Article Text

Abstract
Objective To evaluate current evidence on the efficacy and safety of topical and systemic medications in patients with primary Sjögren syndrome (SjS) to inform European League Against Rheumatism treatment recommendations.
Methods The MEDLINE, EMBASE and Cochrane databases were searched for case-control/prospective cohort studies, randomised controlled trials (RCTs) and systematic reviews.
Results Current evidence in primary SjS patients fulfilling the 2002 criteria is based on the data from 9 RCTs, 18 prospective cohort studies and 5 case-control studies. Two Cochrane systematic literature reviews (SLRs) have reported that topical treatments for dry mouth and dry eye are safe and effective. Ocular cyclosporine A was safe and effective in two RCTs including 1039 patients with dry eye syndrome. Two Cochrane SLRs on serum tear drops and plugs showed inconsistency in possible benefits, both for symptoms and objective measures. Five RCTs reported significant improvements in oral dryness and salivary flow rates for pilocarpine and cevimeline. An RCT showed no significant placebo-differences for hydroxychloroquine 400 mg/day for the primary outcome (visual analogue scale (VAS) composite of dryness, fatigue and pain). We identified seven RCTs carried out in primary SjS patients. RCTs using infliximab, anakinra and baminercept found no placebo-differences for the primary outcomes. The two largest RCTs randomised 255 patients to receive rituximab or placebo and reported no significant results in the primary outcome (VAS composite), while prospective studies suggested efficacy in systemic disease.
Conclusion The current evidence supporting the use of the main topical therapeutic options of primary SjS is solid, while limited data from RCTs are available to guide systemic therapies.
- Sjøgren's syndrome
- treatment
- multidisciplinary team-care
This is an open access article distributed in accordance with the Creative Commons Attribution 4.0 Unported (CC BY 4.0) license, which permits others to copy, redistribute, remix, transform and build upon this work for any purpose, provided the original work is properly cited, a link to the licence is given, and indication of whether changes were made. See: https://creativecommons.org/licenses/by/4.0/.
Statistics from Altmetric.com
Key messages
What is already known about this subject?
EULAR has issued the 2019 recommendations for the management of Sjögren syndrome.
What does this study add?
The current evidence supporting the efficacy and safety of the main topical therapeutic options for the treatment of the sicca symptoms of primary Sjögren’s syndrome (SjS) is solid.
There is no information on the differential efficacy and safety of the main systemic therapeutic options available.
Limited data are available from controlled trials to guide systemic treatment
How might this impact on clinical practice?
This systematic literature review informed the task force for the ‘EULAR recommendations for the management of Sjögren syndrome’ that will help guide practice for physicians from several medical specialties involved in the management of the disease.
Introduction
Sjögren’s syndrome (SjS), a chronic, systemic autoimmune disease, has no cure. Although it was identified as a disease more than a century ago,1 the therapeutic management has not changed significantly in recent decades.2 The specific pathogenic basis of a disease that targets the exocrine glands has led to a very specific type of therapy (agents locally applied to the mucosal surfaces involved) as one of the key approaches. In contrast, the systemic element of SjS has traditionally been tackled using glucocorticoids (GCs) and immunosuppressive agents, due to their use in similar systemic diseases such as systemic lupus erythematosus or vasculitis.
During the first decade of this century, Food and Drug Administration (FDA) approval of muscarinic agents and topical cyclosporine A (CyA) for oral and ocular dryness in SjS patients, respectively, and the first studies testing biological agents were considered the first signs of a new, game-changing therapeutic scenario for primary SjS patients. Despite this, the first specific systematic literature review (SLR) of SjS therapy, published in 2010, found that evidence remained very limited, without solid results that could change the disease management.3 Since 2010, there have been significant advances, including the accurate characterisation and scoring of the disease burden,4 5 the patient-centred therapeutic response6 and the publication of large, well-designed therapeutic studies.7
The aim of this review was to inform the new EULAR recommendations on the current state of evidence on the efficacy and safety of the main topical and systemic therapies used in SjS.
Methods
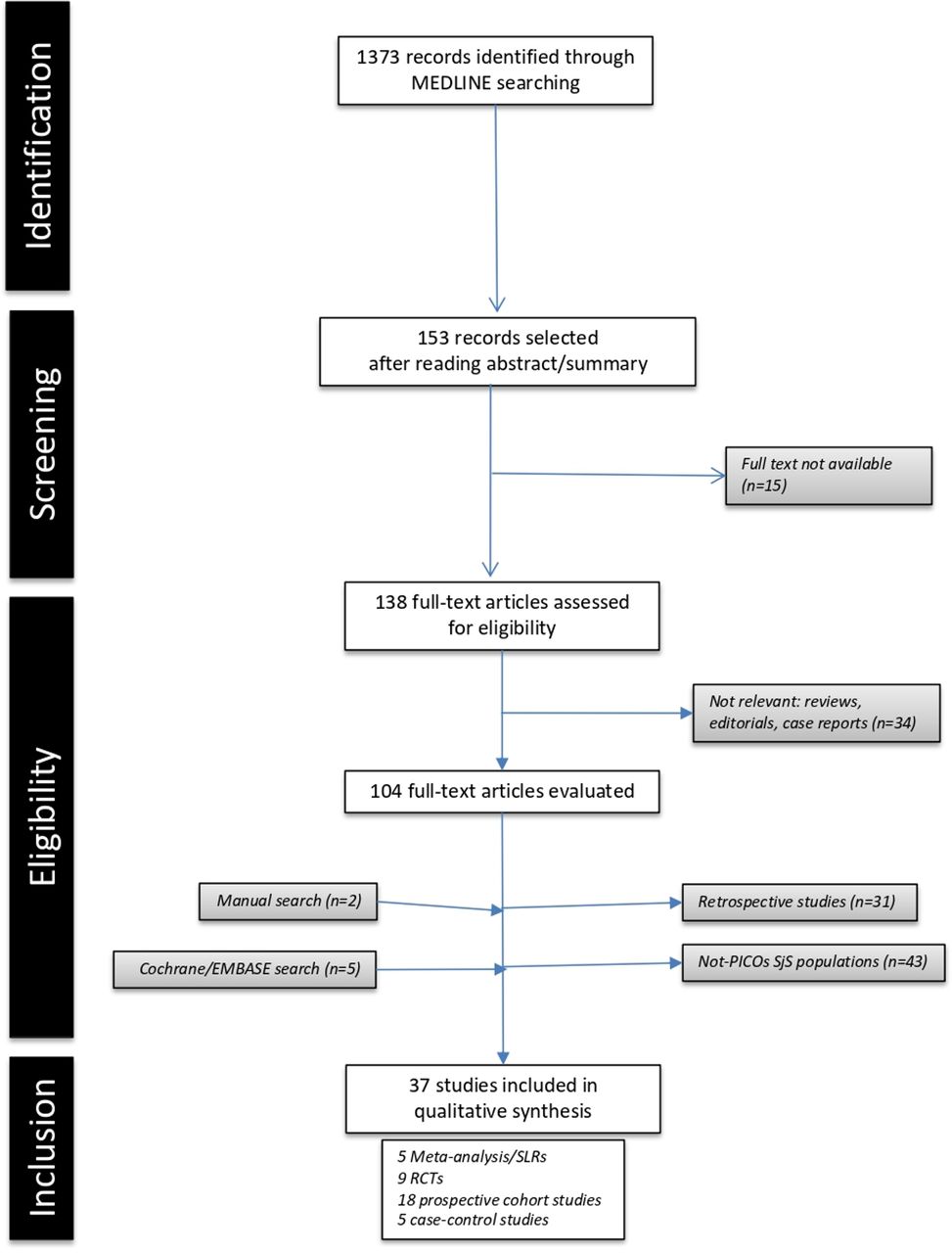
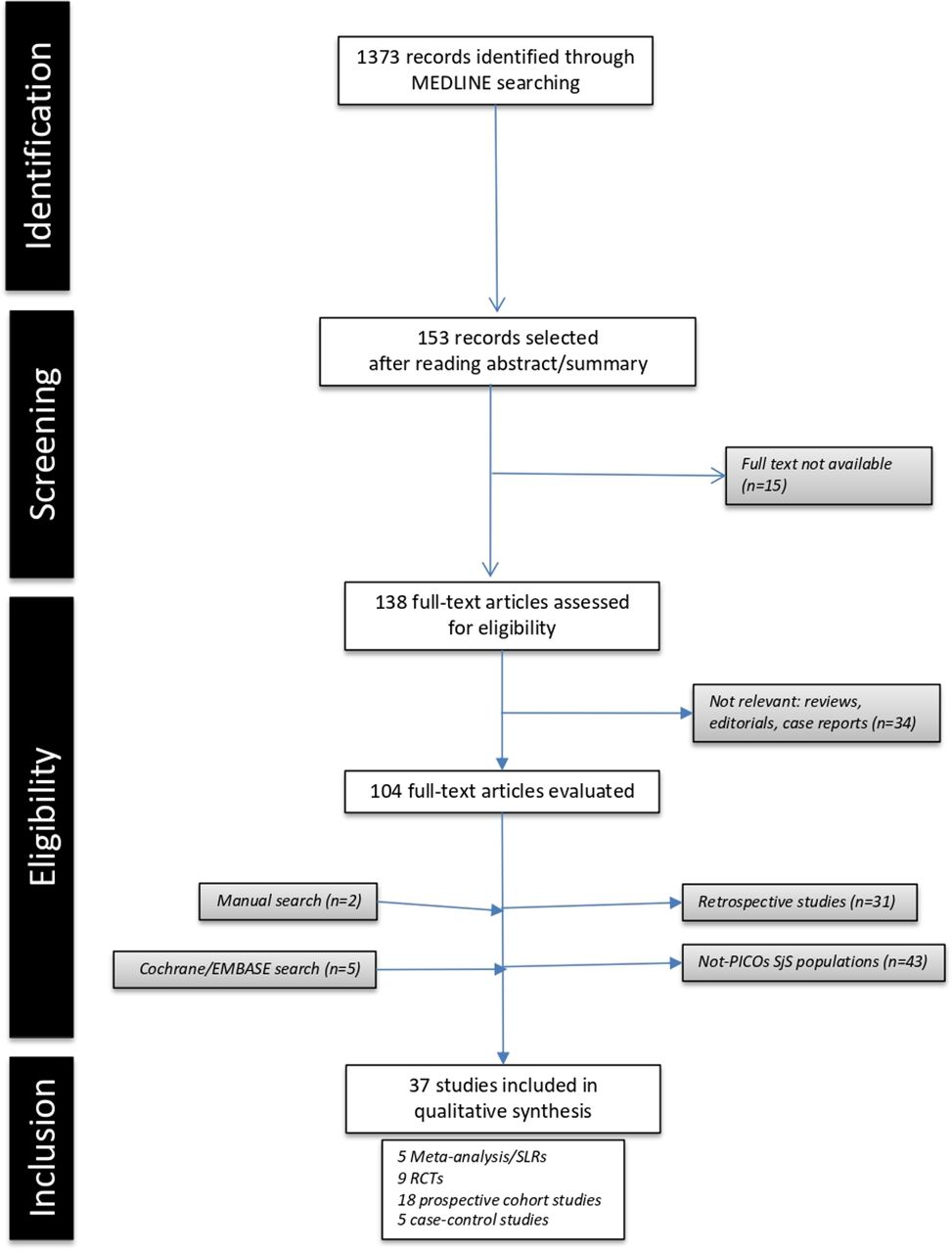
A MEDLINE SLR was carried out by PB-Z and SR using the MeSH term ‘Sjögren’s syndrome’ combined with each therapeutic intervention proposed by the Task Force (see ‘Intervention’ section of the Population, Intervention, Comparison, Outcomes and Study design (PICOS) strategy) with the following restrictions: date (1 January 1986 to 31 December 2017), studies (humans) and age (adults). Additional databases, such as EMBASE and Cochrane Central Library, were also checked. The SLR strategy followed prespecific PICOS definitions agreed by the Steering Committee members: (a) Population: in order to collect evidence from an aetiopathogenically homogeneous population, data was retrieved from studies including adult primary SjS patients fulfilling the 2002 criteria (stated in the manuscript as ‘primary-2002’ patients) or the 2016 ACR/EULAR criteria8 9; (b) Intervention: using the data from a 2010 SLR as a starting point,6 10 interventions were classified as topical or systemic medications; (c) Comparison: therapeutic interventions were compared with placebo (PLA) or other therapeutic interventions; (d) Outcomes: eligible studies had to contain sufficient, clear information on the effect of the therapeutic intervention (efficacy) and on the safety profile; (e) Study design: we included randomised controlled trials (RCTs), cohort studies (prospective non-PLA-controlled, non-randomised studies and those with quasi-experimental designs), case-control studies (comparing therapeutic options) and meta-analyses, according to the definitions proposed by the Oxford Centre for Evidence-Based Medicine (CEBM),11 while case series (descriptive/retrospective therapeutic studies) were considered in the absence of other studies; narrative reviews, experimental animal studies, duplicate publications and isolated case reports were excluded. In the absence of evidence on the target population, extrapolation of results from studies including SjS populations that differed from the definition in the PICOS strategy was allowed. Figure 1 summarises the SLR results. Summary-of-finding tables were generated for RCTs (table 1),10 12–19 prospective cohort studies (table 2)20–37 and case-control studies (table 3).38–42 For RCTs, the risk of bias (RoB) was assessed using the Cochrane RoB assessment tool (Cochrane Handbook for Systematic Reviews of Interventions V.5.1.0 March 2011 (available from: http://handbook.cochrane.org/)), and for uncontrolled studies, we used the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement checklist. The few RCTs available for each therapeutic intervention, together with the heterogeneity in the methodology of the studies included, such as differing participant characteristics, comparative interventions, the small size of the populations studied and the differences in follow-up intervals and outcomes measured, make it impossible to pool data in a meta-analysis.
Summary-of-findings table generated for RCTs in primary-2002 patients with Sjögren syndrome
Summary-of-findings table generated for prospective studies in primary-2002 patients with Sjögren syndrome
Summary-of-findings table generated for case-control studies in primary-2002 patients with Sjögren syndrome
{kind=link}
Flow chart of the systematic literature review. PICOs, Population, Intervention, Comparison, Outcomes and Study design; RCTs, randomised controlled trials; SjS, Sjögren’s syndrome; SLRs, systematic literature reviews.
Results
Oral topical therapies
Saliva substitutes
We identified five studies that evaluated gels/saliva substitutes in SjS patients, of which only one was carried in primary-2002 patients38: Alpöz et al found that Xialine (a saliva substitute containing polysaccharide xanthan gum plus sodium fluoride) and plain water plus diluted tea (serving as PLA) were equally effective in most VAS scoring for specific oral symptoms, with the only between-group differences being an increased preference for Xialine at the end of the study (p=0.011). A Cochrane SLR evaluated the effectiveness of topical treatments for any-cause dry mouth (including SjS) in parallel and crossover RCTs using lozenges, sprays, mouth rinses, gels, oils, chewing gum and/or toothpastes and found no strong evidence supporting any one specific topical therapy as more effective in treating dry mouth.43
Interferon alpha
Three studies have evaluated the use of interferon alpha per the oromucosal route in SjS patients fulfilling the 1993 criteria, including a large RCT of nearly 500 patients that found significant improvement only in unstimulated salivary flow (uSF), with a higher percentage of gastrointestinal adverse events in comparison with PLA.3
Ocular topical therapies
Artificial tear drops
Seven studies testing artificial tears (ATs) in patients with SjS were identified, all of which found significant improvements with respect to baseline in both VAS ocular dryness and diagnostic tests (except in one study) with no reported side effects.3 Only one study,39 comparing the use of AT with plug insertion, was carried out in primary-2002 patients: no significant between-group differences were reported and, after 8 weeks of treatment, patients treated with AT showed significant improvement in all ocular diagnostic tests performed (p<0.001). A recent Cochrane review of AT drops for dry eye syndrome concluded that ATs are safe and effective.44
Non-steroidal anti-inflammatory drugs/GC-based tear drops
Evidence is overwhelmingly limited to studies including patients with associated SjS or non-2002 SjS patients. Only one study40 was carried out in primary-2002 patients, and this compared topical 0.1% fluorometholone (FML) with topical CyA: although no significant differences were detected between groups for the main efficacy parameters (except for tear breakup time (BUT), with better results in the FML group), although patients treated with topical 0.1% FML showed significant improvements with respect to baseline in the Corneal Fluorescein Staining score (p<0.001), BUT (p<0.001) and Ocular Surface Disease Index (p<0.001) after 8 weeks of therapy, but not for the Schirmer test; no serious side effects were reported: the mean intraocular pressure change at 8 weeks was +0.4 mm Hg in the FML group versus −1.15 mm Hg in the CyA group (p=0.389).
Cyclosporine-based tear drops
In December 2002, an ophthalmic formulation containing 0.05% CyA was approved by the US FDA to treat dry eye disease at a recommended two times per day dose, based on the results of two RCTs that included 1039 patients with keratoconjunctivitis sicca (SjS patients were included in varying proportions).3 Since then, a summary of the results reported until now shows that most studies only demonstrated within-group improvements, and those that reported significant between-group differences (drug and vehicle) found improvement in only one to two of the four to eight ocular outcomes evaluated.45 In addition, a study extension trial found no additional improvement in subjective and objective measurements after 6 months of therapy.46 With respect to adverse events, the largest RCT47 found that most events were mild-to-moderate and transient, with a significantly higher percentage of burning eye in comparison with PLA (15% vs 6% in PLA), and only 2% of patients discontinued because of burning and stinging.3
There are no specific RCTs in primary-2002 patients, with only one case-control study, the above-mentioned study by Lin and Gong,40 which showed no significant differences with topical 0.1% FML and with a higher frequency of moderate-to-severe transient burning sensation in patients receiving CyA.
Tacrolimus-based tear drops
A recent small RCT using 0.03% tacrolimus tear drops in 24 SjS 2002 patients found significant improvements in the Schirmer test and corneal staining (fluorescein, rose Bengal) after 3 months of therapy in comparison with drops that included only the vehicle. Nearly 80% of those receiving tacrolimus experienced a burning sensation after instillation.48
Serum tear drops
Autologous serum (AS) has been tested in six small (<30 patients) uncontrolled studies in SjS patients and has shown inconsistent benefits (improvement in some but not all ocular tests performed).49 Only one study was carried out in primary-2002 patients, which showed a significant improvement with respect to baseline in three out of five ocular outcomes.41 A recent Cochrane review of AS for dry eye syndrome49 confirmed inconsistency in the possible benefits of AS for both symptoms and objective measures, with no evidence of an effect after 2 weeks of treatment.
Insertion of lachrymal plugs
Of the nine studies identified in SjS patients, only two were carried out in p2002-SjS patients. Qiu et al39 compared the insertion of plugs with ATs in 40 patients: both treatments improved all ocular outcomes (subjective and objective) without statistically significant between-group differences. In a prospective study, Egrilmez et al20 reported improvement in two out of four ocular tests with respect to baseline 12 months after inserting plugs. A recent Cochrane SLR reviewed the use of plugs for dry eye syndrome50 and found that the evidence was very limited and improvements in symptoms and ocular tests were inconclusive.
Diquafosol
In 2004, an ophthalmic formulation of diquafosol (an agonist of the purinergic P2Y receptor) was tested by Tauber et al51 in an RCT including 527 patients with dry eye (only 76 had SjS), which reported statistically significant differences between groups in only one of the two defined primary outcomes, with no further studies being reported, making it impossible to recommend their use.
Oral muscarinic agonists
Two muscarinic agonists (pilocarpine and cevimeline) were licensed by the FDA in 1998 and 2000, respectively, for the treatment of oral dryness in SjS patients; these agents stimulate the M1 and M3 receptors present on salivary glands, leading to increased secretory function.
Pilocarpine
The two pivotal RCTs included 629 SjS patients (fulfilling the 1993 criteria and including both primary and associated cases) and found significant improvements in oral dryness VAS and salivary flow rates at doses of 5 and 7.5 mg/6 hours in comparison with the PLA arm.3 The RCTs showed a high frequency of adverse events, including sweating (43%), increased urinary frequency (10%) and flushing (10%). In a dose-escalating RCT, nearly a quarter of patients reduced from 7.5 to 5 mg/6 hours in a second 6-week period of therapy. Only two studies have been carried out in primary-2002 patients, and only one assessed efficacy. In a prospective study, Aragona et al21 reported a significant improvement with respect to baseline in oral dryness VAS (p<0.001) after 2 months of therapy with pilocarpine 5 mg/6 hours.
Cevimeline
Three RCTs including 332 SjS patients (fulfilling the 1993/Japanese criteria, both primary and associated cases) tested the use of cevimeline using dosages ranging between 15 and 60 mg/8 hours. The best results were achieved with a dose of 30 mg/8 hours, including significant improvements in dry mouth and salivary flow rates, with a significantly higher frequency of nausea (relative risk 1.68) and sweating (relative risk 2.16) in comparison with PLA.3 There is only one study carried out in primary-2002 patients, but there was no information detailed about overall efficacy and safety.30 Only one study has compared cevimeline with pilocarpine but only assessed the safety profile. Noaiseh et al42 retrospectively analysed 118 primary-2002 patients and found a lower failure rate of cevimeline both in first-time (27% vs 47%, p=0.02) and all (32% vs 61%, p<0.001) users in comparison with pilocarpine. Severe sweating was the main reason for therapy cessation and occurred more frequently in pilocarpine users (25% vs 11%, p=0.02).
Hydroxychloroquine
We identified 12 studies that assessed hydroxychloroquine in SjS patients, with only 4 (2 prospective and 2 RCTs) carried out in primary-2002 patients. Yavuz et al31 prospectively enrolled 32 patients treated with hydroxychloroquine for at least 2 years (no data on mean length or cumulative dose) and reported, in a further 12-week control study, a significant improvement in four out of eight ocular outcomes with respect to baseline, with no information on concomitant ocular therapies. Çankaya et al32 prospectively evaluated 30 women who started on 400 mg/day of hydroxychloroquine and reported a significant improvement in uSF rate (0.212 vs 0.162 baseline, p<0.05) but not stimulated salivary flow rate at 30 weeks, with improvement in only two of the five subjective oral VAS scores. Yoon et al17 carried out a small RCT in 26 patients and found no significant differences in dry eye in comparison with PLA, but with no definition of the primary outcome.17 The pivotal RCT was carried out by Gottenberg et al16 in 120 patients with primary-2002 SjS who were randomised to receive 400 mg/day of hydroxychloroquine (n=56) or PLA (n=64): the primary outcome was defined as a ≥30% reduction in two out of three VAS scores—dryness, fatigue, pain—without significant PLA differences at week 24 (17.6% vs 17.3%, p=0.96). For one of the secondary outcomes, hydroxychloroquine was associated with a statistical trend to improved pain (p values between 0.06 and 0.10 at 12, 24 and 48 weeks) although it was not superior to PLA for articular involvement; with respect to fatigue, no statistical differences were found.16 No cases of retinal toxicity or severe adverse events were reported in any of these studies.
Oral GCs
The frequent use of GCs in clinical practice in primary SjS patients is not supported by reliable scientific evidence. In the absence of controlled studies in 2002 patients, we briefly analysed the data in other SjS populations.3 The first study was a very small RCT (eight patients per arm) comparing prednisone 30 mg/day with piroxicam 20 mg/day and PLA, which found significant differences in subjective symptoms but not in objective tests.52 However, a prospective study of 60 patients followed for a mean of nearly 4 years found that corticosteroids did not influence the progressive decrease in salivary flow rates.53 No controlled studies are published in primary-2002 patients, and only retrospective studies have reported the use of GCs for systemic disease,54 with a high rate of GC-related adverse events, including increased appetite and weight gain,52 a two-fold higher frequency of diabetes mellitus55 56 and Cushing in up to 80% of patients.56
Immunosuppressive agents
Seven studies have tested immunosuppressive agents in SjS patients (two studies using leflunomide and cyclophosphamide, respectively, and one study each for azathioprine, methotrexate and mycophenolate), of which only two were carried out in primary-2002 patients. van Woerkom et al27 carried out a prospective study using 20 mg/day of leflunomide, which showed significant improvement in 5 out of 16 efficacy parameters tested after 24 weeks of therapy (2 were components of quality of life (QoL) questionnaires and 3 analytical parameters); all 15 patients experienced adverse events (between 4 and 8 per patient), principally gastrointestinal (67%), cytopenia (47%) and lupus-like cutaneous lesions (33%). Willeke et al28 tested the use of micophenolic acid 1440 mg/day, reporting significant improvement in 8 out of 16 efficacy parameters after 24 weeks of therapy, including VAS for sicca features (p<0.02) and mean AT use (p<0.02) (other parameters that improved included components of QoL questionnaires and analytical parameters); adverse events were reported in 72% of patients.
Biological therapies
Of the 34 studies in which biological agents have been tested in SjS patients, we identified 6 RCTs (using infliximab (INF), anakinra and rituximab) and 10 prospective cohort studies (using etanercept, abatacept, epratuzumab, rituximab and belimumab) carried out in primary-2002 patients. A summary of the results of the efficacy parameters is provided in table 4.
Summary of the outcomes evaluated in RCTs including primary-2002 patients with Sjögren syndrome
Abatacept
Two small prospective cohort studies have tested abatacept in primary-2002 patients. The first enrolled 15 patients with early active disease who received eight intravenous abatacept infusions24 and reported that ESSDAI, EULAR Sjogren’s Syndrome Patient Reported Index (ESSPRI), rheumatoid factor and IgG levels decreased significantly at 48 weeks; fatigue and health-related quality of life parameters improved significantly, while salivary and lacrimal gland function did not change; 6 (40%) patients experienced mild acute adverse events and 10 (67%) self-reported infections. The second study included 11 patients and reported increased saliva production (1.74 vs 1.61 g/2 min baseline, p=0.029) after 24 weeks of therapy and decreased lymphocytic foci in total (but not lymphocytic foci per mm2); one patient developed lupus-like cutaneous lesions.25
Anakinra
A small RCT that randomised 26 patients (13 to anakinra and 13 to PLA) found no significant reduction in fatigue in the primary endpoint14 (comparison of fatigue scores at week 4, p=0.19); 2 patients experienced severe side effects (injection site reaction and gastroenteritis, respectively), 2 had a transient episode of neutropenia and 7 (54%) mild injection site reactions.
Baminercept
St Clair et al18 have recently reported on the clinical efficacy and safety of baminercept in 52 patients with primary-2002 randomised in a 2:1 ratio to receive subcutaneous injections of 100 mg of baminercept every week for 24 weeks or matching PLA. The primary end point was the change between screening and week 24 in the stimulated whole salivary flow (SWSF) rate. The change from baseline to week 24 in the SWSF rate did not differ significantly between the baminercept and the PLA groups (baseline-adjusted mean change −0.01 vs 0.07 mL/min; p=0.332). Baminercept was associated with a higher incidence of liver toxicity, including two serious adverse events.
Belimumab
The results reported by the Efficacy and Safety of Belimumab in Subjects with Primary Sjögren’s Syndrome (BELISS) open-label trial57 in 30 primary-2002 patients (all with systemic complications, early disease and/or abnormal biomarkers) showed that belimumab 10 mg/kg (weeks 0, 2 and 4, and then every 4 weeks until week 24) was associated with a higher rate of improvement in the composite outcome (improvement of at least two of the five following items: ≥30% reduction in VAS for dryness, fatigue, musculoskeletal pain and physician systemic activity, and ≥25% reduction in any of the B-cell activation biomarkers) in patients with early disease in comparison with those with systemic disease (73% vs 47%); the mean ESSDAI score decreased from 8.8 to 5.59 (p<0.0001) and the ESSPRI score from 6.44 to 5.56 (p=0.01). In the 19 patients who completed 1 year of treatment, a significant improvement in some ESSDAI involvements (glandular, lymphadenopathy and articular) was maintained.22 With respect to the safety profile, only one serious adverse event was reported (pneumococcal meningitis) after six drug infusions.
Epratuzumab
In 2006, a small prospective study including 15 patients with primary-2002 SjS23 reported a beneficial effect on VAS fatigue (<0.05), patient assessment (<0.05), physician assessment (<0.05) and tender joints (<0.05); five patients experienced severe adverse events (acute infusion reactions and infections).
Etanercept
Two studies (one RCT, one prospective) have been carried out in SjS patients; only the prospective study included primary-2002 patients and showed no significant improvements in the main sicca signs and symptoms.29
Infliximab
A prospective open-label study in 16 patients found significant improvements in subjective and objective measures after the administration of INF, although recently the authors have retracted the manuscript.58 In 2004, Mariette et al12 conducted an RCT including 103 patients and found no significant differences in the primary outcome, defined as improvement in at least 30% of the joint pain, fatigue and dryness VAS at 22 weeks (INF 20.4% vs PLA 16.7%, p=0.62) or in the majority of secondary outcomes (symptoms, salivary flow rates, ocular tests, QoL and salivary biopsy), with improvement only in fatigue and some analytical parameters in comparison with PLA.
Rituximab
Rituximab has been tested in three prospective cohort studies,33–35 one case-control study36 and four RCTs.10 13 15 19 A summary of the significant improvements reported with respect to baseline in the prospective cohort studies showed improvement in VAS for dryness,34 36 fatigue34–36 and pain/tender point count,34 while no significant improvements were reported for objective oral and ocular tests (except in the study by Pijpe et al33 in a subset of patients). In the case-control study, Carubbi et al36 compared the therapeutic effect of rituximab (n=22) and conventional immunosuppressive therapy (n=19) and found a significant improvement in patients treated with rituximab in the ESSDAI (<0.05), global VAS (<0.05), fatigue VAS (<0.01), dryness VAS (<0.01), physician VAS (<0.05), uSF (<0.01) and Schirmer test (<0.05) at the end of follow-up (120 weeks); the authors reported a complete lack of reported adverse events in either of the two arms in spite of the long-term nature of the study. With respect to the two small RCTs, Dass et al13 randomised 17 primary-2002 patients to receive rituximab (n=8) or PLA (n=9) and found no significant results in the primary outcome (improvement >20% VAS fatigue at 6 months, rituximab 87% vs PLA 56%, p=0.36), while Meijer et al10 randomised 30 primary-2002 patients to receive rituximab (n=20) or PLA (n=10) with no significant results for the primary outcome (improvement in SWSF rate at 48 weeks, p>0.05). Two large RCTs have recently been reported. In 2014, Devauchelle-Pensec et al15 randomised 122 primary-2002 patients to receive rituximab (n=63) or PLA (n=57) and found no significant results in the primary outcome (≥30 mm improvement at week 24 on at least 2 out of 4 VAS scores—dryness, fatigue, pain, global, 23% vs 22%, p=0.91), while Bowman et al19 randomised 133 primary-2002 patients to receive rituximab (n=67) or PLA (n=66) and found no significant results in the primary outcome (reduction ≥30% at week 48 in either fatigue or oral dryness VAS, rituximab 39.3% vs PLA 36.8%, p=0.76). Two recent meta-analyses including the four RCTs have confirmed the lack of significant between-group differences in mean improvements between baseline and week 24 values for fatigue VAS, oral dryness VAS, salivary flow rate and Schirmer test, and no significant difference between groups for the main adverse events.59 60
Discussion
Current evidence on the therapeutic management of primary-2002 SjS patients is based on 9 RCTs (only four including ≥100 patients randomised to drug/PLA), 18 prospective cohort studies (all including ≤30 patients per study) and 5 case-control studies.
For oral topical therapies, available evidence is limited to five studies carried out in SjS patients (only one in primary-2002 patients) and one Cochrane SLR that assessed the management of dry mouth. Xerostomia is a subjective symptom with wide interindividual variation, and a satisfactory output of unstimulated whole saliva in one patient may lead another to complain of symptoms of dry mouth. All studies have shown significant within-group improvement in comparison with baseline subjective oral outcomes. Mechanical stimulation (chewing gum) was associated with increased saliva production in patients with residual capacity, but there is no evidence that gum may have more or less efficacy than saliva substitutes in reducing dry mouth symptoms. Due to the wide range of interventions, small trials (mean of 45 participants per trial), the RoB and the range of outcome measures for oral dryness, there is no strong evidence to support any specific intervention over another, and the conclusion is that, in the absence of an effective topical treatment, we recommend that the treatment of xerostomia should be directed towards improving patients’ complaints rather than increasing saliva production, including improvements in tooth health and the prevention of oral infections. The cost of long-term topical therapy is another important consideration, but there are no available studies on this issue. Other therapeutic interventions are under investigation. A recent double-blind, crossover-design study has evaluated the effects of intraoral electrostimulation,61 and further studies in primary-2002 patients are required to make a specific recommendation on its use.
For ocular topical therapies, among the 43 studies in SjS patients, only 6 (14%) were carried out in primary-2002 patients, while there are 4 SLRs on the management of dry eye using ATs, AS and plugs.44 49 50 62 The Cochrane SLR on AT showed that the AT formulations tested improved the signs and symptoms over the course of the studies included, although they found no consistent between-group differences when conducting head-to-head AT comparisons. The authors concluded that, given the large number of AT formulations compared and the wide variety of outcomes, it was difficult to propose that one over the counter AT formulation is superior to another for the treatment of dry eye syndrome. However, AT consistently improved ocular symptoms over the course of the trials included, based on within-group analyses, and three of four PLA-controlled trials consistently found that AT improved ocular symptoms compared with PLA (saline or vehicle), with a similar trend for many of the secondary outcomes. This review also found that the use of ATs is relatively safe, with the most common adverse events being blurred vision, ocular discomfort and foreign body sensation. It is important to consider that most outcomes were subjective measures of patient-reported outcomes rather than objective outcomes.44 With respect to non-steroidal anti-inflammatory drug (NSAID)/GC-based ocular tears, evidence not including primary-2002 SjS patients suggests careful use of tears containing NSAIDs or GCs due to the side effects associated with prolonged use.63 In these patients, ocular topical NSAIDs or corticosteroids may be a short-term therapeutic approach prescribed by ophthalmologists for the minimum time necessary (maximum 2–4 weeks).63
With respect to topical CyA, the pivotal study (a combination of two trials including 877 patients—270 fulfilled the 1993 SjS criteria, not detailed how many were primary or associated) evaluated 14 efficacy outcomes (4 objective, 10 subjective) with no definition of which were primary or secondary and found statistically significant differences between groups only in 4 (2 subjective and 2 objective). In spite of this, the FDA approved their use. In addition, a review of the results of all reported studies shows that most studies only demonstrated within-group improvements, and those that reported significant between-group differences (drug and vehicle) found improvement in only 20%–30% of the outcomes evaluated.45 In addition, a study extension trial found no additional improvement in subjective and objective measurements in patients treated for >6 months.46 Although SjS patients were included in variable proportions in the above-mentioned RCTs, there are no RCTs specifically in primary-2002 patients.64 Only one recent prospective study was made in primary-2002 patients, which found no significant differences between topical CyA and topical 0.1% FML.40 A recent small RCT using 0.03% tacrolimus tear drops found significant improvements in 24 primary-2002 patients48; the lack of definition of the population included (unclear whether they were primary or associated cases), the high rate of side effects and, especially, the limited number of cases does not support their widespread use in primary SjS patients, although they could be considered as a rescue therapy for CyA non-responders/intolerant patients.
With respect to AS and plug insertion, in addition to the very limited evidence available for primary-2002 patients, the two Cochrane SLRs found significant limitations in the quality of trials (incomplete descriptive statistics for reported treatment outcomes, sample sizes with too few participants, quasi-randomisation methods, complete masking may not have been feasible, short-term evaluation of efficacy, lack of details on adverse outcomes and tolerance). For AS, the Cochrane SLR concluded that current evidence suggests that 20% AS might provide some benefit in improving patient-reported symptoms over the short term (2 weeks), but longer periods of follow-up provide no evidence of improvement over longer periods, while no clear effects were found for objective clinical measures of the ocular surface. For punctal occlusion, the certainty of the evidence ranged from moderate to very low (frequently downgrading the level of evidence due to the high RoB or imprecision in effect estimates), and it was concluded that current evidence suggests that punctal plugs are a modestly effective means of treating dry eye. For all these reasons, the use of AS and plugs in primary SjS has been considered as a rescue therapeutic option, always under prescription by an ophthalmologist. A combination of AS and plugs has recently been evaluated65 in 28 SjS patients (primary and associated, criteria not detailed). Ophthalmologists play a key role in prescribing topical and systemic therapies for ocular dryness, always with a close multidisciplinary follow-up.
The two pivotal trials of pilocarpine included 629 patients with primary/associated SjS fulfilling the 1993 criteria and reported statistically significant differences between groups for the two primary VAS outcomes defined. With respect to cevimeline, the two pivotal trials included 272 patients with primary/associated SjS fulfilling the 1993 criteria and reported statistically significant differences between groups for the primary VAS outcomes. There is very limited evidence to support the use of these drugs in the treatment of oral dryness in primary-2002 patients (only one study using pilocarpine). It would seem appropriate to offer patients a trial of the drug, assuming there are no contraindications (ie, uncontrolled asthma, uncontrolled chronic obstructive pulmonary disease, uncontrolled cardiorenal syndrome, acute iritis, pregnancy, breast feeding) to the use of the drug. The trial should be prolonged, since the response can be delayed (up to 12 weeks), with a recommended dose of 5 mg three times a day to keep side effects to a minimum, since the adverse effects are dose dependent. Additional studies are required to clarify the role of muscarinic agonists in the treatment of xerostomia in primary SjS patients.
With respect to systemic synthetic immunosuppressive drugs, there are no new studies specifically assessing GCs in primary SjS in the last 20 years. For immunosuppressive agents, all reported studies (all including <20 patients) were principally centred on the efficacy in sicca features (with limited benefits) and laboratory parameters, with no specific analysis of the outcomes recommended in the guidelines (efficacy in systemic disease) and with an unacceptable rate of adverse events (41%–100%).3 In addition, there is a lack of head-to-head studies comparing the efficacy and safety profile of the different immunosuppressive agents.
The emergence of biological therapies has increased the therapeutic armamentarium available to treat SjS, but their use is limited by the lack of licensing. Available evidence is principally supported by the studies testing rituximab in primary SjS, making this drug the most frequently tested in these patients. There are six additional prospective cohort studies including ≤30 patients (one for etanercept, two—one extension—for belimumab, one for epratuzumab and two for abatacept), one small study (<30 patients) using anakinra, one medium-sized study (n=52) using baminercept and one large trial (>100 patients) using INF.
The results of trials on the efficacy of rituximab in the outcomes evaluated are summarised in the SLR published by Letaief et al.59 There were no statistically significant differences between groups for the primary outcomes based on subjective VAS dryness. The quality of evidence according to the Grades of Recommendation Assessment, Development and Evaluation (GRADE) approach was low for oral dryness, salivary flow rates, fatigue, mental health and ESSDAI meta-analysis and moderate for the Schirmer test meta-analysis. All studies included reported adverse effects, but with no significant differences between groups; the meta-analysis presented low-quality evidence according to the GRADE approach. The promising results obtained in small uncontrolled studies for the use of belimumab and abatacept should be confirmed in large RCTs before a solid therapeutic recommendation for use in primary SjS patients in standard clinical practice can be made. Limited data have been obtained from controlled trials to guide systemic treatment, although prospective studies using rituximab have suggested efficacy in systemic disease, especially in cryoglobulinemic vasculitis, as reported in unselected cryoglobulinemic patients.66
The current evidence supporting the efficacy and safety of the main topical therapeutic options for the treatment of sicca symptoms of primary SjS is solid but is extrapolated from the results of RCTs carried out in mixed populations of patients with dryness caused by SjS and other aetiologies. The overall low level of evidence from therapeutic studies specifically carried out in primary SjS patients fulfilling the current classification criteria underscores the need for considerably larger trials. In addition, there is no information on the differential efficacy and safety of the main systemic therapeutic options available and treatment-by-treatment choices will remain challenging in clinical practice.
Acknowledgments
The Task Force gratefully acknowledges the financial support from EULAR and the support of the EULAR Standing Committee on Clinical Affairs (Professor Ulf Müller-Ladner). The Task Force also expresses its sincere appreciation and gratitude to Désirée van der Heijde for your methodological suggestions and to the EULAR Secretariat and especially to Patrizia Jud, executive assistant, for the outstanding organisation. The authors also wish to thank David Buss (BA, Medical Writer) for technical assistance. These recommendations are also endorsed by the European Reference Network (ERN) for rare and low prevalence complex diseases ReCONNET (Rare Connective and Musculoskeletal Diseases Network).
References
Footnotes
Twitter @@ramos_casals
Contributors PB-Z and SR performed the systematic literature review (SR); MR-C and PB-Z drafted the manuscript. BK supervised the methodology of the SR and the Delphi process. All authors edited the manuscript and accepted its final form.
Funding European League Against Rheumatism.
Competing interests SB’s salary is part funded by the Birmingham Biomedical Research Centre.
Patient consent for publication Not required.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement All data relevant to the study are included in the article.