Article Text

Statistics from Altmetric.com
Key messages
What is already known about this subject?
Large granular lymphocyte expansion (LGLe) have frequently been described in association with rheumatoid arthritis, but rarely with primary Sjögren’s syndrome (pSS).
The role of LGLe in neutropenia following treatment with rituximab (RTX) has already been suggested in patients with lymphoma.
What does this study add?
Our study suggests for the first time that LGLe associated neutropenia could be a side effect of RTX in patients with pSS.
Methotrexate could be useful in case of severe neutropenia.
How might this impact on clinical practice?
RTX being more and more used in systemic auto-immune diseases, this possible effect must be known.
Primary Sjögren’s syndrome (pSS) is a systemic auto-immune disease (AID) that mainly causes mucosal dryness, asthenia, arthralgia and, sometimes, severe organ involvement requiring immunosuppressive treatment. Despite negative randomised controlled trials, rituximab (RTX) is frequently used in case of systemic complications.1
Large granular lymphocyte (LGL) disorders are characterised by proliferation of LGL cytotoxic lymphocytes of either T-cell (mainly CD3+TCRαβ+CD8+CD57+CD56+/−CD16+/−, rarely CD4+CD8+/−) (T-LGL) or less frequently NK-cell (CD3-CD2+CD16+CD56+CD57+/−) (NK-LGL) origin. The spectrum of LGL disorders extends from reactive LGL expansions (LGLe), which are usually asymptomatic, transitory and have polyclonal or oligoclonal profile, to LGL leukaemias, which are monoclonal proliferations associated with cytopenias and somatic activating mutations in STAT3.2 T-LGL expansions (T-LGLe) have frequently been described in several AIDs,2 especially rheumatoid arthritis (RA). In this context, they could exhibit either polyclonal, oligoclonal or monoclonal profile, and could be accompanied by neutropenia irrespective of their clonal status.3 However, LGLe have been exceptionally reported in pSS. Thus, we here report eight cases of LGLe in patients with pSS.
In our study, all patients from the Paris-Sud hospital, national reference centre for pSS, diagnosed with pSS and having a LGLe were retrospectively included between September 2016 and March 2018. Diagnosis of pSS was based on ACR/EULAR 2016 criteria.4 Three of our eight patients did not fulfil these criteria, but diagnosis was validated by experts from our reference centre based on anti-SSA antibodies (patient 4), focal sialadenitis (patient 3) and/or associated specific systemic complications (patients 3 and 7) (table 1). Collected data included: clinical and biological characteristics, treatments received for LGLe or pSS and patients’ outcome. Disease activity was measured using the EULAR Sjögren Syndrome Disease Activity Index (ESSDAI),5 with active disease defined as an ESSDAI ≥5. Since neutropenia was considered as a feature of LGLe, it was not included in the calculation of the ESSDAI. LGLe were defined on flow cytometry results, as monoclonal, oligoclonal or polyclonal, expansions of T-cells or NK-cells harbouring an LGL phenotype (different combinations of CD57, CD56 and CD16 markers), representing ≥10% of peripheral lymphocytes. In patients with T-LGLe, Vβ repertoire analysis of the T-cell receptor was performed to assess clonal rearrangement. When possible, STAT3 mutational status of LGL cells by direct sequencing was also performed.
Characteristics of patients and LGL expansions
LGLe were identified in eight pSS patients. Their main characteristics are reported in table 1. All but one had active disease at the time of LGLe diagnosis (median ESSDAI: 11 (range: 3–35)) and a history of systemic manifestations. Circumstances of LGLe diagnosis were neutropenia (n=6), hyperlymphocytosis (n=1) and incidental (n=1). Seven patients (87.5%) had a T-LGLe, all having a predominant T-CD8+population, but three patients had additional LGL-type T-cell populations: CD4+CD8+in one and CD4+CD8 in two. In these three patients, each LGL population displayed expansions of different TCR Vβ families. T-LGLe were monoclonal in two patients and oligoclonal in four patients; clonality has not been assessed in one. One patient had NK-LGL expansion whose clonality could not be determined. STAT3 mutation was negative in the three patients tested.
Neutropenia (<1500/mm3) was observed in 6 (75.0%) patients and was <500/mm3 in 3 (37.5%) of them. Lymphocyte phenotyping showed an inverted CD4/CD8 ratio (<1) in four patients with absolute CD4+lymphopenia (<500/mm3) in three patients and CD8+lymphocytosis (>1000/mm3) in three patients; CD19+cell counts were low or undetectable in all the patients previously treated by RTX, normal in others. Five patients had received RTX (one for lymphoma, four for pSS systemic manifestations of cryoglobulinemia). The median time between LGLe diagnosis and first RTX injection was 7 months (range 15 days to 12 months). In all patients who received RTX, a lymphocyte immunophenotyping was performed prior to RTX administration and did not reveal any LGLe. Neutropenia occurred in 4/5 patients having received RTX and in 2/3 in patients who did not receive RTX. Patient 8 was retreated with RTX for a cryoglobulinemia relapse: neutropenia occurred after the first cycle of RTX (1200/mm3) and worsened after the second (700/mm3).
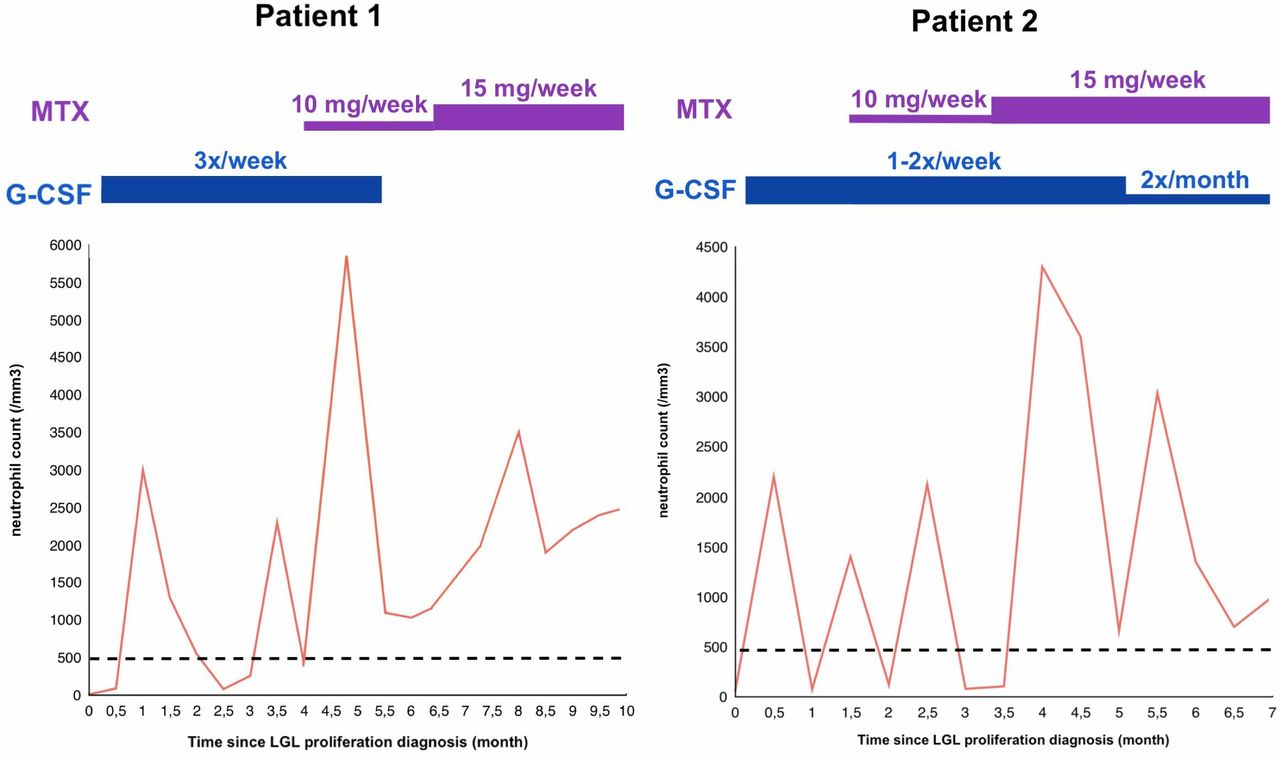
In two patients, severe neutropenia required treatment by Granulocyte-Colony Stimulating Factor (G-CSF) which only led to transient efficacy. Methotrexate was added in these two patients; it allowed neutrophil count normalisation in one case and improvement of neutropenia in the other (figure 1). Among the four remaining neutropenic patients, spontaneous remission occurred in one and non-severe neutropenia persisted in the three others.
{kind=link}
Treatments and Changes in neutophil counts in patient 1 and 2. LGL, large granular lymphocyte; MTX, methotrexate.
Contrarily to RA, there are only a few reports of LGLe in pSS patients. Friedman et al6 reported that pSS was present in 27% of patients in a case series of 48 patients presenting with T-LGL leukaemia. However, the other studies having explored the prevalence of systemic AIDs in LGL disorders did not underline a specific association with pSS.7
Since all pSS patients with LGLe had an active disease, the hypothesis of a relationship between pSS activity and occurrence of LGLe could be raised. Nevertheless, since 5/8 patients developed LGLe after treatment with RTX, LGLe may be linked to RTX treatment rather than to pSS itself. Neutropenia is a well-known adverse effect of RTX, particularly late onset neutropenia (occurring >4 weeks after treatment). Its frequency is estimated around 7%–27% in lymphoma,8 1.3%–3% in RA and 2.3% in other AIDs.9 Of note, in this context, LGLe may not necessarily be monoclonal.10 Several pathogenic hypotheses have been raised and expansion of T-LGL cells is one of them. Indeed, LGLe could induce immune-mediated neutropenia via Fas/Fas-ligand dependent pathways, antineutrophil antibodies production and/or myelosuppression.8
Mechanisms by which RTX could induce T-LGLe remains unclear. One can wonder if RTX could lead to depletion of regulatory B-cells implicated in immune surveillance against T-cell clones. Alternatively, CD4+T cell depletion has been described after RTX in RA patients.11 If some of these T-cells are regulatory, their depletion might promote expansion of LGL cells. Among our patients who received RTX, three presented an inverted CD4/CD8 ratio and three presented absolute CD4+lymphopenia. An increased production of STAT3-activating cytokines, such as interleukin 6, triggered by RTX administration could be another hypothesis.
Surprisingly, Schwaneck et al did not identify RTX as a risk factor for LGLe in RA.12 Also, RTX has been used in the treatment of LGL leukaemia associated with RA, sometimes with success.13 This opposite effects of RTX suggest different mechanisms underlying LGLe: changes in regulatory cells/cytokine profile induced by RTX treatment on the one hand, or beneficial effect of RTX on persistent antigenic stimulation due to an active AID on the other hand.
In our study, the number of LGL cells was lower than the usual threshold used to define LGL leukaemia (≥500/mm3) in 4/8 patients. However, LGLe represented ≥10% of total lymphocytes, a threshold recently proposed in RA.12 In fact, these four patients had a global lymphopenia (<1000/mm3) due to disease activity and/or associated treatments. Thus, the relative threshold of ≥10%, seems to be more appropriate in the context of AIDs, where peripheral lymphopenia is a hallmark of the disease.
Finally, we hypothesise that, even small, these LGLe could be involved the pathogenesis of neutropenia. Nevertheless, although T-LGLe have been previously reported in post-RTX neutropenia in patients with lymphoma, our study lacks power to affirm with certainty the existence of a link between RTX administration and LGLe. However, the simultaneous occurrence of LGLe and neutropenia made this link likely. Bone marrow examination, anti-neutrophil antibody testing and measurement of soluble Fas ligand might have been useful to determine the exact mechanism of neutropenia but have not been performed.
In conclusion, these results suggest for the first time that post-RTX neutropenia could be linked to LGLe in pSS patients, as already observed in lymphoma but rarely in RA. Also, methotrexate could be a valid therapeutic option in severe cases. While RTX is frequently used in different systemic AIDs, this possible effect must be known by clinicians. However, larger scale studies are needed to confirm this relationship between RTX administration, LGLe and neutropenia in patients with AIDs.
Footnotes
AB and GN contributed equally.
XM and RS contributed equally.
Presented at This letter is based on work previously presented at the 2018 ACR/ARHP Annual Meeting*.
*Baber A, Nocturne G, Mariette X, Seror R. Large Granular Lymphocyte Proliferations in Primary Sjögren’s Syndrome: An Iatrogenic Manifestation [abstract]. Arthritis Rheumatol. 2018; 70 (suppl 10). https://acrabstracts.org/abstract/large-granular-lymphocyte-proliferations-in-primary-sjogrens-syndrome-an-iatrogenic-manifestation/. Accessed October 28, 2018.
Contributors All authors contributed to the manuscript. AB, XM and RS were responsible for conception and design. AB, GN, JH, RB, RK, XM and RS were responsible for collection of data and analysis. All authors were responsible for the interpretation of data. AB and RS wrote the first version of the manuscript. All authors critically revised and approved the final version of the manuscript.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests RS received consulting fees from Roche (<10.000€). Other authors declared any competing interest in link with the present study.
Patient consent for publication Not required.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement All data relevant to the study are included in the article.