as disease activity and physical function, can only partially explain the impact of AS on work. 10 Past studies provided empirical evidence that lack of control, reflected by passive coping, self-efficacy or helplessness were strongly associated with adverse work outcome, independent of disease-specific impairments.4, 11, 12 However, it remains unclear whether the effect of personal attitudes or beliefs has a generic (ubiquitous) effect on work participation or plays a different role in patients compared with general population subjects. Such information would be relevant to emphasise the role of self-management specifically in persons with a chronic disease and would support reinforcing the role of self-efficacy in patient education programmes for employed patients with AS for whom continuation in the workforce is an important goal.13
In the current study, the first objective was to update the current knowledge on employment of patients with AS in comparison to the general population in the Netherlands, also in relation to symptom duration. The second objective was to understand whether mastery, reflecting level of control over life and disease, would have a similar association with employment in patients as in controls.
Methods
Study population
Data from the Social Participation in AS Study (SPASS), a multicentre cross-sectional survey-based study including patients with AS in the Netherlands, were used for this analysis.1 Patients were recruited from six hospitals during a 6-month period in 2011. Patients were eligible if at least 18 years of age and if the treating rheumatologist confirmed fulfilment of the modified New York criteria for AS.14 Exclusion criteria were insufficient ability to read/understand the Dutch language, no access to a computer with online connection and severe immediate life-threatening comorbidities according to the treating physician. A control population was recruited in parallel by Ipsos, an ISO-certified independent company specialised in population surveys for global market, policy and research purposes. Population controls were sampled to yield an age and gender distribution as expected from previously published observational studies in AS (mean age 42 years, male to female ratio 3:1).15 The study was approved by the ethical committee of the Maastricht University Medical Center and all participants provided informed consent.
Assessments
All participants completed a similar online survey, with questions on sociodemographics including income (four categories), education (primary school, lower (professional) education, secondary (vocational) education, higher education/university) and a question on employment (currently employed, yes/no). Lifestyle was assessed using questions on smoking and drinking behaviour. Generic health status was assessed using the Short Form-36 (SF-36), providing a Physical Component Summary (SF-36PCS) and Mental Component Summary (SF-36MCS).16 Disease-related questions included questions on symptom duration (defined as time in years since symptom onset) and medication use. Disease activity and functioning were measured among patients using the Bath AS Disease Activity Index (BASDAI) and Bath AS Functional Activity Index (BASFI), respectively.17, 18 Presence, treatment and functional impact of comorbidities and extra-articular manifestations (psoriasis, uveitis and inflammatory bowel disease (IBD)), were assessed using the Self-Administered Comorbidity Questionnaire (SCQ).19 Mastery, the extent to which one feels their life chances as being under their personal control, was assessed using the 7-item Pearlin’s mastery scale.20 This instrument measures the extent to which individuals perceive themselves in control of forces that significantly impact their lives. Each item can be scored on a 1 to 4 scale (1: strongly disagree; 2: disagree; 3: agree; 4: strongly agree) resulting in a score range of 7 (worst) to 28 (best). The individual items of Pearlin’s mastery scale are presented in online supplementary file 1.
Supplemental material
Statistical analysis
Being employed (yes/no) was the main outcome for the current analyses, which is why the study sample was restricted to those aged≤65 years (the legal age of retirement in the Netherlands in 2011). Differences in demographic and health characteristics between patients and population controls were explored with independent t-test, Mann Whitney test or χ² test, depending on level of measurement and distribution. If appropriate (expected count<5), Fisher’s exact test was preferred over χ² test.
Standardised employment ratios
The impact of AS on work participation when compared with population controls was assessed for the total group and subsequently for three strata of symptom duration (tertiles: 0–14, 15–27 and 28–50 years), by computing standardised employment ratios (SERs) with 95% CI using indirect standardisation methods. Standardisation accounted for gender, age (categorised:<35, 35–<50 and 50–65 years of age) and education (university/college level versus no/lower/secondary education). The SER can be interpreted as the relative chance of patients with AS having a paid job compared with the control group (set as reference, value=1.00). To investigate the effect of disease activity on employment, SERs were also presented for patients with a BASDAI≥4 and patients with a BASDAI<4 separately. Using the SER, the adjusted absolute employment rate for patients was computed by multiplying the SER for patients by the absolute employment rate of controls.
Differential effect of contributory factors in patients and controls
To assess the differential impact of mastery on employment in patients or controls, a regression model was developed with employment (yes/no) as dependent variable. As incidence rate ratios (IRRs, generated by modified Poisson regression) more accurately reflect risks than ORs (generated by logistic regression) when the prevalence of the outcome is >10%, modified Poisson regression was preferred over logistic regression.21 Exploratory analysis revealed that patients on TNFi were in a worse health state compared with patients not on TNFi. Likely, these patients had even worse disease at the start of TNFi, and the role of TNFI at the individual level cannot further be explored as this covariate is subject to confounding by indication. Consequently, TNFi use was not included in the multivariable models to prevent biased results. Also, as the aim of this analysis was to compare the differential effect of factors in patients and controls, generic variables (such as SF-36PCS) were preferred over disease-specific factors (such as BASDAI). Variables of interest were thus education (dichotomised, higher education/university versus other), smoking, alcohol use, body mass index, comorbidity, health status (SF36-PCS, SF36-MCS) and mastery. These were first explored in univariable analysis, correcting for gender and age. Next, a basic multivariable model was computed in the total sample including age, gender and group-membership (patient versus control). Subsequently, demographic variables and health variables (SF-36PCS, comorbidity) that were associated with being employed in univariable analyses (p<0.20) were added using a manual forward method, after ruling out collinearity between variables. Variables were retained if significantly associated with the outcome (p<0.05) and/or a confounder (changed the IRR of included variables>10%). As a final step, mastery was added.
Interactions between group-membership and all variables in the model were tested, and p<0.10 was considered sufficient reason to explore stratified analyses. As significant interactions were found between group-membership and mastery (p=0.02) as well as SF-36PCS (p=0.08), further analyses were carried out in patients and controls separately. As an additional interaction was observed between education and mastery in the patient group (p=0.08), the final analyses were carried out in three separate subsamples: controls, patients with lower education and patients with higher education. All statistical analyses were performed with SPSS V.23.0 (IBM, Armonk, New York, USA) and Stata Release 14 (Stata, College Station, Texas, USA).
Results
Comparison of patients with AS versus controls
In total, 214 subjects diagnosed with AS and 470 controls of 65 years or younger participated. Against expectations, patients were significantly older than controls (48.3 vs 39.3 years, p<0.01) and less frequently male (59.3% vs 68.7%, p=0.02). Patients more frequently had low income and low education. Further, comorbidity score was higher and SF-36PCS and mastery were worse in patients with AS compared with population controls (table 1).
Characteristics of the patients with AS and population controls aged≤65 years
Standardised employment ratios
The SER (95% CI) in patients with AS, having controls as reference (value 1.00), was 0.83 (0.69 to 0.98) overall; 0.84 (0.67 to 1.04) for males and 0.80 (0.59 to 1.07) for females (figure 1A). The adjusted absolute employment rates for patients and controls were 69% vs 84% in the total population; 73% vs 86% for males and 62% vs 78% for females. Although not statistically significant, SERs in males were lowest in the tertile of those with longest symptom duration. This was not observed in females. Along the same line, SERs were slightly (but not significantly) lower in females than in males, except for the subgroup with a symptom duration of 15–27 years (figure 1A). It should be noted that also absolute (adjusted) employment was somewhat lower in females compared with males (figure 1B). The SER in patients with a BASDAI≥4 was significantly lower compared with controls. In contrast, in patients with a BASDAI<4, the SER was almost similar to controls (figure 2).
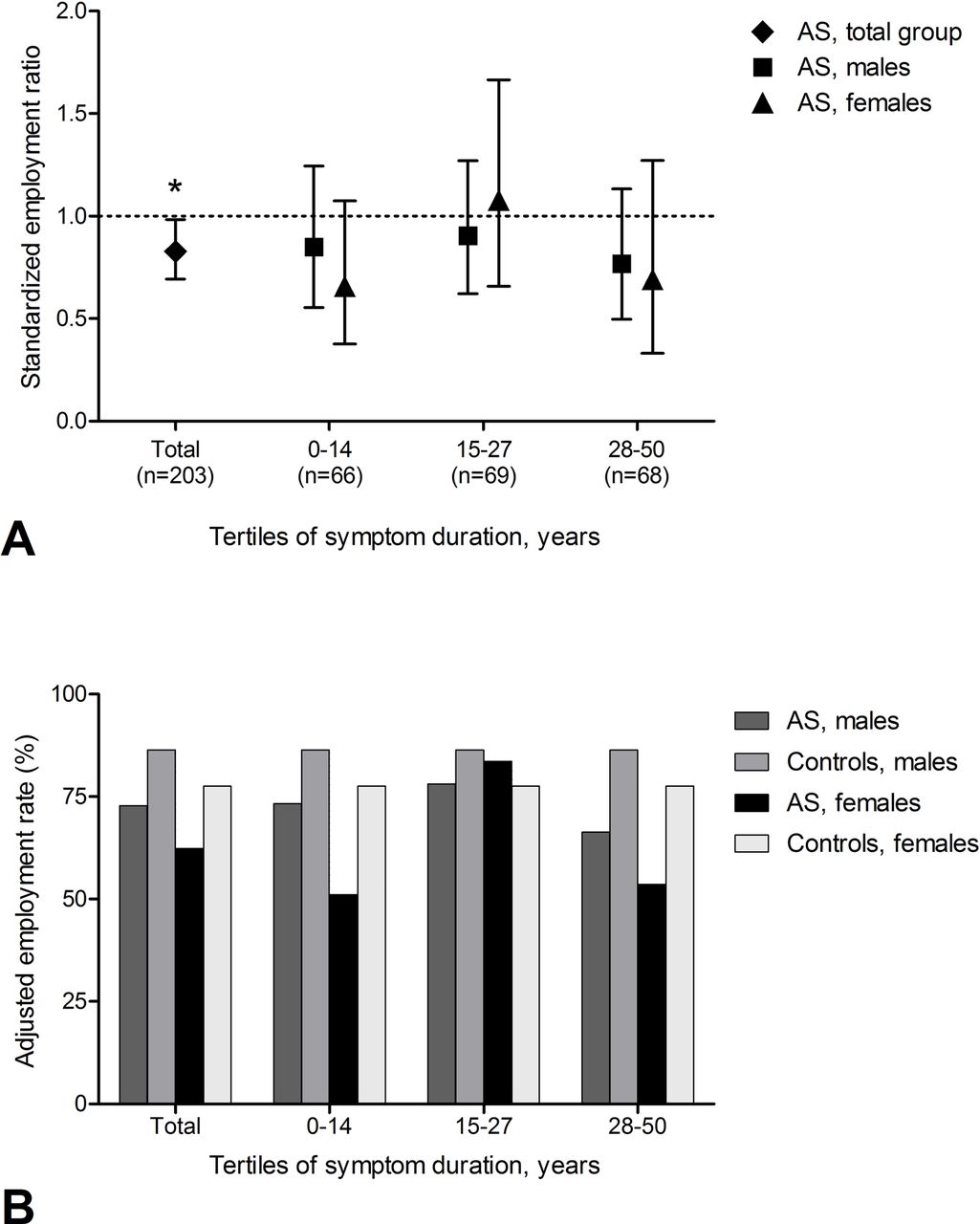
Employment of patients with AS compared with controls. SERs with 95% CIs of patients with AS with controls set as reference (dotted line, 1A) and adjusted absolute employment rates for patients with AS and controls (1B), stratified by symptom duration and gender. Calculation of adjusted absolute employment=SERAS × employment rate of controls. Due to missing data, 203 (of 214) patients were included in this analysis. *P<0.05 compared to controls. AS, ankylosing spondylitis; SERs, standardised employment ratios.

{kind=link}
{kind=link}
Employment of patients with AS compared with controls, by BASDAI. SERs with 95% CIs of patients with AS with controls set as reference (dotted line), stratified by symptom duration and BASDAI. Due to missing data, 203 (of 214) patients were included in this analysis. *P<0.05 compared to controls. AS, ankylosing spondylitis; BASDAI, Bath Ankylosing Spondylitis Disease Activity Index; SERs, standardised employment ratios.
Differential effect of mastery in patients and controls
The results of univariable analyses are shown in table 2. Multivariable stratified analyses by group-membership and further by education in patients are presented in table 3. Among controls, better SF-36 PCS and higher educational attainment were associated with increased employment rates (IRR=1.01, 95% CI 1.00 to 1.02 for SF-36PCS; IRR=1.09, 95% CI 1.01 to 1.18 for higher education). No association between mastery and employment was observed in controls. However, in patients with AS with lower education a significant association was seen between mastery and employment (IRR=1.04, 95% CI 1.01 to 1.08), while this was not observed in those with higher education (mastery forced into multivariable model: IRR=1.01, 95% CI 0.98 to 1.04). In addition to education, higher age was associated with a decreased employment, while better SF-36PCS with an increased chance of being employed (table 3).
Univariable stratified analysis exploring determinants of employment in subjects aged≤65 years
Multivariable stratified analysis exploring determinants of employment in subjects aged≤65 years
To confirm the role of mastery in patients with a low level of education, a scenario analysis was carried out for which BASDAI or BASFI (separate models due to collinearity between these variables) was used in the models instead of SF-36PCS. This analysis led to similar results (table 4). Of note, mastery was not significant nor a confounder in patients with a high level of education, and if forced into the models, its effect size was small to none (data not shown).
Multivariable analysis exploring determinants of employment in patients aged≤65 years stratified by level of education
Discussion
Employment among patients with AS in the Netherlands was 14.4% lower than in a general population sample after adjustment for age, gender and education. Although this adverse effect on employment was also observed in patients with AS with shorter symptom duration, the impact seemed stronger in those with longest symptom duration. Mastery, a personal factor assessing level of control over life and disease, was associated with employment in patients with AS who had a lower educational level, but not in controls.
Considering the innovations in diagnosis and biomedical management of patients with AS over the last two decades, one would expect the difference in employment between patients and general population to have become smaller. Instead, almost 15 years after a comparable study among Dutch AS patients (data from 1997) which reported a reduction in employment of 11%, our findings were of similar magnitude.3 It should be emphasised that overall employment in the general population increased substantially over this 15-year period. While employment rate for the general population in the previous study was 66% (54% in AS, adjusted), this was 84% in the current study (69% in AS, adjusted). Likely the concurrent increase in employment in the general population, but also the higher work load in times of economic austerity that likely affects patients more severely, attenuates the expected improvement on work participation of patients when compared with controls. A recent study from Germany investigating employment (among other outcomes) in a mixed prevalence and incidence cohort of patients with AS in the period 2000–2012 revealed overall employment ratios comparable to our results.22 Somewhat contrary to our study, they found that the overall difference in employment rates between patients with AS and general population was decreasing, and even non-existent in the younger subgroups. When stratifying our sample for symptom duration, employment rates were even decreased in those with less than 15 years’ symptom duration. This suggests that employment remains challenging despite improved medical treatment. Notwithstanding, the decrease in employment was somewhat stronger in those with a longer symptom duration. This may reflect that patients diagnosed in the last 15 years have benefitted from the availability of biologicals.
Although previous studies in AS pointed towards a greater reduction in work participation among men than women, the current study suggests no gender difference.3, 6 The non-significant higher employment ratio of 1.08 in women with a symptom duration between 16 and 30 years was unexpected. Of note, the sample size of this subgroup was small (n=25 patients, of which 8 were with higher education), as reflected by the large CI surrounding the IRR and chance likely played a role.
An adverse impact of comorbidities on employment in spondyloarthritis has recently been described in a cross-sectional international study.23 In the current study, comorbidities were associated with employment in univariable analysis in both controls and patients with AS, but such association was not confirmed in multivariable analysis in either of the populations. Possible explanations for this discrepancy could be the differences in study populations and instruments used to assess comorbidity. Also, the influence of comorbidities on outcome might not be similar across countries.24
The current analyses confirm the role of personal contextual factors in relation to employment among patients with AS. Specifically, lower mastery was associated with not being employed. Importantly, mastery was only relevant in patients with lower education, another personal contextual factor. Apparently, in lower educated persons, low mastery is a barrier to overcome challenges to remain active in the labour force. To the best of our knowledge, this is the first study to reveal that mastery is not a ‘generic’ determinant of work outcome, as clearly mastery played no role in employment outcome among controls. It seems that persons with a chronic disease are more vulnerable to the effect of lower mastery.
In addition to the role of context, physical health (SF-36 PCS) remains suboptimal in patients compared with controls and contributes importantly to the lower employment. Although biologicals were widespread available in 2011, active disease was present in a significant number of patients in SPASS (BASDAI≥4 in 57.5% of patients). Within the limits of interpretability in a cross-sectional study, subgroup analysis of the data also suggested employment in patients is particularly reduced in those with BASDAI≥4. Currently, the treat-to-target principle is being investigated in axial spondyloarthritis (axSpA). It is important that studies on treat-to-target in axSpA also consider work participation as an outcome. If treat-to-target (ie, to low disease activity) for axSpA turns out to be effective, the difference in employment between patients with AS and the general population should become smaller.
Strengths of our study were inclusion of a general population sample, participation of centres with different settings (academic and private hospitals) and from various geographical regions and availability of all predictors in patients as well as controls. Nevertheless, there are some limitations. First, it should be emphasised that the current observations apply only to patients under care of a rheumatologist. Further, matching of patients to control subjects was less successful than intended, but extensive adjustment was performed in all analyses. Also, given our retrospective approach, reverse causality (loss of employment or unable to become employed having negative influence on mastery) cannot be excluded. Comparison with the 1997 Dutch data, while insightful, should be done with some caution as data collection was not similar (for 1997 aggregated data from the Central Bureau of Statistics was used for standardization, while for the current study direct sampling allowed to collect more patient level characteristics).[3] Next, as cultural, societal and legal provisions are likely to influence employment status in both patients and the general population, generalisability of our results to other countries is limited. Finally, although we had information on use of TNFi medication (55% users in AS group), the effect of TNFi medication on employment could not be investigated, due to confounding by indication. It should be noted that data on the health state and disease activity of these patients before TNFi initiation were not available. Consequently, no conclusions regarding the benefits of TNFi use regarding employment can be drawn. Note that this limitation does not impact our primary analysis of employment rates in patients versus controls.
In summary, our findings showed that despite the widespread availability of bDMARDs, employment of Dutch patients with AS was decreased when compared with general population controls. Not only biomedical but also contextual factors explain employment. Higher mastery was associated with better employment in patients only, especially those with lower educational level. Programmes aimed at work participation in AS might need to focus on self-management skills to be effective. Further research is necessary to develop interventions and confirm their effectiveness.
References
Footnotes
Contributors AB designed the study. LH, MvdL, JL, DvdH, FAvG, AS, AB, SvG and CW were involved in data collection and/or data management. CW, LV and AB analysed the data and critically interpreted the results. CW, LV and AB were involved in drafting the manuscript. All authors revised the manuscript critically for important intellectual content and approved the final manuscript.
Funding This work was supported by AbbVie. AbbVie sponsored data collection but had no role in the study design, analysis or interpretation of the data or the writing of the manuscript. Publication of this article was not contingent on approval by AbbVie.
Competing interests None declared.
Ethics approval The study was approved by the ethical committee of the Maastricht University Medical Center.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement No additional data are available.