Article Text

Abstract
Rheumatoid arthritis (RA) is associated with a significant disease burden and high costs for society. Because the disease has identifiable preclinical stages, screening and prevention have become a possibility in RA. Anticitrullinated peptide antibodies (ACPAs) are arguably the most likely candidate biomarker to screen for RA. This paper reviews the evidence for the use of ACPAs as a screening test in the broader general population, to identify individuals at high risk of subsequent onset of RA. We will review the diagnostic properties of the test and its positive and negative predictive value in different settings. We will discuss how ACPA testing could effectively be integrated in a broader screening strategy for RA.
- rheumatoid arthritis
- health services research
- Anti-CCP
- autoantibodies
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Key messages
What is already known about this subject?
Autoantibodies associated with rheumatoid arthritis (RA), including anticitrullinated peptide antibodies (ACPAs), precede the onset of RA by several years.
Only if preventive intervention demonstrate efficacy in reducing the incidence of subsequent onset of RA, is screening for RA warranted.
Although cumulative evidence suggest a direct involvement of ACPA in the pathogenesis of RA itself, more extensive and rigorous experiments are needed.
How might this impact on clinical practice?
While the diagnostic properties of ACPAs are good, the test still has low positive predictive value when applied to the general population or when the prevalence of the disease is low.
Background
Screening for a disease is intimately linked to the concept of prevention. Some have even argued that screening for a disease might be unethical if patients cannot be offered preventive treatment.1 2 Once viewed as an unavoidably damaging disease, rheumatoid arthritis (RA) has recently become a potentially curable disease. Based on data from animal models and limited clinical evidence in RA, the existence of a critical period is proposed, a ‘therapeutic window of opportunity’, during which antirheumatic therapy may be capable of modifying the disease permanently or preventing it altogether.3–7 Several trials are currently exploring the impact of early, aggressive use of disease-modifying antirheumatic drugs (DMARDs) in preclinical RA. DMARDs such as abatacept, rituximab, methotrexate, methylprednisolone or hydroxychloroquine have/are being tested in individuals who do not have yet developed classifiable RA.8–17 Most preventive trials in RA have focused on secondary prevention in patients with recent onset, undifferentiated arthritis. Only few studies have explored the impact of early DMARD therapy in subjects with arthralgias, prior to clinical arthritis, or even subjects with only biomarkers for RA, the so-called ‘autoimmunity associated with RA’ phase.18
WHO has established guidelines for screening and preventive interventions.19 If RA screening and prevention is to gain acceptance, it will have to meet specific criteria established by public health agencies.7 At present, only one musculoskeletal disease meets these requirements. In osteoporosis, screening of individuals at high risk and treating patients with low bone density have demonstrated benefits. WHO general guidelines recommend among others pursuing screening only for diseases that represent a significant disease burden for society, and diseases that have an identifiable preclinical stage.19 Another prerequisite is the ability to predict an individual’s risk of disease adequately and access to an effective treatment to prevent the development of the condition.19 RA certainly qualifies for a number of these conditions. Markers of early phases of RA exist and can be used before the clinical onset of disease. Studies in healthy blood donors have shown that the presence of autoantibodies, such as anticitrulinated peptide antibodies (ACPAs), precedes the onset of RA by several years.20–23 Almost all completed or ongoing preventive trials have used the presence of ACPA as one of their inclusion criteria. One could argue that widespread autoantibody screening makes little sense before a preventive intervention has demonstrated its ability to reduce the incidence of RA. However, even before any pharmacological intervention demonstrates efficacy in preventing RA development, one can claim that there is currently already enough evidence to recommend specific lifestyle modifications in individuals at high risk for the disease.24 The question we will be exploring in this review is whether ACPA could be used as a screening test in a broader general population or primary care setting to identify individuals who could benefit from a preventive intervention.
A brief history of ACPAs
The history of ACPA started in 1964 when Nienhuis et al reported antiperinuclear factor (APF), an antibody against human keratohyalin granules of buccal mucosa cells in the serum of patients with RA.25 Fifteen years later, antikeratin antibodies (AKA) were identified by Young et al, displaying a high specificity for RA.26 Both APF and AKA were then found to belong to a family of autoantibodies directed against citrullinated filaggrin peptides.27–29 Over the years, other citrullinated peptides were identified, such as vimentin, fibrin, fibrinogen and α-enolase.30–32 In 2013, van Beers et al used the term ‘citrullinome’ to refer to the various citrullinated proteins (n=53 in all) identified in the sera and the synovial fluid of patients with RA.33 Citrulline is a non-standard amino acid generated by the post-translational modification of arginine by peptidylarginine deiminase enzymes, in a calcium-dependant process called citrullination.34 It occurs naturally in cell differentiation, inflammatory responses, cell apoptosis, keratinisation, gene regulation and ageing process. The citrullination causes loss basic charges, which can influence the protein structure and promote the generation of neoantigens and in turn an autoimmune response.34 Abnormal citrullination of various peptides is observed in RA, but also in other human diseases, including Alzheimer’s disease, psoriasis, systemic lupus erythematosus, primary biliary cirrhosis and multiple sclerosis.35 36 However, the development of systemic ACPAs seems to be highly specific for RA, while the significance of ACAPs in other conditions is still unclear.37
The first available ACPA test (first generation or anti-CCP1), based on the ELISA method, was developed by Eurodiagnostica in 2000 using a cyclic citrullinated peptide (CCP) derived from human filaggrin.38 Synthetic peptide libraries were then screened to select better epitopes, to improve diagnostic accuracy.39 In 2002, a second generation cyclic citrullinated peptide (CCP2) assay was introduced by Eurodiagnostica and has been widely used as routine test for ACPAs in RA. Multiple versions of anti-CCP2 kits are available from various manufacturers (Eurodiagnostica, Inova diagnostics, Axis-Shield, Euroimmun, Phadia, etc.), with slightly different features and diagnostic accuracy for RA.40 CCP3 (third generation CCP) assays were later developed and based on additional epitopes, not present in the CCP2 antigen sequence.41 Despite some controversy in the literature, there is no clear evidence for superiority of the CCP3 compared with the CCP2 assay. However, it seems that CCP2 may be more specific in established patients with RA, whereas CCP3 may have a higher predictive value for RA development in subjects with undifferentiated inflammatory arthritis.42 Several alternative methods for detecting ACPA have been developed, including assays based on citrullinated proteins instead of peptides, such as mutated citrullinated vimentin (Orgentec), filaggrin (CPA; Genesis) or a viral citrullinated peptide, but none is widely used in routine diagnosis of RA. Bead-based chemiluminescent immunoassays have been recently developed to quantify ACPAs and may potentially improve the sensitivity due to the larger surface binding area of the bead-based assay.43
The potential biological functions of ACPAs
Even though citrullination is a common biological phenomenon, and the secretion of IgA-ACPAs occurs physiologically at mucosal sites, the development of a systemic antibody response against citrullinated peptides is fairly specific for RA. The reasons for the specificity of systemic ACPAs in RA are not completely understood, but suggest a potential role of these autoantibodies in the pathophysiological processes leading to the development of RA, but it is also possible that ACPAs just represent a bystander phenomenon.
The generation of ACPA starts in early developmental phases of RA and ACPAs are strongly predictive for the progression to established RA. Some evidence suggest that genetic (eg, the shared epitope) and environmental risk factors (eg, tobacco smoke) act in concert to increase the formation of citrullinated proteins, to promote their presentation to the immune system, to break the tolerance towards these antigens and lead to the development of ACPA.44 Interestingly, these autoantibodies are transformed over the period of time, from their systemic appearance up to RA onset, with both qualitative and quantitative changes, extensive diversification, increased avidity, new isotypes and acquisition of specific agalactosylation and core fucosylation profiles.45 Several investigations have suggested mechanisms by which ACPA may be directly pathogenic in RA.46 One potential mechanism relates to the ability of ACPA to form immune complexes (IC) that can activate inflammatory cells. The effector functions of ACPA containing IC can be enhanced by the concomitant presence of rheumatoid factor (RF), suggesting a potential synergetic role of ACPA and RF, clinically linked to a more severe arthritis.47–49 Another mechanism by which ACPA may interfere in RA pathogenesis could be via the stimulation of neutrophil extracellular traps formation, a phenomenon that externalises citrullinated autoantigens and immunostimulatory molecules, leading to a perpetuation of inflammation and autoimmunisation processes in RA.50 Another mechanism proposed for ACPAs suggests that these antibodies function as agonists for a receptor-mediated cell response and directly induce both pain and osteoclastogenesis.51 52 However, more data are needed to support the finding of direct binding of ACPAs to molecules expressed on the surface of osteoclasts.53
While several authors have proposed a direct pathogenic role of ACPAs, it is also possible that these autoantibodies just reflect pathogenic cellular and humoral activity leading to the development of RA, but without affecting directly joint inflammation. In other terms, ACPA could be innocent bystanders, generated by the biological processes characteristic of the disease. Toes and Pisetsky have recently drafted several recommendations to define with more experimental rigour the potential pathogenic activity of either polyclonal or monoclonal antibodies.53 Although ACPAs are highly cross reactive and bind a large variety of citrullinated proteins, their primary antigenic target relevant to RA and its precise tissue site are unknown.
Screening, case finding and diagnosis
Conceptually, screening needs to be distinguished from case finding and from diagnosis. The principal aim of screening is to detect potential early signs of disease in a large, generally asymptomatic, population. The principal aim of case finding is to search systematically for undiagnosed early disease in groups at increased risk for the disease.54 The principal aim of diagnosis is to establish the presence or absence of disease in symptomatic individuals. The characteristic of tests will need to be tailored for its primary use. A screening test needs to be inexpensive and easy to perform to be acceptable to a healthy population, and will generally favour sensitivity over specificity in order not to miss potential cases.19 On the contrary, a diagnostic test may be more invasive and more expensive in order to establish disease, and tends to favour specificity over sensitivity.
ACPAs as a diagnostic test
What makes a good diagnostic test? First, the biomarker should have good sensitivity, which means correctly being positive (above the threshold) in patients with the disease. Second, the biomarker should also have good specificity, meaning correctly being negative (below the threshold) in people without the disease. Furthermore, the test needs to provide good positive and negative predictive values (PPV and NPV). PPV estimates the probability for a person having a positive test, to really have the disease, while NPV estimates the probability for a person having a negative test, to actually not have the disease. However, even tests with very good sensitivity and specificity may not provide good predictive values, because the predictive value depends on the sensitivity and the specificity of a diagnostic test, and on the probability of the disease in the population. The mathematical link among sensitivity, specificity, prevalence and predictive values, often called Bayes’ theorem, is not always well-understood by physicians.55 Indeed, more than 80% of physicians did not correctly take into account the prevalence when asked to estimate the predictive ability of a given test.
Two scenarios may illustrate the differential value of ACPA testing in diagnosing RA in patients with recent-onset undifferentiated arthritis56: (1) A young male with a 2-month history of arthritis of both knees, some morning stiffness, no RF and slightly raised C reactive protein (<50 mg/L) has little risk for RA within the next year (estimated probability between 0% and 6%).57 Even if this patient had a positive ACPA test, it would not increase substantially his risk of developing RA (estimated post-test probability, ~7%).57 (2) On the other side of the spectrum, a mid-aged woman with a 2-month history of painful and swollen metacarpophalangeal joints of a single hand, some morning stiffness, no RF and slightly raised C reactive protein level (<50 mg/L) has a risk of developing RA within the next year of approximately 26%.57 If this patient had a positive-ACPA test, her risk of having RA would climb to 67%.57 These scenarios illustrate a major consequence of Bayes’ theorem: the value of a positive ACPA test depends decisively on the a priori likelihood of RA.56
While ACPAs have a higher specificity than the RF,58 the sensitivity and specificity of ACPAs for RA remain far from perfect.59 A meta-analysis of the diagnostic performance of ACPAs in established RA combined 37 studies and found a pooled sensitivity of 67% (95% CI 65% to 68%) and a pooled specificity of 95% (95% CI 95% to 96%).58 The limited sensitivity of the test can be explained by the fact that not all patients with RA seem to have autoantibodies (‘seronegative disease’), even if in some of the patients with ACPA-negative RA have other autoantibodies. The limited specificity of ACPAs can be explained by the fact that these antibodies also occur in other conditions, such as periodontal disease,60 61 chronic lung diseases62 or other autoimmune diseases.63
ACPAs as a screening test
ACPAs are present in 0.8% of Caucasians without RA64 and in 1.7% of Asians without known autoimmune disease.65 Several factors are known to be associated with the presence of ACPA, such as older age, in particular for women where the perimenopausal period seems to be associated with an increased prevalence,66 tobacco smoking and undifferentiated joint complaints.
The predictive value of ACPA testing will differ when applied as a screening tool in an asymptomatic general patient population from when it is applied as a diagnostic tool, because the pretest probability of RA will be much lower (figure 1). Let us illustrate this with a real-world example: screening for ACPA positivity was performed in large population representative cohort from Sweden of over 12 000 individuals.59 After excluding patients already known to have established RA, 247 participants tested ACPA positive (2%). Of these, 21 developed incident RA within the next 3 years, which results in a PPV of less than 9%.59 While it can be argued that a follow-up period of 3 years might be insufficient, the results remain clearly disappointing and do not support using ACPA indiscriminately in the general population.
{kind=link}
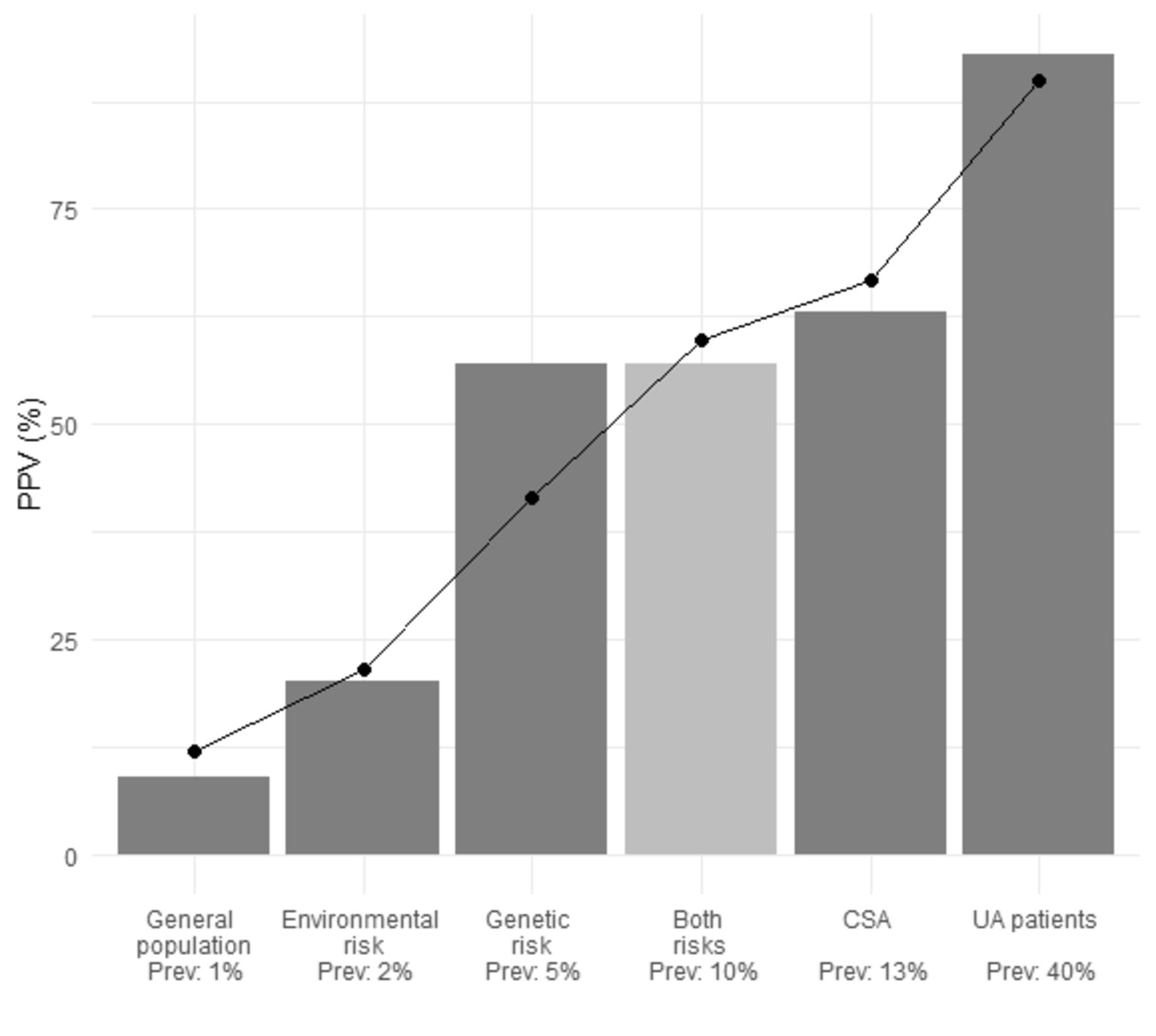
Positive predictive value (PPV) of anticitrulinated peptide antibody (ACPA) testing in different at risk populations: hypothetical and reported predictive ability by incidence rates of rheumatoid arthritis (RA). The PPV of ACPAs testing increases in populations at higher a priori risk for the disease. The line displays the hypothetical PPV based on the established diagnostic properties of ACPA, with a specificity of 67% and a sensitivity of 95%.58 The barchart displays actual PPV reported in various at risk populations with different incidence rates of RA.59 68 91 92 CSA, clinically suspect arthralgia patients; UA, undifferentiated arthritis.
While using ACPA as a screening tool in the general population does not make much sense because of insufficient PPV, it could add up in a population at higher baseline risk of developing RA. Several of such at risk groups have been identified. For example, in individuals genetically at increased risk for RA, such as family members of patients who have an autoimmune disease or individuals of an ethnic group known to have a high prevalence of RA. Thus, the PPV for RA at 5 years for a positive ACPA test was 58% in first degree relatives of patients with RA,67 and the PPV for RA at 5 years was 56% in a particular indigenous American Indian tribe.68 While the PPV for RA in these individuals at risk for RA may vary substantially depending on the strength of the genetic risk or the prevalence of other conditions known to promote the production of ACPAs,60–63 the PPV of ACPAs is overall substantially better when screening populations at higher a priori risk for the disease (figure 1). Other at risk populations warranting screening could be groups exposed to specific environmental risk factors of RA or having specific comorbidities that put them at higher risk. Examples of environmental risk factors increasing the likelihood of RA are, for example, obesity, tobacco smoking or other inhaled pollutants, certain nutritional habits; viral infections have also been suggested to increase the odds of developing the disease.69–72 Hormonal factors such as the rapid decline in ovarian function at menopause or after a total hysterectomy have been proposed as a condition warranting screening for autoimmunity.66 Other autoimmune comorbidities, such as autoimmune thyroiditis, have been demonstrated to increase the risk of RA and may justify regular screening for RA.73 Chronic periodontitis, chronic interstitial lung disease or chronic diarrhoea have also been proposed as comorbid conditions increasing the risk for future RA.60–62 74 75 In order to integrate the different risk factors, clinical prediction rules have been developed to estimate the risk of progression to RA.76 Some prediction rules are solely on easily ascertained lifestyle factors77; others have combined family history, genetic markers, serological markers and environmental factors, with a good discriminative ability.78–81 Validated prediction rules may be useful to select at-risk populations with a higher likelihood of developing RA prior to ACPA screening.
Another approach to increase the predictive value of ACPAs could be to enhance the diagnostic performances of the test to better suit the needs of screening. Some have modified the cut-off level and used higher titters of ACPAs, or have required multiple ACPA reactivity’s (called ‘fine-specificity ACPAs’).59 Other have proposed to combine ACPAs with additional biomarkers to increase its specificity or its sensitivity, for example, when both RF and ACPA are present, the specificity for future RA appears to be close to 100%.23 The discriminative power of ACPAs may be improved by combining other putative biomarkers, such as genetic markers,82 highly sensitive C reactive protein,83 cytokine and chemokine profiles,84 and other autoantibodies,22 85 in combination or in series.56 86 Still others have proposed to add imaging modalities, such as MRI or articular ultrasound.87 88 but the optimal combination of biomarkers and imaging tests to predict future development of RA has not yet been established.
WHO also recommends to consider the cost effectiveness of screening, to weigh the costs involved in identifying a case against the global medical expenditure in a particular setting.19 Unfortunately, combining several biomarkers or imaging modalities is likely to decrease the cost effectiveness of screening for RA and should probably be reserved for diagnosis rather than for screening strategies. Liang et al have proposed that screening and case finding may be realistically and cost effectively accomplished in a fairly infrequent condition, such as RA, by a serial testing strategy.54 He proposed to start screening with an inexpensive, sensitive test to prescreen individuals, which could involve an internet questionnaire or a prediction rule.54 Individual’s testing positive would be proposed increasingly more specific tests, which includes ACPAs, and ultimately, a medical assessment for diagnosis and confirmation.
Conclusions
Given the low prevalence of RA or of preclinical phases of RA in the general population, in this setting ACPAs are probably not an adequate screening tool in isolation. In an unselected general population and as a first-line screening tool, ACPAs have insufficient PPV, result in a high number of false-positive tests and generate unjustifiable medical costs. As the rheumatological community is starting to discuss the risks of overdiagnosis and overtreatment,89 90 other means for the initial screening of RA should be considered. Taking advantage of the well-established risk factors of the disease, using validated prediction rules or internet-based techniques could be an attractive option to preselect a population with a higher pretest probability of RA, warranting ACPA testing.54 ACPA testing is an effective diagnostic tool and useful for RA case finding in selected at risk populations.
References
Footnotes
Collaborators Recherche clinique en rhumatismes inflammatoires: O. Studer, E. Trunk, B. Gilbert.
Contributors All authors have seen and approved the final manuscript and contributed significantly to this work (meet criteria for authorship).
Funding Study was funded by Fondation Jean et Linette Warnery.
Competing interests The author’s institution has a scientific collaboration with Inova and Thermofisher, 2 producers of ACPA tests. The research collaboration is scientific and does not involve any monetary compensation or other kind of benefits.
Patient consent for publication Not required.
Provenance and peer review Commissioned; externally peer reviewed.
Data availability statement No additional data are available.