Article Text

Abstract
Background Association between diabetes mellitus (DM) and risk of osteoarthritis (OA) can be confounded by body mass index (BMI), a strong risk factor for both conditions. We evaluate the association between DM or hyperglycaemia with OA using systematic review and meta-analysis.
Methods We searched PubMed and Web of Science databases in English for studies that gave information on the association between DM and OA. Two meta-analysis models were conducted to address: (1) risk of DM comparing subjects with and without OA and (2) risk of OA comparing subjects with and without DM. As far as available, risk estimates that adjusted for BMI were used.
Results 31 studies with a pooled population size of 295 100 subjects were reviewed. 16 and 15 studies reported positive associations and null/ negative associations between DM and OA. 68.8% of positive studies had adjusted for BMI, compared with 93.3% of null/negative studies. In meta-analysis model 1, there was an increase prevalence of DM in subjects with OA compared with those without (OR 1.56, 95% CI 1.28 to 1.89). In meta-analysis model 2, there was no increased risk of OA (OR 1.14, 95% CI 0.98 to 1.33) in subjects with DM compared with those without, regardless of gender and OA sites. Comparing subjects with DM to those without, an increased risk of OA was noted in cross-sectional studies, but not in case-control and prospective cohort studies.
Conclusions This meta-analysis does not support DM as an independent risk factor for OA. BMI was probably the most important confounding factor.
- osteoarthritis
- diabetes mellitus
- obesity
- meta-analysis
- systematic review
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Key messages
What is already known about this subject?
Obesity is a strong risk factor for development of osteoarthritis (OA).
The association between diabetes mellitus (DM) or hyperglycemia and OA is less clear.
There is conflicting results regarding the association between OA and DM from existing studies.
What dose this study add?
This study is a updated and comprehensive systemic review and the first meta-analysis to refute an independent association between OA and DM.
BMI was the most important confounding factor.
How might this impact on clinical practice?
Future research should account for the effects of BMI as it is a major confounding factor in the development of OA.
Introduction
Osteoarthritis (OA) is one of the leading causes of disability globally with increasing burden,1 driven mainly by increasing age and obesity.2 Our group has previously demonstrated that increasing body mass index (BMI) is a very strong risk factor for OA, even in non-obese ranges.3 In addition to the mechanical stress caused by weight that contributes to the development of OA, evidence has suggested that metabolic mediators of obesity including diabetes mellitus (DM) or hyperglycaemia may play a role. However, whether DM or hyperglycaemia is a causative factor for OA independent from obesity remains controversial.
Obesity is well known to be a strong risk factor for DM or hyperglycaemia.4 Even in experimental animal studies, it is difficult to separate the biomechanical effects of obesity from the effects of diabetes.5 In studies conducted among Caucasian populations that have examined the association between DM or hyperglycemia and knee OA, subjects with DM or hyperglycaemia had much higher BMI compared with those without,6–8 raising the possibility of residual confounding effect of BMI despite statistical adjustments. On the other hand, a large prospective cohort study conducted in a lean population with comparable BMI between comparison groups has demonstrated a negative association between DM and knee OA.9
Recent systematic reviews have reported conflicting results. Both Louati et al and Williams et al reported a positive association between OA and DM.10 11 However, the former meta-analysis pooled crude odd ratios (ORs from studies that did not adjust for BMI. Although the latter meta-analysis reported a positive association between OA and DM that was maintained after adjustment of BMI, this meta-analysis involved a much fewer number of studies and did not include several more recent large studies which showed negative results.9 12 13 More recently, Dawson et al reported that there was little evidence to suggest impaired glucose metabolism as a risk factor for OA.14 However, it was a qualitative analysis which did not include a meta-analysis.
Given the close correlation between obesity and DM or hyperglycaemia in epidemiological studies, it is essential to acknowledge the confounding effect of BMI in the association between DM and risk of OA. There is therefore a need to clarify the association between DM and OA as it has implications on the pathogenesis of OA as well as the clinical management of both diseases. Hence, we conducted a systematic literature review on the association between DM or hyperglycaemia and risk of OA, with attention to how obesity has been adjusted as a confounding factor.
Methods
Literature search and selection of articles
We performed a database search through PubMed and Web of Science for relevant original studies published in full text and in English up to 11 May 2017 that gave information on the association between DM or hyperglycaemia and the risk of onset or progression of OA. We focused on studies in human. The search terms for PubMed were: (“diabetes mellitus, type 2” [MeSH] or “diabetes mellitus, type 1” [MeSH] or “diabetes complications” [MeSH] or “metabolic syndrome X” [MeSH] or (“blood glucose” [MeSH] or “blood glucose” [All Fields])) and “osteoarthritis” [MeSH] and (“humans” [MeSH] and (English[lang])). The search terms for Web of Science were (TS=(diabetes mellitus) and TS=(osteoarthritis) and TS=(human)) and LANGUAGE: (English). An updated search from 11 may 2017 to 22 Jan 2018 was performed using PubMed using the same search terms. Two researchers (CM and YYL) reviewed the titles, abstracts and full-text articles (when appropriate) and selected eligible articles by consensus. A third researcher (AK) was involved in consensus meeting for selection of articles in cases of disagreement.
Data extraction and quality assessment
Four independent researchers worked in teams of two (YYL/AK, YYL/CH, YYL/LH) to extract data independently onto a standardised protocol, followed by consensus of the data. In cases where there was disagreement between the two researchers, a third researcher reviewed the data to achieve consensus. The data extraction protocol consisted of the following: study design (cross-sectional, case-control or prospective cohort) and population (community, registry or hospital), case definition for OA, site of OA, BMI or number of subjects with obesity, population size and the outcome (relative risk, OR or HR or conclusion).
Quality assessment for the selected studies was performed using Newcastle-Ottawa Scale (NOS) for case-control study or prospective cohort study where applicable.15 Studies were assessed according to three domains: selection, comparability and outcome for prospective cohort studies; and selection, comparability and exposure for case-control studies. Stars (*) were awarded for each of the categories, to a maximum of four stars for selection, two stars for comparability and three stars for outcome/exposure. For comparability, BMI and age were chosen as the main factors for consideration. According to NOS, one star is awarded for comparability if the study controls for the most important factor (BMI) and another star for the second most important factor (age), with a maximum of 2 stars were awarded for compatibility for each study. In this study, we specifically evaluated the comparability of BMI between DM with non-DM, and OA with non-OA for each study in a more stringent manner. A star for BMI compatibility was awarded to a study only if the difference in BMI between the comparison groups was less than 1 kg/m2. For study with baseline BMI between comparison groups exceeding 1 kg/m2, but have adjusted BMI in the statistical models, a half star (denoted by (∅)) was awarded.
Qualitative appraisal of studies
We summarised studies in table formats separately for positive and null/negative studies. We presented in tables the study designs, sample sizes, difference in baseline BMI comparing participants with or without OA and participants with or without DM whichever were available. We made descriptive comparison between positive and negative studies for these baseline characteristics.
Meta-analysis
We performed comparative analysis for OR and 95% confidence intervals (CIs) in assessing the association between DM or hyperglycaemia and OA. We performed the meta-analysis with a random effect model using Comprehensive Meta-analysis V.3. Data for each study were entered as sample size/events, ORs/CIs for cross-sectional/case-control studies or hazard ratios (HRs)/CIs for prospective cohort studies. These were computed and summarised as standardised OR and variance. We expect high heterogeneity of these epidemiology studies that have different study designs, definition of cases and were conducted and in multiple centres and countries with multiple ethnicities and thus cannot be assumed to share a common effect. Rather, the summary effect was an estimate of the mean of a distribution of true effect.16 Therefore, the random effect model was more appropriate and was used throughout.
Two models were conducted to address: (1) the risk of DM or hyperglycaemia comparing subjects with and without OA and (2) the risk of OA comparing subjects with and without DM. As far as data are available, we used the best adjusted model from each study that accounted for age, BMI and other covariates in the meta-analyses. For studies that have multiple subgroups comparing to the same non-case (controls), such as prevalence or progression of OA compared with controls, prevalence of OA was chosen in the main model. Similarly, if multiple sites of OA sites were compared with controls, one site of OA (knee as first choice) was chosen. For studies that had stratified analysis for subgroups (such as gender and age), data were presented as separate study data point in the meta-analysis.
For model 2, we performed additional sensitivity analyses with comparability of BMI in studies, first limited to studies that have adjusted for BMI in the statistical models and second limited to in studies that had comparable BMI between subjects with DM compared with without DM. Limiting to studies with comparable BMI between groups at baseline may allow the possible biometabolic effect of DM on risk of OA to be revealed more independently from the biomechanical effect of BMI. In addition, we conducted subgroup analyses to evaluate the effects of study design, gender and sites of OA on effect of risk estimates.
We tested publication bias by visual assessment using funnel plots and quantitatively using Egger’s test (p>0.05=no publication bias).17 We also simulated missing studies using the ‘Trim and Fill’ method.18 The imputed studies were plotted with the observed studies in the funnel plot and the risk estimates were re-evaluated to give insight of possible change when the models were free of publication bias.
Results
Literature search results
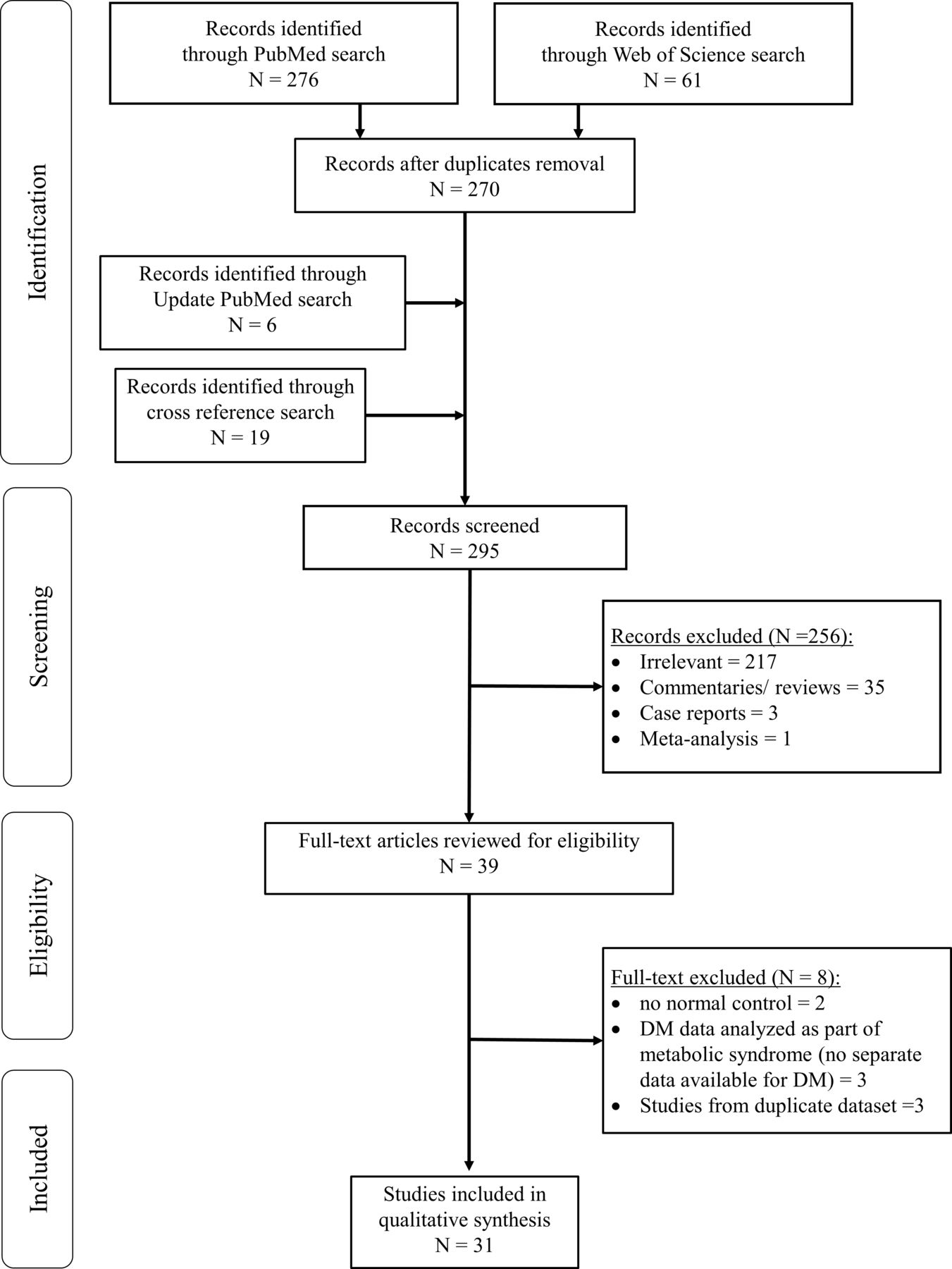
Our literature search through January 2018 identified a total of 337 articles. After removal of duplicates, 270 unique articles remained. Majority of these were excluded for the following reasons: irrelevant (217 articles), commentaries or reviews (35 articles), case reports (three articles) and meta-analysis (one article). An updated search added six more articles while 19 other articles were identified by cross reference checking. In total, 39 relevant articles were retrieved for full text review. Of these, two were excluded for lacking a control group without OA, three were excluded as DM was evaluated as part of metabolic syndrome without separate data available for DM or hyperglycaemia and three were excluded for duplicated publications from same databases. The final review included 31 studies comprising 8 prospective cohort, 11 cross-sectional and 12 case-control studies (figure 1), representing a total study population of 295 100 subjects.
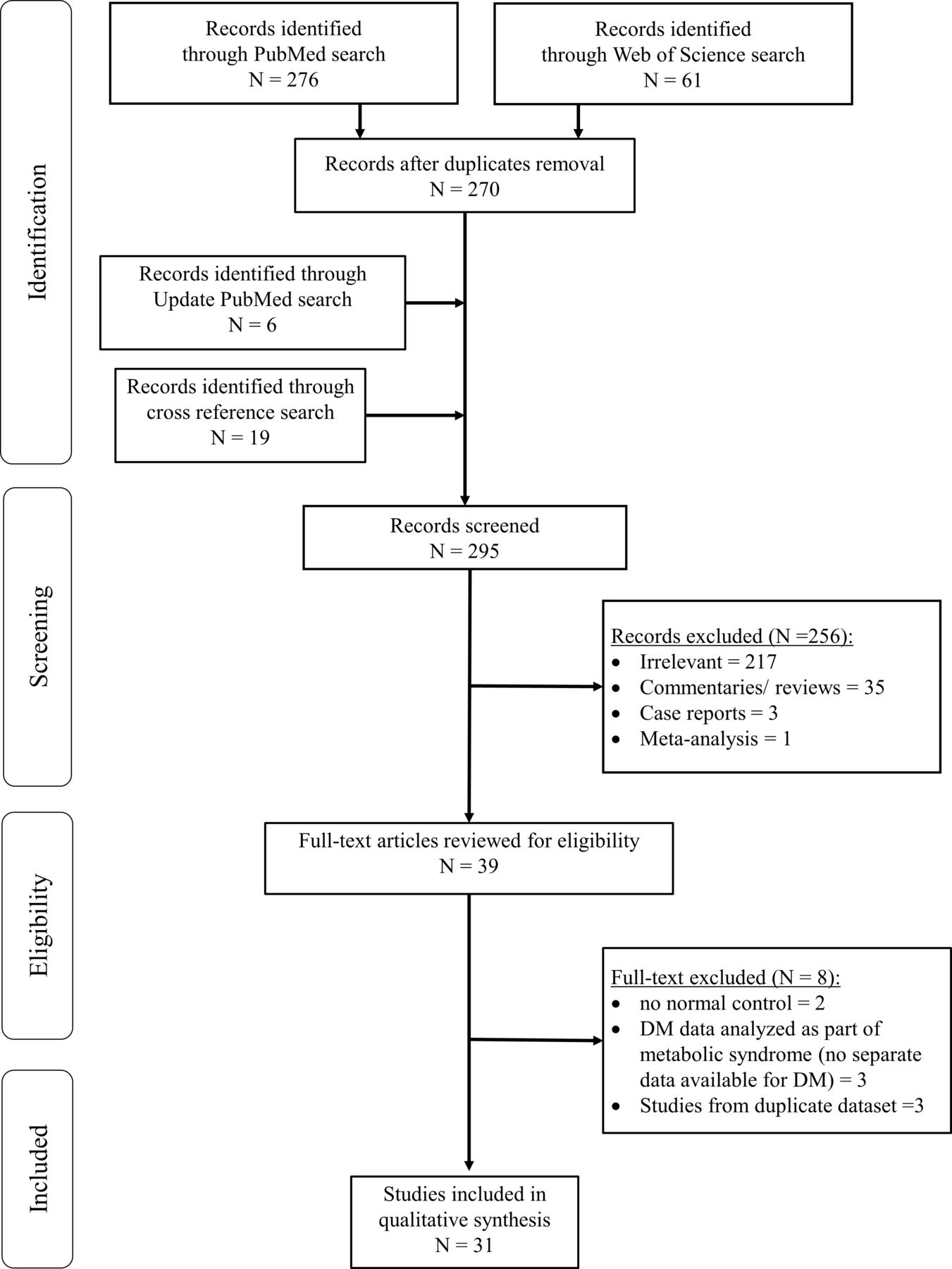
Flowchart for selection of articles. DM, diabetes mellitus.
Study characteristics
Of the 31 studies, 16 reported positive associations between DM or hyperglycaemia and OA (table 1), while 15 showed null/negative associations (table 2).
Epidemiology studies reporting positive association between hyperglycaemia or diabetes mellitus and osteoarthritis
Epidemiology studies reporting null or negative association between hyperglycaemia or diabetes mellitus and osteoarthritis
Positive studies
Studies that showed positive associations represented a pooled study population size of 108 258. Only three of these studies were prospective cohorts (table 1), representing 2782 subjects. As majority of the positive studies had small sample size, the results were mainly driven by one large cross-sectional study with a sample size of 81 634,19 for which BMI was not adjusted in the model. Overall, 11 out of 16 studies (68.8%) had at least some form of adjustment for BMI. Two studies20 21 (12.5%) had comparable BMI between subjects with and without DM. Nine studies adjusted for BMI with statistical modelling.7 8 22–28
Null/negative studies
The 15 studies that reported null or negative association between DM or hyperglycaemia and OA, represented a total population size of 186 842. There was a higher number of prospective cohort studies (five studies),9 29–32 in which exposure and covariate factors prior to the outcome were minimised. These 5 prospective cohort studies involved much higher number of 83 857 subjects compared with the 2782 subjects involved in the positive studies with prospective cohort design (table 2). Within these five prospective cohort studies, four reported negative associations between DM and OA.9 12 13 33
These null/negative studies generally had larger sample sizes than the positive studies. Fourteen out of 15 null/negative studies (93.3%) had adjusted for BMI in the final models, while 5 studies (33.3%) had comparable BMI between subjects with DM and those without.9 31 33–35
Meta-analysis Model 1: Risk of DM comparing subjects with OA to those without OA
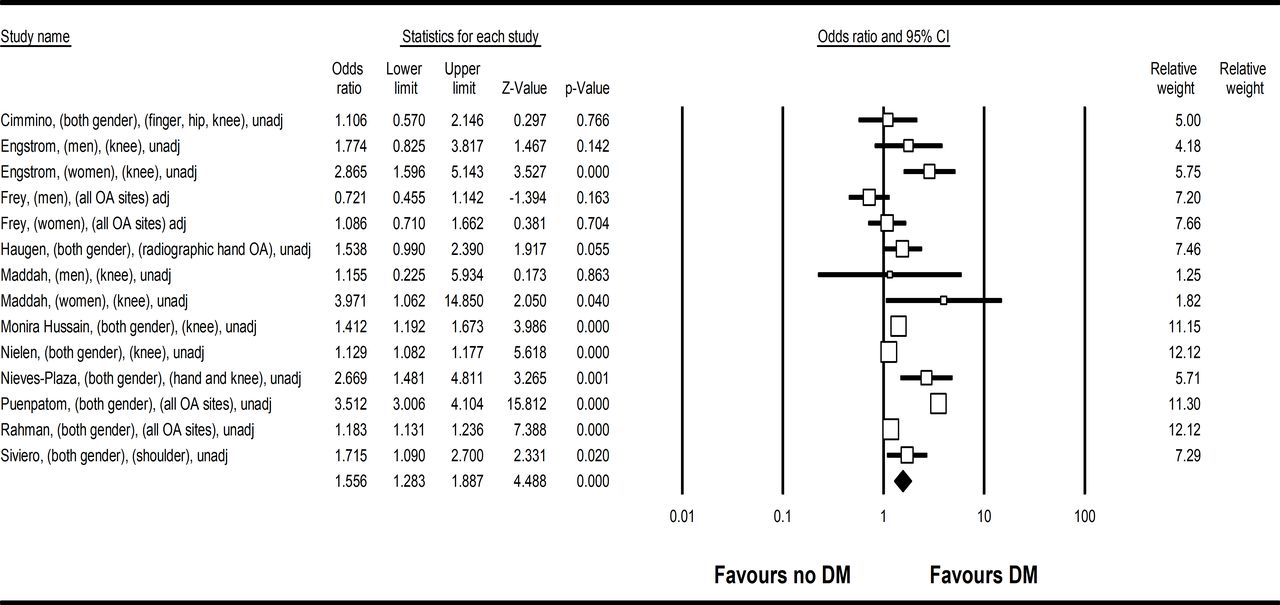
Eleven studies were analysed in the meta-analysis to assess risk of DM in subjects with OA compared with those without OA. The pooled population size was 209 610. There was increased risk of DM comparing subjects with OA to those without (OR 1.56, 95% CI 1.28 to 1.89, heterogeneity I2=94.2%) (figure 2). Apart from one study,31 all studies did not adjust for body weight, obesity or BMI in the models. This pooled OR represented a higher crude prevalence of DM among subjects with OA compared with those without. Funnel plot (online supplementary figure 1) revealed no publication bias (Egger’s test p=1.50).
Supplemental material

Forest plot on meta-analysis on risk of DM comparing subjects with OA to those without OA (OR 1.56, 95% CI 1.28 to 1.89). Legend: Study name were described as first author, gender, OA site, adjusted or unadjusted for BMI. BMI, body mass index; DM, diabetes mellitus; OA, osteoarthritis.
Meta-analysis Model 2: Risk of OA comparing subjects with DM to those without DM
Twenty-two studies were analysed in the meta-analysis to assess risk of OA in subjects with DM or hyperglycaemia compared with those without. Among the pooled population size of 200 686 subjects, there was no significant association between DM and OA, (OR 1.14, 95% CI 0.98 to 1.33, heterogeneity I2=74.2) (figure 3). Two studies have not adjusted BMI in their statistical models, one of which did not provide detail on baseline BMI between DM and non-DM subjects,36 while another had comparable BMI between DM and non-DM subjects at baseline.33 For the other 20 studies, the best adjusted OR that included BMI from studies were used. This model showed no significant increase risk of OA comparing subjects with DM and those without, when other confounding factors including BMI were accounted for. Funnel plot was asymmetrical with missing studies with negative associations (online supplementary figure 1), indicating possible publication bias (Egger’s test p=0.02). The re-evaluated risk estimate was 1.06 (95% CI 0.91 to 1.24).

{kind=link}
{kind=link}
{kind=link}
Forest plot on meta-analysis on risk of OA comparing subjects with DM and to those without DM (OR 1.14, 95% Cl 0.98 to 1.33). Legend: Study name were described as first author, gender, OA site, adjusted or unadjusted for BMI. BMI, body mass index; DM, diabetes mellitus; OA, osteoarthritis.
In the sensitivity analyses that limit to studies with BMI adjustment in statistical models (20 studies), and studies with comparable baseline BMI between subjects with or without DM (seven studies),9 20 31 33–35 37 no significant associations were noted between OA and DM (OR=0.94, 95% CI 0.68 to 1.29) (table 3). Publication bias with missing negative studies was revealed in model with adjusted BMI, but not in model with comparable baseline BMI (online supplementary figure 6, table 3).
Summary of risk estimates of the association between diabetes or hyperglycaemia and osteoarthritis
In the subgroup analysis stratified by study design, increased risk of OA was noted comparing DM with non-DM subjects in cross-sectional studies (OR 1.29, 95% CI 1.10 to 1.51), but not for case-control (OR 0.82, 95% CI 0.49 to 1.38) and prospective cohort studies (OR 1.08, 95% CI 0.80 to 1.44). Other sensitivity analyses for genders and site of OA did not reveal significant association between OA and DM (table 3). The forest plots of all subgroup analyses are shown in online supplementary figures 2–5. No publication bias was noted in sensitivity analysis stratified by study design (table 3). Publication bias was noted in the sensitivity analysis for studies in women, but not noted in studies in men (table 3).
Discussion
This systematic review and meta-analysis refute DM as an independent risk factor for OA, when BMI is accounted for. This finding remained consistent regardless of gender and site of OA.
Our findings corroborate with a recent systematic review,14 which reported little evidence to suggest that impaired glucose metabolism was a risk factor for OA. This is in contrary to two previous meta-analyses on the same topic.10 11 There are several strengths of our current findings compared with that of the two previous meta-analyses. First, our updated literature search included several recent and larger studies that reported null/negative association between DM and OA.9 12 29 Two of these studies were of prospective cohort design,9 29 while the other was a huge population-based case-control study with cases of hip and knee OA matched to age and gender with population control.12 All three recent studies had adjusted for BMI in their final model, one had comparable BMI between those with or without DM for the knee OA model,9 while the other two had comparable BMI for cases of OA versus non-OA cases in the hip OA model (but not for knee model).12 29 Second, we used the best adjusted OR which included BMI, the strongest confounding factor in our meta-analysis. In our qualitative systematic review, we have demonstrated that there were fewer positive studies that had adjusted for BMI. BMI is an established and strong risk factor for both DM4 and OA, particularly for weight-being joints. It is therefore not unexpected that in most of these studies conducted among Western populations, subjects with diabetes or hyperglycemia had much higher BMI, or higher proportion of obesity compared with those without these conditions.6 7 13 33 38 For example, in a prospective cohort study from Italy,7 the mean baseline BMI in subjects with DM was 27.0 kg/m2 compared with 24.8 kg/m2 for subjects without DM. Given the large discrepancy between baseline characteristic, it is challenging to eliminate residual confounding effect of obesity on the association between diabetes and knee OA risk, even after adjusting for BMI with statistical modelling.
The result of our study may be explained by two possibilities. First, DM is truly not a risk factor for OA. Second, when BMI is such a strong risk factor for OA, any weaker risk factors for OA would be masked by the confounding effect of BMI. Therefore, we proposed that the true risk estimates attributed by DM independently towards OA may be revealed in populations where BMI is more comparable between comparison groups. Indeed, we have demonstrated that among the seven studies that had comparable baseline BMI between subjects with or without DM,9 20 31 33–35 37 only one study showed a positive association between DM and OA,20 four did not show an association,31 34 35 37 while two showed a negative association between DM and OA.9 33 We found no publication bias in this model. Limiting to studies with comparable BMI between groups at baseline may allow the possible biometabolic effect of DM on risk of OA to be revealed more independently from the biomechanical effect of BMI. Of note is that we used an arbitrary BMI of within 1 kg/m2 difference to define comparability, which may not be truly comparable. However, it is a relatively smaller difference compared with the other studies.7 In our sensitivity analyses, we asked whether the association between DM and OA may only be applicable to certain subgroups, including women and non-weight bearing joints. The notion of no significant association between DM and OA remained, apart from the subgroup analysis for cross-sectional studies which reached statistical significance.
Several in vitro and in vivo studies have suggested that increased oxidative stress, cytokines and the accumulation of advanced end glycation products (AGE) may link hyperglycaemia to OA.39 40 However, BMI was not accounted for in these studies. Even in experimental animal studies, it is difficult to separate the biomechanical effects of obesity from the biometabolic effects of diabetes.5 All diabetes animal models, either induced from genetic manipulation or high fat diet, were more obese than the control animals without induced diabetes.5 Laiguillon et al reported greater interleukin-6 and prostaglandin E2 expression on stimulation with interleukin-1β comparing human cartilage taken from OA subjects with DM to those without DM.39 However, subjects with DM in their study weighed on average 5 kg higher compared with their non-DM counterparts. Similarly, Zhang et al reported significantly higher levels of AGE in synovial fluid in subjects with DM compared with those without.40 Again, subjects with DM had significantly higher BMI than those without DM. It has been postulated that obesity results in an increased state of systemic inflammation with increase in inflammatory cytokine, adipokine and acute phase reactant production41 which may link to insulin resistant, and mimic those seen in OA. The implications of our current study that refuted an association of DM and risk of OA indicate that BMI is a strong confounding factor which cannot be ignored in analysis of the relationship between DM and OA. Until further mechanistic causative link is found between DM and OA on the molecular level, caution should be exercised in interpreting the association between DM and OA from epidemiological studies.
The main limitation of the current study was the moderate to substantial heterogeneity among the studies (I2=74%). This was likely related to the expected diversity in the characteristics of the population from the various studies. Therefore, the random effect models have been applied. Attempts have been made to mitigate this through sensitivity analyses in various subgroups, although a moderate to substantial degree of heterogeneity was still present. Second, majority of the studies in the analysis were retrospective cross-sectional and case-control design. As community-based prospective cohort studies measure potential exposures before the outcome of interest, they are generally subject to less risk of recall bias and selection bias, although attrition bias may present.42 There were higher number of prospective cohort studies in those reported null/negative association between the DM and OA, yet the total number of prospective cohort studies was less than one third. Apart from one study that was specific to type 1 DM,35 all studies did not specify type of DM. Therefore, the results of this meta-analysis may only be generalisable to a mixed population with type 1 and type 2 DM.
Conclusion
In summary, we report the first meta-analysis showing no association between DM and OA. Future research should account for the effects of BMI as it is a major confounding factor in the development of OA.
References
Footnotes
Contributors YYL and CM conceptualised and designed the study. AK, CM, CH, LH and YYL acquired the data. AK and YYL performed the data analysis. All authors interpreted the data. AK and YYL drafted the manuscript. All authors critically revised the manuscript and approved the final version of manuscript.
Funding YYL was supported by the National Medical Research Council, Singapore (NMRC/CSAINV/0022/2017).
Competing interests None declared.
Patient consent for publication Not required.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement All data relevant to the study are included in the article or uploaded as supplementary information. Data are available on reasonable request. Request can be made by email to the correspondent author.