Article Text

Abstract
Fatigue in rheumatoid arthritis is highly prevalent. It is correlated only weakly with disease activity but more so with pain, mood, personality features, poor sleep, obesity and comorbidities. Fatigue can be measured by many standardised questionnaires and more easily with a Visual Analogue Scale or numeric rating scale. Most patients with RA have some fatigue, and at least one in six have severe fatigue. Chronic pain and depressed mood are also common in RA patients with significant fatigue. It affects function and quality of life and is worse on average in women. Evidence-based treatment for fatigue includes treatment of underlying disease activity (with on average modest improvement of fatigue), exercise programmes and supervised self-management programmes with cognitive-behavioural therapy, mindfulness and reinforcement (such as reminders). The specific programmes for exercise and behavioural interventions are not standardised. Some medications cause fatigue such as methotrexate. More research is needed to understand fatigue and how to treat this common complex symptom in RA that can be the worst symptom for some patients.
- Ant-CCP
- Rheumatoid Arthritis
- Systemic Lupus Erythematosus
- Systemic Sclerosis
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
SCOPE OF THE PROBLEM
Rheumatoid arthritis (RA) is an autoimmune inflammatory condition with joint damage, pain, functional impairment and fatigue.1 Even though there are many treatments approved for RA, fatigue affects at least three-quarters of patients.2 Using a fatigue Visual Analogue Scale (VAS), 50% of RA patients have fatigue, that is at least five out of 10.2 3
Key messages
Fatigue is very common in RA and is weakly correlated with disease activity.
Fatigue adversely affects the quality of life in RA.
Fatigue is related to pain, comorbidities, mood, poor sleep and personality factors.
Treatment of active RA can improve fatigue modestly.
Evidence-based treatment of fatigue in RA with mostly modest or weak effect size includes exercise and some guided self-management/cognitive-behavioural treatments.
Research is needed to find a more effective treatment for fatigue in RA.
Fatigue can be from disease activity, chronic pain, sleep disturbance, poor mood and other reasons including comorbidities. It is often correlated with disease activity but more with strongly with pain.2 4 When there are high inflammatory markers, cytokines that are elevated may cause a person to feel tired or even exhausted. This can be similar to the prodrome of an infection.5
A previous review of fatigue in RA did not consistently show the same factors associated with fatigue.4 Depressed mood, sleep disturbance and functional impairment (disability) appear to frequently explain fatigue in patients with RA. Of course, if it can be exhausting to do usual activities when RA is active, and damage and/or pain will worsen fatigue. Many activities of daily living are affected in RA patients such as dressing, walking, meal preparation, eating and personal care such as bathing.6
When fatigue is rated very high repeatedly, it is likely not related solely to active RA. There are differences in the findings of associations with physical function and significant fatigue in RA. For instance, severe fatigue in people with RA is associated with self-rated health, pain and anxiety/depression rather than with physical capacity.7 Whereas, in multivariate models, severe fatigue has been associated with females more than males, disease activity, impaired function, current treatment with NSAIDs and biologics, multimorbidity, obesity and anxiety/depression. Severe fatigue has been correlated with the number of morbid conditions, including obesity, hypertension, COPD and anxiety/depression.8 Fatigue certainly is related to pain and mental health issues (depressed mood) and with other comorbidities whereby more health problems increase the likelihood of fatigue in RA.
More than three-quarters of patients with RA experience chronic pain within 5 years of their diagnosis.9 Personality traits and stress will affect fatigue in RA. RA patients have higher stress compared with osteoarthritis and population controls.10–12 It was observed that worrying, catastrophising and certain personality traits decrease physical and psychological function,13 and pain catastrophising (helplessness) worsens stress even when adjusting for age, gender and pain, all of which likely impact fatigue adversely.14 In contrast, the authors of a recent study concluded that fatigue was associated more in extroverts with RA.6 However, the association between fatigue and personality traits likely needs verification in other studies. In general, if very few studies find an association between patient factors and fatigue, then more research may reconcile if findings are consistent and generalizable to fatigue in RA.
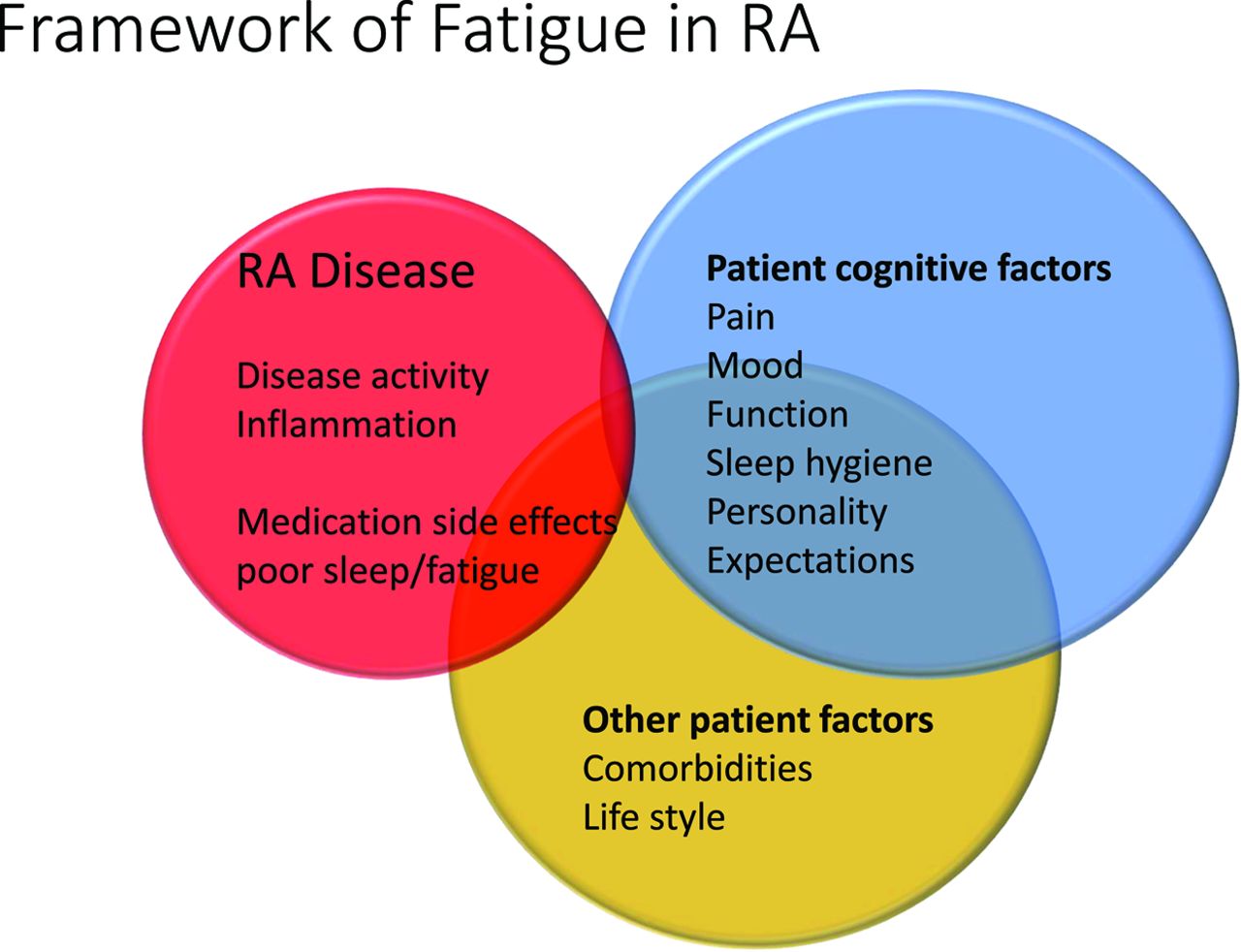
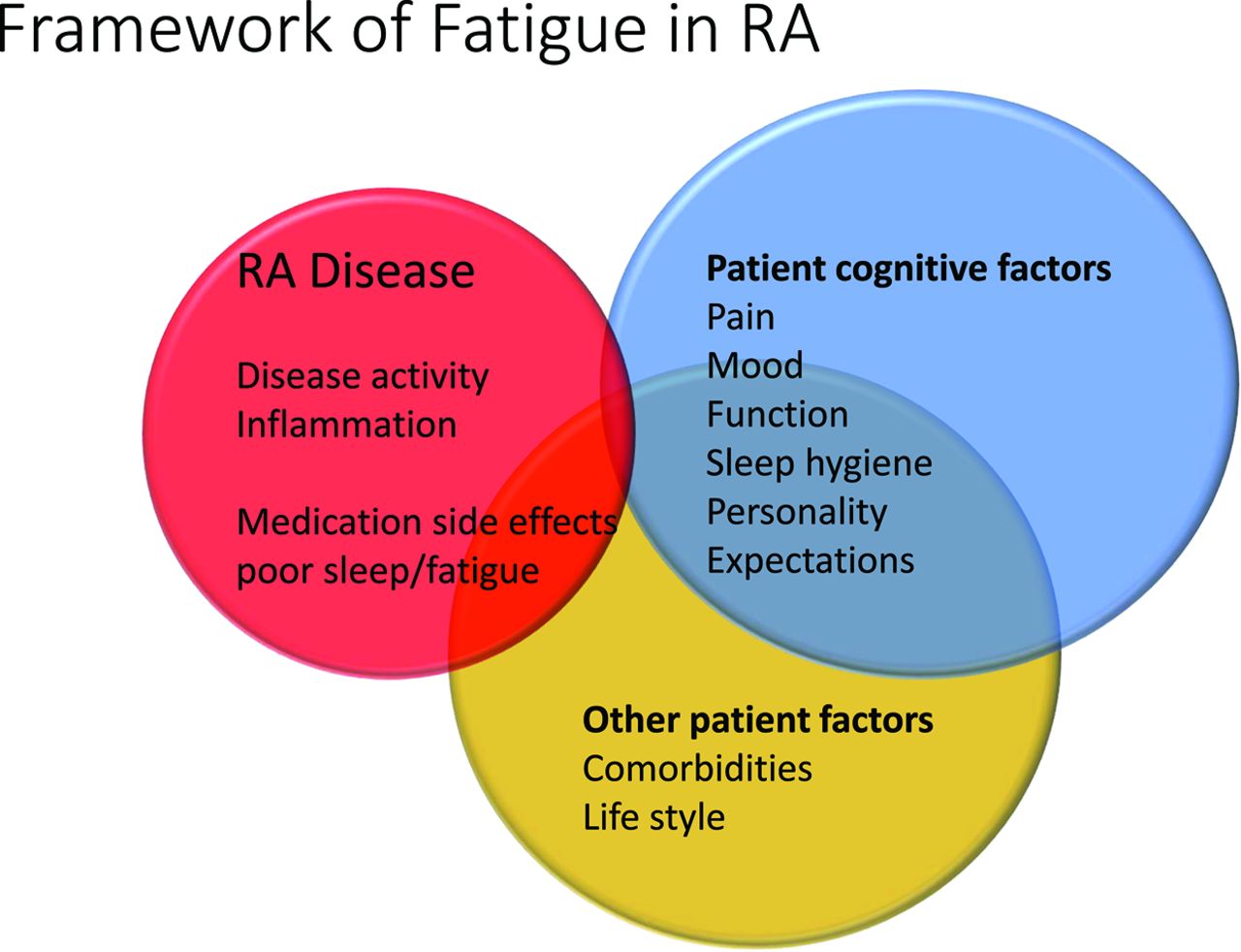
A framework has been suggested of fatigue in RA and includes disease factors (inflammation, pain, disrupted sleep and disability), personal factors (comorbidities and work) and cognitive-behavioural interface (personality, thoughts and feelings driving reactions and activity).15 16 Figure 1 shows factors that can impact fatigue and their relative contribution to chronic fatigue in RA. Clinicians should note that disease activity only plays a minor role in chronic severe patient-reported fatigue. Consideration of pain, mood and poor sleep could be explored in each patient in order to determine a more comprehensive treatment plan. Patient comorbidities that could contribute to poor sleep such as sleep apnea should be ruled out when there is a high index of suspicion. Anaemia, hypothyroidism, uncontrolled diabetes mellitus and other morbidities can contribute to fatigue.
{kind=link}
Framework of fatigue in rheumatoid arthritis (RA).
Measurement of fatigue in RA
Numerous fatigue tools/scales have been used in RA. A systematic review described 23 different fatigue tools which were published before Patient-Reported Outcomes Measurement Information System (PROMIS) was developed.17 18 In their review, they concluded that ordinal (Likert) and VAS, the Short Form 36 vitality subscale, the Functional Assessment of Chronic Illness Therapy Fatigue Scale (FACIT), the RA-specific Multidimensional Assessment of Fatigue scale (MAF) and the Profile of Mood States were validated and seemed sensitive to change.17 19 20 Some scales are generic, and others are disease specific.
Commonly used measures of fatigue in RA include numeric rating scales such as VAS 0 to 100 mm or an 11-point scale (from 0 to 10). Other scales such as change in fatigue have been used (such as 5-point scale from much worse, worse, no change, better and much better). Other questionnaires within RA trials include the Functional Assessment of Chronic Illness-Fatigue (FACIT-F); Bristol Rheumatoid Arthritis Fatigue-Multidimensional Questionnaire (BRAF-MDQ); SF-36 vitality domain (0 to 100) and PROMIS-29 Fatigue T-score. The FACIT-F scale ranges from 0 to 52, where higher numbers imply less fatigue. Fatigue scales are correlated to each other, but there is no universally agreed-upon fatigue questionnaire/tool to use in RA.17–20 The PROMIS fatigue score has face validity; measures fatigue across the spectrum of severity; is correlated with pain, sleep disturbance, anxiety and depression and disease activity and is also strongly correlated with other fatigue scales.18
Concordance with active disease
RA disease activity and fatigue are correlated in many studies, but often the associations are weak.4 21–23 When patients with RA flare, usually pain and fatigue increase.24 For instance, fatigue was associated with flare in RA patients with the TNF inhibitor dose decreased, but other variables had more impact in the analyses such as baseline DAS28 and mental health.25
The mean fatigue in RA patients studied cross-sectionally was 4/10, with 40% having severe fatigue.9 Associations with fatigue are not necessarily consistent between studies. High fatigue in one study was associated with females, disease activity, function, treatment and multimorbidity (especially obesity and anxiety/depression). However, significant fatigue in RA in another study was associated with self-rated poor health, pain and anxiety/depression but not physical capacity/function.7
In the Canadian early RA (ERA) cohort (CATCH cohort), correlations between fatigue and disease activity were studied. It was found that fatigue was related to pain and the patient global rating moderately at baseline but only weakly correlated with disease activity as measured by swollen and tender joint counts, physician global assessment of disease activity and inflammatory markers.26 Fatigue at baseline and at 3 months predicted fatigue, pain, joint counts, global assessments and disease activity at 12 months.26 In general, fatigue is weakly correlated with disease activity.27 In general, medications that improve disease activity partially improve fatigue.28 Another study suggested that the variation in fatigue was explained by problems other than RA including obesity, physical inactivity, poor sleep and depression.16 Worse Health Assessment Questionnaire (HAQ) was related to higher fatigue, especially in women with RA, even when treating to a target.29 Poor function and fatigue could be the results of other factors such as depression and pain as many of these variables are inter-related. The biggest predictor of fatigue at 1 year in ERA was baseline fatigue and fatigue at 3 months.30 In summary, disease activity and other patient-reported outcomes in RA are often concordant with fatigue, but RA disease activity does not account for most of the fatigue in RA.
Discordance with disease activity
Fatigue in RA is usually present even if disease activity is low. This can be due to chronic pain which is common in RA. Pain can lead to poor sleep, depressed mood and fatigue, all of which are connected.6 18 28 31 32 Also, more than 10% of patients with RA have fibromyalgia33 and 10% report depression in ERA.26 Behavioural and psychological factors are more likely explanations of fatigue in RA and not disease activity.16
When patients with ERA were treated using a treat-to-target strategy, it was observed that there was only a small mean change in fatigue. In fact, three-quarters with baseline fatigue who had improved with respect to disease activity had residual fatigue at 1 year30; in another study one in four ERA patients had worsening fatigue over time, one in three was stable and 40% improved fatigue by 1 year.34
Remission does not necessarily equate to low fatigue
When in remission in ERA, many patients have low levels of fatigue; but some still have significant fatigue. RA patients with a sustained state of low disease activity (LDA) had a mean FACIT-F score in the 40s so residual fatigue persisted for many patients.35 The SF-36 vitality domain (scale, 0–100) demonstrated all but approximately 15% were not in fatigue remission when in DAS remission (DAS of <2.6).36
Within the Outcome Measures in Rheumatology (OMERACT) flare working group, a Delphi exercise was performed, and fatigue did not meet consensus for inclusion within the development of the flare questionnaire in RA.24 Fatigue in RA is multifactorial and only partially related to disease activity which may have accounted for poor agreement with respect to a fatigue domain within a flare questionnaire in RA.
Reasons for fatigue in RA
There are several causes of fatigue in RA.2–5 10 16 For instance, active RA with inflammation22 and pain cause fatigue directly by altered cytokines but also disruption of sleep due to pain.4 5 10 Chronic pain alters sleep through changes in mood affecting sleep patterns.2 5 6 9 16 Decreases in physical activity and stress due to a chronic disease that is life altering will impact energy in a negative way.7 Medications such as methotrexate and even sulfasalazine can cause fatigue.7 37 Different routes of administration or dosing of methotrexate may be helpful to reduce fatigue as a side effect.37 Treatments should be multidimensional in order to improve fatigue in people living with RA.
Chronic pain and fibromyalgia in RA influence fatigue
In ERA, fibromyalgia is increased 10-fold in the first year and fivefold in the second year after the onset of RA. Fibromyalgia was related to pain and poor mental health and not inflammation.33
Timing of maximal improvement in fatigue when in sustained remission in ERA
An ERA cohort which included 1864 patients studied how fatigue varied over time.26 A quarter had low fatigue, nearly 20% moderate and approximately 60% high fatigue at baseline. The baseline fatigue and pain scores were similar, around 5 out of 10. DAS28 seemed to be moderately related to fatigue at baseline where the DAS28 score was highest in the highest fatigue level, next highest in the middle level and smallest in the lowest fatigue group.
The baseline SF-36 mental component summary scores (MCS of SF-36) also were different differed significantly between the fatigue groups. The mean baseline fatigue score measured by a VAS was highest at baseline than follow-up visits. Fatigue decreased by the 3-months visit where the largest between visit change occurred (from baseline to 3 months compared to other time points within the first year).
If a patient achieved remission or a low disease state by 3 months, this was predictive of lower fatigue over time than if they did not. The question was asked when the lowest fatigue level occurred after a patient with ERA was in sustained remission. The lowest mean level of fatigue seemed to lag behind remission by many months. This could imply that once disease activity has markedly improved, it takes time to optimise fatigue. One could speculate that it takes time after chronic inflammation is controlled to have better quality and quantity of sleep. Sustained remission within 1 year of ERA onset was associated with improved fatigue compared with not achieving remission with parallel decrements, except optimal lowest fatigue level lagged behind remission by approximately half a year.26
Established RA: is there a lag in fatigue improvement?
Patients with RA in the Ontario Best Practices Research Initiative (OBRI) registry that were not in a low disease state at baseline were followed to determine if patient-reported outcomes (PROs) improved differently comparing ERA with established RA. In nearly 1000 RA patients of whom one-third had early disease, time to remission was faster in ERA as was time to achieving a physician and patient global assessment of 0 or 1 out of 10. However, the time to improving fatigue was the same in both those with early and established RA.38
TREATMENT
There is no uniform treatment for fatigue in RA, and many proven interventions have small effect sizes from small trials. This is probably due to the fact that fatigue is from multiple different causes within and between individuals and that when it becomes chronic, it is less likely to dramatically improve. This seems similar to chronic pain in RA. Treatment can be divided into pharmacologic and non-pharmacologic. Table 1 illustrates the evidence of treatment of fatigue in RA. Future research should be focused on designing well-powered randomised trials of interventions thought to have at least a moderate effect size. Possibly several interventions could be studied in one trial in order to determine if there is incremental benefit combining multiple modalities and thereby increasing the likelihood of a larger treatment effect. For instance, a trial could be designed comparing exercise, cognitive-behavioural therapy (CBT) and pharmacological treatment together versus each individual treatment. Better interventions for fatigue in RA are an unmet need.
Summary of treatment of fatigue in RA
Pharmacologic treatment of fatigue
Pharmacological treatment of fatigue in RA has been primarily studied by treating disease activity and/or pain. Treating to a target and achieving rapid remission or very low disease state in ERA predicts lower fatigue early and later (even at 5 years).26 Effective treatment in RA will only partially reduce fatigue if it is related to the disease activity in RA.
Virtually all treatments in RA will reduce fatigue, including conventional synthetic disease-modifying anti-rheumatic drugs (csDMARDs), targeted synthetic DMARDs, biologic DMARDs and corticosteroids.37 39–54 The average effect of treatment on fatigue in active RA with various advanced therapies is meaningful but not large.39 Treatment of disease activity in RA has a small impact on fatigue, whereas physical inactivity, poor sleep and depressed mood explain most of the fatigue.28 Often fatigue is an exploratory outcome in trials. Medications can cause or exacerbate fatigue. A strong predictor of nonadherence to methotrexate was fatigue (but baseline fatigue was not related to methotrexate; whereas increasing fatigue later could be due to methotrexate).37
More than 2000 patients with RA who were followed in a registry and started either methotrexate monotherapy or a TNFi were studied to determine associations with fatigue.40 At 6 months, nearly one-third were in remission with a median fatigue of 2/10 and 25th percentile was 0.6 and 75th percentile was 4.3/10. However, 28% had fatigue >4/10. Higher pain levels at baseline and 6 months were associated with fatigue. So, other methods of treating fatigue in RA are needed beyond treatment of active disease. In a different study, 48 RA patients demonstrated significant improvements in fatigue measured by the Fatigue Severity Scale after initiation of biologic DMARDs.41 PROs such as fatigue, pain and patient global assessment have only weak correlations in active RA when biologics are used.42
Improvement in fatigue has been related to the line of therapy in a review of abatacept trials. Abatacept improved fatigue more than placebo, and improvements in fatigue were higher in ERA compared with biologic exposed patients.43 More than 1500 patients from the three trials were analysed, and the authors concluded that improvement in fatigue and other outcomes such as pain, sleep and remission had poor agreement and earlier lines of therapy had more responsiveness with respect to fatigue in patients treatd with abatacept.
Half the patients in the Corrona Database reated with rituximab (N=667) after one or more TNF inhibitors had improvement in fatigue.44
Interleukin-6 may be important in the perception of fatigue, as it is an inflammatory cytokine. There are two anti-IL-6 biological treatments approved for RA. Tocilizumab improves signs and symptoms of active RA in RCTs including fatigue.45 In an observational study, at 2 years of follow-up, tocilizumab significantly decreased fatigue.46 The variance in fatigue in a tocilizumab treatment study was explained mostly by sleepiness, depressive symptoms and disease activity (DAS28).47 In RCTs, sarilumab has shown improvement in PROs, with an effect size that was clinically relevant for fatigue but not as large as for pain.48
The Janus kinase (JAK) inhibitors have also demonstrated clinically relevant improvements in fatigue in patients with active RA across lines of therapy such as in ERA (methotrexate naive), methotrexate inadequate responders and biologic inadequate responders.49–54 Tofacitinib and baricitinib are approved in many countries and upadacitinib has been approved in the USA and elsewhere. It is anticipated that filgotinib will also be approved in RA. Treatment with baricitinib in active RA patients who were inadequate responders to methotrexate improved pain, fatigue, function and work productivity more than placebo.52 Possibly, JAK inhibitors are more effective in treating pain in active RA than TNF inhibitors (or at least adalimumab), and this may also correspond to improved fatigue.49 51 Not all RA treatment trials show superiority with respect to fatigue as an outcome and some individuals will respond better to one treatment than another, so there are no strong predictors with respect to who will have a marked improvement in fatigue when treating active RA.
Non-pharmacologic treatment of fatigue in RA
The age of the patient with RA does not seem to affect the choice of non-pharmacologic treatment for improving fatigue in RA, so similar strategies for treating fatigue may be applicable to all adults with RA.55
Physical activity and psychological interventions are effective in reducing fatigue in RA.56 A Cochrane meta-analysis of RCT of nonpharmacological interventions in RA patients with fatigue analysed six trials, with 388 patients showing physical activity improved fatigue by a difference of 14 points on a 0 to 100 fatigue scale compared with controls.56 The number needed to treat to have a beneficial effect was 7.56 Another systematic review compared trials using the minimal important difference and it also showed that aerobic exercise was effective in reducing fatigue, but most participants would not achieve a clinically relevant improvement in fatigue.57 It was shown that providing pedometers with or without providing step targets was helpful in increasing physical activity in RA with a small reduction in fatigue.58 The effect size of most physical activity interventions for fatigue improvement in RA is small.
Older patients with RA (>65 years) were compared with respect to changes in fatigue between a 20-week moderate-intensity to high-intensity exercise at a gym with supervision, or exercise of light intensity at home. Exercise did not improve fatigue rated by a VAS. However, using the Multidimensional Fatigue Inventory (MFI-20), both physical and mental fatigue improved more in the moderate-intensity to high-intensity group at the gym.59 We do not know if the improvements would be sustained after the programme ended nor if it was the socialisation/attention that improved fatigue versus the actual exercise.
In RA, it is uncertain what exercise to recommend to patients with high fatigue and whether supervision has ‘added-value’. Patients with RA who were in an exercise trial felt that physical activity was important for coping with fatigue.60 Time with a physiotherapist guiding a personalised exercise programme was also important. Of course, patients who agreed to be interviewed had already participated in a trial, so the sample could be biased in favour of exercise.
In one study, a comprehensive exercise programme to improve fatigue in RA consisted of seven sessions with a physiotherapist who provided handouts, discussed the benefits of exercise (in general and disease specific), demonstrated exercises and equipment and allowed patients to choose exercises with supervision. Patients completed an activity diary, set goals and had graded exercises. They re-evaluated their goals over the programme and learnt pacing, stress reduction and relaxation techniques and weight reduction.61 Interestingly, motivational counselling followed by text message reminders to improve physical activity improved pain. There was sustained increased exercising 18 months after the intervention.62 Fatigue reduced by 12 mm on a 100 mm VAS which was a small difference but clinically relevant.
RCTs of weight loss in RA are sparse. Obesity is common and is a risk factor for RA. In ERA, one-third of patients are at ideal weight, one-third are overweight and one-third are obese.63 Studies in psoriatic arthritis have demonstrated that weight reduction improves disease activity.64 Dietary manipulation to provide improvement in pain in RA and weight reduction has been studied, but studies are small with a high risk of bias and do not provide definitive data on improving disease activity or fatigue.65
Thirteen trials of psychosocial interventions in RA studied a total of 1579 patients. The mean difference in fatigue between the treatment and control groups was 10 (on a 0 to 100 scale) with an NNT of 10. The overall quality of the trials was low; and the effect size was modest at best.56 A very large RCT was published using a cognitive-behavioural approach to decrease fatigue in RA over 2 years (Reducing Arthritis Fatigue Trial).66 Fatigue had to be at least six out of 10 to be enrolled in the trial. For the group randomised to cognitive-behavioural approach, seven sessions were given by trained rheumatology occupational therapists and nurses. Whereas the control group received a usual care booklet. There were 333 randomised, of whom 93% completed outcomes at 26 weeks. A small improvement in the active (cognitive-behavioural) treatment group that persisted to 2 years was observed, including the impact of fatigue and self-efficacy. Satisfaction with the intervention was higher in active treatment (89%) vs controls (54%). The minimal clinically important difference in RA for change within a fatigue scale is likely to be at least 10%. The control group changed by 12% and the cognitive-behavioural group by 19%, so the between-group difference was very small. The rating of fatigue, unfortunately, was not different between the groups, but coping with fatigue was better in the intervention group.
Other studies in the Cochrane review were either negative or not analyzable for fatigue, including one trial each of herbal treatment, omega-3 fatty acid supplementation, a Mediterranean diet, reflexology and the use of Health Tracker information (one large trial with 714 participants).56
Theoretically, improving sleep quality can help fatigue. Patients with RA who have a lower quality of sleep have more fatigue.67
Maintaining ability to work
Patients with RA who maintained their ability to work had less fatigue compared to those who were work disabled, and these differences seemed related to better mental health, not physical health.68 However, other factors are likely related to an ability to work, which may not have been measured, where both fatigue and work disability are a consequence of joint damage, age, type of job, less flexibility at work and so on. A prospective study is needed to determine if a programme that keeps people in the workplace will improve fatigue.
Behavioural interventions
A 12-month-long self-management programme delivered via the internet did not improve pain or fatigue compared with standard of care treatment in an RCT of 157 patients with RA.69
Vitamins and supplements
In RA patients who are vitamin D deficient, there does not appear to be clinically relevant improvements in RA with vitamin D supplementation, even though function and inflammatory markers slightly improved.70 A systematic review showed that vitamin D had no improvement in fatigue.56 This is contrary to systemic lupus erythematosus (SLE), where data suggest that vitamin D supplementation may improve fatigue.71
Omega 3 supplementation or fish oil has some positive RCTs in active RA improving disease activity when added to standard of care.72 73 However, the effects on fatigue are uncertain.
It seems that social support, hope, optimism and resilience improve fatigue.74 Perhaps ways at improving resilience and social support can also help people with RA who have significant fatigue. There are no RCTs.
Ineffective strategies for improving fatigue in RA
Tight control alone does not fully improve fatigue. At 12 months, 43% of RA patients experienced ongoing fatigue in a treat to target strategy study. Nearly one in four who were fatigued at the onset of the study showed lower levels of fatigue by 1 year, but one in six of the patients who were not initially fatigued recorded increased fatigue.30
Treatment of anaemia should theoretically improve fatigue. RA can cause anaemia of chronic disease. A Cochrane review of erythropoietin for anaemia in RA did improve patient global assessment, but the results for fatigue were not provided or inconsistent.75
An RCT of morphine and naloxone studied pain in various conditions including RA. Active treatment was comparable with placebo.76 An RCT of tetrahydrocannabinol (THC) for treating chronic pain in RA and ankylosing spondylitis is ongoing, and outcomes will include pain and fatigue.77 The design is innovative as cannabidiol (CBD) nonresponders will have THC added to their treatment after 12 weeks.
SUMMARY
In conclusion, fatigue in RA is due to multiple factors and only partially from disease activity. The treatment of active RA can improve fatigue somewhat. Many predictors such as high pain, multimorbidity, obesity, personality factors and depressed mood increase the likelihood of fatigue. Other reviews have provided insights into the effects of pain and psychological factors on fatigue in RA.78 79
Treatment of fatigue is difficult with some positive data for exercise, CBT and some self-management programmes with reminders. In general, treatment effects in RCTs of fatigue in RA are small. It is unknown if weight loss can improve fatigue, but dietary changes have not resulted in positive results. There are multiple natural herbals and other vitamins and minerals that claim to help fatigue in chronic disease (and have multimillion dollars of sales), but lack RCT ‘proof’. More research is needed to find an effective treatment of fatigue after disease activity is controlled. Until then, fatigue will have a negative impact on many people living with RA.80
REFERENCES
Footnotes
Contributors JEP performed the literature search, writing of the paper and formed the opinions presented.
Competing interests AbbVie, Actelion, Amgen, Bayer, BMS, Emerald, Genzyme, Janssen, Lilly, Merck, Novartis, Pfizer, Roche, Sandoz, Sanofi, UCB; RCTs: Bayer, BMS, Merck, Roche, Seattle Genetics, UCB.
Patient consent for publication Not required.
Ethical approval There was no ethics approval as this is a review article.
Provenance and peer review Commissioned; externally peer reviewed.