Article Text

Abstract
Objectives To describe electrocardiographic (ECG) development in patients with ankylosing spondylitis (AS) and identify associations between baseline characteristics and cardiac conduction disturbances (CCD) at 5-year follow-up.
Methods In a longitudinal cohort study, 172 patients (54% men, mean age (SD) of 50 (13) years at baseline) with AS underwent ECG, physical examination, questionnaires and laboratory testing at baseline and at 5-year follow-up. Descriptive statistics and univariate and age- and sex-adjusted logistic regression analyses were used. CCD included both atrioventricular and intraventricular blocks.
Results Twenty-three of the 172 patients (13.4%) had a CCD at follow-up. Eight patients had developed a new CCD and eight had normalised their ECG. In the age- and sex-adjusted analyses, CCD at baseline (OR 24.8, 95% CI 7.3 to 84.5), male sex (OR 6.4, 95% CI 2.0 to 20.8), history of anterior uveitis (OR 4.4, 95% CI 1.3 to 14.5), higher ASDAS-CRP (OR 2.3, 95% CI 1.3 to 4.0), greater waist circumference (OR 1.3, 95% CI 1.1 to 1.6, per 5 cm), and medication with antiplatelets (OR 7.0, 95% CI 1.5 to 31.8) and beta-blockers (OR 3.4, 95% CI 1.0 to 11.5) were associated with a CCD at follow-up. Higher age and longer symptom duration were highly correlated and were both associated with a CCD at follow-up.
Conclusions The presence of CCD in AS is in part dynamic and associated with both AS and non-AS characteristics. Our results suggest that patients especially prone to present with CCDs are older men with a previous CCD, longer symptom duration, higher AS disease activity, a history of anterior uveitis and medication reflecting cardiovascular disease.
- ankylosing spondylitis
- spondyloarthritis
- cardiovascular disease
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Key messages
What is already known about this subject?
An association between ankylosing spondylitis (AS) and cardiac conduction disturbances (CCD) has been recognised for long, but contemporary longitudinal studies are scarce.
What does this study add?
In this longitudinal cohort study with ECG at baseline and at 5-year follow-up, we detected a CCD, mostly atrioventricular block of first degree, at least once in 18% of patients.
CCD varied between the recording occasions and was associated with both AS and non-AS characteristics: male sex, older age, longer symptom duration, a history of anterior uveitis, higher AS disease activity, greater waist circumference and medication reflecting cardiovascular disease.
How might this impact on clinical practice?
The study identifies a number of simple factors that can be used clinically to identify patients who are prone to present with a CCD with or without related symptoms.
Introduction
Ankylosing spondylitis (AS) is a rheumatic disease with mandatory involvement of the sacroiliac joints and spine, often enthesitis and peripheral arthritis, and a strong genetic link with human leukocyte antigen (HLA)-B27.1 2 Patients with AS may experience inflammation at locations outside of the musculoskeletal system, for instance the eyes and gut. Also, an association between AS and cardiac manifestations, such as conduction disturbances and aortic regurgitation, has been recognised for long, although the prevalence and severity have been debated.3–7
A few large register-based studies, all lacking individual AS characteristics of the included patients, show an increased risk of aortic valve disease, atrioventricular block (AVB) and pacemaker implantation in patients with AS compared with the general population.4 8 9 Else, the majority of previous studies of conduction disturbances or aortic regurgitation in AS are cross-sectional or historical cohort studies.3 10–19 It is not clear which, if any, AS characteristics may predispose to the presence of these cardiac manifestations. In addition, there is growing evidence for an increased risk of atherosclerotic cardiovascular disease (CVD) in AS.20
We have previously published cross-sectional results from an electrocardiographic (ECG) investigation.21 A 5-year follow-up study was also planned at that time with the aim to study (1) ECG development from baseline to 5-year follow-up, and (2) if cardiac conduction disturbance (CCD) at follow-up was associated with any AS and non-AS characteristics at baseline.
Methods
Patients
The enrolment process, inclusion and exclusion criteria, and study protocol have previously been described in detail.21 In short, 210 patients with AS fulfilling the modified New York criteria but without psoriasis, inflammatory bowel disease, malignancy, pregnancy, dementia or difficulties understanding Swedish were enrolled in 2009 and underwent physical examination by one investigator (EK).22 The physical examination included 66/68 swollen/tender joints index and Bath Ankylosing Spondylitis Metrology Index (BASMI). The patients also answered questionnaires regarding their medical history, smoking habits, current medication, Bath Ankylosing Spondylitis Disease Activity Index and Bath Ankylosing Spondylitis Functional Index (BASFI). For patients who reported known heart disease and/or medication against CVD, the medical records were further scrutinised for signs of ischaemic heart disease.
Body weight and height were measured, and blood sampling and recording of resting ECG were performed. Erythrocyte sedimentation rate (ESR) and C reactive protein (CRP) were analysed by standard laboratory techniques at the Department of Clinical Chemistry. HLA-B27 status was determined. AS Disease Activity Score based on CRP (ASDAS-CRP) was calculated and further categorised, where ASDAS-CRP <2.1 corresponded to an inactive disease or low disease activity and ASDAS-CRP ≥2.1 to a high or very high disease activity.23 24
The majority of patients were subsequently also examined with transthoracic echocardiography (n=187) to identify the presence of aortic regurgitation and with lateral spine radiographs (n=204) for grading of AS-related changes with modified Stoke Ankylosing Spondylitis Spinal Score (mSASSS).11 25
In 2014, 172 (82%) patients agreed to participate in the 5-year follow-up using the baseline protocol and were re-examined by one investigator (AD). The mean age (SD) of the patients was 55 (13) years and 93 (54%) were men.
Of the 38 patients (mean age at baseline of 50 (14) years, 74% men) not participating in the follow-up investigation, 5 patients had died, and the rest either declined to participate (n=26) or did not respond to the invitation (n=7). A CCD at baseline was noted in 8 of these 38 patients (21%), all men, of whom 3 had died during follow-up and 4 had an aortic regurgitation verified by echocardiography.
Electrocardiogram
Standard resting 12-lead ECG was recorded at a paper speed of 50 mm/s. In 2009 and 2014 the ECGs were first read by one of the investigators (HW and KB), respectively, and thereafter jointly with a cardiologist (LB), who were unaware of patient characteristics except for sex and age. In 2009, the PR, QRS and QT intervals were manually measured (HW). In 2014, these measures were obtained from the computerised analysis provided by the ECG machine (CARDIOVIT AT-2 Plus, Schiller).
CCD was defined as the presence of AVB of first to third degree (AVB I–III) and intraventricular conduction disturbances such as right (RBBB) or left (LBBB) bundle branch block, unspecified intraventricular conduction disturbance in the presence of a QRS interval ≥120 ms but without typical bundle branch block morphology, left anterior (LAFB) or left posterior fascicular block; in addition, pacemaker rhythm was included in this category. Two different cut-off intervals were used to define first-degree AVB: PR interval 200–219 ms (from here AVB Ix) and PR interval ≥220 ms (from here AVB I).
Statistics
Descriptive statistics are presented as number (percentage), mean (SD) or median (25th percentile (Q1), 75th percentile (Q3)). Related-samples Wilcoxon signed-rank test was used to compare ECG characteristics at baseline and follow-up. Univariate and age- and sex-adjusted logistic regression analyses were used to identify associations between baseline characteristics and present CCD at follow-up. The dependent variable was present CCD at follow-up (yes=1, no=0). Each respective baseline characteristic was included as independent variable in the univariate analyses. CRP was categorised as <5 and ≥5 mg/L, and body mass index (BMI) was categorised as <25 and ≥25 kg/m2. Due to skewness of distribution, log transformation of mSASSS +1 was used in the statistical comparisons. Dichotomous baseline characteristics with 10 or less positive observations were not analysed. Age and sex were included as independent variables in addition to each baseline characteristic in the age- and sex-adjusted models. Correlation between the independent variables (sex, age and respective baseline characteristics) was checked, and if Spearman’s rank correlation coefficient was high (ρ>0.6 or <−0.6) adjusted regression models were not done. The results of the logistic regression analyses are presented as OR with 95% CI. All tests were two-tailed and p<0.05 was considered statistically significant.
Statistical analyses were performed using PASW Statistics V.19.
Results
At follow-up, 23 patients (13.4%) had a CCD, 19 were men (20% of all men) and 4 were women (5% of all women). Five of them were ≤49 years at baseline (6% of all patients in this age group), and the remaining 18 patients were ≥50 years (22% in this age group). The characteristics of all 172 patients are described in table 1 stratified by sex and in online supplementary table 1 stratified by median age at baseline (49 years). All but one patient with CCD was HLA-B27-positive. Numerically, median ASDAS-CRP and Bath Ankylosing Spondylitis (BAS) indices were higher in patients with versus without CCD in both sexes. Likewise, ASDAS-CRP and BAS indices were higher in patients with versus without CCD ≥50 years of age, whereas this was not seen in the younger age group.
Supplemental material
Baseline characteristics of patients with AS with and without cardiac conduction disturbance at 5-year follow-up, stratified by sex
Electrocardiogram
ECG characteristics are described in table 2 stratified by sex and in online supplementary table 2 stratified by median age. While the majority had normal sinus rhythm, there were 16 exceptions at follow-up, 9 had sinus bradycardia, 2 each had sinus tachycardia and atrial fibrillation, and 3 had pacemaker rhythm. The PR interval increased significantly during follow-up in both sexes, while the QRS increased in men only.
ECG characteristics at baseline and at 5-year follow-up in patients with AS, stratified by sex
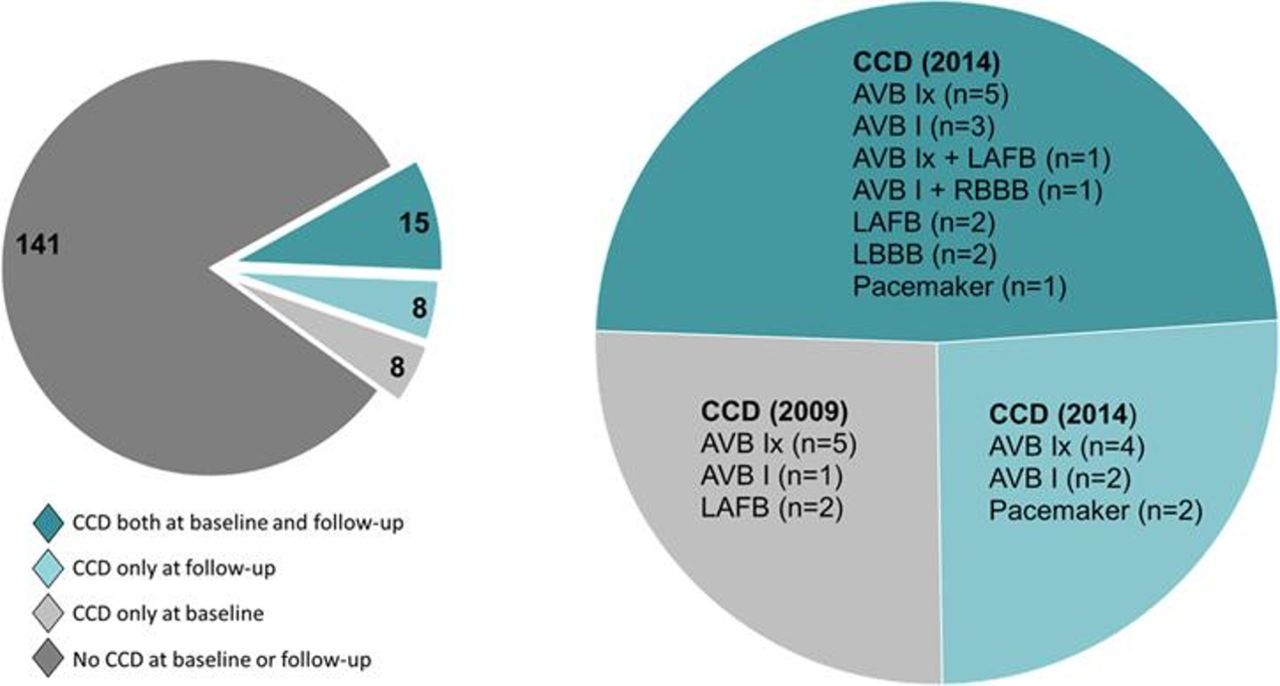
A description of subtypes of CCDs is presented in figure 1. In total, 31 patients (18.0%) had a detected CCD either at baseline or at follow-up. Individual characteristics of each of these 31 patients are listed in online supplementary table 3. The indications for the two implanted pacemakers during follow-up were sick sinus syndrome and AVB II during an acute myocardial infarction, respectively. The third patient had pacemaker implantation before baseline due to an AVB III; he also had a severe aortic regurgitation. Of the 15 patients with CCD both at baseline and at follow-up, 3 had developed a more advanced CCD (AVB Ix → AVB I, AVB Ix → LBBB, RBBB → AVB I combined with RBBB) and two had shorter PR interval (AVB I → AVB Ix) at follow-up.

{kind=link}
Description of the CCDs detected in the 172 patients with AS. The left pie chart presents the number of patients with a CCD or not at baseline and/or follow-up. The right pie chart describes the different CCDs. AS, ankylosing spondylitis; AVB, atrioventricular block; AVB I, PR interval ≥220 ms; AVB Ix, PR interval 200–219ms; CCD, cardiac conduction disturbance; LAFB, left anterior fascicular block; LBBB, left bundle branch block; RBBB, right bundle branch block.
Associations between baseline characteristics and CCD at follow-up
In the univariate logistic regression analyses (table 3), the strongest association was found for having a CCD already at baseline. Male sex and higher age, greater waist circumference and BMI ≥25 kg/m2 were also associated with a CCD at follow-up. AS characteristics at baseline associated with a CCD at follow-up were longer symptom duration, a history of anterior uveitis, presence of ≥1 syndesmophyte, higher mSASSS, ASDAS-CRP and BASFI, and for men also higher BASMI. Higher systolic blood pressure, reported hypertension and hyperlipidaemia, and medication reflecting CVD were also associated with a CCD at follow-up.
Logistic regression analyses for cardiac conduction disturbance at 5-year follow-up in 172 patients with AS
In the age- and sex-adjusted logistic regression analyses (table 3), the strongest association was again noted for having a CCD at baseline. A history of anterior uveitis and higher ASDAS-CRP at baseline were also associated with a CCD at follow-up. Additionally, male sex (adjusted for age only), greater waist circumference, and baseline medication with antiplatelets and beta-blockers were associated with a CCD at follow-up. Symptom duration and BASMI (in men) were highly correlated with age. These variables were therefore stratified by sex and not further age- and sex-adjusted.
Since a history of anterior uveitis can be related to the symptom duration, anterior uveitis was further adjusted for symptom duration and sex in an additional model with only a slight change of the point estimate (OR 4.1 vs 4.4). When analysing the separate components for ASDAS-CRP, back pain and patient global assessment of disease activity were significantly associated with a CCD, whereas the other components were not (data not shown).
Sensitivity analyses
Beta-blockers can slow atrioventricular (AV) conduction and cause a prolonged PR interval per se. At follow-up 24 of 172 patients were treated with orally administered beta-blockers. In a sensitivity logistic regression analysis, no significant association was found between current treatment with beta-blockers and a CCD at follow-up (age- and sex-adjusted OR 1.5, 95% CI 0.5 to 4.9). In a second sensitivity analysis the 3 patients with a lone AVB I(x) and current treatment with beta-blockers at follow-up were excluded from the logistic regression analyses. The main results were unchanged except that beta-blockers at baseline were no longer significantly associated with a CCD in the age- and sex-adjusted analysis.
Discussion
In this 5-year follow-up cohort study reinvestigating CCD in patients with AS, we found that 31 (18%) of the patients had a CCD, either at baseline or at 5-year follow-up. CCDs were found infrequently in women and in ages below 50 years. Characteristics of AS, such as a history of anterior uveitis and higher disease activity measured by ASDAS-CRP, were significantly associated with the presence of CCD at follow-up. Longer symptom duration, although highly correlated with age, was also associated with CCD at follow-up. Most CCDs were first-degree AVB, but 3 patients had a pacemaker and 2 had LBBB. The presence of CCD was partly dynamic in which 8 patients with initial first-degree AVB or LAFB had normalised their ECG at follow-up.
Prior studies of cardiac manifestations in AS have also looked for associations with patient characteristics, although most of them had a cross-sectional design. Dik et al14 found, in their cross-sectional study of ECG alteration in patients with AS, that age, disease duration and BMI were associated with the PR interval. Further, they found that male sex, disease duration and BASMI were associated with the QRS interval. Their patients were approximately 10 years younger than the patients in our cohort and anterior uveitis was not reported. In another cross-sectional study of 77 patients with AS, Lange et al18 found that patients with ECG abnormalities had significantly higher CRP and ESR than those without. This is in line with our finding of the association between ASDAS-CRP and CCD, although we did not observe any association specifically with CRP or ESR. Notably, our cross-sectional results from the baseline investigation did not reveal any association with markers of disease activity and CCD.21 A cross-sectional study from the 1980s specifically analysing AV conduction disturbances found that patients with AS and anterior uveitis had longer PR intervals than those without anterior uveitis.26 Three historical cohort studies showed that clinical presentation with peripheral arthritis was associated with a cardiac manifestation.7 12 13 Two of these studies had access to repeated ECGs and found that conduction disturbances could be intermittent and also resolve, in line with the present study. However, we could not detect a significant association with peripheral arthritis. On the other hand, active signs of peripheral joint disease at baseline were rare in our cohort.
HLA-B27 has been genetically linked to cardiac disease and anterior uveitis even in the absence of rheumatic disease.27–29 We could not detect any significant difference in HLA-B27 status between patients with and without a CCD, possibly explained by the overall high prevalence of HLA-B27. All except one of the patients with a CCD were HLA-B27-positive.
In line with the sex difference found in our study, a prior study demonstrated that men but not women with pacemaker-treated heart block had an increased frequency of HLA-B27 and associated rheumatic disorders.13 30 Likewise, we found an increased risk of AVB II-III in men but not in women with AS compared with the general population in a register-based Swedish cohort study.9
In the present study, also non-AS characteristics such as greater waist circumference and medication reflecting CVD, antiplatelets and beta-blockers, were associated with the presence of CCD at follow-up. Moreover, at least one of the CCDs, the pacemaker implantation due to an AVB II during an acute myocardial infarction, can be attributed to underlying ischaemic heart disease. Ischaemic heart disease is associated with several ECG findings, including AVB and intraventricular blocks.31 In addition, beta-blockers can per se slow AV conduction.
ECG findings and their prognostic values have been extensively studied in the general population. The PR interval is usually longer in men and increases with age and BMI.32–34 In agreement with our results, a prolonged PR interval and AVB can normalise and resolve, respectively, also in the general population.33 The risk with a prolonged PR interval and AVB I has been debated, but a recent meta-analysis suggested an increased risk of atrial fibrillation, heart failure and mortality.35 Additionally, an increased risk of pacemaker implantation has been demonstrated in persons with prolonged PR.36 37 Regarding intraventricular blocks, their frequency also increases with higher age, and RBBB, LAFB and prolonged QRS interval are more common in men than in women.31 32 38 LBBB may cause ventricular dyssynchrony and contribute to the development of heart failure.39 Both LBBB and RBBB are associated with an increased risk of future pacemaker implantation.40 41
Little is known concerning clinical implications of CCDs in AS. We have previously demonstrated a twofold increased risk of pacemaker implantation, a possible consequence of severe arrhythmia, in patients with AS.9 In another register-based study including patients with AS aged 65 years and older, Ward4 found only a slightly elevated risk of pacemaker implantation compared with controls without AS and therefore concluded there was no support for ECG screening in asymptomatic patients. Yet another study has investigated the usefulness of routine ECG for heart disease screening in patients with spondyloarthritis (SpA) and rheumatoid arthritis without known CVD or symptoms suggestive of CVD.42 The study found no statistical differences in ECG findings between the patients with SpA (n=108) and controls with non-inflammatory joint disease (n=74), and suggested that routinely obtaining ECG may be of limited usefulness in SpA. However, the study was cross-sectional without long-term data and did not account for the different age and sex distributions among the study populations. The present study has not been designed to address the multiple dimensions that exist with screening, and we can consequently not give any recommendations concerning screening with ECG in asymptomatic patients with AS.
We found an association between a history of anterior uveitis and CCD at follow-up. In line with our observation, it has been reported that the ciliary body and aortic valve have histological similarities to the enthesis. Furthermore, there is evidence supporting shared features and timing of inflammation in experimental models. HLA-B27/hβ2m-transgenic rats developed spontaneous inflammation in their hearts in addition to joints, gastrointestinal tract, eyes and skin.43 In another animal model, interleukin (IL)-23 stimulation of entheseal resident cells induced both enthesitis and aortic root and valve inflammation.44 In accordance, γ/δ T cells, suggested as key players in the pathogenesis of IL-23-induced inflammation, were found to be accumulated in the (Achilles tendon) enthesis, the aortic root and adjacent to the ciliary body in mice overexpressing IL-23.45 In an IL-23-independent animal model (TNF∆ARE) mechanical unloading was shown to prevent the development of enthesitis, and the authors concluded that mechanical strain induced entheseal inflammation.46 We therefore hypothesise that patients with AS who may be especially prone to develop CCD have a higher vulnerability to mechanical stress in both entheses, ciliary body and the heart.
Limitations
First, we were constrained by the low number of detected CCD and could therefore neither perform a multivariable model of associations between baseline characteristics and a CCD at follow-up nor check extensively for possible interactions. The age-stratified patient characteristics at baseline indicated that the observed association with ASDAS-CRP might be restricted to older patients. Second, since only few cases with CCD were found in ages below 50 years at baseline, our findings may not be applicable to this age group. Third, enthesitis was not assessed due to the difficulties in evaluating enthesitis clinically. Fourth, since we show that CCDs can fluctuate in AS, repeated ECG during follow-up could have added valuable information. Fifth, the study lacked age-matched and sex-matched controls without AS. Another limitation linked to the longitudinal cohort study design is the dropout of patients during follow-up. Thirty-eight of the initial 210 patients (18%) did not participate in the follow-up and 21% of these had a CCD at baseline. Last, since the ECG from 2009 and 2014 used different methods to gain the specific ECG measurements (manually and ECG provided, respectively), we cannot categorically exclude a variation in intervals related to the two methods.
Strengths
First, the cohort of patients with AS is well defined, with the diagnosis set by a rheumatologist and all the included patients fulfilled the modified New York criteria. Second, the patients are thoroughly described both regarding AS-specific as well as cardiac characteristics. Third, to our knowledge, the present study is the first contemporary follow-up investigation of CCD in patients with AS and therefore reduce the gap of knowledge in the field.
Conclusions
To conclude, the results of this longitudinal study suggest that in addition to higher age/longer symptom duration and male sex, both AS characteristics (anterior uveitis and higher disease activity) as well as markers of CVD are associated with the presence of CCD in patients with AS.
References
Footnotes
Presented at Preliminary results have been presented as abstract/poster at EULAR in Amsterdam in 2018, at the 11th International Congress on Spondyloarthritides in Gent in 2018, and at the Swedish Rheumatology Meeting in Uppsala in 2018.
Contributors KB contributed to the data acquisition of the ECG characteristics at follow-up, analysis and interpretation of data, and drafting the first version of the manuscript. EK and AD recruited patients to the study and performed examinations and data acquisition at baseline and follow-up, respectively. HW contributed to the data acquisition of the ECG characteristics at baseline. LB contributed to the data acquisition of the ECG characteristics and interpretation of data. LJ contributed to the interpretation of data. HFdE conceived the study and contributed to the design of the study, acquisition and interpretation of data. EK, AD, HW, LB, LJ and HFdE revised the first version of the manuscript critically and participated in the editing until its final version. All authors agreed to be accountable for all aspects of the work and have read and approved the final manuscript.
Funding This study was supported by grants from the Health and Medical Care Executive Board of the Västra Götaland, Rune and Ulla Amlövs Foundation for Rheumatology Research, Göteborg’s Association Against Rheumatism, Swedish Rheumatism Association, Swedish Society of Medicine, Göteborg Medical Society, the Swedish state under the agreement between the Swedish government and the county councils, the ALF agreement (ALFGBG-141111, ALFGBG-430851, ALFGBG-678731), Controlling Chronic Inflammatory Diseases with Combined Efforts (COMBINE), and the Margareta Rheuma research foundation.
Competing interests LJ has received advisory board fees from Eli Lilly, Pfizer and Novartis. HFdE has received advisory board fees from Sandoz, AbbVie and Novartis, and unrestricted grant from Novartis.
Patient and public involvement statement One trained patient research partner from the Swedish Rheumatism Association participated in the planning of the study and contributed with comments on the study protocol and the written information to the patients.
Patient consent for publication Not required.
Ethics approval The study was approved by the Regional Ethics Committee, Gothenburg, Sweden, and carried out in compliance with the Helsinki Declaration. All patients gave their written informed consent to participate both at baseline and at follow-up.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement The data sets generated and/or analysed during the present study are not publicly available due to the General Data Protection Regulation, but at limited and fully anonymised data set that support the main analyses is available upon reasonable request.