Article Text

Abstract
Background/purpose Cardiovascular (CV) risk, cancer, infections and osteoporosis should be screened for in rheumatoid arthritis (RA). The objective was to assess 3-year effects of a nurse visit for comorbidity counselling.
Methods This was an open long-term (3 years) extension of the Comorbidities and Education in Rheumatoid Arthritis 6-month randomised controlled trial in which patients with definite, stable RA were visiting a nurse for comorbidity counselling. Comorbidity status was assessed and nurses provided advice on screening and management, at baseline and 3 years later. A score was developed to quantify comorbidity screening and management: 0–100, where lower scores indicate better screening and management. The score was compared between baseline and 3-year assessment using a Wilcoxon test for paired data.
Results Of the 970 recruited patients, 776 (80%) were followed-up at 2–4 years and 769 (79%) had available data for comorbidities at both time points: mean (±SD) age 58 (±11) years and mean disease duration 14 (±10) years; 614 (80%) were women, the mean Disease Activity Score 28 was 3.0±1.3, and 538 (70%) were receiving a biologic. At baseline, the mean comorbidity screening score was 36.6 (±19.9) and it improved at 3 years to 24.3 (±17.8) (p<0.0001), thus with a relative improvement of 33% (improvement of 12 points). CV risk screening, vaccination status and bone densitometry performance improved the most.
Conclusions Comorbidity screening was suboptimal but improved notably over 3 years, after a nurse-led programme aiming at checking systematically for comorbidity screening and giving patient advice. This long-term efficacy pleads in favour of nurse-led interventions to better address comorbidities in RA.
Trial registration number NCT01315652
- rheumatoid arthritis
- cardiovascular disease
- nursing
- vaccination
- multidisciplinary team care
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Key messages
What is already known about this subject?
Comorbidites are frequentin rheumatoid arthritis (RA). Screening for these comorbidities is important.
What does this study add?
At baseline, the most frequent comorbidities in this RA population aged around 60 years, were history of fracture (31.9%) and high blood pressure (30.9%); and at 3 years, these were also the comorbidities had the most increased incidence for 100 patient-years, 3.1 and 2.1, respectively.
An innovative comorbidity prevention and screening score (range 0–100) was developed, where lower scores indicate better screening and management.
Three years after a nurse intervention, the comorbidity prevention and the screening score improved by 33% compared with the baseline score. This confirms the role of nurses in comorbidity screening and prevention in RA patients.
How might this impact on clinical practice?
The role of the nursing team in screening for comorbidites should be emphasized. The screening score developed here can be useful to assess such interventions.
Introduction
Rheumatoid arthritis (RA) is a chronic inflammatory rheumatic disease which, on top of the burden associated with the disease itself, is often associated with comorbidities.1–4 Indeed, in RA patients, some comorbidities are more common than in the general population (in particular, cardiovascular (CV), osteoporosis, infections or lymphoma), whereas some are not more frequent but appear to be less well-managed than in the general population (eg, breast cancer).3 5–10
Some comorbidities of particular interest in RA are CV risk factors and disease, cancer, infections and osteoporosis. Numerous studies have shown that excess mortality in RA patients is due to increased CV disease, and that both the inflammation and traditional CV risk factors, such as hyperlipidaemia or high blood pressure, are involved.5 11–13 Cancers are overall not more frequent in RA patients though an increase is noted for lung–chest cancers and lymphomas. Furthermore, it appears RA patients are less well screened for cancer than subjects without RA; this is the case for mammography in women.10,14 15 Infections are frequent in RA due to iatrogenic immunodepresssion.3 Finally, osteoporosis is a frequent comorbidity, and RA is considered a risk factor for osteoporosis in the FRAX risk tool endorsed by the WHO.16–18
Some of these comorbidities can be screened for or prevented. CV risk factors can be managed; cancers can be screened for; infections can in part be prevented by adequate vaccination (ie, influenza and pneumococcus) and osteoporosis can be screened for and treated.19–21 The European League Against Rheumatism (EULAR) has issued recommendations for CV risk assessment and vaccination in RA, and international recommendations for cancer and osteoporosis screening also exist.19 22–24 In France, national recommendations have recently been developed as well.14 However, to date, the screening and prevention of comorbidities is far from optimal in both the primary and secondary prevention.5 20 21 25–28
In 2012, we ran the COMEDRA (Comorbidities and Education in Rheumatoid Arthritis) trial.4 In this randomised controlled trial, RA patients with stable disease were randomised to an early or delayed intervention comprising a nurse-led visit to assess comorbidities and inform patients and physicians of need for intervention. The nurse did not prescribe any intervention but intervened for patient education and systematic screening. The COMEDRA trial yielded positive results, with better comorbidity screening and management in the early intervention group, at the 6 months time point.4
We were interested to explore the long-term effects of a nurse intervention (as performed in COMEDRA) on the screening and prevention of comorbidities.4 For this reason, the patients in the COMEDRA trial were followed-up in an open-label extension study of 36 months to reassess the comorbidities and the long-term utility of the initial standardised follow-up.
The objectives of this follow-up study were to (i) assess comorbidity incidence and prevalence in the COMEDRA trial, at baseline and 3 years after the trial ended and (ii) assess screening and management of selected comorbidities in this population.
Patients and methods
Study design
The COMEDRA initial trial was a prospective, randomised, 6-month, parallel-group, open-label trial.4 COMEDRA was a multicentre French study in 5 centres around Paris and 13 centres over the whole country; centres were tertiary care centres with a focus on RA. The trial comprised two arms (ie, comorbidity assessment and a control group, where patients were taught disease activity self-assessment) and lasted 6 months (see figure 1).
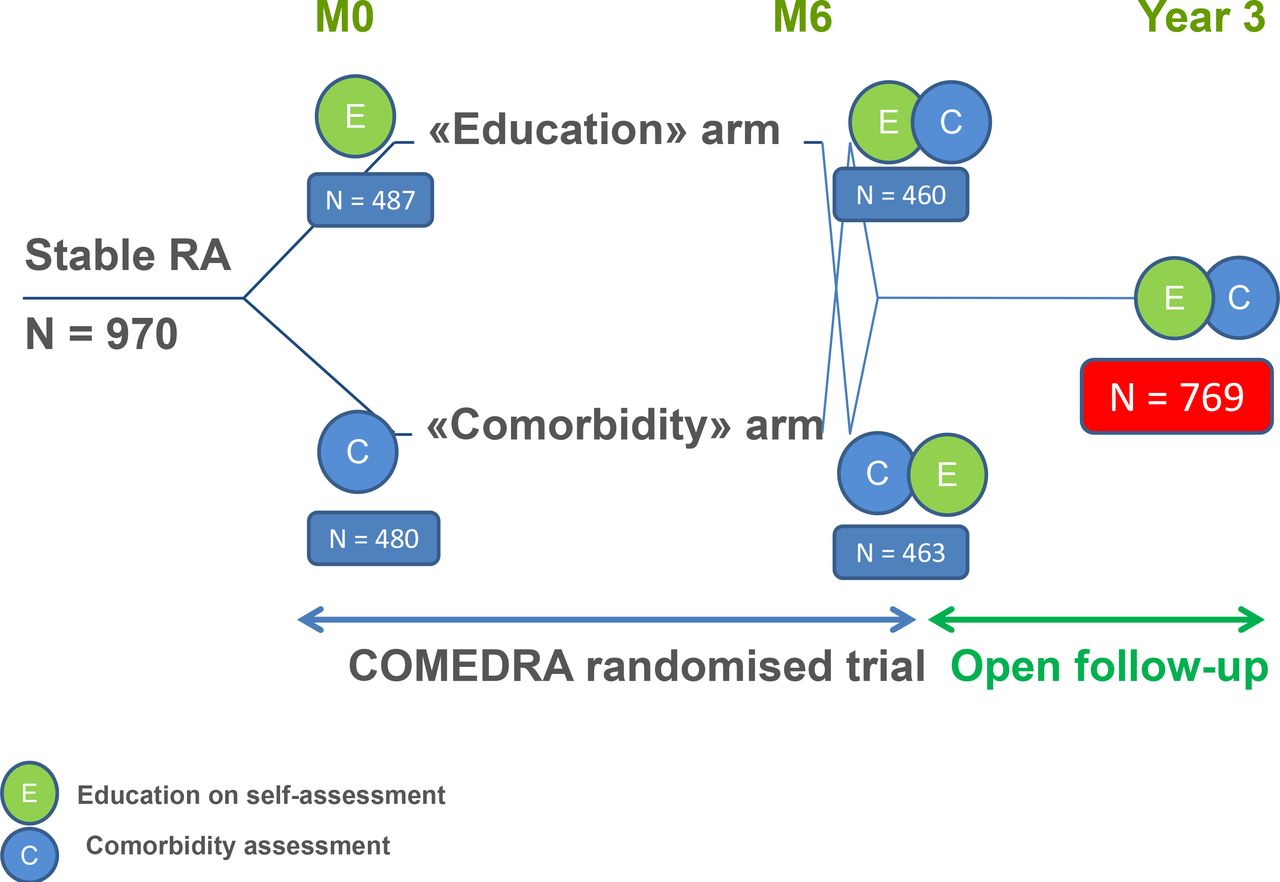
Flowchart of patient disposition in the COMEDRA trial and for the 3-year follow-up. COMEDRA, Comorbidities and Education in Rheumatoid Arthritis; M0, month 0; M6, month 6; RA, rheumatoid arthritis.
The present results are issued from an open-label long-term (3 years) extension of the COMEDRA trial.
Patients
Patients in COMEDRA had definite, stable RA, as explained elsewhere.4 Briefly, consecutive patients fulfilling the 1987 American College of Rheumatology criteria for the diagnosis of RA, aged between 18 and 80 years, with a disease considered by the treating rheumatologist to have been stable for at least 3 months, were included.4 29
Intervention
Comorbidity status was assessed, and nurses provided advice on screening and management, during the trial and 3 years later. A screening prescription, including blood cell count, erythrocyte sedimentation rate, C reactive protein, creatinine and vitamin D levels, lipid profile and dipstick urine protein test, was sent to each patient. The nurses were asked to (i) report the presence of comorbidities (eg, stroke); (ii) screen for risk factors (eg, hypertension for CV disease) and (iii) give patients advice on targets for screening and management (eg, need for vaccination) without prescribing the interventions. The nurse advised the patient to visit her/his general practitioner and/or rheumatologist if risk factors were detected. In parallel, a report of the screening findings was sent to the general practitioner and the rheumatologist of each patient.
Data collection
General and patient-reported data
Patient demographics and disease characteristics were collected at baseline, including previous/current RA treatments (glucocorticoids and disease-modifying drugs, synthetic and biological). The presence of rheumatoid factor and/or anticyclic citrullinated peptide, the presence of radiographic erosions and the Disease Activity Score 28 (DAS28) at inclusion were recorded.30 Pain and patient global assessment single questions were assessed. Function was collected using the modified Health Assessment Questionnaire.
Comorbidities
For this follow-up study, the baseline comorbidity data were issued from either the first visit (for patients randomised to the comorbidity arm) or the 6-month (second) visit (for patients randomised to the control arm) (figure 1). The follow-up comorbidity data were collected at the 3-year visit. The prevalence of comorbidities was assessed at baseline (as defined above) and incidence was assessed at the 3-year visit. This incidence corresponds to new cases over the follow-up (thus prospective incidence); it is reported for informative purposes, and should not be considered in parallel with the screening procedures. The comorbidities of interest collected here were CV risk factors (diabetes, high blood pressure, hyperlipidaemia, obesity: body mass index≥30 kg/m2, and current smoking) and major CV events (defined as myocardial infarct angina, stroke and obliterating arteriopathy), cancers (including colon cancer, breast cancer, lung cancer, prostate cancer, uterus cancer, skin cancer (all types) and lymphoma) and history of fracture.
Comorbidity screening and prevention score
The following screening and prevention measures against comorbidities were considered (table 1): (i) for CV disease: blood pressure measurement, and blood tests for fasting blood glucose, lipids and serum creatinine to be performed at least once a year as per EULAR guidelines at the time of the study24 31 32; (ii) for cancers: screening of colon/rectum cancer, skin cancer, and prostate (for men) or breast and cervix cancer (for women), screening to be performed at frequencies in accordance with international guidelines14; (iii) for infectious disease prevention: agreement with the vaccination recommendations was defined as influenza vaccination performed within the last 12 months and pneumococcal vaccination performed within the last 5 years23 and (iv) for osteoporosis screening: bone mineral density once in lifetime.
Comorbidity screening/prevention score
To assess these screening and prevention measures, a comorbidity screening and prevention score was developed by the steering committee (table 1). This score quantifies comorbidity screening and management as a continuous score (range 0–100), where lower scores indicate better screening and management (ie, optimal screening and detection=0 points). The points were attributed to the four main comorbidity screening measures as explained above, taking into account the prevalence and severity of these comorbidities with the most points being given to CV disease. Given gender differences in prevalences of cancer, points for cancer detection differed between women and men (table 1). Patients not at risk (eg, demographically not at risk, such as women for prostate cancer) or people presenting already with the comorbidity (ie, considered not in need of screening/detection) were scored as 0=optimal screening.
Illustration of the score
For illustration purposes, some examples are: A score of 20–25 points could correspond to (no lipid screening and no pneumococcus vaccination), or (neither breast nor cervix cancer screening and no osteoporosis screening), with other measures properly taken. A score of 35–40 points could correspond to (no lipid screening, no pneumococcus vaccination and no diabetes screening), or (neither breast nor cervix cancer screening, no osteoporosis screening, no colon screening and no influenza vaccination).
Statistical analysis
We analysed all patients who took part in the study visit at month 36. Continuous variables are presented as means and SD and categorical variables as counts (percentage). The comorbidity screening and prevention score were compared between baseline (either study entry or month 6 visit) and 3-year assessment using a Wilcoxon-Mann-Whitney test for paired data. The prevalence of comorbidities was assessed as overall percentage of patients at baseline. The relative increase in the given comorbidity during the follow-up was also evaluated as percentage increase and as incidence per 100 patient-years. Then for each comorbidity, the proportion of patients in conformity for screening/prevention was compared between baseline and 3-year assessment using a McNemar test for paired data. Statistical analyses were performed by using ad hoc routines implemented in R V.3.3.1 software.
Results
Patient disposition
Of the 970 recruited patients, 776 (80%) were followed-up at 2–4 years, between May 2014 and October 2015 (15, 1.5%, had died) and 769 (79%) had available data for comorbidities and screening at both time points. There were no notable differences between those followed-up or not (data not shown).
Patient characteristics
Patients were typical of an RA tertiary care population (table 2): mean (±SD) age 58 (±11) years and mean disease duration 14 (±10) years; 614 (80%) were women and 538 (70%) were receiving a biologic. The mean baseline and 3-year DAS28 scores were, respectively, 2.99±1.30 and 2.83±1.34.
Characteristics of 769 patients with RA
Incidence and prevalence of comorbidities
At baseline, the most frequent comorbidities (table 3) were a history of fracture (31.9%) and high blood pressure (30.9%).
Prevalence of selected risk factors and comorbidities at baseline and 3 years
At 3 years, most of the comorbidities had increased (table 3). The comorbidities those had the most increased in this population aged around 60 years were fractures (incidence 3.1 per 100 patient-years) and high blood pressure (2.1 per 100 patients-years). Among CV risk factors, hyperlipidaemia had increased the most (incidence, 1.1 per 100 patient-years), whereas smoking had decreased (2% of the population stopped smoking).
Comorbidity screening and prevention
At baseline, the mean comorbidity screening score was 36.6 (±19.9) and it has improved at 3 years to 24.3 (±17.8) (p<0.0001), thus with an absolute mean improvement of around 12 points, and a relative improvement of 33% (figure 2). The improvement for each element of the score is presented in table 4. CV risk screening, vaccination status and bone densitometry performance improved the most.

{kind=link}
{kind=link}
Comorbidity screening and prevention score. (A) Baseline score. (B) Three years follow-up score.
Percentage of patients in conformity with screening and management recommendations, for each comorbidity
Discussion
The present study brings important information on comorbidities in RA, and importantly, addresses the long-term effects of a nurse intervention to enhance screening and prevention of comorbidities. We found the most frequent comorbidities/risk factors and with the highest incidence in this population of patients with moderate-to-low disease activity and frequent intake of biologics were a history of fracture (prevalence 31.9%) and high blood pressure (prevalence 30.9%). We also developed a screening and prevention score, and found that screening and prevention was suboptimal in this population but improved after the nurse-led intervention.
This study has strengths and weaknesses. It is a large-scale study with granular information on comorbidities and screening procedures. However, some comorbidities, such as depression, were not assessed. Furthermore, we assessed in detail screening procedures, but not interventions performed on patients after these screening procedures.4 However, screening is a necessary step before interventions can be performed. The patients analysed here were often receiving biologic therapies. This can be explained by the tertiary centre recruitment. It may, however, lead to higher comorbidity rates and to better screening, as these patients are often followed-up in a more rigorous way than other patients. The loss to follow-up rate was of 20% at 3 years, which indicates the difficulties of long-term follow-up studies in observational settings; however, patients lost to follow-up had similar characteristics as the other patients. Preventative measures, such as the ones taken in the present study, are costly; it would be interesting to perform cost–benefit analyses. Perhaps this may be performed in future studies of comorbidity screening.32 Finally, we report herein as the main criterion, screening measures; we also report incidence of comorbidities but it is important to keep in mind the lack of causality between the screening and the prevalence of comorbidities, both are presented in parallel but are not linked.
Comorbidities are frequent in RA and in the present study, the most frequent comorbidities were CV risk-related and fractures. CV risk is now well-recognised in RA.3 12 13 Osteoporosis was frequently noted in this population; of note, the nurses who collected information relating to fractures noted all fractures, whatever the cause, which may have overestimated events. However, fractures are frequent in RA and furthermore, this can be explained in part by glucocorticoid intake in RA patients.16 17
In this study, the steering committee developed an innovative comorbidity prevention and screening score. This score does not assess the frequency of comorbidities, but rather focuses on the frequency of optimal screening/prevention. We believe that such a score will be useful to assess the quality of care in terms of comorbidity screening and prevention. Of note, however, not all screening or prevention actions are assessed in this score. For example, interventions to help with smoking cessation or weight loss are not assessed, since we found that such interventions are (i) difficult to quantify reliably and (ii) not often efficacious.31 Another issue with this score is that the definition of ‘optimal screening’ is subject to both the national guidelines (which may vary, eg, for cancer detection) and the changing recommendations (eg, for prostate cancer detection).33 In fact, in our score, we applied the EULAR CV screening recommendations of the time the study was designed,22 which referred to as yearly screening of CV risks, whereas now these recommendations have been revised to 5-yearly screening.24
Comorbidity screening was suboptimal in the present study. The mean score at the end of the study was 24 points on a 0–100 scale, which could correspond to (no lipid screening and no pneumococcus vaccination), or (neither breast nor cervix cancer screening and no osteoporosis screening), with other measures properly taken. Screening does not always address the most frequent or severe comorbidities. Some resistance may be due to (i) poor knowledge of the constantly evolving screening procedures; (ii) painful or costly or otherwise anxiety-creating screening procedures and (iii) lack of clear responsibility for screening (should it be the general practitioner, the rheumatologist and the hospital team?). Empowering patients to be responsible for the comorbidity screening reminders should be explored.
The improvements seen over 3 years in the screening and prevention score after a nurse-led programme aiming at checking systematically for comorbidity screening and giving patients advice plead in favour of nurse-led interventions to better address comorbidities in RA. Of note, these patients were mainly on biologics and the study was performed in tertiary centres; perhaps both the patients and the health professionals were particularly aware of comorbidities.
The improvements were particularly notable for CV screening and vaccinations. Influenza and pneumococcal vaccinations are recommended in all patients with RA. However, it is well known that a gap exists between recommendations and their implementation in real life. As EULAR recommendations for vaccinations are now widely disseminated, it can be hoped that these simple and effective measures will be more widely implemented. However, currently in France and in several other countries, there are important controversies around vaccinations (often relayed through social media with deleterious effects, at least in Western Europe and North America).34 35 Time will tell if this will impact the vaccination rates of our patients.
The single observed improvement for cancer screening was the one related to skin cancer. This probably reflects the current interest in a potential higher risk of skin cancer on tumour necrosis factor inhibitors.36 37
In spite of the improvement of the comorbidity screening and management score, the incidence of comorbidities increased over 3 years in the three domains (CV, cancers and fractures). It has not to be interpreted as the non-usefulness of the screening and detecting risk factors but it reinforces the previous data demonstrating that these four types of comorbidities are at risk in RA patients. Future studies need to evaluate if patients with a decrease of the comorbidity screening and management score will experience a lower increase rate of comorbidities over time.
In summary, this study strongly supports the long-term benefit of a single nurse-led programme for screening and preventing comorbidities. Further studies are required to evaluate different strategies, including the repetition over time of this nurse-led programme, to improve comorbidity screening and prevention in RA patients.
Acknowledgments
The authors thank the URC-CIC Paris Descartes Cochin for implementation, monitoring and data management of the study. We acknowledge prior presentation of this work in conference abstracts as follows: ACR 2016 Congress: Gossec L, Soubrier M, Foissac F, Molto A, Fayet F, Bardin T, etal. Screening for and management of comorbidities after a nurse-led program: results of a 3 year longitudinal study in 776 established RA patients. Arthritis Rheumatol 2016;68 (suppl 10). https://acrabstracts.org/abstract/screening-for-andmanagement-of-comorbidities-after-a-nurse-led-program-results-of-a-3-yearlongitudinal-study-in-776-established-ra-patients/ (accessed 05 April 2019). EULAR 2017 Congress: Gossec L, Soubrier M, Foissac F, Fayet F, Balandraud N, Bardin T, et al. Prevalence and incidence over 3 years of different comorbidities in rheumatoid arthritis (RA): a 3-year longitudinal study in 769 established RA patients. Annals of the Rheumatic Diseases 2017;76 (suppl 2):811.
References
Footnotes
Contributors All the authors except F Foissac, statistician, have provided data for the study; all the authors have participated in the data interpretation and have approved the final version.
Funding The initial COMEDRA trial was supported by the Roche France and a grant from the French National Research Program. This follow-up study was supported by a research grant from the French Ministry of Health (PHRC AOM 12072) and sponsored by the Département de la Recherche Clinique et du Développement del'Assistance Publique—Hôpitaux de Paris.
Competing interests None declared.
Patient consent for publication Not required.
Ethics approval The study was approved by the French institutional review board, file #8-14 (ID RCB 2014-A00102-45).
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement Data may be obtained from a third party and are not publicly available.