Article Text

Abstract
Objectives The aims of this study were to update the evidence on the incidence and prevalence rates of vaccine preventable infections (VPI) in patients with autoimmune inflammatory rheumatic diseases (AIIRD) and compare the data to the general population when available.
Methods A literature search was performed using Medline, Embase and Cochrane library (October 2009 to August 2018). The primary outcome was the incidence or prevalence of VPI in the adult AIIRD population. Meta-analysis was performed when appropriate.
Results Sixty-three publications out of 3876 identified records met the inclusion criteria: influenza (n=4), pneumococcal disease (n=7), hepatitis B (n=10), herpes zoster (HZ) (n=29), human papillomavirus (HPV) infection (n=13). An increased incidence of influenza and pneumococcal disease was reported in patients with AIIRD. HZ infection-pooled incidence rate ratio (IRR) was 2.9 (95% CI 2.4 to 3.3) in patients with AIIRD versus general population. Among AIIRD, inflammatory myositis conferred the highest incidence rate (IR) of HZ (pooled IRR 5.1, 95% CI 4.3 to 5.9), followed by systemic lupus erythematosus (SLE) (pooled IRR 4.0, 95% CI 2.3 to 5.7) and rheumatoid arthritis (pooled IRR 2.3, 95% CI 2.1 to 2.6). HPV infection-pooled prevalence ratio was 1.6, 95% CI 0.7 to 3.4 versus general population, based on studies mainly conducted in the SLE population in Latin America and Asia. Pooled prevalence of hepatitis B surface antigen and hepatitis B core antibody in patients with AIIRD was similar to the general population, 3%, 95% CI 1% to 5% and 15%, 95% CI 7% to 26%, respectively.
Conclusion Current evidence shows an increased risk of VPI in patients with AIIRD, emphasising that prevention of infections is essential in these patients.
- autoimmune diseases
- epidemiology
- infections
- vaccination
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Key messages
What is already known about this subject?
The first EULAR recommendations for vaccination in adult patients with autoimmune inflammatory rheumatic diseases (AIIRD) were published in 2011, based on available literature through September 2009 and expert opinion.
What does this study add?
Since 2009, a significant body of data has been published in the field of epidemiology of vaccine preventable infections (VPI) within AIIRD population, including influenza, pneumococcal disease, herpes zoster, hepatitis B and human papillomavirus infection.
This systematic literature review provides an updated overview on the incidence and prevalence rates of VPI in patients with AIIRD.
Patients with AIIRD are at increased risk of influenza, pneumococcal, herpes zoster and human papillomavirus infections, indicating the importance of their monitoring and use of vaccination to decrease the risk of these infections.
How might this impact on clinical practice?
This systematic literature review informed the task force for the 2019 update of the EULAR recommendations for vaccination in adult patients with AIIRD.
Introduction
In 2011, the first EULAR evidence-based recommendations for vaccination in adult patients with autoimmune inflammatory rheumatic diseases (AIIRDs) were published,1 with the main goal to reduce infection-related morbidity and mortality in the AIIRD population. Despite the well-established fact of a high burden of infections among patients with AIIRD,2 limited evidence was available concerning the real incidence and prevalence of vaccine preventable infections (VPIs) in this population.3 In light of the newly accrued data over the last decade, this paper presents the results of the systematic literature review (SLR) on the incidence and prevalence of VPI in adult patients with AIIRD. Together with the SLR on efficacy, immunogenicity and safety of vaccinations in patients with AIIRD,4 it provided the EULAR task force an evidence-based rationale for the 2019 update on the recommendations for vaccination in this population of patients.
Methods
Literature search
A systematic literature search was conducted via Medline (Ovid), Embase (Embase.com) and Cochrane (Wiley) databases, from 1 October 2009 up to 15 August 2018. Additionally, reference lists of included studies and additional papers considered relevant in the opinion of experts were screened. For all databases, we used free text terms describing our lists of AIIRD and VPI. Additionally, we searched with the corresponding Medical Subject Headings for Medline and Embase subject heading Emtree for Embase. We used a broad filter for locating incidence and prevalence studies, adapted from a previously published systematic review.5 The full search strategy of all databases is documented in online supplementary file 1. We manually searched the references cited by the retrieved articles and reviewed articles for additional references.
Supplemental material
Search strategy
Our research question was formulated according to the PICO format (Population, Interventions, Comparators, Outcomes) (box 1). The population was defined as patients with AIIRD, treated or untreated with immunosuppressive drugs (table 1, supplementary file). Interventions were not applicable to our research question. The comparators were healthy individuals or the general population when the data were available. Outcomes were defined as the incidence or prevalence rates for the following vaccine preventable infectious diseases: influenza, tetanus, diphtheria, pertussis, measles, mumps, rubella, varicella, herpes zoster (HZ), human papillomavirus (HPV) infection, Streptococcus pneumoniae infection, hepatitis A, hepatitis B, Neisseria meningitidis infection, Haemophilus influenzae infection, tick-borne encephalitis, typhoid fever, yellow fever.
Supplemental material
PICO-formulated research question.
What is the incidence or prevalence of vaccine preventable infections (VPI) in adult patients with AIIRD?
Population: Patients with AIIRD treated or untreated with immunosuppressive drugs
Intervention: None
Comparison: Healthy controls or general population
Outcome: Incidence or prevalence of vaccine-preventable infections: influenza, tetanus, diphtheria, pertussis, measles, mumps, rubella, varicella, herpes zoster, human papillomavirus infection, Streptococcus pneumoniae infection, hepatitis A, hepatitis B, Neisse ria meningitides infection, Haemophilus influenza e infection, tick-borne encephalitis, typhoid fever, yellow fever.
AIIRD, autoimmune inflammatory rheumatic disease(s).
Influenza studies characteristics, influenza incidence rates and incidence rate ratios
Inclusion and exclusion criteria
Eligible studies were observational longitudinal studies/cohort studies, including registries and claims database studies, for the IRs and cross-sectional studies for the prevalence rates only, when the data on the disease incidence were unavailable. SLRs of cohort studies and meta-analyses were also included. For hepatitis B, only studies reporting the seroprevalence of hepatitis B surface antigen (HBsAg) and/or hepatitis B core antibody (anti-HBc) were included. Only articles in English on adult patients (≥18 years old) were included. Case-control studies, case reports, intervention studies, vaccination studies, abstracts presented in scientific meetings, in vitro and animal studies were excluded. Papers included in the previous recommendations were also excluded. Studies on patients with non-rheumatic autoimmune diseases, immunodeficiency, transplantation, atopic diseases and malignancies were excluded.
Data extraction and quality assessment
Two reviewers (OE and VF) independently screened titles and abstracts to determine eligibility for inclusion, according to the predefined inclusion criteria, followed by full-text review when necessary. Data were extracted using a standardised form and included study characteristics: title, authors, journal, publication year, country, study design, study period; population characteristics: study population (AIIRD), controls (when available), number of patients, number of controls, age, gender, ethnicity, immunosuppressive medications; outcome definitions: number of VPI cases, diagnostic criteria used for the diagnosis/definition of infection, IRs and IRRs with 95% CI (when available) or HRs and prevalence rates and prevalence rate ratios (for infections for which IRs were not applicable) or ORs, and the risk of complications (when reported). For studies on incidence that did not report 95% CI, we computed exact 95% CI.
Quality assessment was performed for each study based on the study design: cohort studies were assessed by a critical appraisal adjusted for the specific infection, and cross-sectional studies were assessed by the New Castle Ottawa scale,6 as specified in the online supplementary file 2. Based on the quality assessment, all studies were rated with a level of evidence according to the Oxford Level of Evidence.7 The quality assessment was used to upgrade or downgrade the level of evidence. For example, low-grade quality cohort studies were downgraded from 2b to 4. The present SLR follows the Preferred Reporting Items for Systematic Reviews and Meta-Analyses guidelines.8
Data analysis
Statistical analysis including meta-analysis was performed for the studies reporting on the following diseases: herpes zoster (HZ), human papillomavirus (HPV) infection and hepatitis B (HBV). For HZ, meta-analysis included the original studies that reported the incidence of HZ by disease, whereas studies that reported the incidence of HZ by treatments only were excluded. A very small number of studies in case of influenza and the use of different outcomes in studies on influenza and pneumococcal diseases precluded the performance of meta-analysis. The statistical analysis and graphical presentation were performed using Stata V.12.1 (Stata Corp, College Station, Texas, USA).
For incidence studies (HZ), the incidence rate (IR) was calculated by dividing the number of new cases by the total person time (multiplied by 1000 to present the results per 1000 person-years). The pooled IR was estimated for each type of AIIRD and overall. In addition, the incident rate ratio (IRR) was calculated for HZ studies that compared patients with AIIRD patients with the control group. The pooled IRR was estimated for each type of AIIRD and overall.
For prevalence studies (HBV and HPV), we used the metaprop command to pool the prevalence rate for each type of AIIRD and overall. For studies that compared the prevalence with the control group, the prevalence ratio (PR) was calculated and pooled for each type of AIIRD and overall.
Heterogeneity of the studies was explored using Cochrane’s Q test of heterogeneity (p<0.1 considered statistically significant). Inconsistency in the studies’ results was assessed by I², which describes the percentage of total variation across studies that is due to heterogeneity rather than chance. When I²≥50%, we assumed that there was more than moderate inconsistency. Random effects model (DerSimonian and Laird) was chosen if Cochrane’s Q test p<0.1 or I²≥50%. Otherwise, the fixed effects model (inverse variance methods) was chosen. For quality analysis, we explored the association between the effect size (prevalence, IR, IRR and so on) and the studies quality assessment via metaregression. Sensitivity analysis for HPV included subgroup analysis with and without outlier studies. Publication bias was explored via funnel plots and the Egger test for asymmetry.
Results
The literature search identified 3876 articles and two additional articles identified by experts (figure 1). After removal of duplicates, 3349 studies were screened by abstracts. A total of 230 articles underwent a full-text review. Sixty-three of these met the full inclusion criteria. Data on the incidence/prevalence rates were available for five VPI: influenza, pneumococcal disease, hepatitis B, HZ and HPV.

Flow chart of the literature search. HPV, human papillomavirus; HVB, hepatitis B virus.
Influenza
Annual incidence of influenza in the general population is estimated as 5%–10% of adults, according to the WHO. One in 10 unvaccinated adults are estimated to be infected by seasonal influenza annually, with rates of symptomatic influenza roughly half of these estimates.9
In the 2011 review, two large cohort studies from the USA confirmed a high risk for influenza and influenza-related complications in elderly patients (≥65 years) with rheumatic diseases.3 In the present review, four additional studies reported on the incidence of influenza in the AIIRD population (table 1). The diagnosis of influenza was based either on the patients’ reports of influenza-like illness (ILI) or International Classification of Diseases (ICD) codes.
Two studies addressed the frequency of influenza among patients with rheumatoid arthritis (RA). A large administrative study from the USA provided the most detailed data on the rates of influenza in the RA population compared with controls: influenza IRR 1.2, 95% CI 1.1 to 1.4.9 Influenza-related complications, including pneumonia, stroke and myocardial infarction, within 30 days of influenza diagnosis, were also more common in RA versus controls: IRR 1.8, 95% CI 1.2 to 2.8, translating into a 2.75-fold increase in incidence of influenza-related complications in RA.10 Complications occurred most frequently in patients aged ≥70 years old. Notably, concomitant disease modifying anti-rheumatic drug (DMARD) or biological use did not significantly affect the rate of influenza or its complications.10 A questionnaire-based study from the Netherlands reported a 5.9% incidence of ILI among patients with RA, a twofold higher rate compared with the general Dutch population.11 The use anti-tumour necrosis factor (anti-TNF) therapy was associated with a higher risk of contracting influenza in this study. A questionnaire-based study from Italy reported a 17% incidence of ILI among patients with RA, psoriatic arthritis (PsA), ankylosing spondylitis (AS) and spondyloarthropathy (SpA) treated with biological treatments,12 compared with a lower incidence of influenza in the general Italian population (9.7%). Notably, no significant influenza-related morbidity or hospitalisations were reported in this study. In a Swedish cohort of ANCA-associated vasculitis (AAV), the combined incidence of influenza and pneumonia was significantly higher in patients with vasculitis compared with the general population (IRR 3.3, 95% CI 2.2 to 4.8).13 In summary, the present data suggest a higher risk for contracting influenza in patients with AIIRD compared with the general population.
Streptococcus pneumoniae
Pneumococcal pneumonia is the most common clinical presentation of pneumococcal disease and the most common cause of hospitalisation for community-acquired pneumonia in the adult population.14 15 Since 1998, the incidence of invasive pneumococcal disease (IPD) in the USA has significantly decreased from 100 to 9/100 000 persons in 2015, following the implementation of the vaccination policy for pneumococcal disease.16
In the 2011 review, four studies reported on the incidence of pneumococcal infection in patients with systemic lupus erythematosus (SLE), without comparison to the general population.3 The present literature search yielded seven retrospective cohort studies conducted in the AIIRD population in Europe and USA17–23 (table 2). A large study using the data from USA healthcare claims repositories (2006–2010) identified RA and SLE as risk conditions for both pneumonia and IPD in all age groups.17 Compared with healthy controls, IRR for pneumococcal pneumonia was 4.4, 95% CI 3.8 to 5.2 in patients with RA and 4.3, 95% CI 3.8 to 4.7 in patients with SLE. The highest risk for IPD was reported in young patients of age 18–49 years old, IRR 7.1, 95% CI 4.9 to 10.1.17 Another large study from the UK demonstrated that patients with AIIRD admitted to the hospital or receiving hospital-based care had an increased risk for IPD compared with controls.18 IRR for IPD was highest in SLE 5.0, 95% CI 4.6 to 5.4 and polyarteritis nodosa 5.0, 95% CI 4.0 to 6.0, followed by systemic sclerosis (SSc) 4.2, 95% CI 3.8 to 4.7, Sjögren’s syndrome 3.2, 95% CI 2.9 to 3.5, and the lowest in RA 2.5, 95% CI 2.4 to 2.5.18 Consistently, data from a Canadian population-based surveillance for IPD showed a substantially increased incidence rate of IPD among patients with SLE, SSc, Sjögren’s syndrome and dermatomyositis/polymyositis (DM/PM) during 1995–2012.19 Two studies focusing in particular on patients with SLE have confirmed the previously reported notion of a substantially high risk of pneumococcal pneumonia and IPD in this susceptible population.20 21 Moreover, case-fatality ratio related to IPD in patients with SLE was higher compared with immunocompetent controls, OR 1.3, 95% CI 0.4 to 4.8.19 In summary, the rates of pneumococcal disease are significantly higher in patients with AIIRD compared with immunocompetent controls.22 Patients with SLE, including young patients, are particularly at increased risk for pneumococcal disease, with a more complicated course.23
Pneumococcal disease studies characteristics, pneumococcal disease incidence rates and incidence rate ratios
Herpes zoster (HZ)
The lifetime risk of developing HZ in the general population is between 25% and 30%, rising to 50% in those aged at least 80 years. The estimated average overall incidence of HZ is about 3.4–4.8/1000 person years, increasing to more than 11/1000 person years in those aged ≥80 years.24
In the 2011 review,3 the incidence of HZ in RA ranged from 0.55 to 14.5/1000 person years in different studies. RA per se and the use of steroids, conventional synthetic DMARDs (csDMARDs) and anti-TNF therapies were identified as predisposing factors to develop HZ. In SLE, a significantly increased incidence of HZ was consistently reported, ranging from 16 to 91.5/1000 person years. The increased risk of HZ among patients with SLE was estimated as fivefold to 16-fold compared with the general population and as threefold compared with other musculoskeletal disorders. Immunosuppressive therapies were associated with the increased risk of HZ in SLE. Increased incidence of HZ was also observed in systemic vasculitis and PM/DM.3
The present review has contributed 29 studies,25–51 among them 2 meta-analyses,52 53 expanding the data on the incidence of HZ in AIIRD (table 3). Eleven studies included a control group.25 28 34 39 40 44–46 49–51 Based on the analysis of 21 studies including 894 891 patients, pooled IR and pooled IRR were calculated for patients with AIIRD in general and for specific disease subtypes (figure 2; s upplementary file table 1). In comparison to the general population, the risk of HZ infection in the AIIRD population was increased, pooled IRR 2.9, 95% CI 2.4 to 3.3, based on 11 studies, n=762 553 patients. The results of the studies were heterogeneous as reflected by Q test (p<0.1), except for studies in DM with a low heterogeneity (Q test p=0.6). Publication bias assessed by funnel plots of the IR and IRR (online supplementary figure 1) showed an asymmetric distribution of the results, whereas Egger’s meta-regression tests with quantitative and descriptive p values were non-significant (p>0.1).
HZ studies characteristics and HZ incidence rate (IR), incidence rate ratio (IRR) and HR according to AIIRD
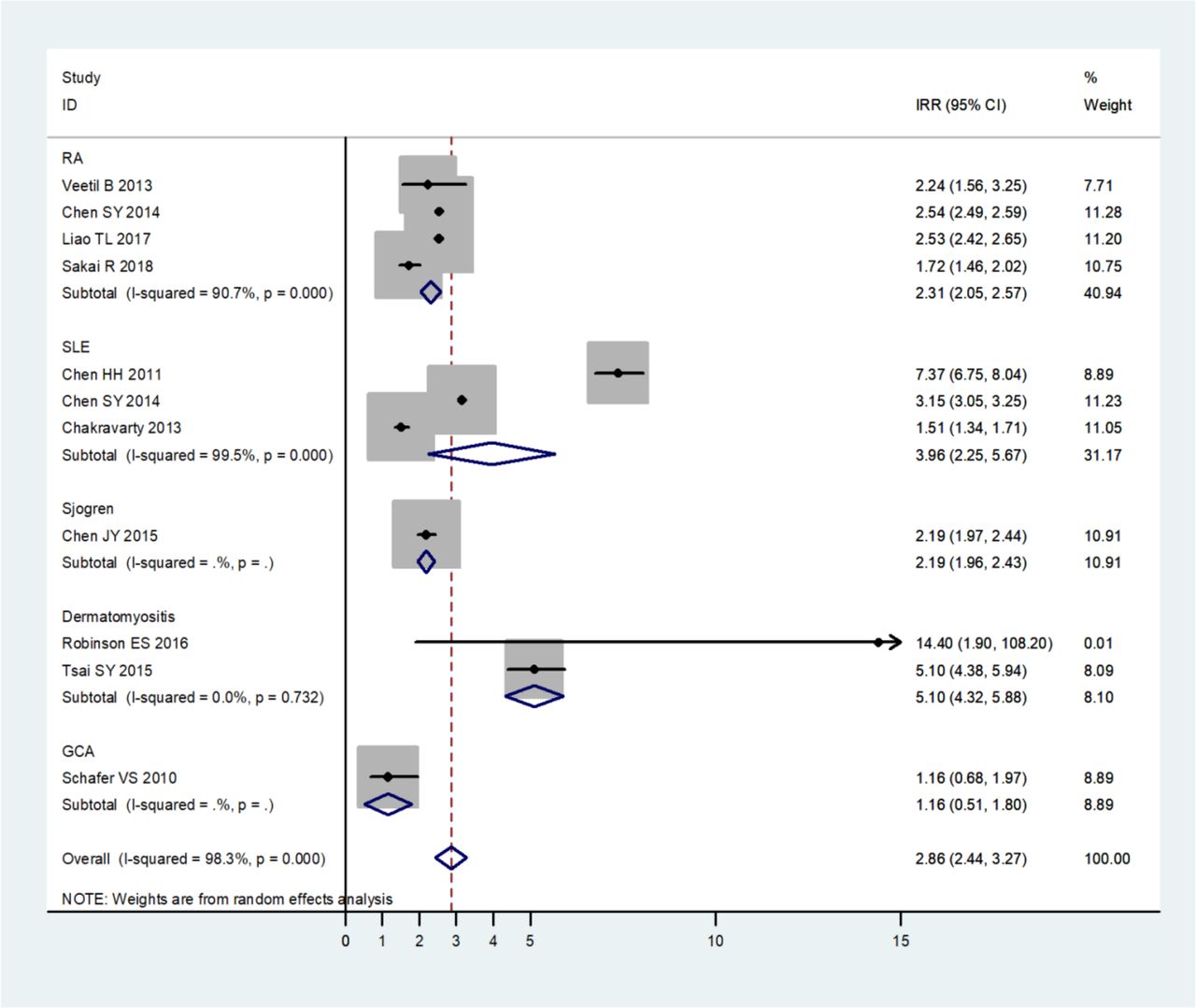
Forest plot of the meta-analysis of pooled incidence rate ratios (IRRs) of herpes zoster in patients with autoimmune inflammatory rheumatic diseases compared with the general population. GCA, giant cell arteritis; RA, rheumatoid arthritis; SLE,systemic lupus erythematosus.
In RA,25–40 the incidence of HZ ranged from 6.7 to 21.3/1000 person years, with the highest incidence observed in the elderly patients.34 The risk of HZ infection among patients with RA was estimated to be twofold compared with the healthy population within the same age range. Among patients with RA, the pooled IR (based on nine studies, n=726 711 patients with RA) was 11.6/1000 person years, 95% CI 9.4 to 13.9 vs 6.5, 95% CI 4.7 to 8.2/1000 person years among controls (based on four studies, n=473 406 controls); the pooled IRR 2.3, 95% CI 2.1 to 2.6 based on four studies (85 419 patients with RA and 473 406 controls). A meta-analysis of five studies further confirmed the increased risk of HZ in patients with RA, pooled IRR of 1.7, 95% CI 1.4 to 2.0.53
The rates of HZ-related complications were reported by a number of studies.25 27 29 37 38 40 Overall, the rate of disseminated disease and HZ-related hospitalisation was low. The IR of disseminated HZ ranged from 0.2, CI 95% 0.1 to 0.6/1000 person years in a Japanese study40 to 3, CI 95% 2 to 4/1000 person years in a pooled analysis of patients with RA exposed to tofacitinib in clinical trials.38 Importantly, a study from Taiwan reported an increased risk of stroke in patients with RA with HZ compared with patients with RA without HZ (adjusted hazard rate (aHR) 1.3, p=0.047), particularly in those with HZ-related neurological complications (aHR 1.5, p=0.015).39 The following risk factors for HZ infection in RA were identified: old age, high disease activity and dose-related use of glucocorticoids (GCs).25 26 29 30 32 37 54 No clear association between the use of MTX and HZ infections in RA was established.55 The role of anti-TNF and other biological therapies regarding the contribution to HZ risk in RA remains controversial. Some studies reported that treatment with anti-TNF agents significantly increased the risk of HZ compared with csDMARDs27 31 37 52 and was associated with more severe HZ disease.27 54 Others reported a similar risk of HZ in patients with RA treated with different csDMARDs and biologic DMARDs.29 30 32 33 40 56 The use of an anti-JAK inhibitor, tofacitinib, doubled the risk of HZ in RA compared with other biologics.35 54 Similarly to tofacitinib, baricitinib was also associated with a particular increased risk of HZ, which served the main reason for the treatment discontinuation in a clinical trial.57
In SLE, the incidence of HZ ranged from 6.4 to 37.7/1000 person years28 34 43–45 and was estimated two fold to 10-fold higher compared with the general population.28 43–45 The pooled IR of HZ infection was 18.9, 95% CI 8.1 to 29.6/1000 person years in SLE vs 5.1, 95% CI 4.5 to 5.6/1000 person years in controls. The pooled was IRR 4.0, 95% CI 2.3 to 5.7, based on three studies including 155 959 patients and 51 087 635 controls. Another meta-analysis of four studies confirmed the increased risk of HZ in patients with SLE: pooled RR of 2.1, 95% CI 1.4 to 3.2.53 Importantly, patients with SLE aged 18–30 years had the highest risk for HZ infection compared with older patients with SLE.34 44 Risk factors for HZ in the SLE populations mainly included use of GCs and immunosuppressive therapy in a dos- dependent manner.28 43 45 58 Notably, the new pipeline medications for SLE including anti-interferon-a antibodies, anifrolumab59 and sifalimumab,60 also seem to contribute to the increased risk of HZ. To underline the burden of HZ in patients with SLE, a trend for increased hospitalisation rates due to HZ in SLE versus non-SLE patients was observed over the last decade.61
Among other AIIRD, a particularly high incidence of HZ was reported in patients with DM and PM compared with controls with a pooled IRR 5.1, 95% CI 4.3 to 5.9/1000 person years.47–50 These studies were notable for a low heterogeneity (Q test p 0.6). Patients with primary Sjögren46 and giant cell arteritis51 also had a high risk to contract HZ, as reflected by a single study for each disease group. In summary, the present review demonstrates an increased risk of HZ infection in patients with AIIRD compared with the general population, with the highest risk in patients with inflammatory myositis and GCA, followed by SLE and RA.
Human papillomavirus (HPV)
The global prevalence of HPV infection is estimated as 11.7%, 95% CI 11.6 to 11.7, with considerable regional differences, with higher rates reported in sub-Saharan Africa (24%), Eastern Europe (21%) and Latin America (16%).62 The highest HPV prevalence is observed at young ages, peaking in women younger than 25 years (24.0%; 23.5 to 24.5), then declining in older ages.62 The majority of HPV infections (70%–90%) are asymptomatic and transient, resolving spontaneously in 1–2 years. Certain HPV serotypes (‘high-risk’) are responsible for cervical dysplasia, premalignant abnormalities and cervical cancer. HPV16 is the most frequent oncogenic type, followed by HPV18, HPV52, HPV31 and HPV58.63
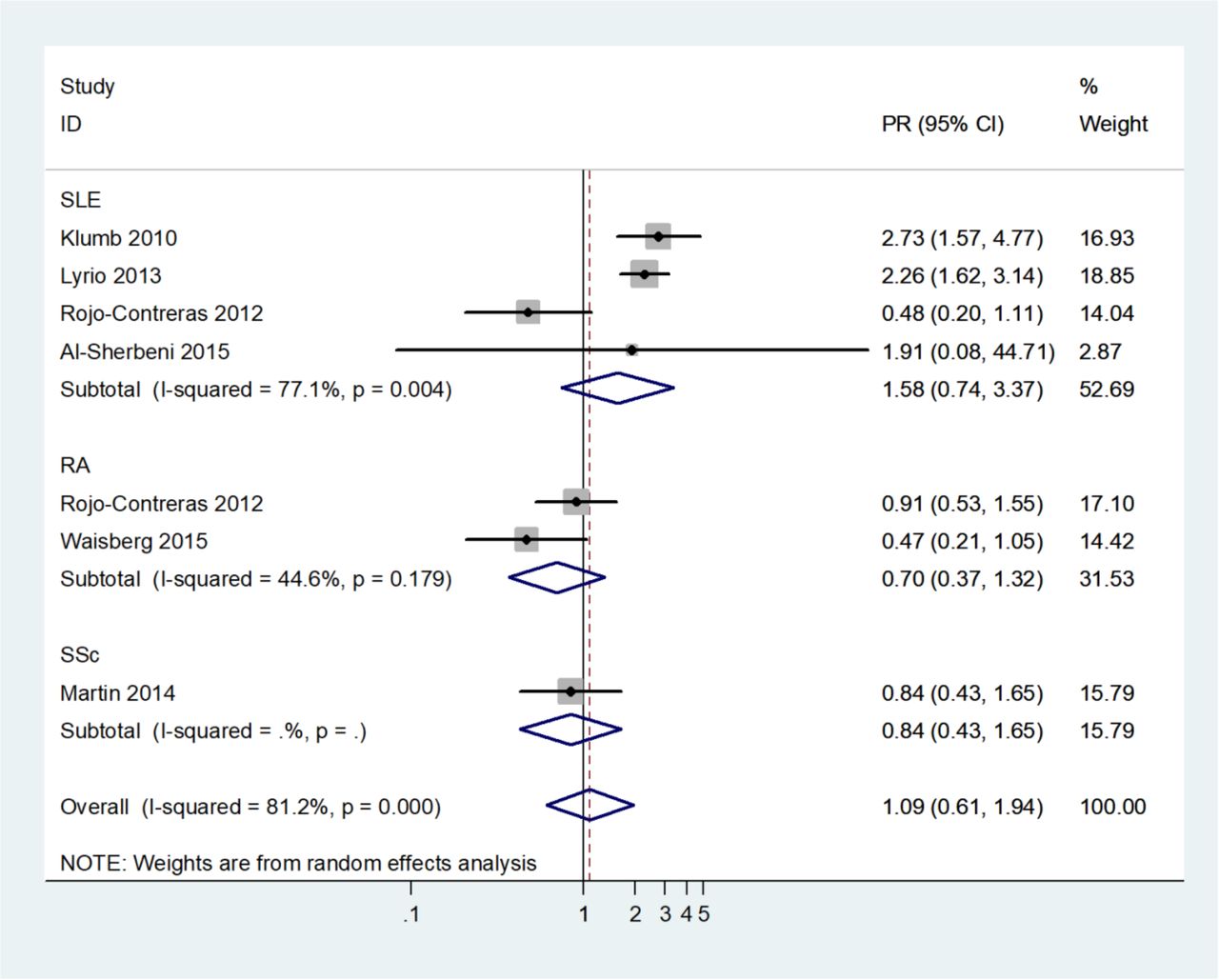
In the 2011 review,3 five studies reported on the increased prevalence of HPV cervical infection in female patients with SLE compared with the general population.64 65 The present review has significantly expanded the knowledge on the genital HPV infection in SLE (n=11),66–76 RA (n=2)69 77 and SSc (n=1), including 1313 patients altogether78 (table 4). Most studies on the SLE population were conducted in Latin America (n=9), followed by Asia (n=2). The HPV prevalence mainly ranged from 12% to 30% of HPV in patients with SLE, with two exceptions: a negligible prevalence in a small group of patients with SLE in Egypt73 and a strikingly high prevalence in a Brazilian SLE cohort.70 The authors suggested that using a very sensitive technique of PCR (n-PCR) might have resulted in a significant increase in the detection of the virus.70 Seven studies also reported the prevalence of cervical dysplasia, including the high-grade squamous intraepithelial lesions (HGSILs).67–70 72 76 77 The pooled prevalence of HPV and pooled prevalence and prevalence ratios of HPV, high-risk HPV and HGSIL are summarised in table 2 in the supplementary file and depicted in figure 3. Most studies were heterogeneous as estimated by the Q test, with the exception of data on HGSIL. For publication bias assessment, a funnel plot of the prevalence of HPV, high-risk HPV and HGSIL was depicted (figure 2 in supplementary file), with Egger’s meta-regression tests with quantitative and descriptive p values being non-significant (p>0.1).
Genital human papillomavirus (HPV) infection studies characteristics and HPV incidence/prevalence rates
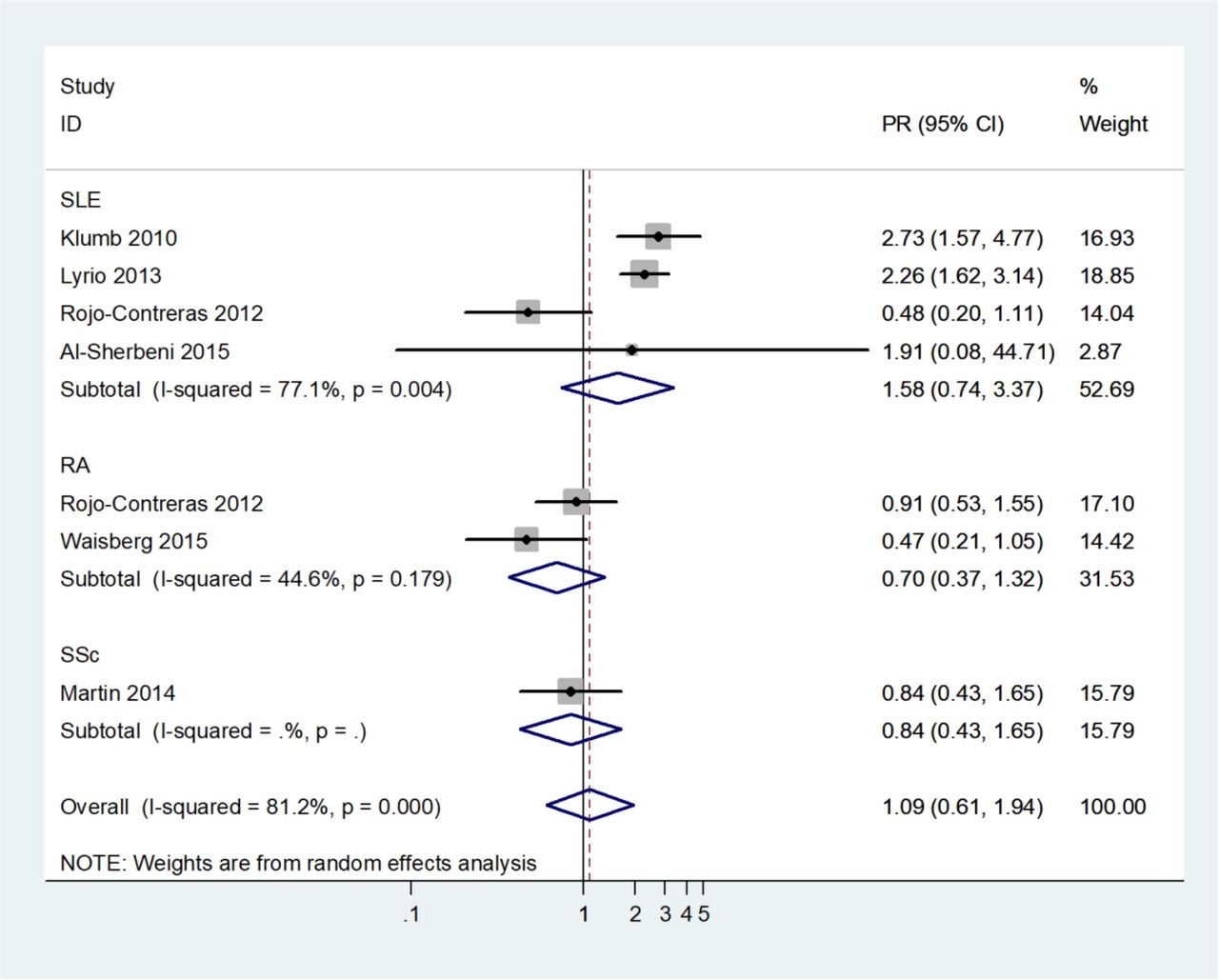
Forest plot of the meta-analysis of pooled prevalence ratio (PR) of human papillomavirus in patients with autoimmune inflammatory rheumatic diseases compared with the general population. RA, rheumatoid arthritis; SLE, systemic lupus erythematosus; SSc, systemic sclerosis.
A limited number of studies included a control group, reporting a higher prevalence of HPV in SLE compared with controls in two studies66 68 and the opposite in a small Mexican cohort.69 Compared with the general population, pooled prevalence ratio of HPV in SLE patients was 1.6, 95% CI 0.7 to 3.4. Excluding the study by Rojo-Contreras et al,69 with an exceptionally high background HPV prevalence in the control group, from the analysis resulted in a statistically significant pooled PR for SLE – 2.4, 95% CI 1.8 to 3.2.
In patients with RA, no difference in the prevalence of HPV was found between patients and controls (pooled PR 0.7, 95% CI 0.5 to 1.1). Furthermore, important information on HPV persistence, clearance and incidence of de novo infection was obtained from cohort studies (n=3) of patients with SLE with a follow-up to 3 years.67 74 76 In one study, the cumulative prevalence of HPV infection and specifically high-risk HPV infection significantly increased from 12.5% to 25.0% after 3 years (p=0.006) and from 11.1% to 20.8% after 3 years (p=0.02), respectively.67 Overall, 90.6% of the preexisting infection and 14.7% of the incident infections were cleared,67 consistent with a high clearance rate of 88.6% in another study.74 The rate of acquisition of a new HPV infection was about 13%.76 Risk factors for HPV infection among patients with SLE were similar to the general population, including multiple sexual partners,74 previous HPV infection, previous sexually transmitted disease66 and younger age.71 The presence of SLE itself was found as an independent predictor for HPV infection,70 and a risk factor for high-risk HPV types.68 The impact of immunosuppressive therapy on the increased prevalence of HPV remains controversial, with some data supporting a causal relation, especially related to a high cumulative dose of corticosteroids, azathioprine and cyclophosphamide exposure.66 69 71 74
In RA, a lower prevalence of HPV infection was observed in pre-anti-TNF-treated patients compared with controls (14% vs 30 %, p=0.054).77 Treatment with anti-TNF (for 6 months) did not increase a risk of exacerbation and/or progression of HPV in this small cohort.77 In a small study of patients with SSc (n=25, 80% limited SSc), the prevalence of HPV was similar in patients and controls (32% vs 38%).78 High-risk HPV52 was the most common genotype with a greater multi-HPV infection rate.78
In summary, the prevalence of genital HPV infection, including high-risk HPV serotypes and HGSIL, was increased in the female population with SLE from Latin America and Asia and comparable to the general population in patients with RA and SSc, based on the limited data.
Hepatitis B (HBV)
The epidemiology of HBV infection widely varies around the globe. The seroprevalence of hepatitis B surface antigen (HBsAg), reflecting chronic infection with HBV, is estimated as 3.6% (95% CI 3.6% to 3.6%) worldwide, with the highest prevalence in countries of the African (total 8.8%, CI 8.8% to 8.8%) and Western Pacific regions (total 5.3%, CI 5.3% to 5.3%).79 In the Americas and the WHO European region, the prevalence ranges from 0.2% to 13.6%.79
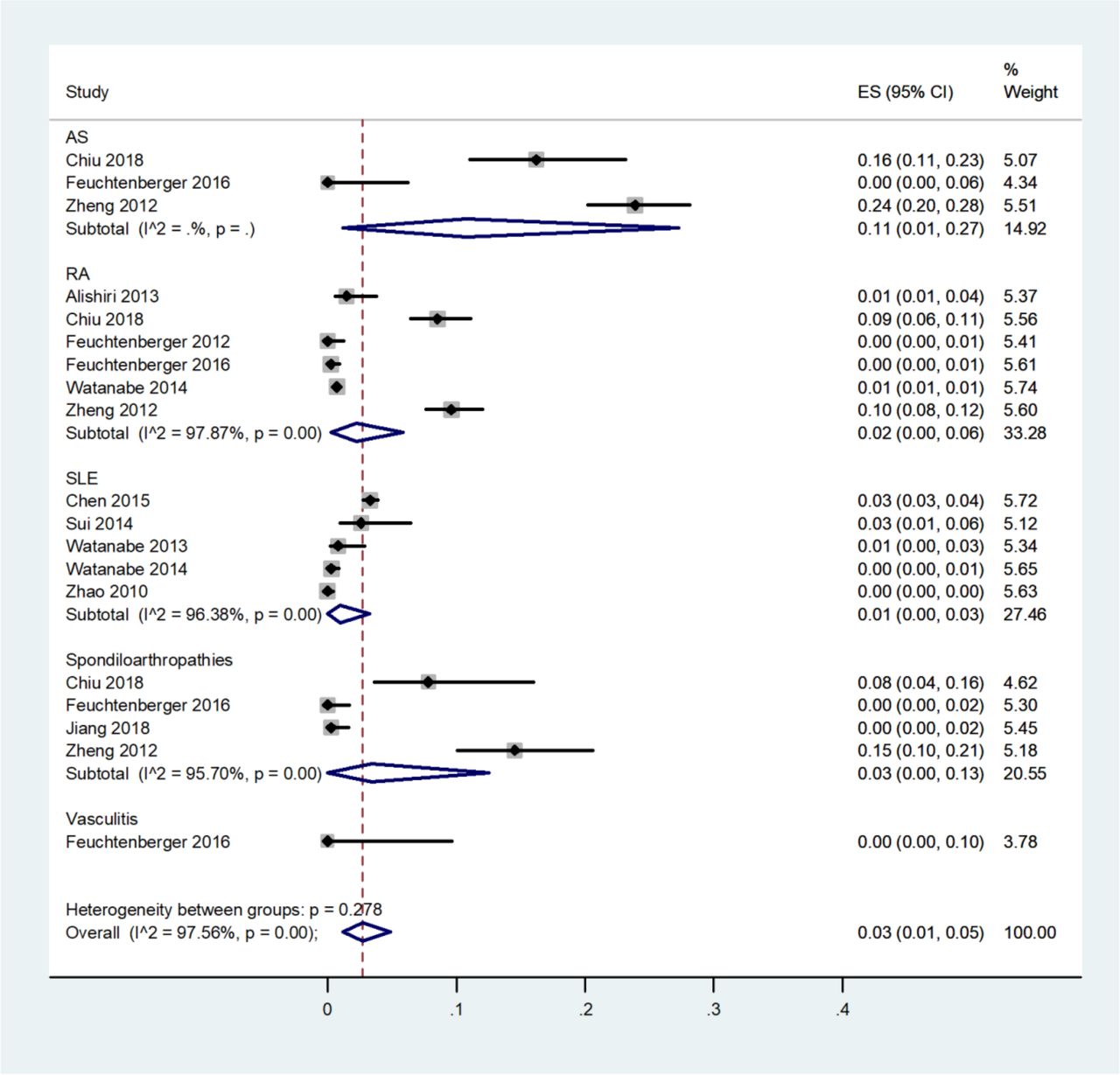
The scope of the SLR performed in 2011 did not include data on HBV infection. The present SLR retrieved 10 cross-sectional studies, conducted mainly in the Asian population (China, Japan, Taiwan) on the seroprevalence of HBV, defined by positive HbsAg and/or positive anti-hepatitis B core antibody (anti-HBc) among patients with AIIRD.80–89 All studies were of cross-sectional design with level of evidence 3b.
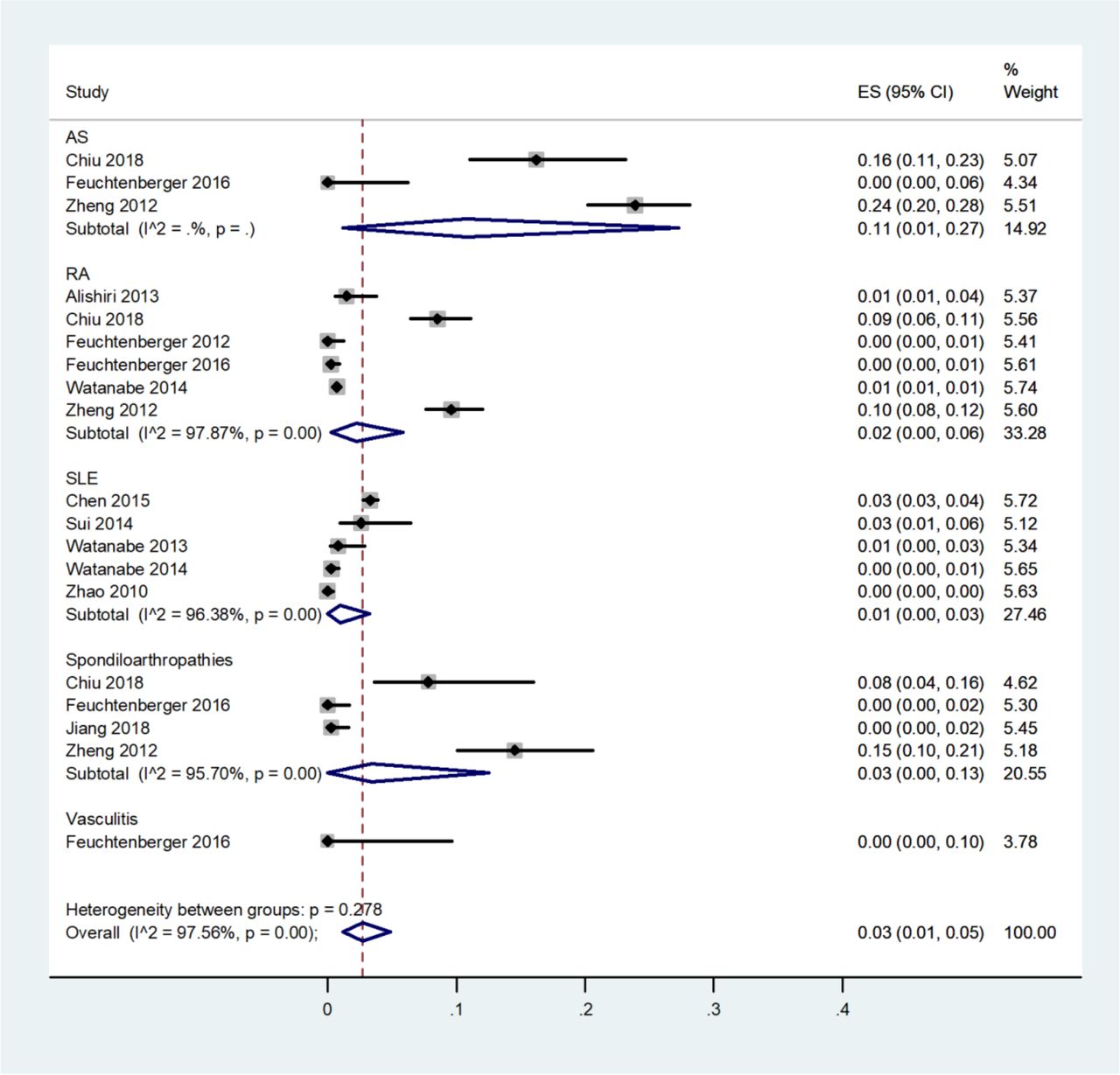
The documented HBV seroprevalence differed considerably between the studies (table 3 in the supplementary file). The lowest prevalence of HBsAg was reported in patients with SLE, followed by RA and SpA in the increasing order, with the highest prevalence detected in patients with AS.82 89 The pooled seroprevalence of HBsAg was 3% (95% CI 1% to 5%) and for anti-HBc 15% (CI 95% 7% to 26%) (figure 4; table 4 in the supplementary file). There was a high heterogeneity among the studies, Q<0.1. For publication bias assessment, a funnel plot of the seroprevalence results was depicted (figure 3 in the supplementary file) with Egger’s meta-regression tests with quantitative and descriptive p values being non-significant (p>0.1). Overall, in the present studies, the prevalence of HBV in the AIIRD population seems to be similar, and in some studies even lower,80 86 87 compared with the general population.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Forest plot of pooled prevalence of hepatitis B surface antigen virus in patients with autoimmune inflammatory rheumatic diseases. AS, ankylosing spondylitis; RA, rheumatoid arthritis; SLE, systemic lupus erythematosus.
Discussion
This SLR presents the update on the incidence and prevalence of VPI among patients with AIIRD. The results of the SLR highlight the insufficient data on the epidemiology of most VPI in the AIIRD population. In fact, data were available on only 5 out of 18 searched VPI: influenza, S. pneumonia e, HZ, HPV and HBV infections. Furthermore, there was a paucity of European studies addressing the epidemiology of HPV and HBV infections, with most studies being conducted in Latin America and Asia. However, this information was extremely useful in the process of formulation of the recommendations for vaccination in patients with AIIRD, since it emphasised the increased prevalence of influenza, S. pneumonia e, HZ and HPV among patients with AIIRD, especially encouraging vaccination against these agents. The observation of a similar prevalence of hepatitis B infection among patients with AIIRD and the general population supported the recommendation to vaccinate patients with AIIRD for HBV as indicated for the general population.
Concerning influenza, patients with AIIRD are prone for contracting influenza and influenza-related complications compared with the general population. A limited number of the eligible studies (n=4) and their heterogeneous outcomes (patient reported ILI symptoms and ICD codes) precluded the performance of a meta-analysis. Lack of data concerning microbiological confirmation of the diagnosis of influenza should be noted in all four studies. This limitation is pertinent to epidemiological studies on influenza in general, as the evaluation of the precise incidence of influenza represents a complex epidemiological challenge, due to lack of access to sensitive and specific diagnostic tests, difficulty obtaining specimens for testing, the unpredictability of influenza epidemics, and the complexity of assembling and following large cohorts.90
Concerning pneumococcal infection, patients with AIIRD are prone for contracting pneumococcal disease compared with the general population. Importantly, patients with SLE, including young patients, are at particular increased risk for pneumococcal disease.23 In this dataset, heterogeneity of the outcomes and reporting the pneumococcal disease incidence for the combined groups of inflammatory diseases, including inflammatory bowel diseases in some studies, precluded conducting a meta-analysis.
With regard to HZ, the sample size of studies reporting the incidence of HZ infection, most of which were of moderate to good quality, permitted the performance of a meta-analysis, that unequivocally demonstrated that patients with AIIRD are at increased risk to contract HZ compared with the general population. This conclusion was consistent with the previous 2011 review results. A particularly high risk for HZ was observed in patients with inflammatory myositis and SLE, including young patients with SLE, for whom vaccination for HZ has not been approved by the regulatory agencies but only for those aged 50 years and older. Importantly, the burden of HZ in SLE is also reflected by an increasing trend in hospitalisation for HZ in patients with SLE in the recent decade.61 91
The prevalence of HPV infection is significantly affected by both geographical distribution and socioeconomic status of the population, factors that may preclude extrapolation of the data retrieved in the present SLR to the European AIIRD population. Most studies included in the meta-analysis showed a tendency towards a higher prevalence of genital HPV, including high-risk serotypes of HPV, and HGSIL in patients in SLE but not in patients with RA and SSc. These data should be cautiously interpreted given the heterogeneity of the studies and their diverse geographical distribution (Latin America and Asia).
The common assumption is that the increased prevalence of influenza, pneumococcal disease, HZ and HPV is related to the status of immunodeficiency inherent to the nature of autoimmune diseases and immunosuppressive treatments. Concerning HPV, it has been suggested that the virus itself may be a trigger for the onset or exacerbation of SLE.92 93
The meta-analysis of the seroprevalence of chronic HBV infection in patients with AIIRD mirrored the global epidemiology of the disease in the general population.
This SLR reports an increased risk of VPI in patients with AIIRD, emphasising that prevention of infections is essential in these patients. In addition, it highlights the importance of the epidemiological research of the incidence and prevalence of VPI in patients with AIIRD. The proposed research agenda, therefore, includes the collection of reliable epidemiological data using standardised methodology of disease rates and development of prevention and control strategies for infectious diseases in patients with AIIRD.
Supplemental material
References
- 1.↵
- 2.↵
- 3.↵
- 4.↵
- 5.↵
- 6.↵
- 7.↵
- 8.↵
- 9.↵
- 10.↵
- 11.↵
- 12.↵
- 13.↵
- 14.↵
- 15.↵
- 16.↵
- 17.↵
- 18.↵
- 19.↵
- 20.↵
- 21.↵
- 22.↵
- 23.↵
- 24.↵
- 25.↵
- 26.↵
- 27.↵
- 28.↵
- 29.↵
- 30.↵
- 31.↵
- 32.↵
- 33.↵
- 34.↵
- 35.↵
- 36.↵
- 37.↵
- 38.↵
- 39.↵
- 40.↵
- 41.↵
- 42.↵
- 43.↵
- 44.↵
- 45.↵
- 46.↵
- 47.↵
- 48.↵
- 49.↵
- 50.↵
- 51.↵
- 52.↵
- 53.↵
- 54.↵
- 55.↵
- 56.↵
- 57.↵
- 58.↵
- 59.↵
- 60.↵
- 61.↵
- 62.↵
- 63.↵
- 64.↵
- 65.↵
- 66.↵
- 67.↵
- 68.↵
- 69.↵
- 70.↵
- 71.↵
- 72.↵
- 73.↵
- 74.↵
- 75.↵
- 76.↵
- 77.↵
- 78.↵
- 79.↵
- 80.↵
- 81.↵
- 82.↵
- 83.↵
- 84.↵
- 85.↵
- 86.↵
- 87.↵
- 88.↵
- 89.↵
- 90.↵
- 91.↵
- 92.↵
- 93.↵
Footnotes
Contributors VF, with collaboration with OE, performed literature search and reviewed articles on the prevalence and/or incidence of vaccine preventable diseases in patients with autoimmune inflammatory rheumatic diseases. The systematic literature review (SLR) and meta-analysis, when applicable, was performed under the supervision by SvA, the expert in infectious diseases, and the methodologists, JMvL and RL. The results of the SLR were presented to all task force members, discussed and reviewed during the task force meetings. VF drafted and edited the manuscript, under the supervision of OE. All authors read and approved the final version of the manuscript.
Funding This project was supported by EULAR.
Competing interests MD reports grants and personal fees from Pfizer, grants and personal fees from Abbvie, grants and personal fees from UCB, grants and personal fees from Novartis, grants and personal fees from Lilly, grants and personal fees from Merck, grants and personal fees from Roche, grants from BMS, outside the submitted work. OE reports grants and personal fees from Pfizer, grants, personal fees from Abbvie, grants and personal fees from Roche, grants and personal fees from Janssen, personal fees from Novartis and Lilly. AM reports grants and personal fees from Abbvie, grants and personal fees from Pfizer, grants and personal fees from BMS, grants and personal fees from UCB, grants and personal fees from Merck, during the conduct of the study. KW reports personal fees from Pfizer, during the conduct of the study; grants and personal fees from Biotest, grants and personal fees from CSL Behring, personal fees from LFB, personal fees from Grifols, grants from BMS, personal fees from Baxter, personal fees from Roche, personal fees from Octapharma, outside the submitted work.
Patient consent for publication Not required.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement All data relevant to the study are included in the article or uploaded as supplementary information.