Article Text

Abstract
Objective To assess the association of gout with new-onset atrial fibrillation (AF) in the elderly.
Methods We used the 5% Medicare data from 2005 to 2012 to assess whether a diagnosis of gout was associated with incident AF. We used multivariable Cox regression adjusted for demographics, Charlson-Romano comorbidity index, common cardiovascular medications, allopurinol and febuxostat use, to calculate hazard ratios (HRs) and 95% confidence intervals (CIs).
Results Among 1 647 812 eligible people, 9.8% had incident AF. The mean age was 75 years, 42% were male, 86% were white and the mean Charlson-Romano index score was 1.52. We noted 10 604 incident AF cases in people with gout and 150 486 incident AF cases in people without gout. The crude incidence rates of AF in people with and without gout were 43.4 vs 16.3 per 1000 patient-years, respectively. After multivariable-adjustment, gout was associated with a higher HR of incident AF, 1.92 (95% CI 1.88 to 1.96), with minimal attenuation of HR in sensitivity models that replaced the Charlson-Romano index score with a categorical variable, HR was 1.91 (95% CI 1.87 to 1.95). In another model that adjusted for AF-specific risk factors including hypertension, hyperlipidaemia and coronary artery disease and individual Charlson-Romano index comorbidities, the HR was slightly attenuated at 1.71 (95% CI 1.67 to 1.75). Older age, male sex, white race and higher Charlson-Romano index score were each associated with higher hazard of incident AF.
Conclusion A diagnosis of gout almost doubled the risk of incident AF in the elderly. Future studies should explore the pathogenesis of this association.
- Gout
- Atrial fibrillation
- Epidemiology
- Risk factor
- Older adults
This is an Open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Key messages
What is already known about this subject?
In the general population of adults, gout is associated with 9%–13% increased risk of atrial fibrillation (AF), but the risk in older adults in unknown.
What does this study add?
After multivariable-adjustment for AF risk factors, gout was associated with a higher HR of incident AF in adults 65 years or older with a HR of 1.92 (95% CI 1.88 to 1.96).
Older age, male sex, white race and higher Charlson-Romano index score were associated with higher risk of AF.
How might this impact on clinical practice?
Screening for AF in people with gout, both in the presence or the absence of heart disease, may lead to early detection and treatment of AF.
Introduction
Gout is the most common inflammatory arthritis in adults affecting 3.9% of US adults.1 Atrial fibrillation (AF) is the most common cardiac arrhythmia worldwide2 that increases the risk of mortality and stroke.3–7 Population is ageing worldwide. In the USA, people 65 years or older will grow from 34.4 million in 2000 to more than 70 million in 2030.8 Both conditions are far more common in adults 65 years or older: 57% of Americans with gout are 60 years or older and gout was present in 9% of adults 70 years or older and 12.6% of adults 80+ years1 and compared with 2% of Americans younger than age 65 with AF, about 9% of people aged 65 years or older have AF.9–11 The AF prevalence is 9% in elderly Portuguese12 and 12% in 75–76-year-old Swedish general population,13 similar to that described in the US Epidemiologic data from other countries showing a similar prevalence of gout in the general population as in the USA have been reported, 2% in the Sweden general population,14 1.4% in UK and Germany,15 1.7% in Australia16 and 2.7% in New Zealand.17 This indicates that the study of AF and novel risk factors in the elderly is very important, given its current and future public health impact. Few, if any studies have focused on older adults, indicating that there is a major knowledge gap in this area.
Chronic inflammation and oxidative stress are the hallmarks of gout.18 Recent studies have shown that gout is associated higher cardiovascular morbidity and mortality.19–24 Many factors likely contribute to a higher cardiovascular disease burden in people with gout, including higher rates of metabolic syndrome and associated comorbidities (hypertension, hyperlipidaemia, diabetes and so on)25 26 as well as hyperuricaemia27–29 and chronic inflammation,30 both of which have an adverse effect on the cardiovascular system.
Few studies have focused on the risk of arrhythmias, such as the AF.31 32 In a study of the UK Clinical Practice Research Data-link (CPRD), gout was associated with higher HR of 1.09 (1.03 to 1.16) for AF, after adjusting for comorbidities.31 In a study of US commercial insurance plan data from 2004 to 2013, compared with osteoarthritis, people with gout had higher multivariable-adjusted HR for new AF at 1.13 (95% CI 1.04 to 1.23).32 Key study limitations were misclassification bias and the lack of assessment of this risk in the elderly population, who are at the highest risk of AF9 and associated complications including stroke and associated mortality.3–7 The elderly also have the highest prevalence of gout among all age groups.1 Therefore, our objectives were to assess whether gout was associated with a higher risk of AF in people 65 years and older, independent of pre-existing cardiovascular disease and other risk factors for AF, and whether this association varied by demographic or clinical characteristics, such as pre-existing cardiovascular disease.
Methods
Data source
In this retrospective cohort study, we used data from the 5% random sample of Medicare claims obtained through the Centers for Medicare and Medicaid Services Chronic Condition Data Warehouse. The Institutional Review Board (IRB) at the University of Alabama at Birmingham approved the study and the need for individual consent was waived, as data are deidentified and no beneficiaries were contacted.
Study population and variables
In order to maximise data available for analysis for this cohort study, we used 2005 as our baseline period and 2006o 2012 as the observation period. Beneficiaries were required to be enrolled in Medicare fee-for-service, be US residents from 2006 to 2012, and be older than 64 and younger than 110 on 1/1/2006.
The gout diagnosis was based on two claims with an International Classification of Diseases, ninth revision, common modification (ICD-9-CM) code 274.xx occurring more than 4 weeks apart during 2006–2012, a validated approach with sensitivity of 90% and specificity of 100%.33
A new diagnosis of AF was our outcome of interest and was based on occurrence of two claims for AF more than 4 weeks apart with an ICD-9-CM code of 427.31 during the study period, 2006–2012. This approach had a median accuracy of 89% of identifying AF in a systematic review (range, 70%–96%).34 People who had ICD-9-CM code for AF in 2005 were considered to have baseline AF and were excluded from the cohort.
We used the 2005 claims data to identify pre-existing comorbidities and calculated the Charlson-Romano comorbidity score. Part D files were used to assess for concomitant medication use, including common cardiovascular drugs (statins, beta-blockers, diuretics and ACE-inhibitors) and gout drugs (allopurinol, febuxostat).
Statistical analysis
Patient demographics and the occurrence of incident (new) AF were summarised, categorical variables as frequency (per cent) with p values based on χ² test and continuous variables as mean (SD) with p values based on Student’s t-test. We assessed the association of gout with incident (new) AF using the multivariable-adjusted Cox proportional hazards model, while adjusting the analyses for known or suspected risk factors for AF (ie, some were potential confounders), including age, gender, race, cardiovascular and gout medications, and medical comorbidities (Model 1). Several covariates were assessed at baseline including gender, race and comorbidities, while others were allowed to vary over time, such as age, gout diagnosis and medication use for cardiovascular disease and gout.
We performed sensitivity analysis by replacing the continuous Charlson-Romano score in the main model by a 3-level categorised Charlson-Romano score (Model 2). We examined an additional AF-specific model by controlling for comorbidities that are known/suspected risk factors for AF including hypertension, hyperlipidaemia and coronary artery disease (CAD) and individual components of Charlson-Romano index (diabetes, myocardial infarction (MI) , peripheral vascular disease and heart failure were among the 17 comorbidities; Model 3). We performed sensitivity analysis by removing CAD from Model 3, due to collinearity of CAD with MI (1 of the 17 Charlson-Romano index comorbidities).
We also performed subgroup (secondary) analyses with additional multivariable-adjusted Cox proportional hazards models by subsetting the data based on age, gender, race and select baseline comorbidities that are well-known risk factors for AF (congenital heart disease, CAD, previous MI).
Results
Study population
We observed 1 647 812 eligible people from 2006 to 2012, of whom 9.8% developed incident AF. Mean age was 75 years, 42% were male, 86% were white and the mean Charlson-Romano index score was 1.52 (table 1). Fifty-four per cent had a Charlson-Romano index score of 0, 10% had a score of 1% and 36% had a score of 2 or more (table 1).
Demographic and clinical characteristics of people with vs without incident AF
Crude incidence rate of atrial fibrillation
There were 0.24 million person-years of follow-up for people with gout and 9.46 million person-years of follow-up available (including 9.2 million follow-up years in people without gout). We noted 10 604 incident AF cases in people with gout and 150 486 incident AF cases in people without gout. The crude incidence rates of AF in people with and without gout were 43.4 vs 16.3 per 1000 patient-years, respectively.
Multivariable-adjusted risk of atrial fibrillation, sensitivity analyses and subgroup analyses
After multivariable-adjustment, gout was associated with higher hazard rate of incident AF, 1.92 (95% CI 1.88 1.96) (table 2). Older age, white race and higher Charlson-Romano index score were each associated with higher hazard of incident AF (table 2).
Multivariable-adjusted association of gout and select risk factors with incident AF
In sensitivity analyses that replaced the continuous score in the main model with categorical Charlson-Romano index score (model 2), the findings from the main analyses were confirmed with some attenuation of the association of gout with incident AF, with HR of 1.91 (95% CI 1.87 to 1.95) (table 2). In the AF-risk factor specific model, including hypertension, hyperlipidaemia, CAD and all individual Charlson-Romano index comorbidities (model 3), the HR of AF with gout was slightly attenuated at 1.71 (95% CI 1.67 to 1.75) (table 2). In sensitivity analyses that removed CAD from model 3 (to avoid collinearity), the main findings were confirmed; gout was associated with AF with HR of 1.72 (95% CI 1.68 to 1.76).
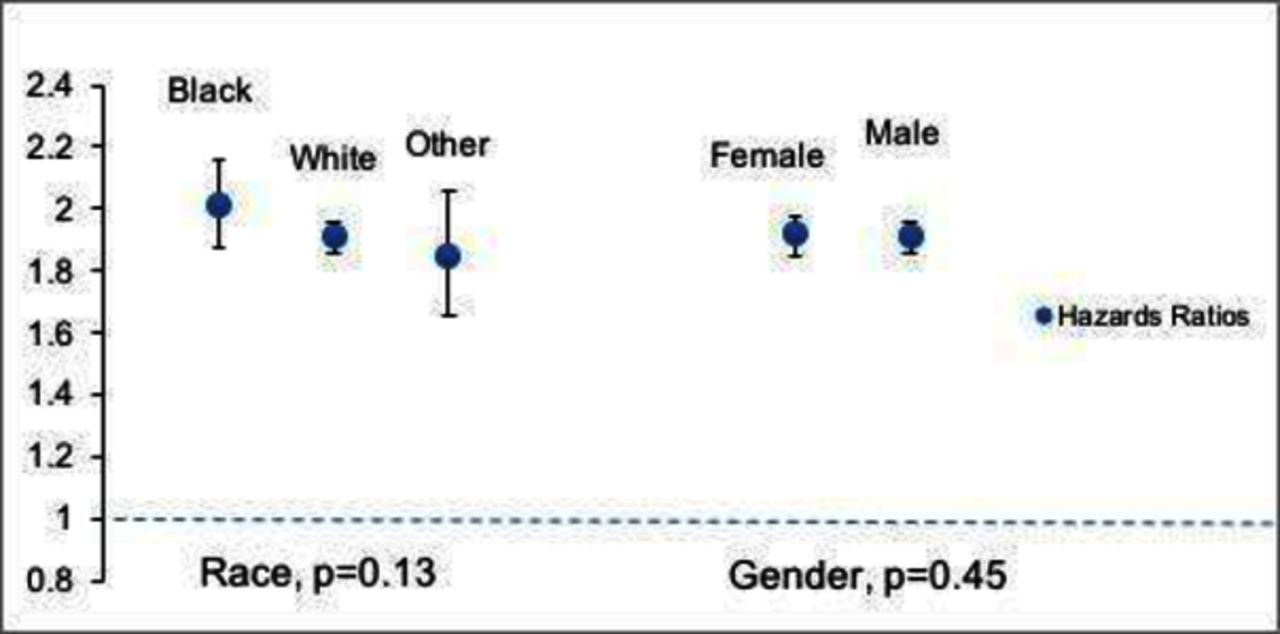
In subgroup analyses, we found that risk of AF with gout was higher in people without known congenital heart disease, CAD or a previous MI (p<0.05 for interaction term in each model; online supplementary appendix 1), although a higher risk of AF with gout was noted in both categories (figure 1). Borderline differences were also noted by race/ethnicity, with slightly higher AF risk with gout in Blacks (p=0.13), but no differences by sex (p=0.45; figure 2).
Supplemental material

Subgroup analyses of association of gout with incident AF by clinical characteristics that are risk factors for AF. Point estimates indicate the HR of incident AF with gout and the whiskers 95% CI. We show these for each subgroup analysis, based on the presence or absence of each disease. The horizontal line through HR of 1 represents null hypothesis. Any HR with 95% CI that overlaps this line is not statistically significant. AF, atrial fibrillation.

{kind=link}
{kind=link}
Subgroup analyses of association of gout with incident AF by key demographic characteristics, race and gender. Point estimates indicate the HR of incident AF with gout and the whiskers 95% CI for subgroup analysis by race and gender. The horizontal line through HR of 1 represents null hypothesis. Any HR with 95% CI that overlaps this line is not statistically significant. AF, atrial fibrillation.
Discussion
In this study of elderly Americans, we found that the crude incidence of AF was 4.3/100 person-years in people with gout vs 1.6/100 in those without gout. The higher AF incidence in our study compared with the previous studies is likely related to our cohort being 15–20 years older than the previous cohorts,31 32 and older age is a well-known risk factor for higher risk of AF.9 Gout was independently associated with a 71%–92% higher hazard/risk of incident AF in people who were 65 years of older. We also noted that the increase in the risk of AF with gout varied by the underlying cardiac disease and possibly by race/ethnicity. Several findings in our study merit further discussion.
Recent studies including systematic reviews35 36 support the association of gout with increased cardiovascular morbidity including the risk of CAD and stroke.35–40 Emerging data have suggested that gout is associated with slightly higher risk of AF in the general UK or an insured US population, with increased odds of 9%–13%, compared with those without gout or those with osteoarthritis.31 32 However, no estimates were provided for the elderly population that is at the highest risk for gout1 and AF,9 6 and also the most rapidly expanding US population subgroup that will grow from 34.4 million in 2000 to more than 70 million in 2030 in the USA.8 To our knowledge, our study is one of the first studies to assess the risk of AF in older Americans, who are 65 years or older.
We found that gout independently increased the risk of incident AF by 71%–90%; the excess risk attributable to gout was much larger than previously reported 9% and 13% by the two studies.31 32 Our study differs from the previous studies in that we focused on people 65 years or older as the population of interest for the reasons previously cited (as opposed to all people or people 40 years of older),8 defined the comparator group as people with no gout (compared with osteoarthritis), defined gout as the presence of gout diagnosis (rather than diagnosis plus medication use, which has higher sensitivity, but has lower generalizability) and performed subgroup analyses by the common risk factors for AF, including CAD, MI and so on, previously not assessed by other studies. Medication adherence with gout is poor with only 33%–50% of gout people using gout medications long-term.41 42 Definitions of gout that require the use of gout medications are designed to have higher specificity at the cost of missing a large proportion of gout people (50%–67%), making findings only generalisable to small proportion of people with gout that use gout medications. In addition, urate-lowering drugs would reduce urate crystal deposition, which could reduce the observed risk of AF associated with gout. Therefore, we did not require the use of medications for defining gout, but used the presence of diagnostic codes, a validated approach with sensitivity of 90% and specificity of 100%.33 We adjusted for medication use to understand the disease associations independent of the treatments. Our study finding advances our understanding of cardiovascular comorbidity of gout in the elderly. Healthcare providers who already discuss the possible increased risk of CAD with people with gout should also incorporate the discussion regarding the associated increased risk of AF. These discussions can fully inform patients with gout that associated ongoing inflammation may have implications not only for their joints, but other vital body organs.
We found that even though the risk of AF with gout was increased in people in both groups in subgroup analyses, the risk was higher in people without CAD, congenital heart disease or previous MI, compared with the AF risk in people with any of these conditions. CAD, MI and congenital heart disease are associated with a higher risk of AF,43 which indirectly explains a smaller risk contribution of gout to AF in their presence. The AF risk with gout was statistically and clinically significantly different in people with vs without CAD, 1.55 vs 2.01. This observation is similar to that noted by Kuo et al of a higher MI risk with gout in people without vs with CAD.21 If confirmed in another dataset, these findings have practical clinical implications, mainly that a good control of gout may be more beneficial for AF prevention in those without CAD.
We found that in contrast to the gender difference in risk of other cardiovascular comorbidity with hyperuricaemia and gout,19 the AF risk was similarly increased in men and women. Gout was associated with a higher AF risk in all race/ethnicities with minor differences by race/ethnicity. Not surprisingly, higher medical comorbidity index score was associated with a higher risk of incident AF. Compared with people with no Charlson-Romano index comorbidities, those with Charlson-Romano index score of 1 had 65% higher hazard and those with a Charlson-Romano index score of 2 or more comorbidities had 102% higher HR. Older age was associated with a higher hazard of incident AF. Compared with those 65 to <75 years old, those 75 to <85 years and 85 years and older had 68% and 108% higher hazard of incident AF. This finding confirms a previous similar finding.10 Our study adds to the growing evidence of higher cardiovascular morbidity and mortality in people with gout and/or hyperuricaemia.
Hyperuricaemia,44–48 oxidative stress49 50 and chronic inflammation51–53 increase the AF risk, and all are features of gout, which might explain the higher AF risk with gout. Supporting evidence also comes from animal studies that showed that allopurinol reduced the risk of AF54 and prevented oxidative stress and fibrosis.55 A recent cohort study in the elderly found AF risk reduction with allopurinol.56 This effect may be mediated by allopurinol-associated oxidative stress reduction by its inhibition of xanthine oxido-reductase,57 or an improvement of the endothelial dysfunction by allopurinol, as previously noted in heart failure.58 Allopurinol may also reduce the AF risk by the reduction of serum urate (sUA), urate crystal deposition and associated chronic inflammation.59 These data lead to the hypothesis that hyperuricaemia, oxidative stress and chronic inflammation in gout may contribute to the risk of AF.
Our study has several strengths and limitations. Study strengths include the use of US Medicare claims data, which is representative of Americans 65 years and older, adjustment for multiple covariates/potential confounders and the replication of findings in sensitivity analyses that support robustness of findings.
Study limitations include potential non-differential misclassification bias since we used the diagnostic codes to identify people with gout and AF, and we would expect to bias results towards the null. Residual confounding is possible given our observational cohort design, despite our attempts to control for demographic factors, medical comorbidity and the use of common medications. We did not adjust for aspirin, non-steroidal anti-inflammatory drug use, alcohol use, smoking or exercise, which may have contributed to some residual confounding, since these data including over-the-counter medication use are not available in Medicare claims. Findings can only be generalised to Americans 65 years or older. We were unable to assess potential mechanistic pathways for study findings, due to the lack of data on sUA and inflammation markers (C reactive protein or others) in Medicare data, which does not include results of laboratory tests. We performed subgroup analyses by several common correlates of AF (age, race, CAD, MI, congenital heart disease), but limited resources, low numbers and/or lack of data in Medicare made it infeasible to analyse whether association of gout with AF varied by the presence/absence of other AF risk factors, for example, heart failure, obesity, heavy alcohol use, hyperthyroidism. The recent finding of cardioprotective effect with the inhibition of IL-1 pathway with canakinumab in people with heart disease in the CANTOS study60 indicates that subsequent studies should explore the role of other medications that inhibit IL-1 pathway including colchicine for the prevention of AF.
Conclusion
We found that gout was associated with a higher risk of incident AF in adults 65 years or older, after controlling for several known and suspected risk factors, including age, sex, race, medical comorbidities including cardiovascular disease and medication use. The presence of cardiovascular disease had some impact on this association. Future studies should reproduce these findings in similar elderly cohorts and assess what mechanisms underlie this increased risk. An equally important question is whether inhibitors of xanthine oxidase such as allopurinol can independently reduce the risk of AF and could potential treat or prevent AF in high-risk patients.
Acknowledgments
We thank Dr Jeffrey Curtis of the UAB Division of Rheumatology, who permitted us to reuse the 5% Medicare data. We thank patients at the University of Alabama gout clinic for asking us to questions whether controlling gout can benefit other comorbid conditions, which prompted us to ask this question.
References
Footnotes
Contributors JAS designed the study, developed study protocol, reviewed analyses and wrote the first draft of the paper. JDC performed the data abstraction and data analyses. All authors revised the manuscript, read and approved the final manuscript.
Funding This material is the result of work supported by research funds from the Division of Rheumatology at the University of Alabama at Birmingham and the resources and use of facilities at the Birmingham VA Medical Center, Birmingham, Alabama, USA.
Disclaimer The funding body did not play any role in design, in the collection, analysis and interpretation of data; in the writing of the manuscript and in the decision to submit the manuscript for publication.
Competing interests JAS has received research grants from Takeda and Savient and consultant fees from Savient, Takeda, Regeneron, Merz, Iroko, Bioiberica, Crealta/Horizon and Allergan pharmaceuticals, WebMD, UBM LLC and the American College of Rheumatology. JAS serves as the principal investigator for an investigator-initiated study funded by Horizon pharmaceuticals through a grant to DINORA, Inc., a 501 (c)(3) entity. JAS is a member of the executive of OMERACT, an organisation that develops outcome measures in rheumatology and receives arms-length funding from 36 companies; a member of the American College of Rheumatology's (ACR) Annual Meeting Planning Committee (AMPC); Chair of the ACR Meet-the-Professor, Workshop and Study Group Subcommittee and a member of the Veterans Affairs Rheumatology Field Advisory Committee. JAS is the editor and Director of the UAB Cochrane Musculoskeletal Group Satellite Center on Network Planning Committee (AMPC); Chair of the ACR Meet-the-Professor, Workshop and Study Group Subcommittee and a member of the Veterans Affairs Rheumatology Field Advisory Committee. JAS is the editor and Director of the UAB Cochrane Musculoskeletal Group Satellite Center on Network Meta-analysis.
Patient consent Not required.
Ethics approval The University of Alabama at Birmingham’s Institutional Review Board approved this study and all investigations were conducted in conformity with ethical principles of research. The IRB waived the need for informed consent for this study.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement These data can be obtained from the Centers for Medicare and Medicaid Services (CMS) Chronic Condition Data Warehouse. We are ready to share the data with colleagues, after obtaining appropriate permissions from the Centers for Medicare and Medicaid Services (CMS) Chronic Condition Data Warehouse and the University of Alabama at Birmingham (UAB) Ethics Committee, related to HIPAA and Privacy policies.