Article Text

Abstract
Objectives Disease Activity index for PSoriatic Arthritis (DAPSA) (sum score 68/66 tender/swollen joint counts (68TJC/66SJC), patient’s global assessment, pain and C-reactive protein (CRP)) is recommended for clinical assessment of disease activity in patients with psoriatic arthritis (PsA). Ultrasound (US) (grey scale (GS) and power Doppler (PD)) detects inflammation in joints and extra-articular structures. The present objectives were to explore the longitudinal relationships between DAPSA, clinical assessment as well as patient-reported outcome measures (PROMs) with US in patients with PsA initiating biological DMARDs and the associations between DAPSA and US remission.
Methods 47 patients with PsA were examined at baseline and after 3, 6, 9 and 12 months. Assessments included 68TJC/66SJC, examiner’s global assessment (EGA), PROMs, CRP, erythrocyte sedimentation rate (ESR) and US GS and PD (48 joints, 10 flexor tendons, 14 entheses, 4 bursae). Clinical composite scores and PD sum scores (0=remission) were calculated. Longitudinal associations were explored by generalised estimating equations with linear and logistic regression.
Results DAPSA was not longitudinally associated to PD. 66SJC, ESR, 28-joint Disease Activity Score, EGA and CRP were longitudinally associated with PD (p<0.001–0.03), whereas the pain-related components of DAPSA (68TJC and pain) as well as PROMs were not associated. At 6–12 months, remission was achieved in 29%–33 % of the patients for DAPSA and 59%–70 % for PD. The association between DAPSA and PD remission was not significant (p=0.33).
Conclusions DAPSA was not associated with US inflammatory findings which indicates that DAPSA and US may assess different aspects of PsA activity.
- psoriatic arthritis
- ultrasonography
- bDMARDs
- patient perspective
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Key messages
What is already known about this subject?
Recent studies have demonstrated discrepancy between clinical and ultrasound (US) measures of inflammation in patients with psoriatic arthritis (PsA).
What does this study add?
Our longitudinal study of patients with PsA starting treatment with biological disease-modifying antirheumatic drugs demonstrated no significant association between clinical composite score Disease Activity index for PSoriatic Arthritis (DAPSA) and ultrasound power Doppler (US PD) in assessment of both disease activity and remission. While DAPSA was mostly influenced by tender joint count and pain, US PD showed low level of inflammation and was associated with other objective signs of inflammation and not with patient-reported outcome measures (PROMs).
How might this impact on clinical practice?
Our study underlines the importance of US assessment in addition to clinical evaluation of patients in treat-to-target strategy in PsA to assess the ongoing inflammation comprehensively, especially when evaluating patients with higher levels of PROMs and lower levels of objective measures of inflammation.
Introduction
Psoriatic arthritis (PsA) is a chronic inflammatory disease with a prevalence of 0.20%–0.67% in Norway.1 It includes inflammation of peripheral joints, tendons, bursae and entheses as well as axial skeleton and skin. The heterogenic nature of the disease poses a great challenge for clinical examinations as well as developing treat-to-target strategies, which is essential when monitoring patients regarding the efficacy of biological disease-modifying antirheumatic drugs (bDMARDs).
Evaluation of PsA activity is based on measures of inflammation including joint counts, laboratory measures and examiner’s evaluations as well as subjective measures including pain and patient global assessment (PGA). In addition, several other patient-reported outcome measures (PROMs) are used for addressing function, quality of life and mental health. Discrepancies in assessing disease activity have been reported between the more objective and the patient-reported measures of disease activity both in rheumatoid arthritis (RA)2 3, and recently also in PsA.4 In addition to inflammation, the patient perspectives may be influenced by factors like joint damage, degenerative changes, central sensitisation, mental health (eg, anxiety and depression) and illness perception.5–9
Several composite scores have been developed in the past years including both subjective and objective measures to provide more comprehensive tools for disease assessment in PsA. Recent recommendations by an international task force suggested the use of the Disease Activity index for PSoriatic Arthritis (DAPSA) in evaluation of the musculoskeletal domain of the disease.10 DAPSA is the numerical sum of 66 swollen and 68 tender joint counts, pain, PGA (pain and PGA scored on a 0–10 scale) and C-reactive protein (CRP (mg/dL)).11 It can be used for evaluation of disease activity and includes cut-offs for different disease activity states including remission.12 DAPSA has been validated in clinical trials and shown to be responsive to treatment.11 13 However, patient’s evaluations have a major contribution to the index score. To which extent DAPSA is reflecting inflammatory disease activity as assessed by ultrasound (US) has not been studied in longitudinal observational cohorts.
US is increasingly implemented by clinicians as an important additional tool for assessing pathology in inflammatory joint diseases, and several studies of PsA patients have proven US to be a valid, sensitive and reliable tool in assessing inflammation.14 Recent European League Against Rheumatism recommendations support the use of imaging in the diagnosis and monitoring of disease activity in PsA.15 Inflammation in joints, tendons, bursae and entheses may be assessed by use of grey scale (GS) changes and vascularisation by use of power Doppler (PD) activity, where PD is considered to be the best proxy to active inflammation.16–19 US is sensitive to differentiate between active lesions and structural damage within the entheses20 and also detects response to therapy,21 which is important for treatment decisions. On the other hand, clinical evaluations have been shown quite unreliable in this regard due to low specificity.22
Recent cross-sectional US studies in patients with PsA have pointed out a discrepancy between clinical and US measures as well as low association between clinical composite scores like DAPSA and US scores.23 24 With emphasis on the present use of clinical composite scores in the treat-to-target strategy of patients with PsA, there is a need for longitudinal studies exploring the associations between clinical composite scores and US assessments for evaluation of disease activity in patients with PsA. The objectives of this study were to explore the longitudinal relationships between DAPSA, the clinical assessments of individual components of DAPSA as well as PROMs with an US score based on a comprehensive US examination in patients with PsA initiating bDMARDs. We also aimed to study the concordance between remission defined by DAPSA and US.
Patients and methods
Patients
A total of 47 PsA patients fulfilling the Classification Criteria for Psoriatic Arthritis25 were consecutively included in this single centre study after referral from their treating rheumatologist during a period from December 2011 to March 2015. Comprehensive examinations including PROMs, clinical, laboratory and US assessments were performed at baseline and after 3, 6, 9 and 12 months.
The study was registered (ClinicalTrials.gov identifier: NCT01219257).
Patient-reported outcome measures
The patients scored pain and PGA during the last week on visual analogue scales (VAS, 0–100). Physical function was assessed by use of Modified Health Assessment Questionnaire (MHAQ, range 0–3)26, and general disease symptoms were assessed by use of Bath Ankylosing Spondylitis Disease Activity Index (BASDAI, range 0–10).27 The Rheumatoid Arthritis Impact of Disease (RAID, range 0–10),28 was included as a general patient-reported score for seven domains, since this study was initiated before publication of the Psoriatic Arthritis Impact of Disease (PsAID) questionnaire.29 However, the questions in RAID are to a large extent comparable to PsAID. The Hospital Anxiety Depression Scale (HADS) was used to assess depression and anxiety.30
Clinical and laboratory assessments
A study nurse with more than 20 years of experience with joint counts in clinical studies, unaware of US results, assessed 68/66 joints for tenderness and swelling, respectively, performed clount of digits affected by dactylitis31 and scored examiner’s global assessment of disease activity (EGA, VAS 0–100). Disease duration (time since disease diagnosis) and years of formal education were also recorded. Axial involvement was retrospectively determined by medical chart review as presence of abnormal findings by MRI or conventional radiographs of spine and/or sacroiliac joints. Erythrocyte sedimentation rate (ESR; mm/hour) and CRP (mg/L) were analysed locally by in-house standard methodology.
Clinical composite scores of disease activity
Clinical composite scores of disease activity were calculated at each visit including DAPSA11 and Disease Activity score for 28 joints with ESR (DAS28ESR), developed for RA, but also used for patients with PsA.32 33 DAPSA remission was defined as ≤4 (12) and DAS28 remission as <2.634 Boolean remission definition modified for PsA (68 tender joint count, 66 swollen joint count, dactylitis count, CRP (mg/dL) and PGA (VAS 0–10), all ≤1) was also explored.35
Ultrasonography
One out of two rheumatologists (PBK and HBH), performed the US examinations on the same day as the clinical assessments, but blinded for these results, by use of a GE Logiq E9 machine (GE Medical Systems Ultrasound and Primary Care Diagnostics, Wauwatose, Wisconsin, USA) equipped with a 6–15 MHz linear probe. The two sonographers have previously shown high agreement on US scoring.36 Complete US scoring protocol is described in the online supplementary file S1. In brief, a total of 48 joints were assessed by use of standard projections37 including bilateral wrist (radiocarpal, midcarpal, radioulnar joints scored separately), metacarpophalangeal 1–5, proximal interphalangeal 1–5, elbow, hip, knee, ankle (talocrural joint), talonavicular, posterior subtalar and metatarsophalangeal 1–5 joints. Ten finger flexor tendons (bilateral digits 1–5) were also assessed. GS and PD abnormalities for joints and tenosynovitis were scored semiquantitatively graded 0–3.36 38 39
Supplemental material
A total of 14 entheses were assessed (lateral epicondyle, triceps, distal quadriceps, proximal and distal patellar, Achilles and plantar fascia bilaterally). GS signs reflecting active inflammation were in all entheses evaluated as increased thickness (scored 0–1) as well as hypoechogenicity (scored 0–3) (except for plantar fascia) according to recently published definition of elementary components of enthesitis.20 40 On the other hand, GS signs reflecting chronic changes20 40 were evaluated as calcifications, enthesophytes and erosions (see online supplementary file S1). PD activity in entheses (defined as <2 mm from the bone surface)20 was scored 0–3.
Four bursae were also assessed (deep infrapatellar and retrocalcaneal bursae bilaterally) and scored by GS (size) and PD (inflammatory activity) (0–3).
Total sum scores indicating inflammation were calculated separately for GS and PD including joint synovitis, tenosynovitis, enthesitis and bursitis (range 0–236 and 0–222, respectively). In addition, a GS entheses chronicity sum score was calculated including enthesophytes size/number, erosions size/number and calcifications (range 0–210). US remission was defined as total PD sum score of zero.
Statistical analysis
Descriptive statistics were used to summarise the data. Patients’ baseline characteristics are presented as means with SD for normally distributed and as medians with 25th–75th percentiles for non-normally distributed variables. Clinical composite scores were calculated.11 32 Quantitative results were compared using Mann-Whitney U test. Proportions were analysed using the Χ2 test.
Correlations were assessed using Spearman’s rank correlation test due to non-normal distribution of most variables, with 95% CIs for the correlation coefficients calculated using bootstrapping with 1000 replications.
Longitudinal analyses were performed by generalised estimating equations (GEE), using linear or logistic regression where appropriate. GEE was used to include all available data and account for intrasubject correlations on repeated measurements. The analyses were adjusted for age at baseline, gender and years of disease duration. Time was treated as a categorical variable in all analyses.
Standardised beta coefficients were estimated by applying the GEE modelling to standardised variables. Responses to treatment were explored by standardised response means (SRMs, mean change divided by the SD of the change) with confidence intervals estimated using bootstrapping with 5000 replications Results are presented as all observed data, without imputation for missing values. P values ≤0.05 were considered significant. Statistical tests were performed using SPSS V.21.0 for Windows.
Results
A total of 47 patients (68% biologic-naïve and 32% single or multiple biologic-switchers) were consecutively included in the study (table 1).
Demographic characteristics of the patients (n=47)
Number of patients completing the predetermined study period was 43 (91.5 %) at 3 months, 37 (78.7%) at 6 months, 34 (72.3%) at 9 months and 32 (68.1%) at 12 months (the results for 12 months follow-up are illustrated in table 2.
Longitudinal scores over the 12-month follow-up period
Baseline characteristics did not differ significantly between patients completing versus not completing the 12-month follow-up except for longer formal education years in completers (p=0.014).
Cross-sectional correlations at baseline
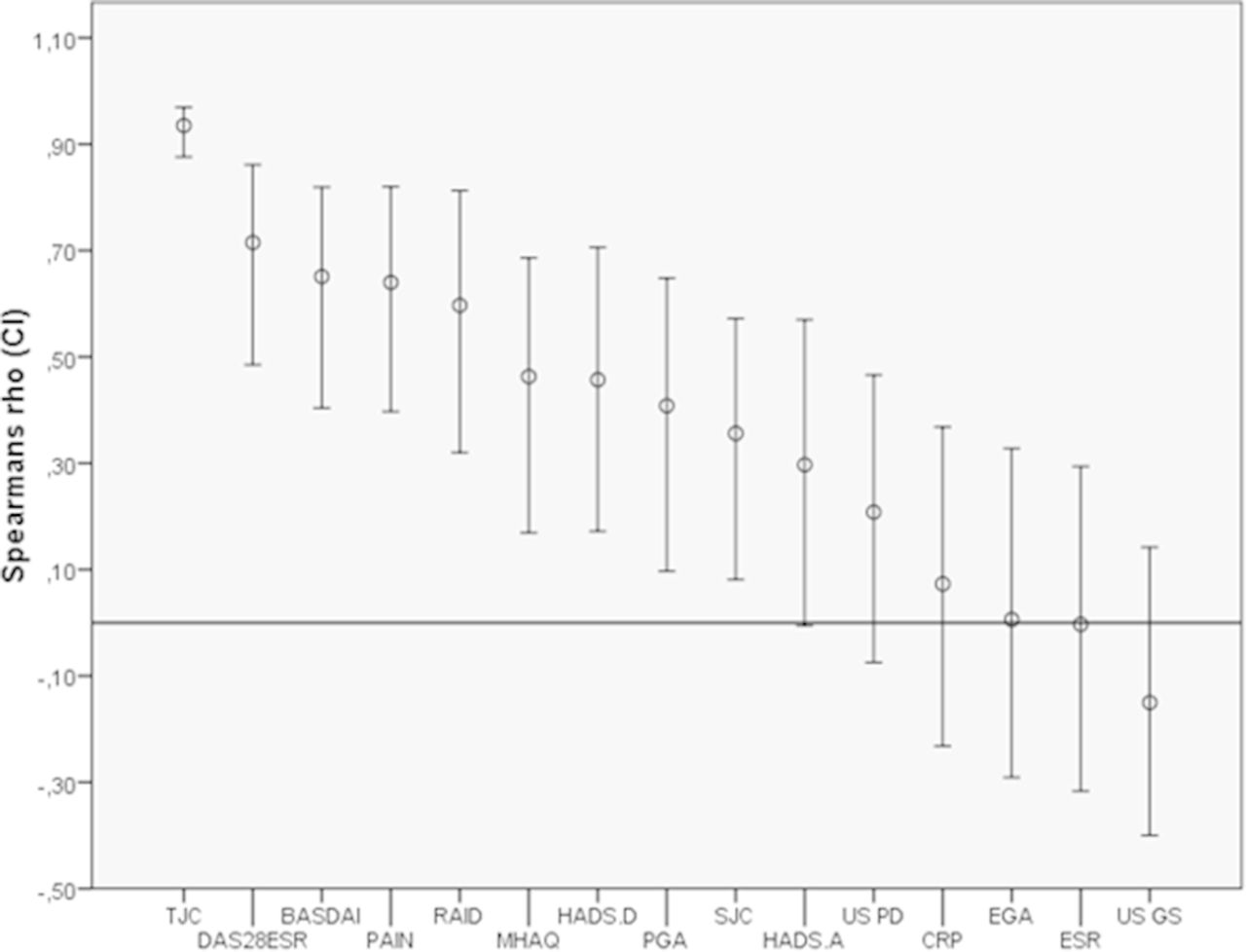
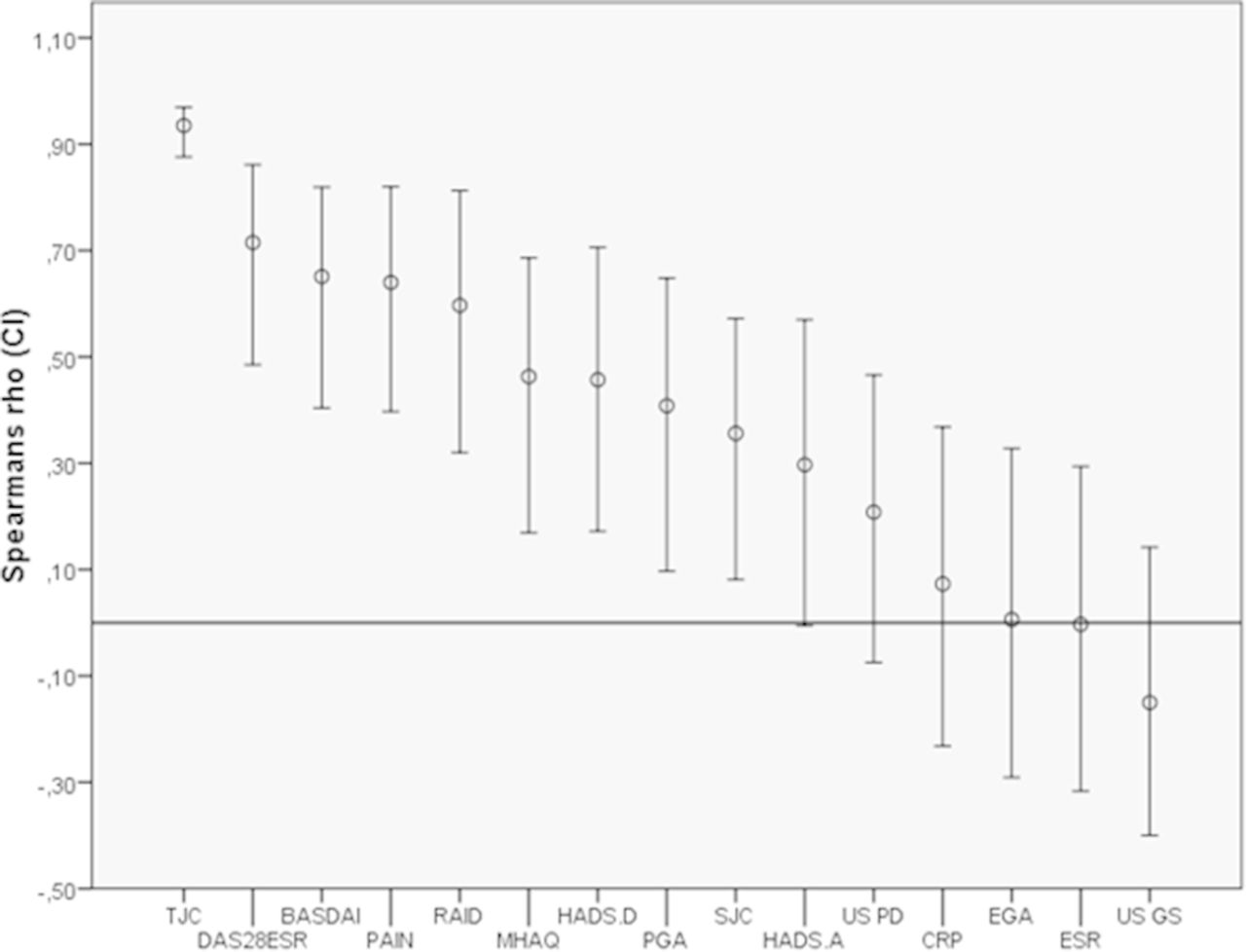
Figure 1 illustrates the baseline cross-sectional correlations between DAPSA and clinical variables, ESR/CRP, PROMs and US. DAPSA had the highest correlation with TJC (r=0.94 (CI 0.88 to 0.97), p<0.001). Significant correlations were also found between DAPSA and pain, DAS28ESR, BASDAI, RAID, MHAQ, HADS depression, PGA and SJC, but there were no significant correlations between DAPSA and ESR/CRP or GS/PD US. The PD sum score was significantly correlated with the GS sum score (0.65 (0.45 to 0.79), p<0.001), SJC (0.49 (0.26 to 0.71), p<0.001), DAS28ESR (0.35 (0.09 to 0.61), p=0.015) and EGA (0.29 (0.02 to 0.53), p=0.05), but not with ESR/CRP, TJC or any of the PROM`s.
{kind=link}
Cross-sectional correlations between DAPSA and clinical variables, PROMs and US scores at baseline. BASDAI, Bath Ankylosing Spondylitis Disease Activity Index; CRP, C-reactive protein; DAS28ESR, Disease Activity Score for 28 joints with ESR; EGA, examinator's global assessment; ESR, erythrocyte sedimentation rate; HADS.D, The Hospital Anxiety Depression Scale—depression; HADS.A, The Hospital Anxiety Depression Scale—anxiety; TJC, tender joint count; MHAQ, Modified Health Assessment Questionnaire; PAIN, patient's pain; PAIN, patient's pain; PGA, patient's global assessment; RAID, Rheumatoid Arthritis Impact of Disease; SJC, swollen joint count; US PD, ultrasound power Doppler; US GS, Ultrasound Grey Scale.
Standardised response mean SRMs of clinical, laboratory and US assessments
The patients improved across the majority of clinical, laboratory and US variables as well as clinical composite scores during bDMARD treatment (table 3).
Standardised response mean with 95% CI (bootstrap with 5000 replications) with changes from baseline
EGA had the highest SRM at all time points. DAPSA as well as other composite scores had high overall SRMs while sum scores of inflammatory GS and PD had lower levels. However, the GS sum score of chronic changes in entheses did not change during the study.
Longitudinal associations with US PD or DAPSA as dependent variable
Table 4 illustrates significant longitudinal association with US PD as the dependent variable and US GS, SJC, DAS28ESR, EGA and ESR/CRP. There were no significant associations with DAPSA or PROMs.
Longitudinal associations with US PD as dependant variable*
Table 5 illustrates strong longitudinal associations between DAPSA and PROMs and weak associations between DAPSA and EGA, SJC and ESR/CRP.
Longitudinal associations with DAPSA as dependant variable*
No longitudinal association was found between DAPSA and US PD or GS inflammatory sum scores. TJC was the individual component of DAPSA found to have the highest contribution to DAPSA change (standardised β 0.88, p<0.001), followed by PAIN (standardised β 0.52, p<0.001).
Remission by clinical composite scores and US PD
At 6, 9 and 12 months follow-up, remission was found in 27.3%–33.3% for DAPSA, 54.5%–58.1% for DAS28ESR, 21.2%–27% for Boolean and 59.4%–69.7% for US PD remission. PD remission was longitudinally associated with DAS28ESR remission (OR 2.1, 95% CI 1.2 to 3.8, p=0.016), while no significant association was found with DAPSA or Boolean’s remission.
Discussion
The present study highlights some of the challenges related to using relevant outcome measures in a treat-to-target approach in patients with PsA. We found that DAPSA had cross-sectionally and longitudinally strong associations with PROMs, especially with TJC and pain as its individual components. On the other hand, DAPSA had low association with clinical signs of inflammation and no associations with US scores. US PD was associated with clinical signs of inflammation, but not with any of the PROMs. US scores were generally low, but decreased significantly during the study. Remission was found in twice as many for US PD than for DAPSA at follow-up. However, there was no association between these two assessments of remission.
Studies of patients with RA have shown that subjective measures of disease activity correlate more strongly with objective measures including US in high disease activity states, but this relationship is weaker in patients with lower disease activity and remission as well as in presence of comorbidities that strongly influence the subjective component such as fibromyalgia.41 42 The patients in the current study had low inflammatory activity as evaluated by objective assessments, and DAPSA scores were found to be strongly associated to TJC and pain. Although pain ideally reflects inflammation, the present discrepancy with US findings may indicate that in this study pain could also have other explanations than inflammation. Earlier investigations have reported discordance between inflammation and pain in RA2 confirming that decreased inflammation in arthritis is not always associated with decreased pain. A recent study found global pain, joint pain and PGA to be higher in PsA than in RA43, and in the present study, the levels of PGA and pain were high compared with signs of inflammation including US. It is proposed that PGA and pain are components of DAPSA that account indirectly for skin involvement and axial disease, and thus capture more than just the peripheral joint pathology.44 However, in our cohort, only one third of the patients had documented axial involvement.
US is a valid and reliable tool for assessing inflammation in joints, tendons and entheses with comparable sensitivity to MRI.45 US PD may be considered as the best proxy for ongoing inflammation16–18 and was presently used as the gold standard for inflammation whereas US GS entheseal thickening and hypoechogenicity may also represent chronic pathology rather than only inflammatory activity . In this study, rheumatologists experienced in US performed comprehensive US examinations using a high-end US machine. Thus, we may assume that the present findings reflect the overall inflammatory activity and serve as a good comparator to clinical disease assessments which is also supported by the significant associations between clinical signs of inflammation and US PD scores.
Recent cross-sectional PsA studies support our findings showing US variables to have only weak associations with clinical assessments, PROMs and DAPSA.4 23 24 Still, it remains open for further research whether US imaging is sensitive enough to detect all the pathological changes in PsA. A recent high-resolution MRI study of fingers in PsA dactylitis has shown inflammatory activity in miniature entheses of flexor tendon pulleys and sheaths.46 These findings confirm the enthesitis as a primary pathological abnormality in PsA. It remains open whether such findings could explain the enhanced pain in other body areas, although studies of axial SpA which used spine MRI for comparison with clinical composite scores found no or minor correlation between these two measures of disease activity.47
The treat-to-target strategy principle has remission or LDA as a target which is outlined in the recent treat-to-target recommendations for management of PsA and axial spondyloarthritis.10 Early suppression of inflammation prevents progression of joint damage and sustains functional ability. Yet, in our study, only one third of the patients reached clinical composite scores remission despite two thirds reached PD remission. This is striking, since US PD remission reflects no inflammatory activity by a comprehensive assessment. In addition, the US PD and DAPSA remission criteria had no significant longitudinal association. Thus, similar to what has been shown in RA, this discordance of clinical composite score remission and US remission seems to reflect different forms of pathologies, at least on a group level.48
To the best of our knowledge, the present study is the first to explore the longitudinal relationships between clinical and US variables in patients with PsA starting bDMARDs. A major strength of the study is the comprehensive US examination as well as the real-life inclusion of consecutive patients starting bDMARDs. Furthermore, the use of GEE statistical analyses accounted for missing data and within-subject correlations. The limitations include the one centre design which may limit the generalisability of our findings. Another limitation is the lack of randomisation between the current intervention and a control group. Dactylitis was presently not evaluated by US because of no established US definition at study initiation and we did not include skin assessments. Distal interphalangeal (DIP) joints were not included since osteoarthritis abnormalities are common in these joints, and these osteoarthritic abnormalities may be difficult to differentiate from PsA. A limitation is the small number of patients included, however, they were all extensively assessed. Another potential limitation is the low level of inflammation in our patients, which could have influenced the associations in the study. Nevertheless, the patients had clinical indication for initiating bDMARD, and they were thus evaluated to have high disease activity. Other disease activity scores like PASDAS and CPDAI would have been relevant to include, but they were published after the initiation of our study.49
In conclusion, in our cohort, DAPSA was mainly influenced by TJC and pain and was not associated with US inflammatory findings. These results show a discrepancy between DAPSA and US, indicating that the two assessments may reflect different aspects of disease activity. This observation indicates that US assessment may be complimentary to clinical measures in a treat-to-target strategy in patients with PsA. However, this assumption needs to be tested further in a randomised controlled strategy trial.
Acknowledgments
SP acknowledges the European League Against Rheumatism (EULAR) for a scientific training bursary for 6 months, enabling data entry, statistical analyses and writing the manuscript.
References
Footnotes
Contributors HBH, PBK, TKK: were responsible for study design. HBH, PBK, BM, JS, SP: were involved in acquisition and/or interpretation of the data. SP: analysed the data and wrote the draft manuscript. All authors critically revised the manuscript and approved the final version.
Funding The data collection was supported by AbbVie in form of study grant to the Department of Rheumatology, Diakonhjemmet Hospital, Oslo, Norway by Hilde Berner Hammer.
Competing interests HBH has received fees for speaking and/or consulting from AbbVie, BMS, Pfizer, UCB, Roche, MSD, Lilly and Novartis, and received research funding to Diakonhjemmet Hospital from AbbVie, Pfizer and Roche. TKK has received fees for speaking and/or consulting from AbbVie, BMS, Boehringer Ingelheim, Celgene, Celltrion, Eli Lilly, Hospira, Merck-Serono, MSD, Novartis, Orion Pharma, Pfizer, Roche, Sandoz and UCB and received research funding to Diakonhjemmet Hospital from AbbVie, BMS, MSD, Pfizer, Roche and UCB.
Patient consent Obtained.
Ethics approval Norwegian Regional Committee for Medical and Health Research Ethics South East (reference number 2010/2658a).
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement No additional data are available.