Article Text

Abstract
Objective This analysis explored the association of treatment adherence with beliefs about medication, patient demographic and disease characteristics and medication types in rheumatoid arthritis (RA), psoriatic arthritis (PsA) or ankylosing spondylitis (AS) to develop adherence prediction models.
Methods The population was a subset from ALIGN, a multicountry, cross-sectional, self-administered survey study in adult patients (n=7328) with six immune-mediated inflammatory diseases who were routinely receiving systemic therapy. Instruments included Beliefs about Medicines Questionnaire (BMQ) and 4-item Morisky Medication Adherence Scale (MMAS-4©), which was used to define adherence.
Results A total of 3390 rheumatological patients were analysed (RA, n=1943; PsA, n=635; AS, n=812). Based on the strongest significant associations, the adherence prediction models included type of treatment, age, race (RA and AS) or disease duration (PsA) and medication beliefs (RA and PsA, BMQ-General Harm score; AS, BMQ-Specific Concerns score). The models had cross-validated areas under the receiver operating characteristic curve of 0.637 (RA), 0.641 (PsA) and 0.724 (AS). Predicted probabilities of full adherence (MMAS-4©=4) ranged from 5% to 96%. Adherence was highest for tumour necrosis factor inhibitors versus other treatments, older patients and those with low treatment harm beliefs or concerns. Adherence was higher in white patients with RA and AS and in patients with PsA with duration of disease <9 years.
Conclusions For the first time, simple medication adherence prediction models for patients with RA, PsA and AS are available, which may help identify patients at high risk of non-adherence to systemic therapies.
Trial registration number ACTRN12612000977875.
- adherence
- ankylosing spondylitis
- disease-modifying antirheumatic drugs
- psoriatic arthritis
- rheumatoid arthritis
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0
Statistics from Altmetric.com
- adherence
- ankylosing spondylitis
- disease-modifying antirheumatic drugs
- psoriatic arthritis
- rheumatoid arthritis
Key messages
What is already known about this subject?
Adherence to therapy in patients with rheumatic diseases is important for successful outcomes, highly variable, often suboptimal and difficult to predict.
What does this study add?
The ALIGN study explored the association of patient factors with adherence to medications in a population with immune-mediated inflammatory diseases, including rheumatoid arthritis (RA), psoriatic arthritis (PsA) and ankylosing spondylitis (AS).
In ALIGN, medication adherence in RA, PsA and AS depended more on treatment beliefs than disease-related factors.
Results from ALIGN showed that adherence was predicted by current medication type, treatment beliefs, age and race or disease duration.
How might this impact on clinical practice?
Simple models, developed from the ALIGN data, are available and may help identify patients with RA, PsA and AS at high risk of non-adherence to systemic therapies.
Introduction
In rheumatic diseases, adherence to therapy is critical to achieving optimal outcomes1–3 and lowering non-pharmacy healthcare costs.4 5 Adherence varies widely, depending on the particular rheumatic disease, the definition of adherence and the type of treatment. Nonetheless, adherence appears to be suboptimal; in a systematic literature review, values for the proportion of adherent patients ranged from 34% to 93% for rheumatoid arthritis (RA), 45% to 76% for psoriatic arthritis (PsA) and 75% for ankylosing spondylitis (AS).6 Adherence for rheumatic and other chronic diseases is influenced by many factors, including patients’ beliefs about the necessity of treatment and concerns about potential adverse effects.7 Beliefs about and adherence to systemic medication depend on patient characteristics (eg, age, race and sex), disease characteristics, treatment experience and treatment patterns, although previous analyses have produced inconsistent results.8–16 Despite evidence about factors being associated with poor or high medication adherence in patients, identification of patients at high risk of non-adherence remains difficult. A probabilistic adherence prediction model could help rheumatologists identify patients with RA, PsA and AS who are at high risk of non-adherence to systemic therapies. Interventions that influence medication adherence according to such a model, by addressing modifiable factors like patients’ beliefs, could help maximise adherence. However, little specific information is available about the association between medication adherence and patients’ beliefs regarding conventional synthetic disease-modifying antirheumatic drugs (csDMARDs) and tumour necrosis factor inhibitors (TNFis) in RA, PsA and AS as well as non-steroidal anti-inflammatory drugs (NSAIDs) in AS.
The ALIGN study determined patients’ specific and general beliefs towards medications and adherence to selected systemic therapies in six immune-mediated inflammatory diseases (IMIDs) and explored the association of treatment beliefs and other factors with medication adherence.16 The objective of this analysis was to explore the association of patient characteristics and attitudes with adherence to csDMARDs and TNFis in the subset of ALIGN patients who had RA, PsA and AS as well as adherence to NSAIDs in patients with AS and to develop models that predict adherence to systemic therapy in each of these three rheumatic IMIDs based on the strongest significant associations.
Methods
Study design and patients
ALIGN was a cross-sectional patient survey study conducted across Europe, Canada, Latin America, the Asia-Pacific region and the Middle East between June 2012 and October 2013.16 Patients provided consent according to the Declaration of Helsinki. Consecutive patient recruitment was carried out if patients agreed to participate and met eligibility criteria.16 A total of 7328 adult patients with RA, PsA, AS, psoriasis, Crohn’s disease or ulcerative colitis were enrolled if they were receiving conventional and/or biological therapy as part of routine management for their moderate to severe IMIDs, including any csDMARD, NSAID (patients with AS only), glucocorticoid (GC) and/or TNFi. Prior enrolment in a registry was neither required nor an exclusion criterion.
Study assessments
Assessment methods have been previously reported in detail.16 Investigators recorded patient demographics (eg, age, sex and race (white/Caucasian, black, Asian, Hispanic, other)), disease characteristics (eg, IMID diagnosis, duration of disease and symptoms since diagnosis and activity (collected as ‘severity’) based on investigator opinion (mild, mild to moderate, moderate, moderate to severe and severe)) and treatment-related variables (eg, current and prior treatment and response based on investigator opinion (complete, partial, no and inevaluable)) on a case report form. Other assessments (eg, questionnaires) were patient-reported. Patients’ illness perceptions were measured by using the Brief Illness Perception Questionnaire (BIPQ) which consisted of eight questions that assessed the cognitive and emotional aspects of illness perception using a 0 to 10 scale.17 The BIPQ has been used in many studies with a wide range of patient groups.18 Validation of the BIPQ showed that it has good test–retest reliability, with Pearson correlation coefficients ranging from 0.42 to 0.75 depending on the question and length of time between the initial test and the retest.17 The Beliefs about Medicines Questionnaire (BMQ) using a 5-point Likert scale (1=strongly disagree; 5=strongly agree; multiplied by a factor of 5 for this study) was administered to assess general (Overuse and Harm subscales) and specific (Concerns and Necessity subscales) beliefs about medicines.19 Treatment adherence was based on responses to the 4-item Morisky Medication Adherence Scale (MMAS-4©),20 which was derived from the Morisky, Green and Levine adherence scale.20 21 Four questions were asked: (1) Do you ever forget to take your medicine? (2) Do you ever have problems remembering to take your medication? (3) When you feel better, do you sometimes stop taking your medicine? and (4) Sometimes if you feel worse when you take your medicine, do you stop taking it?, with yes=0, no=1 and a total score range of 0 to 4. The MMAS-4© has been shown to be a useful, reliable and valid measure of treatment adherence, with good sensitivity (0.81) and moderate specificity (0.44).20 21
Statistical analysis
Treatments
Patients were grouped based on the treatments they were receiving for RA, PsA and AS at the time of the study visit. The following treatment categories were considered relevant for all three IMIDs: csDMARD therapy (csDMARDs±GCs), TNFi monotherapy (TNFi±GCs) and csDMARD-TNFi combination therapy (TNFi+csDMARDs±GCs). csDMARDs were defined as sulfasalazine, leflunomide, hydroxychloroquine or methotrexate in patients with RA, PsA and AS and cyclosporine in patients with PsA. For AS only, additional categories were also defined because NSAIDs are a cornerstone of treatment in this IMID:22–24 NSAID monotherapy (NSAIDs±GCs), NSAID-csDMARD combination (NSAIDs+csDMARDs±GCs) and NSAID-TNFi combination (NSAIDs+TNFi±GCs). NSAIDs were not included as part of the treatment categories for RA and PsA because they are supportive therapies in these IMIDs but are not disease modifying.
To compare patient-reported high adherence (MMAS-4© score=4) to a particular medication among the three IMIDs, a multivariable logistic regression model was constructed with factors for IMID (RA, PsA or AS) and each possible kind of treatment. It was possible to compare adherence only to treatments that were evaluated in more than one IMID, hence, NSAIDs were not modelled. To account for within-patient correlations, a random-effects model was used. The reference IMID was PsA, which bears clinical resemblances to RA and AS, and the reference treatment was TNFi monotherapy.
Attitudinal segmentation
The BMQ-Specific Necessity and Concerns subscale ratings were analysed in four attitudinal segments, similar to the analysis by Aikens et al.25 On a scale from 5 to 25, the attitudinal segments were defined as: accepting, with BMQ-Specific Necessity score ≥15 and BMQ-Specific Concerns score <15; ambivalent, with both scores ≥15; indifferent, with both scores <15 and s k eptical, with BMQ-Specific Necessity score <15 and BMQ-Specific Concerns score ≥15.
Regression analysis of factors associated with medication adherence
Potential associations of data from study assessments with patient-reported high adherence were assessed by multivariable logistic regression models. The full model included factors for each study assessment. A further exploratory analysis included full models plus the addition of fixed factors for geographic region. For combination therapy, separate ratings of adherence were performed for each treatment component received by the patient. To develop a final model, p value-based backward selection approaches (ie, removal of variables based on p>0.05) were applied to eliminate extraneous factors from the final adherence prediction regression models; this approach automatically selected an adequate complexity for the model based on the observed data. Although backwards selection based on p values was used, factors identifying treatment groups were always kept in the models, regardless of statistical significance, as this was important for the design of the analysis. Furthermore, to account for potential within-patient correlations, the final models were then refitted with a random-effects logistic model with patient indicator as a random intercept. This final refitting procedure was conservative in its treatment of predictors, so that only the most informative variables were likely to remain significant.
Adherence prediction modelling
Two separate approaches were used to independently develop two distinct models to predict medication adherence in patients with RA, PsA and AS. The first approach was automated and aimed to construct, for each IMID (RA, PsA and AS), a model with up to 10 variables with the highest possible predictive power. In this more complex approach, candidate models were developed from the most important factors (based on ORs for risk of non-adherence and practical considerations) for the individual IMIDs in the multivariable regression analyses. The three reference models for RA, PsA and AS, which had the greatest predictive power, comprised as many continuous variables as possible. Beginning with a full model, the backward selection algorithm removed, based solely on statistical estimates (ie, without subjective knowledge), the variable with the largest p value. Then, in stepwise fashion, it continued removing variables by the same rule, stopping when all remaining variables had p values less than the prespecified criterion (here, 0.05). Therefore, the complexity (number of variables) in the final model was determined automatically by the algorithm, without human intervention. Whenever feasible while maintaining adequate predictive accuracy, the models were simplified by dividing continuous factors into dichotomous variables. The final model for each rheumatic disease was the one with the highest predictive accuracy, as estimated by 5-fold cross-validated area under the receiver operating characteristic curve (AUROC) while containing a substantial number of dichotomous variables.
The second approach was conducted manually and aimed to construct for each IMID (RA, PsA and AS) a simplified 4-variable adherence prediction model with good predictive power. In this less complex approach, the choice of four variables balanced practical clinical utility against predictive power; furthermore, four variables can be conveniently presented in a risk prediction matrix. The final simplified model for each rheumatic disease was the one with the highest cross-validated AUROC while containing a substantial number of dichotomous variables. A visual representation of a typical patient medication adherence probability profile for each of the three final models (RA, PsA, and AS) from the second, simplified approach was generated as a tabular matrix. For both the 10-variable and 4-variable models, dichotomous variables were obtained from AUROC analysis. Analyses were conducted with SAS V.9.2 and V.9.4.
Results
Patients
Demographic and disease characteristics
A total of 3390 patients from ALIGN with rheumatic IMIDs were analysed (RA, n=1943; PsA, n=635; AS, n=812). As expected, the percentages of female (highest in RA; lowest in AS) and white (highest in PsA) patients varied significantly across the three rheumatic conditions, as did patient age (lowest in AS). Race was highly dependent on geographic region. The duration of symptoms before diagnosis was shortest in RA and longest in AS, but mean disease duration was 9–10 years for all three evaluated diseases (table 1). Current but not prior disease activity, both of which were defined by the investigators, differed significantly among the three rheumatic indications; moderate, moderate to severe or severe current disease activity was reported in 29.3%, 24.4% and 25.5% of patients with RA, PsA and AS, respectively. The proportion of patients with >3 prior treatments varied significantly, with the highest percentage in patients with RA. Response to current treatments also differed significantly among the three rheumatic IMIDs. A complete response (defined by investigators) was reported in 47.5%, 52.8% and 57.4% of patients with RA, PsA and AS, respectively; a ‘partial’ response was reported in 48.5%, 42.6% and 38.2% of patients with RA, PsA and AS; and a ‘no’ response was reported in 2.9%, 2.1% and 3.1% of patients with RA, PsA and AS.
Patient demographic and disease characteristics, treatments and beliefs about medications
Treatment characteristics
Patients with RA had a significantly longer mean duration of current treatment (5.3 years) compared with patients with PsA and AS (4.1 and 3.8 years, respectively). Among patients with RA, the largest proportion (58.1%) received csDMARD therapy (±GC), whereas in patients with AS, the largest proportion were receiving TNFi monotherapy (46.1%). In patients with PsA, approximately one-third were receiving csDMARD therapy, one-third TNFi monotherapy and one-third csDMARD-TNFi combination therapy (table 1). The most frequently used current systemic compounds were methotrexate (±other therapies) in patients with RA (72.0%) and TNFis (±other therapies) in patients with PsA (65.5%) and AS (79.8%).
BIPQ and BMQ-specific findings
Of BIPQ items used in subsequent analyses, only Timeline (ie, perception of continuing length of illness) differed significantly (highest in PsA, lowest in AS) among the three rheumatic disease groups. Patients with AS had a significantly lower BMQ-Specific Necessity score compared with patients with RA and PsA; patients with RA had a significantly higher mean BMQ-Specific Concerns score compared with patients with PsA and AS.
Medication adherence and attitudes
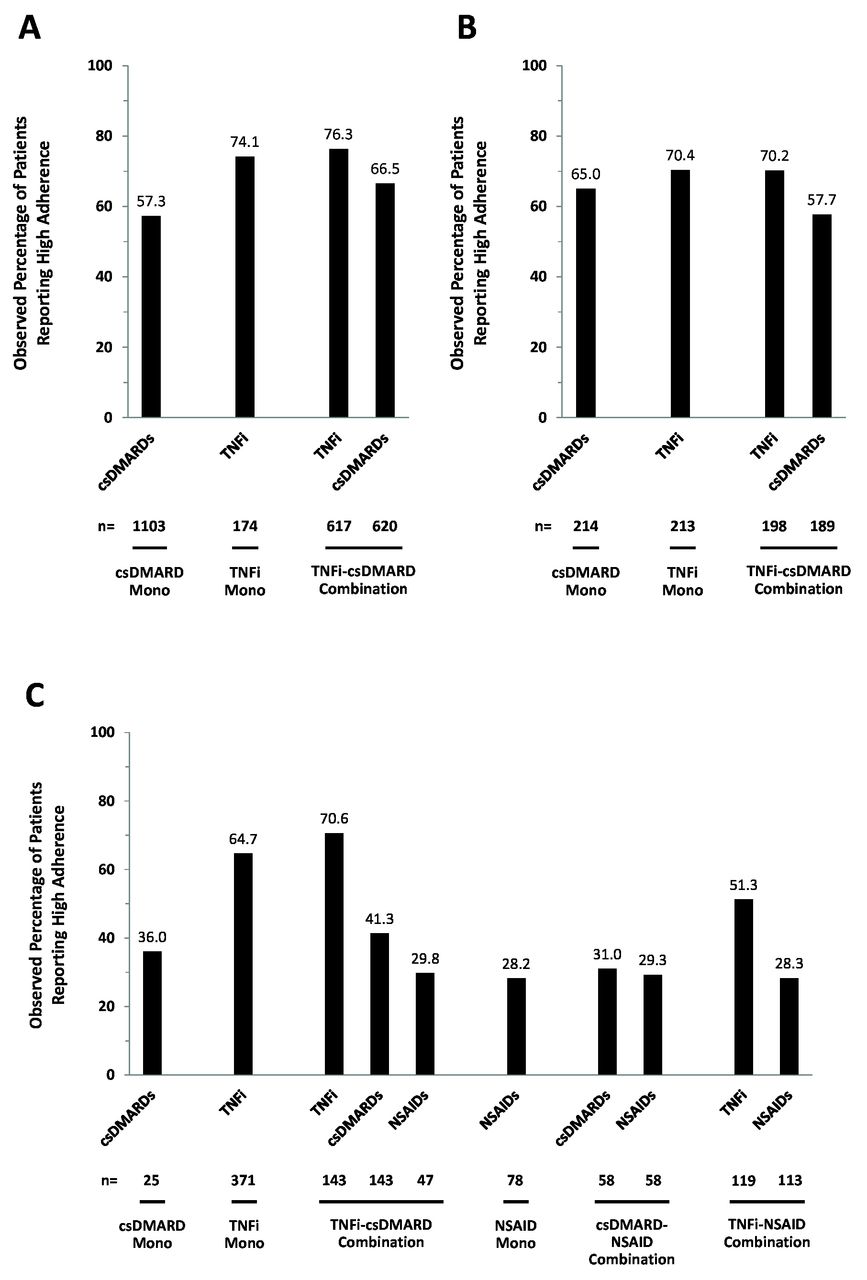
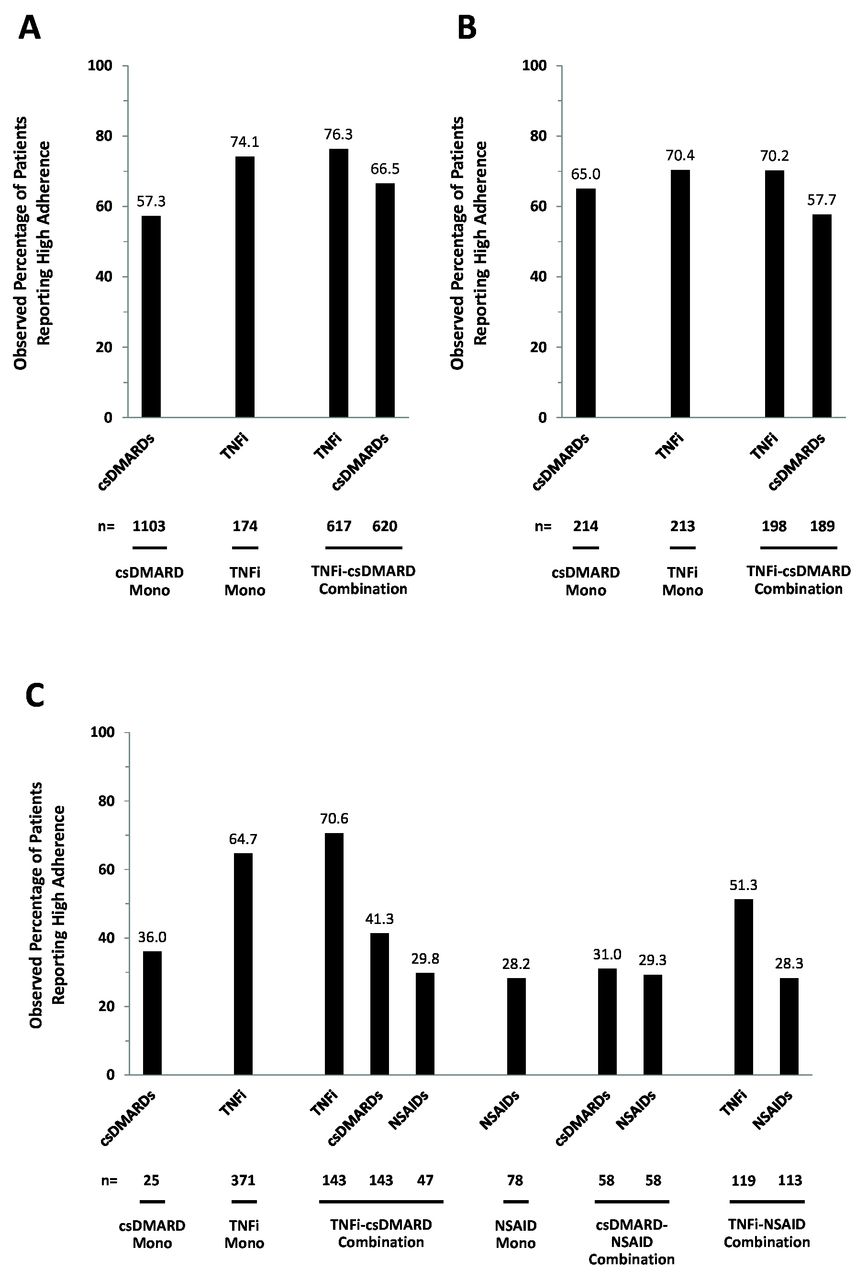
High adherence (MMAS-4© score=4) to a given treatment was similar among patients with RA (OR, 1.106; 95% CI 0.763 to 1.605 and PsA (reference group; OR=1) but significantly lower in patients with AS (OR, 0.424; 95% CI 0.263 to 0.685). The percentage of patients with high adherence also appeared to differ between treatment regimens (figure 1), although no statistical testing was performed because the multivariate regression analyses allowed adjustment for confounding factors. Depending on the treatment, the percentage of patients with high adherence was 57.3%–76.3%, 57.7%–70.4% and 28.2%–70.6% in patients with RA, PsA and AS, respectively. Generally, a larger proportion of patients reported high adherence to TNFis with or without concomitant csDMARDs compared with csDMARDs and NSAIDs (AS). BMQ attitudinal segmentation revealed that large proportions of patients in every rheumatic IMID group were accepting (high treatment necessity beliefs/low concerns; 44.3%–49.4% of patients) towards their medications (online supplementary figure 1). However, 41.9%–47.3% of patients were ambivalent (high treatment necessity beliefs/high concerns) towards their medications. Few patients were indifferent (low necessity beliefs/low concerns) or sceptical (low necessity beliefs/high concerns).
Supplemental material
{kind=link}
Patient-reported adherence towards different IMID treatments in RA (A), PsA (B) or AS (C). Adherence was defined as a binary variable with levels ‘highly adherent’ (MMAS-4©=4) and ‘not highly adherent’ (MMAS-4©<4). Treatments: csDMARD mono=csDMARDs±GCs; csDMARD-NSAID combination=csDMARDs+NSAIDs±GCs; NSAID mono=NSAIDs±GCs; TNFi mono=TNFi±GCs; TNFi-csDMARD combination=TNFi+csDMARDs±NSAIDs±GCs; TNFi-NSAID combination=TNFi+NSAIDs±GCs. AS, ankylosing spondylitis; csDMARD, conventional synthetic disease-modifying antirheumatic drug; GC, glucocorticoid; IMID, immune-mediated inflammatory disease; MMAS-4©, 4-item Morisky Medication Adherence Scale; mono, monotherapy; NSAID, non-steroidal anti-inflammatory drug; PsA, psoriatic arthritis; RA, rheumatoid arthritis; TNFi, tumour necrosis factor inhibitor.
Factors affecting medication adherence
Current treatment type
The full starting models for multivariable regression analyses of treatment adherence, before backwards elimination of factors, are shown in online supplementary figure 2. In multivariable regression analysis, several types of treatment had a positive association with treatment adherence in RA and AS, although not in PsA (table 2). TNFis with or without csDMARDs had the most significantly greater ORs for adherence compared with csDMARD monotherapy in patients with RA (range, 3.63–5.45) and compared with NSAID monotherapy in patients with AS (range, 6.33–22.69). csDMARDs within csDMARD-TNFi combination therapy were significantly associated with greater adherence compared with csDMARD monotherapy in patients with RA (OR, 2.09). NSAIDs as part of any combination therapy in patients with AS were not associated with significantly greater adherence compared with NSAID monotherapy.
Multivariable logistic regression analysis of treatments and other factors associated with medication adherence*
Other factors
In multivariable regression analysis, older age (all three IMIDs) and white race (RA and AS) were significantly associated with better treatment adherence, but sex was not significantly associated with adherence in any of the three rheumatic IMIDs (table 2). Illness perception (higher BIPQ Emotional Representation scores, indicating greater emotional impact) was significantly associated with worse treatment adherence in patients with AS only. None of the disease-related and medication-related factors, such as disease activity or disease duration, were consistently associated with medication adherence across the three rheumatic diseases. Having >3 pretreatments was significantly associated with worse medication adherence only in patients with AS. In patients with PsA, longer duration of current treatment was significantly associated with worse medication adherence, whereas complete treatment response was significantly associated with better adherence. Across all three indications, higher BMQ-Specific Necessity beliefs were associated with higher treatment adherence, whereas higher BMQ-Specific Concerns in patients with RA and higher BMQ-General Harm beliefs in patients with RA and PsA were significantly associated with poorer adherence.
Because race was highly dependent on geographic region, further analyses explored adherence models in which both race and geographic region were included as factors. In these models, geographic region was treated as a fixed variable because geographic categorisation was part of the study design. The full starting models for multivariable regression analyses of treatment adherence, before backwards elimination of factors, are shown in online supplementary figure 3. In multivariable regression analysis (online supplementary table 1), the pattern and magnitude of factors in relation to adherence were mostly similar to the findings from the models without geographic region (table 2). However, in the multivariable model with geographic factors, race was no longer significant and was automatically removed from the model (online supplementary table 1).
Predictive adherence models
Full models (up to 10 variables)
Three variables were shared across the full adherence prediction models for RA, PsA and AS: type of treatment, age and medication beliefs (BMQ-Specific Necessity score). In patients with RA, the best full adherence prediction model (AUROC, 0.68) included five variables besides the common ones: race, medication beliefs (BMQ-Specific Concerns and BMQ-General Harm scores), illness perception (score for BIPQ item 2 (Timeline) with regard to continuing length of illness) and disease duration (online supplementary table 2). In patients with PsA, the best full model (AUROC, 0.68) included three variables besides the common ones: medication beliefs (BMQ-General Harm score), duration of current treatment and complete treatment response. In patients with AS, the best full model (AUROC, 0.74) included three variables besides the common ones: race, illness perception (score for BIPQ item 7 (Coherence) regarding understanding of the disease), and number of prior treatments.
Simplified models (four variables)
Two variables were included in each simplified adherence prediction model for RA, PsA and AS: type of treatment and age. In patients with RA, the best simplified adherence prediction model (AUROC, 0.64) included two variables besides the common ones: race and medication beliefs (BMQ-General Harm score (online supplementary table 2). In patients with PsA, the best simplified model (AUROC, 0.64) included two variables besides the common ones: medication beliefs (BMQ-General Harm score) and duration of disease. In patients with AS, the best simplified model (AUROC, 0.72) included two variables besides the common ones: race and medication beliefs (BMQ-Specific Concerns score).
Predicted probabilities of high adherence in the simplified models ranged widely (RA, 28.6%–96.2% (table 3); PsA, 21.7%–95.5% (table 4); AS, 5.0%–94.1% (table 5)). According to the simplified models, the highest predicted probability of high adherence was to TNFi treatment (especially in combination with csDMARDs; tables 3–5). In patients with RA and PsA, higher adherence was seen in older patients with low treatment harm beliefs; in patients with AS, higher adherence was seen in older patients with low treatment concerns. In patients with RA and AS, the predicted probability of high adherence was greater in white patients compared with non-white patients who otherwise had the same characteristics; in patients with PsA, the predicted probability of high adherence was greater with duration of disease <9 years compared with ≥9 years in patients who otherwise had the same characteristics. Thus, for all three IMIDs, clinicians may wish to promote adherence in younger patients and among those who either had concerns about their specific medications or who believed that medications in general cause harm, as a higher risk of low adherence was found to be related to these factors. Similarly, it also may be advisable to emphasise the importance of adherence to patients with RA or AS who are not white and patients with PsA of long duration.
Predicted probability of high adherence to maintenance treatments per posthoc simplified rheumatoid arthritis model
Predicted probability of high adherence to maintenance treatments per posthoc simplified psoriatic arthritis model
Predicted probability of high adherence to maintenance treatments per posthoc simplified ankylosing spondylitis model
Discussion
ALIGN was the first large cross-sectional study to explore patients’ beliefs and treatment adherence to systemic medication across six IMIDs, including three rheumatological diseases. In all three evaluated rheumatic diseases (RA, PsA and AS), higher treatment necessity beliefs were more consistently associated with medication adherence than disease-related or medication-related factors. The direct positive relationship of TNFi treatment with necessity beliefs in ALIGN16 appeared to be associated with higher medication adherence in patients with RA and AS, although not in patients with PsA. Models that used subsets of the key factors had moderate ability to predict medication adherence in patients with RA, PsA and AS. The adherence prediction models were developed via two distinct approaches. The first approach used automated selection of variables to determine which of a large number of potential factors produced models with a higher predictive performance. The second approach used a prognostic model with only one categorical predictor (treatment type) and three other dichotomized predictors; although the simpler models had slightly less predictive power than the models from the first approach, they would be easier to integrate into clinical practice. In applied psychology and prediction of future behaviour, AUROC values approximately >0.70 are considered strong effects.26 The predictive accuracy of our AS adherence prediction model exceeded an AUROC of 0.70 and appeared to be of higher accuracy compared with those of the RA and PsA models.
To our knowledge, our models are the first that have been developed to estimate the probability of high adherence to systemic therapies in patients with RA, PsA and AS. Thus, no other adherence models are available for comparison to determine the value of our models. Adherence prediction models in other diseases showed higher predictive accuracy.27–32 However, our adherence prediction models cannot be compared with those models because of differences in the aims of the previously published models, their analysed patient populations and diseases, the definitions and measurement of adherence and compliance and study design (eg, longitudinal vs cross-sectional design; single-variable model vs multivariable model). The moderate predictive accuracy of our models may be the result of unidentified factors that could affect adherence on an individual level but which are not identifiable in a large patient population. The degree of self-reported high medication adherence varied widely among patients with RA, PsA and AS in ALIGN, consistent with a systematic review of findings from other studies.6 The reason for a higher observed adherence to TNFi’s compared with other treatments in ALIGN cannot be explained by the results of this study but could stem from a favourable balance between perceptions of treatment necessity versus concerns about adverse effects, which would be in line with multiple reports that found a role for such beliefs in affecting adherence.8 33–37 Because many, and in some countries all, patients receiving TNFi’s or other biological or targeted synthetic DMARDs are enrolled in a registry (particularly in Europe), their physicians or other healthcare providers will regularly monitor their disease in a structured manner; this could also have a positive effect on adherence. In addition to beliefs about treatments, factors that were significantly associated with high medication adherence in ALIGN notably included greater age and white race (the latter interrelated with geographic region). Interestingly, disease-related factors were infrequently associated with high adherence when the variables were considered across the three different IMID groups. The limited number of significant strong predictors did, however, facilitate development of adherence prediction models with manageable numbers of components. Each of the three final models shared type of treatment and age as factors; however, not all treatments were comparable among IMIDs, because NSAIDs (which are considered disease modifying and cornerstone first-line treatment in AS but not RA or PsA) were modelled only for the AS population. Heterogeneity in the structures of the three final models, perhaps deriving ultimately from the dissimilar experiences of patients with RA, PsA and AS, underscores the need for separate analysis in each IMID to enable accurate prediction of medication adherence. Although in the present study separate analyses were needed for the three conditions investigated because of different profiles, it would be desirable to have a single adherence prediction model for all three diseases; based on the present study, it may be possible to develop such a tool in the future.
Several limitations of ALIGN and the current analyses should be noted. First, and perhaps most important, the number of patients with RA was greater than the numbers of patients with PsA and AS; consequently, statistical power was dissimilar in the three groups. This could have impaired detection of significant effects in some analysis groups. Second, as expected from the epidemiology of each condition, patients in the three different rheumatic IMID populations differed in their sociodemographic, disease and treatment characteristics. For example, a higher percentage of patients with AS received TNFi compared with patients with RA and PsA; this presumably was due to the general inefficacy of csDMARDs and other biologics for treating AS.24 Therefore, it was impossible to pool data across rheumatic diseases or to produce an adherence prediction model that would be applicable to all three conditions. Third, the proportion of white patients within each IMID group depended strongly on the geographic region, and adherence as well as treatment patterns may have been linked to country-specific factors, such as restricted access to certain medications, and cultural beliefs. The interdependence of race and geographic region was confirmed by using models in which geographic region was a fixed factor, resulting in the automatic elimination of race as an independent predictive factor. Fourth, disease activity was judged subjectively by the investigators, rather than assessed by some objective measure. Fifth, treatment adherence was based on patient self-reporting and was not confirmed by objective measures. However, patients completed and turned in the questionnaires in private and anonymously so that they could answer honestly without worries about censure. Nevertheless, some other means to measure medication acquisition may be helpful and, indeed, consistent with the results of the present study. A recent study assessed adherence to medications in patients with RA (n=178) using an objective measure of adherence (medication possession ratio) and found that 89% of patients showed good adherence to biological DMARDs.38 Sixth, by design, the survey captured data from only a single point in time; however, information was also collected on the patients’ disease history. Finally, development of the final adherence prediction models via AUROC analysis was a posthoc effort, although the identification of individual predictive factors by multivariable regression analysis was prospectively planned.
In conclusion, patients with rheumatic IMIDs who participated in a large, multicountry patient survey study exhibited treatment beliefs that were strongly associated with adherence to systemic medications. Among the treatment regimens that were examined, adherence was highest for TNFis, whether as monotherapy or in combination with other agents. Simplified models that combined treatment beliefs with other key significant predictive factors, such as age, race and treatment duration, provided moderate power in estimating adherence to different systemic medications. These models may be useful in tailoring interventions to increase adherence in individual patients, as the demographic predictors can indicate whom to target, whereas the medication belief predictors indicate what to target in an adherence support intervention. Tools to facilitate use of these models in community rheumatology practice would allow application and further validation in real-world populations. Because ALIGN was the first large, cross-sectional study of its kind, confirmatory research using more objective criteria is needed.
Acknowledgments
Julia Sommer, PhD, of GKM Gesellschaft für Therapieforschung mbH, Munich, Germany, provided statistical support and input on the manuscript. Medical writing support was provided by Michael J. Theisen, PhD, and Peter A. Rittenhouse, PhD, of Complete Publication Solutions, LLC, North Wales, PA, USA. Use of the ©MMAS is protected by US copyright laws. Permission for use is required. A license agreement is available from: Donald E. Morisky, Professor, Department of Community Health Sciences, UCLA Fielding School of Public Health, 650 Charles E. Young Drive South, Los Angeles, CA 90095-1772, dmorisky@ucla.edu.
References
Footnotes
Permission Use of the ©MMAS is protected by US copyright laws. Permission for use is required. A license agreement is available from: Donald E. Morisky, Professor, Department of Community Health Sciences, UCLA Fielding School of Public Health, 650 Charles E. Young Drive South, Los Angeles, CA 90095-1772, dmorisky@ucla.edu.
Contributors All authors contributed equally to the preparation of the manuscript.
Funding This work was supported by AbbVie.
Competing interests JSS has received grants and personal fees from AbbVie, Lilly, MSD, Pfizer and Roche and personal fees from Amgen, AstraZeneca, Astro, Celgene, GlaxoSmithKline, Janssen, MedImmune, Novartis, Samsung and UCB. DG has received grant/research support from AbbVie, Amgen, Bristol-Myers Squibb, Celgene Corporation, Janssen, Pfizer Inc, Novartis and UCB. HPM has received research grants and consulting fees from AbbVie. PJM has received research grants, consulting fees and/or speaker fees from AbbVie, Amgen, Bristol-Myers Squibb, Celgene, Genentech, Janssen, Lilly, Merck, Novartis, Pfizer, SUN and UCB. JS has received research funds, consulting fees and/or speaker fees from AbbVie, Janssen, Lilly, Novartis, Merck, Pfizer, Roche, Sun Pharma and UCB. MH is an employee of AbbVie and may own AbbVie stock/stock options. PN is a former employee of AbbVie and may own AbbVie stock/stock options. JW has performed work that was paid for by AbbVie and Atlantis Healthcare, either directly or indirectly through an intermediary.
Patient consent Not required.
Ethics approval The study was approved by local ethics committees in each country.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement No additional data are available.