Article Text

Abstract
Objectives To assess the impact of extra-articular spondyloarthritis (SpA) manifestations (anterior uveitis, psoriasis and inflammatory bowel disease (IBD)), and of comorbidities, on tumour necrosis factor alpha inhibitor (TNFi) drug retention in ankylosing spondylitis (AS).
Methods We identified all bio-naïve patients with AS starting a first ever TNFi July 2006 to December 2015 from the Swedish Rheumatology Quality register and followed these from treatment start through December 2015. We determined the presence of extra-articular SpA-manifestations, comorbidities (cardiovascular disease, affective disease, diabetes, malignancies, chronic lung disease and kidney disease) and socioeconomic status before TNFi start, through linkage to five other national registers, and calculated, for each factor, crude and adjusted HRs for discontinuing the TNFi.
Results 2577 patients with AS (71% men) started a first TNFi during the study period. 27% had a history of anterior uveitis, 6% psoriasis and 7% IBD. Anterior uveitis was associated with a superior TNFi drug retention (HR 0.72; 0.62 to 0.83), psoriasis with an inferior (HR 1.48; 1.18 to 1.86), whereas IBD did not affect TNFi drug retention. The effect of the SpA manifestations on TNFi drug retention was of a similar magnitude to that of the comorbidities.
Conclusions In AS, anterior uveitis and psoriasis, but not IBD, affect TNFi drug retention. Possible explanations include differential effects of TNFi on these extra-articular SpA manifestations, or inherent differences in AS, associated with the inflammatory phenotype. Further, comorbidities and socioeconomy affect TNFi drug retention to a similar magnitude as the SpA manifestations, and should, as such, receive due attention in clinical practice.
- ankylosing spondylitis
- anti-TNF
- treatment
- epidemiology
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Key messages
What is already known about this subject?
Tumour necrosis factor (TNF)-inhibitor axial response and drug retention in ankylosing spondylitis (AS) are predicted by young age, male sex and a high disease activity at treatment start.
One in four patients with AS also have a history of extra-articular spondyloarthritis manifestations, namely psoriasis, anterior uveitis or inflammatory bowel disease.
What does this study add?
Having a history of anterior uveitis is associated with a better drug retention, while psoriasis is associated with a poorer drug retention, for TNF-inhibitors in AS.
In terms of long-term treatment success with TNF-inhibitors, socioeconomic status, workability and comorbidities are as important as the AS disease itself.
How might this impact on clinical practice?
The results highlight the importance of the treatment context, in addition to the axial disease, for treatment outcomes with TNF-inhibitors in AS.
Introduction
Randomised controlled trials (RCTs) have demonstrated the efficacy of tumour necrosis factor alpha inhibitors (TNFi) in ankylosing spondylitis (AS), with 40%–50% of patients achieving at least a 40% improvement within 6 months of treatment initiation.1 However, observational studies indicate that only 65%–74% of patients with AS remain on their first-line TNFi after 2 years,2 3 and that remission is rarely the reason for discontinuing the treatment.2 This, in turn, suggests that either loss of efficacy or the influence of other factors are critical for treatment discontinuation.
Several studies have searched for predictors of response to TNFi, and of drug retention, in patients with AS.3–11 Patient characteristics that have emerged as positive predictors for drug retention or treatment response are young age, male sex, high disease activity and good functional status.12 In studies of TNFi in AS, response has typically been defined as an improvement in the AS disease activity score (ASDAS),13 the Bath Ankylosing Spondylitis Disease Activity Index (BASDAI)14 or by the assessment of the spondyloarthritis (ASAS) response criteria,15 all of which primarily reflect spinal inflammation or spinal pain.
Although AS represents a well-defined entity, patients with AS present with a heterogeneous spectrum of inflammatory phenotypes, reflective of the extent of peripheral versus axial disease, and of the presence of other extra-articular inflammatory spondyloarthritis (SpA) manifestations.16 A recent systematic review demonstrated that 26% of patients with AS have a history of anterior uveitis, 9% psoriasis and 7% inflammatory bowel disease (IBD).17 Studies have indicated that the presence or absence of these extra-articular SpA manifestations in patients with AS do not (or only weakly) predict axial response to the TNFi.9 18–22 The same extra-articular SpA manifestations may however, by themselves, also constitute an indication for treatment with TNFi,23 24 and it may therefore be that the presence and activity of extra-articular SpA manifestations could be one of the factors that influence the long-term treatment outcome in clinical practice.
Other morbidities (eg, cardiovascular disease (CVD)25) also occur more often than expected in AS compared with the general population, but the effect of such comorbidities on TNFi drug retention has not been evaluated. However, smoking, which is associated with a number of chronic morbidities, as well as with socioeconomic status,26 has been associated with inferior response rates to TNFi27 and shorter TNFi drug retention in AS.6 Whether the reported detrimental effects of smoking on the performance of TNFi can be explained by comorbidities or is associated with socioeconomic factors have not been assessed.
The primary objective of this study was therefore to assess the impact of the extra-articular SpA manifestations (anterior uveitis, psoriasis and IBD) on the TNFi drug retention in AS. The secondary objective was to evaluate the relative significance of any observed effect, by comparing them with, and adjusting for, the effect of comorbidities and socioeconomic factors.
Methods
Study design
This is an observational, register-based, study on bio-naïve patients with AS in Sweden starting a first ever TNFi.
Data sources and definition of cases and exposures
Patients with AS were identified from the Swedish Rheumatology Quality register (SRQ), which has an estimated national coverage of 86%, for patients with SpA treated with biological disease modifying anti-rheumatic drugs (bDMARD).28 For this study, we identified all individuals with AS in the SRQ who started their first TNFi between 1 July 2006 and 31 December 2015. Data from SRQ were cross-linked to five other national registers: the national Patient Register, the Prescribed Drugs Register, the Population Register, the LISA register (socioeconomic database) and the Cancer Register, which are described in online supplementary table S1.
Supplemental material
Follow-up, censoring and baseline characteristics
Start of follow-up was the date of initiation of the first TNFi. End of follow-up was the date of discontinuation (if present) of the first TNFi, for any reason other than pregnancy or disease remission. Censoring was performed at whichever of the following that occurred first: death, emigration, discontinuation of the TNFi due to pregnancy or remission, no registered visit in the SRQ during a 2-year period, end of follow-up (31 December 2015), or, in the case of the subcutaneous TNFi, not having collected a prescription in 6 months. The rationale for censoring at 2 years after the most recent visit, and when not having collected a prescription in 6 months, was to avoid follow-up of individuals who were likely (though not directly proven) to have discontinued the treatment/follow-up by their own accord. Of all patients, only 9% were censored due to no visit in 2 years, and 8% due to no collected prescription in 6 months.
Characteristics at start of follow-up were collected from the closest available registered visit to the start date of the TNFi, within a period from 6 weeks before to 2 weeks thereafter. The following baseline characteristics were included: age, sex, C-reactive protein (CRP), BASDAI, ASDAS-CRP and other treatments (treated as binary variables): non-steroidal anti-inflammatory drugs (NSAIDs), conventional synthetic anti-rheumatic drugs (csDMARD) and glucocorticoids. Presence of a peripheral arthritis phenotype was determined based on any registration of ≥1 swollen joint (according to 66/68 joint index) during the year prior to TNFi start.
Extra-articular SpA manifestations, comorbidities and smoking
The primary objective was to assess the effect of the extra-articular SpA manifestations on drug retention; hence achieving a high detection rate for these exposures was paramount. While anterior uveitis and IBD are both managed mostly in specialised care, psoriasis is largely managed in primary care, and is therefore not covered by the national Patient Register. Therefore, the SpA manifestations were defined differentially through the Patient Register, based on International Classification of Diseases (ICD) codes, and/or the Prescription Register, based on Anatomic Therapeutic Chemical Codes (ATC codes). The definitions used, including the ICD codes and ATC codes, are detailed in online supplementary table S2. Anterior uveitis was defined as having been registered with this diagnosis in outpatient specialised care ever before the start date for the first TNFi. Similarly, IBD was defined as receiving such a diagnosis in either specialised inpatient care or outpatient care before the start of TNFi, whereas psoriasis was defined as either being diagnosed in specialised care or having collected a prescription of specific anti-psoriatic drugs.
Supplemental material
For the secondary objective, the exposure definition for each comorbidity was set to capture a spectrum of prevalent chronic morbidities with a potential impact on the cases’ health status, covered by a range of ICD diagnoses given in specialised care. If a considerable proportion of the patients with that particular exposure were expected to be treated mostly or exclusively in primary care, the definition was complemented with prescription data on relevant medications. For instance, CVD was defined as having received such a diagnosis during the 5 years prior to start of TNFi or to have collected both a prescription of an antihypertensive drug and a thrombocyte aggregation inhibitor in the last year. Similarly, diabetes and chronic lung disease were defined through a diagnosis in the last five years or a prescription in the last year. Affective disorder (depression and anxiety disorders) was defined only by prescription of antidepressives in the last year, and chronic kidney disease and malignancy only through ICD codes. Socioeconomic data (annual disposable household income), civil status (living without a partner vs other) and length of formal education (≤9 years, 10–12 years,≥13 years) at 31 December in the year before start of TNFi were retrieved from the Population Register, along with data on country of birth. In addition, the percentage of sick leave and disability pension were retrieved for 1 year prior to the start date for TNFi from the LISA register.
Statistics
The primary and secondary outcomes were assessed first through crude Kaplan-Meier curves, for each exposure at a time. Second, Cox regression was used to calculate univariable HRs for each exposure and to construct survival curves adjusted for sex and age at start of the first TNFi. The assumption of proportional hazard was assessed through visual inspection of the log-minus-log survival plots29 and by testing an interaction term between the exposure and follow-up time. Collinearity among the variables was assessed though correlation analysis and visual inspection of the distribution. Third, each exposure was separately entered in a proportional hazard ‘base model’ that was adjusted for those baseline characteristics that had a p value<0.2 as identified in the univariable analysis: age, sex, CRP (categorised as <10 or ≥10), presence of peripheral arthritis (yes or no), BASDAI (categorised as <4, ≥4 and missing) and type of TNFi drug. Fourth, the SpA manifestations were entered simultaneously in one model adjusted for the same factors as the ‘base model’, but also for the socioeconomic factors: disposable annual household income, length of formal education, country of birth and percentage of sick leave and disability pension. The SpA manifestations were also entered into a model adjusted for the same factors as the ‘base model’, but adding the comorbidities, and finally in a ‘full model’ containing both the baseline characteristics, comorbidities and socioeconomic factors.
Smoking status at start of TNFi has been associated with a poorer drug retention and may correlate with SpA manifestations (eg, psoriasis30), socioeconomic factors and several comorbidities. However, registrations of smoking status at baseline were incomplete, and not possible to adjust for in the regression models. Instead, smoking status was introduced separately in the ‘full model’ as a sensitivity analysis only including patients with smoking status registered prior to TNFi start.
Results
In total, 2577 patients with AS, starting a first ever TNFi between 1 July 2006 and 31 December 2015, were identified. Among these, a history of anterior uveitis was observed in 27%, IBD in 7% and psoriasis in 6%. table 1 describes demographic characteristics, morbidities and baseline disease activity measures.
Baseline descriptive data for 2577 patients with AS starting a first ever TNFi 1 July 2006 to 31 December 2015 in the nationwide Swedish Rheumatology Quality register
Extra-articular SpA manifestations as predictors of TNFi drug retention
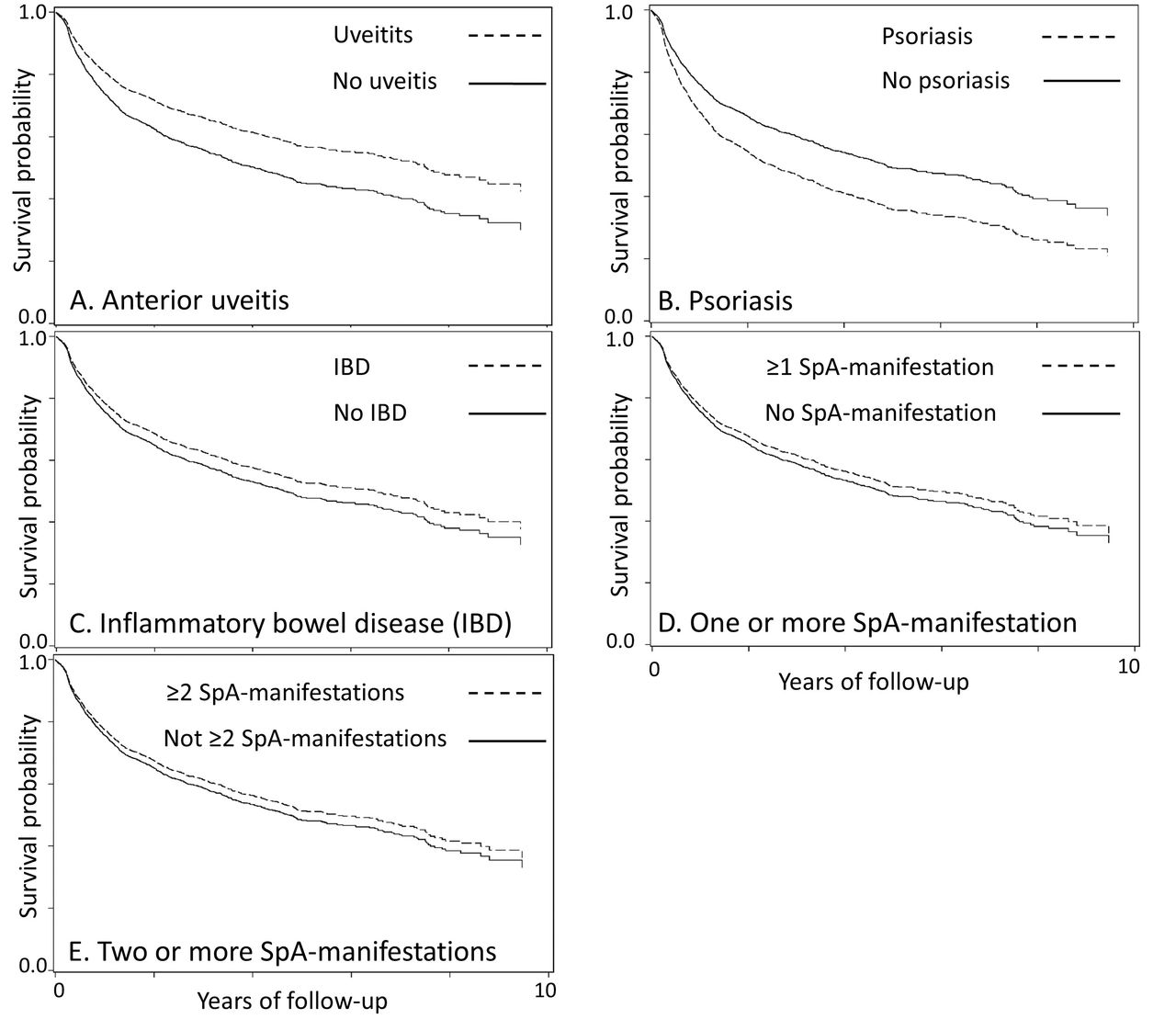
A history of anterior uveitis was associated with a superior TNFi drug retention, while psoriasis was linked to an inferior retention (figure 1). For IBD, no effect on TNFi retention was observed, nor did we find any effect related to the number of these SpA manifestations. For anterior uveitis, assessment of the proportional hazard assumption suggested non-proportionality in risk over time.

{kind=link}
Survival probability curves for drug retention of a first ever tumour necrosis factor alpha inhibitor (TNFi) in patients with ankylosing spondylitis (July 2006–December 2015), depending on presence of one or more extra-articular spondyloarthritis (SpA) manifestations. All curves are adjusted for sex and age at treatment initiation.
The HR (for drug discontinuation) associated with anterior uveitis was 0.72 (95% CI 0.62 to 0.83), but the association was largely confined to the first 1.5 years (HR 0.59 (95% CI 0.49 to 0.71)), rather than thereafter, HR 1.08 (95% CI 0.84 to 1.37) (table 2). For psoriasis (HR 1.48, 95% CI 1.18 to 1.86) and for IBD (HR 0.91, 95% CI 0.71 to 1.16), the associations did not vary over time.
Univariable HRs for discontinuing a first TNFi in patients with AS starting a first ever TNFi 1 July 2006 to 31 December 2015, in the nationwide Swedish Rheumatology Quality register
In the multivariable ‘base model’ adjusted for baselines characteristics, socioeconomic factors and, comorbidities, many of which were by themselves strong predictors of TNFi retention (table 2), we noted similar HRs for each SpA manifestations as in the univariable models, although with somewhat attenuated HRs for psoriasis (table 3). Adjusting for the presence of comorbidities, socioeconomic status and both (table 3) did not alter the HRs significantly. As expected, we observed collinearity between ASDAS versus CRP, and ASDAS versus BASDAI, and therefore we excluded ASDAS (which had more missing data than the other covariates) from the multivariable models.
HRs for discontinuing a first ever TNFi in patients with AS, depending on presence of extra-articular SpA manifestations, adjusted for baseline characteristics, comorbidities and socioeconomic factors
Comorbidities as predictors of TNFi drug retention
A history of CVD was the most common comorbidity (21%), followed by affective disorders (13%) and chronic lung disease (9%) (table 1). All these comorbidities and several socioeconomic factors (other than chronic kidney disease, which was only present in 1% of the patients) were negatively associated with TNFi retention (table 2). In particular, affective disorder, HR 1.81 (95%CI 1.54 to 2.13) and chronic lung disease, HR 1.49 (95% CI 1.22 to 1.82) increased the risk of discontinuing TNFi.
Sensitivity analysis
Data on baseline smoking status were available for 455 patients (18%), of whom 49% were registered as never-smokers, 14% as current smokers and 37% as former smokers. Introducing smoking status in the ‘full model’ described above, and limiting the analysis to only the patients with this data, resulted in similar HR for anterior uveitis: first 1.5 years HR 0.57 (95% CI 0.32 to 1.00; and for IBD: HR 0.64 (95% CI 0.25 to 1.64); but reduced the risk associated with psoriasis: HR 0.85 (95% CI 0.35 to 2.05).
Discussion
The results of our population-based and nationwide study suggest that typical extra-articular SpA manifestations (anterior uveitis, psoriasis and IBD) may affect drug retention in AS, but differently so and without any association with the number of individual SpA manifestations present. Our results also demonstrate the strong impact of comorbidities and socioeconomic factors on drug retention rates.
A few studies have included extra-articular SpA manifestations among the investigated predictors for TNFi treatment response on the axial disease in AS. In an observational study of 1250 patients with AS treated with adalimumab, psoriasis (12% of the cohort) had little effect on the overall axial treatment response.22 In two other studies, of 214 and 283 patients with AS treated with TNFi, the absence of psoriasis at treatment initiation predicted a higher chance of attaining partial remission, while the presence/absence of IBD or anterior uveitis did not affect this outcome.19 20 In one RCT, comparing etanercept to placebo in 277 patients with AS, anterior uveitis, psoriasis and IBD did not predict treatment response.18 Finally, another single-centre observational study of 70 patients with AS starting treatment with infliximab showed no statistically significant difference in the prevalence of anterior uveitis or IBD among responders compared with non-responders.9 Previously published results, based on smaller or substantially smaller numbers of patients, thus seem to point at no, or in case of psoriasis, a weak influence of the extra-articular SpA manifestations on the TNFi response for the axial disease. Our study, being considerably larger, extends these findings by assessing drug retention rather than initial axial response.
The baseline characteristics predicting persistence on TNFi treatment in our study are in line with previously published RCTs and observational studies, on TNFi response and retention: male sex,3 5 7–9 young age,5 8 21 31 32 elevated CRP3 5 7 21 31 32 and low BASDAI.7 Peripheral arthritis has previously been linked to a better drug retention,3 7 but was in our study associated with a slight increase in risk for discontinuation, HR 1.18 (95% CI 1.01 to 1.37), the reason for which is unclear.
Previous observational studies of AS have indicated differences in drug retention among the TNFi,8 which we confirm in this study (table 2). For the extra-articular SpA manifestations, there are also differences in efficacy among the different TNFi, for example, etanercept has been reported to have less effect on anterior uveitis,33–35 is ineffective in Crohn’s disease,36 and some data suggest that at conventional dosage it may also be less effective than adalimumab in psoriasis.37 In the current study, adjustment for type of TNFi (table 3, base model) attenuated the HR for psoriasis but not for anterior uveitis, and excluding etanercept altogether resulted in similar ratios for uveitis.
There are several possible explanations for our findings regarding the impact of extra-articular SpA manifestations on drug retention. First, these inflammatory manifestations could act as markers of AS disease activity, and thus predict a better treatment response in patients with a higher disease activity. For example, some data suggest that a history of anterior uveitis is associated with a higher axial disease activity.38 39 However, adjusting for baseline disease activity (table 3) did not alter our results significantly. Second, primary or secondary inefficacy on a concurrent SpA manifestation may also lead to discontinuation (see limitations below). A third explanation could be that the inflammatory phenotype, represented by the presence or absence of a SpA manifestation, may be caused by underlying differences in inflammatory pathways or genetic risk factors, which could affect drug retention.
Although the effect of the extra-articular SpA manifestations, on TNFi drug discontinuation remained after adjusting for comorbidities, we also found strong associations between these comorbidities and drug discontinuation. In our study, the 13% of patients treated for an affective disorder were at 80% increased risk of discontinuing their first TNFi and there were clear associations between socioeconomic status, such as annual income, workability and drug discontinuation.
This is the first study to assess the effect of SpA manifestations and comorbidities on the long-term TNFi drug retention in AS. Due to the high coverage of the Swedish national registers, we were able to identify a large number of patients, with a small risk of selection bias, and the generalisability of the results should be good.
However, the register-based approach introduces a number of limitations, primarily related to the risk of misclassification and lack of precision in the definitions of certain morbidities, but this should not affect the direction of the results. In this study, we could neither adjust for potential treatment responses for the extra-articular SpA manifestations themselves, nor determine to what extent these disease manifestations, or the presence of comorbidities, affected the decision to start the TNFi. This limitation may introduce a prescription bias, where patients with specific comorbidities are more or less likely to initiate TNFi, for example, physicians may be reluctant to start TNFi in patients with respiratory tract disorders or a history of malignancy, or more prone to start treatment earlier in patients with diabetes to avoid corticosteroids. As in all studies following patients treated according to clinical practice, the results must therefore be interpreted in light of this selection process. Since one of the main exposures, psoriasis, in less severe forms is largely managed in primary care, there is also a risk of under-ascertainment of this exposure. If the cases we did detect were more severe, then this might have resulted in an overestimation of the effect of psoriasis on TNFi drug retention. Further, smoking has been associated with a poorer TNFi drug retention in AS6 and may act as a confounder for drug discontinuation in patients with psoriasis.30 In this study, we could only adjust for smoking status in a subset of patients. Still, the diminished effect of psoriasis on drug retention, when adjusting for smoking, suggests that this effect is confounded by smoking status.
To conclude, a substantial number of patients with AS starting TNFi (in our study: one third) will also have SpA-related inflammatory disorders that may be responsive to TNFi treatment. While these extra-articular SpA manifestations may affect (differently so) the long-term outcome of TNFi treatment, there does not seem to be any association between the number of extra-articular SpA manifestations and remaining on TNFi. By contrast, our results highlight the importance of the treatment context, in addition to the treated disease, for treatment outcomes. Indeed, socioeconomic status, workability and comorbidities are as, or more, important as the AS disease itself in terms of longer-term treatment success. As such, they should receive due attention in clinical practice.
Acknowledgments
The ARTIS (Anti-Rheumatic Therapy in Sweden) study group has advised in the interpretation of results and completion of the study.
References
Footnotes
Contributors All authors have contributed substantially in the process of completing this study and had full access to the data, specified as follows: conception of the study: UL and JA. Designing the study: All authors. Aggregation of data and statistical analysis: UL. Interpretation of data: all authors. Drafting and revising, final approval and agreement to be accountable: all authors.
Funding The ARTIS Study Group conducts scientific analyses using data from the Swedish Biologics Register, run by the Swedish Society for Rheumatology. To this end, Karolinska Institutet has entered into agreements with Abbvie, BMS, Lilly, Merck, Pfizer, Roche, Samsung Bioepis, and UCB. These entities had no influence on the data collection, statistical analyses, manuscript preparation or decision to submit. Companies whose drugs were studied were allowed to comment upon the findings prior to submission although all final decisions resided with the investigators.
Competing interests JA has entered into agreements with Abbvie, BMS, Lilly, Merck, Pfizer, Roche, Samsung Bioepis, and UCB, mainly for safety monitoring via the Swedish ARTIS system (see above), and received a travel reimbursement from Novartis. Karolinska Institutet has received remuneration for JA’s participation in meetings arranged by Pfizer and by Lilly.
Patient consent Not required.
Ethics approval The regional ethical committee in Stockholm, Sweden, approved the study (dnr:2011/29-31/1).
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement Technical appendix and statistical codes are available from the corresponding author at request.