Article Text

Abstract
Background Biologic disease-modifying antirheumatic drugs (bDMARDs) and targeted synthetic DMARDs are used in patients with psoriatic arthritis (PsA), but few studies directly compare their clinical efficacy. In such situations, network meta-analysis (NMA) can inform evidence-based decision-making.
Objective To evaluate the comparative efficacy and safety of approved bDMARDs in patients with PsA.
Methods Bayesian NMA was conducted to compare the clinical efficacy of bDMARDs at weeks 12‒16 in bDMARD-naïve patients with PsA in terms of American College of Rheumatology (ACR) criteria, Psoriatic Arthritis Response Criteria (PsARC) and Psoriasis Area and Severity Index (PASI). Safety end points were evaluated in the overall mixed population of bDMARD-naive and bDMARD-experienced patients.
Results For ACR, all treatments except abatacept were statistically superior to placebo. Infliximab was most effective, followed by golimumab and etanercept, which were statistically superior to most other treatments. Ixekizumab 80 mg every 2 weeks (Q2W) was statistically superior to abatacept subcutaneous, apremilast and both regimens of ustekinumab; similar findings were observed for ixekizumab 80 mg Q4W. For PsARC response, ixekizumab did not significantly differ from other therapies, except for golimumab, infliximab and etanercept, which were superior to most other agents including ixekizumab. For PASI response, infliximab was numerically most effective, but was not statistically superior to ixekizumab, which was the next best performing agent. Analysis of safety end points identified few differences between treatments.
Conclusion Our NMA confirms the efficacy and acceptable safety profile of bDMARDs in patients with active PsA. There were generally few statistically significant differences between most treatments.
- psoriatic arthritis
- DMARDs (biologic)
- DMARDs (synthetic)
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Key messages
What is already known about this subject?
In several network meta-analyses (NMAs) in patients with psoriatic arthritis (PsA), biologic disease-modifying antirheumatic drugs (bDMARDs) and targeted synthetic DMARDs have demonstrated superiority to placebo (ie, American College of Rheumatology criteria, Psoriatic Arthritis Response Criteria and Psoriasis Area and Severity Index).
These NMAs have shown relatively few or no statistically significant differences between bDMARDs.
Findings of the present NMA concur with the results of a recent head-to-head study comparing ixekizumab with adalimumab.
What does this study add?
Few NMAs of bDMARDs in PsA include ixekizumab, a high-affinity monoclonal antibody that selectively targets interleukin 17A.
The current NMA compares a wide range of bDMARDs and targeted synthetic DMARDs, including ixekizumab.
How might this impact on clinical practice?
Head-to-head comparative clinical trials in PsA are limited; therefore, the results of our comprehensive NMA can inform evidence-based decision-making in clinical practice.
Introduction
Psoriatic arthritis (PsA) is a chronic inflammatory rheumatic disease that affects ≈0.25% of the population.1 PsA is characterised by pain, stiffness, swollen joints, joint erosion and bone formation, and psoriasis is a common concomitant condition.1 2 PsA is also associated with reduced quality of life and substantial healthcare resource use and costs.3 4
A number of biologic disease-modifying antirheumatic drugs (bDMARDs) are approved for the treatment of PsA, including tumour necrosis factor (TNF)-α inhibitors (adalimumab, etanercept, infliximab, golimumab and certolizumab pegol), interleukin (IL) antagonists (ustekinumab, secukinumab and ixekizumab) and the immunosuppressant abatacept. Apremilast, an oral phosphodiesterase inhibitor, and tofacitinib, an oral Janus kinase inhibitor, are also available. In addition, newer IL-23 antagonists, such as guselkumab and risankizumab, are undergoing phase 3 trials for PsA.
Patients with active PsA are commonly treated with bDMARDs, but there are few studies directly comparing the clinical efficacy of these drugs. While there is extensive experience in clinical practice with TNF-α inhibitors, limited insights exist as to the relative performance versus therapies with a different mechanism of action. A head-to-head (H2H) study of ixekizumab versus adalimumab was successfully completed at the end of 2018, providing direct comparative efficacy in key outcomes.5 When data from H2H clinical trials comparing agents are limited, network meta-analyses (NMAs) are often used to inform evidence-based decision-making. NMAs expand the scope of traditional pairwise indirect comparisons by combining direct and indirect evidence.6 Thus, NMAs estimate the relative efficacy of each treatment within a network of treatments and build on the principles of indirect comparisons while upholding trial randomisation.7–9
The objective of this study was to conduct a systematic literature review (SLR) and use NMA to evaluate the relative efficacy of bDMARDs approved by the European Medicines Agency (as of July 2018) on joint and skin symptoms, as assessed by American College of Rheumatology (ACR) criteria, Psoriatic Arthritis Response Criteria (PsARC) and Psoriasis Area and Severity Index (PASI), in patients with PsA. Various safety end points were also evaluated, including treatment-emergent adverse events (TEAEs), serious/severe adverse events (SAEs), discontinuation due to adverse events and all-cause discontinuation. Although recent NMAs have been conducted comparing bDMARDs in PsA,10–14 few include ixekizumab, a recently approved high-affinity monoclonal antibody that selectively targets IL-17A.15 In addition, publication and dissemination of NMA results are essential activities to support international health technology assessments of ixekizumab in PsA.
Methods
An SLR was conducted to identify relevant trials with bDMARDs in patients with PsA, and these trial data were synthesised, via Bayesian NMA, to estimate the relative efficacy of the biologics primarily in those who had not previously received bDMARD therapy (ie, those who were naïve to anti-TNF therapy or to any bDMARD (anti-TNF or IL antagonist)) and to compare safety end points in the overall population.
Literature review
Eligibility criteria for the SLR were defined in terms of the PICOS structure (population, interventions, comparisons, outcomes and study design). The SLR was conducted according to the preferred reporting items for systematic reviews and meta-analyses (PRISMA) requirements.16 The process and overall conduct of the SLR were based on the Cochrane Handbook for Systematic Reviews of Interventions.17
Randomised placebo-controlled studies or any other controlled trials assessing the comparative efficacy of bDMARDs and targeted synthetic DMARDs in adult patients with active PsA were identified by conducting structured literature searches (from 1990 to July 2018) of various databases as well as a review of grey literature. The following databases were searched via OVID: EMBASE, MEDLINE, Cochrane Central Register of Controlled Trials and Evidence-Based Medicine Reviews. The therapies of interest included abatacept, adalimumab, apremilast, certolizumab pegol, etanercept, golimumab, infliximab, ixekizumab, secukinumab, tofacitinib and ustekinumab. Efficacy and safety outcomes are described in the subsection on data extraction and outcomes. Details regarding the search strategies used for each database are available on request.
In addition to the database searches, manual searches of grey literature were conducted in the WHO International Clinical Trials Registry Platform, ClinicalTrials.gov and conference proceedings of relevant conferences for the previous 2 years. Recent SLRs in PsA were also reviewed to ensure that all relevant trials were captured.
Study selection
PICOS eligibility criteria for the SLR included randomised placebo-controlled trials, long-term extensions of these trials or any other controlled trials assessing the comparative efficacy and safety of the previously noted interventions of interest for the treatment of adult patients (≥18 years of age) with active PsA. Clinical efficacy and safety outcomes of interest are described in the following subsection. Only studies in English were included. Comparators could be placebo, best supportive care, any other intervention of interest, conventional DMARDs or other non-biologic approved treatments. Studies were excluded if they did not meet the PICOS criteria, such as observational studies and single-arm non-comparative studies not considered extensions of randomised controlled trials.
After removal of duplicate records, two researchers independently reviewed the titles and abstracts of the remaining publications and reviewed the relevant full-text articles. Any discrepancies around inclusion of articles or data extraction were resolved by involving a senior reviewer to reach a consensus.
Data extraction and outcomes
Relevant data points were extracted for a range of parameters, including study interventions and dosage regimens, sample size, demographic details, time of treatment assessment and the main outcomes of interest. Efficacy end points included ACR response rates (ACR20, ACR50 and ACR70, defined as a minimum of 20%, 50% and 70% improvement from baseline in the ACR score),18 PsARC response (defined as improvement from baseline in two of four criteria, one of which must be joint count, without worsening in any measure)19 20 and PASI response rates (PASI50, PASI75, PASI90 and PASI100, defined as 50%, 75%, 90% and 100% reduction from baseline in PASI score).21 Safety end points were evaluated at study end point in the overall population of bDMARD-naïve and bDMARD-experienced patients and included: (1) at least one TEAE; (2) at least one SAE; (3) at least one adverse event leading to discontinuation (DAE) and (4) all-cause discontinuation (ie, withdrawal for any reason, including withdrawals from treatment due to lack of efficacy or DAE).
Study quality assessment
The validity of each study was assessed using the risk of bias instrument, which is endorsed by the Cochrane Collaboration.17 In addition to the Cochrane risk of bias assessment, the quality of more recent publications identified in updated searches was assessed using the UK National Institute for Health and Care Excellence (NICE) methodology checklist.22
NMA methodology
The methodology used for the NMA followed NICE guidelines.23 For the main analysis of clinical efficacy, Bayesian NMA focused on bDMARD-naïve patients and was conducted to compare the relative efficacy of bDMARDs approved in Europe and administered according to their licensed dosage regimens (EU labelling) for PsA. The focus was on bDMARD-naïve patients, in part, because of the potential clinical benefits of earlier treatment,24 which could lead to newer drugs being increasingly used in a first-line setting. In addition, various definitions of bDMARD-experienced patients have been used in clinical trials, ranging from a stringent approach, such as documented TNF intolerance and/or inadequate response, to a more flexible one, such as recent treatment with a TNF during a specified time period. This creates some heterogeneity in the networks, especially in the context of a limited number of studies. In contrast, focusing on bDMARD-naïve patients provides networks that are more homogeneous in terms of patient population and more comprehensive in terms of number of studies. Analyses were also conducted in bDMARD-experienced patients and in the overall population of PsA patients; however, in the interest of brevity, results are presented only for a sensitivity analysis using week 24 data for the overall population of bDMARD-naïve and bDMARD-experienced patients. For the same reason, some additional outcomes that were evaluated (eg, DAS28) are also not reported or are provided as supplementary material (number needed to treat for ACR and PASI response, which are appreciated as useful guidance in clinical practice for the assessment of relative drug performance and are reported to be frequently used in local decision-making25 (online supplementary tables 1 and 2)). Active treatments included in the NMA are provided in table 1 (placebo was also included). For some bDMARDs (abatacept, apremilast, certolizumab pegol and secukinumab), if a study did not report data specifically in bDMARD-naïve patients, data for the full population were used in the NMA. For the primary analysis, relative efficacy for all end points was estimated based on results reported at 12 weeks where available. Otherwise, data relating to the closest time point after 12 weeks were used, up to a maximum of 16 weeks, which is in line with NICE reimbursement criteria in the UK. In addition, a sensitivity analysis was conducted at 24 weeks. For efficacy data, Bayesian network meta-regressions were also performed to control for baseline risk using the methods of NICE.23
Supplemental material
Supplemental material
Biologic and targeted synthetic disease-modifying antirheumatic drugs included in the network meta-analyses (all agents administered as per EU labelling)
The Bayesian analyses were performed in JAGS via R using the R2JAGS package. With respect to statistical methods, a multinomial model with a probit link was used for ordered categorical data (ACR and PASI), whereas a binomial model with a logit link was used for binomial event data (PsARC response and safety). Models were fitted using three chains and uninformative priors, and convergence diagnostics were checked. Both random-effects and fixed-effects models were run for the network, and the Deviance Information Criterion (DIC) was used to assess which model fit the data better. For results presented on a scale that requires a baseline for calculation, a meta-analysis estimate of the placebo arm effect across the placebo-controlled trials was used. Placebo was used as the reference treatment when performing Bayesian network meta-regressions, so that the interaction was assumed to act on the relative comparisons between each treatment in the network and placebo. A common interaction term across treatments was assumed.26
Results from the Bayesian analysis are presented as a point estimate (posterior median) and 95% credible interval (95% CrI). A 95% CrI can be interpreted as a 95% probability that the true treatment effect lies within the interval. If the 95% CrI excludes no difference (0 for continuous outcomes or 1 for binary outcomes), there is a >95% probability that the two treatments are different, which is analogous to a p value of <0.05, and referred to as statistically significant in the interpretation.
Results
Systematic literature review
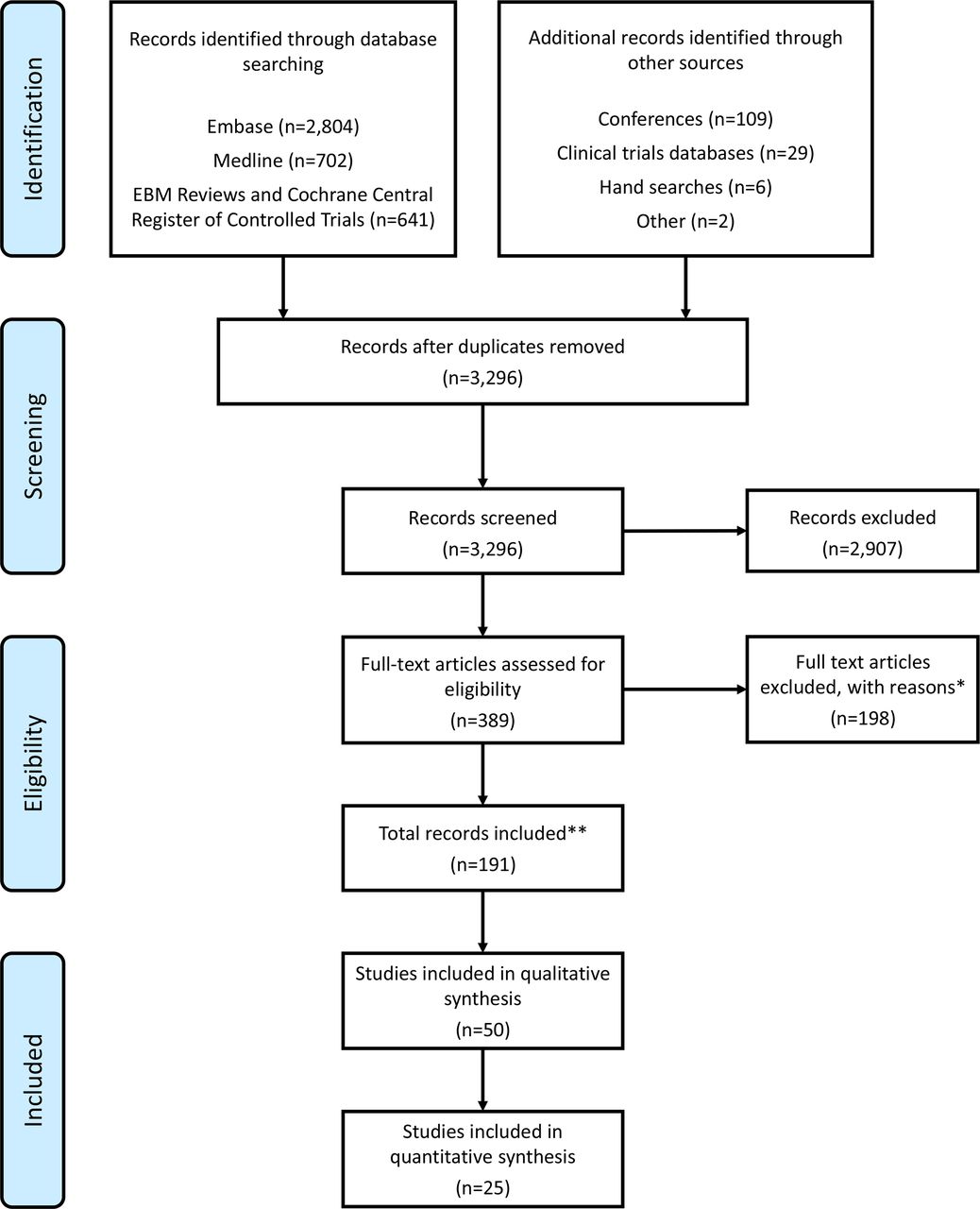
The search strategies yielded a total of 3296 publications, and through the selection process outlined in the PRISMA flow diagram (figure 1) a total of 50 randomised controlled trials were identified for possible inclusion in the NMA. The majority were randomised, placebo-controlled, double-blind trials, and most did not include an active comparator.
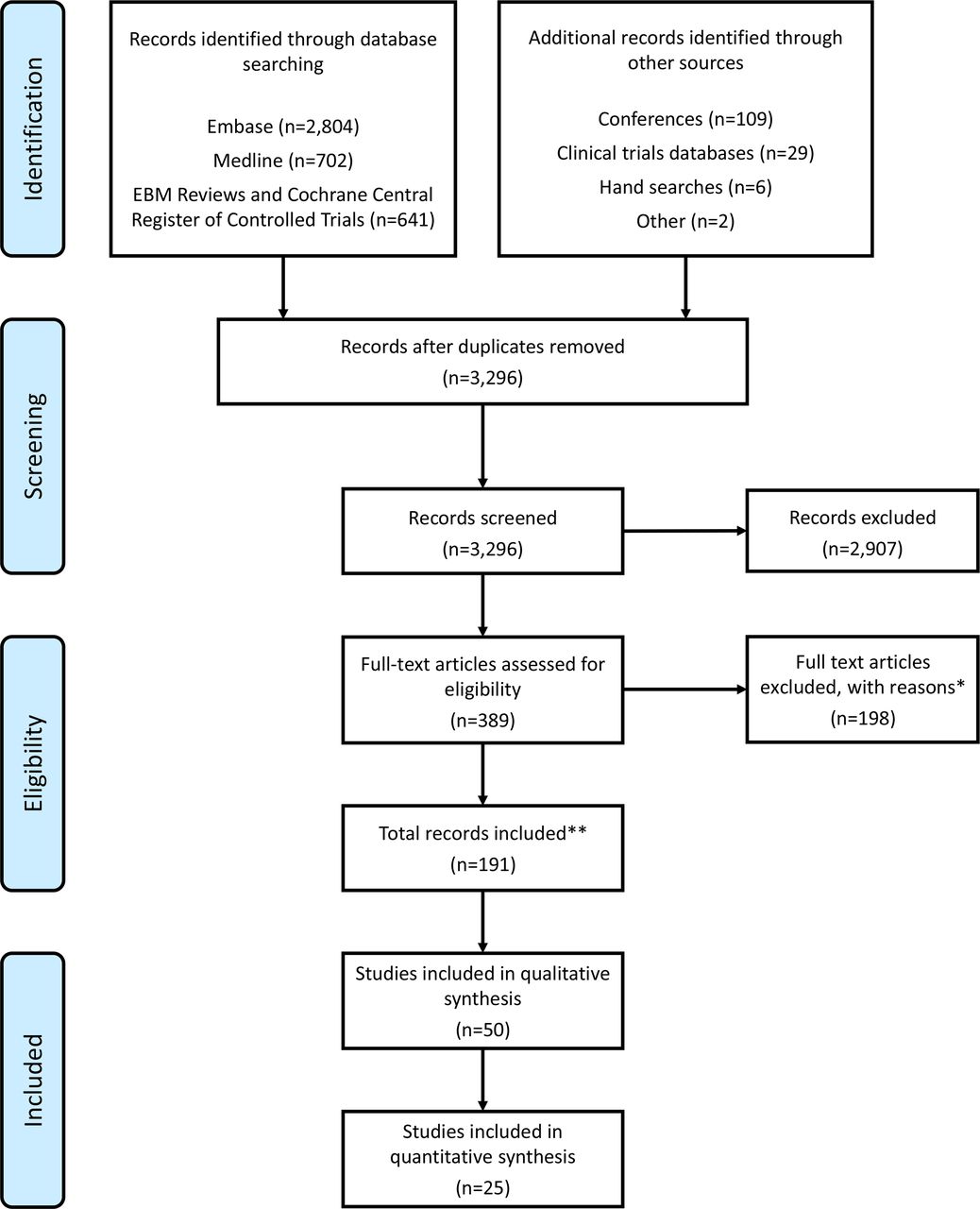
Preferred reporting items for systematic reviews and meta-analyses flow chart showing study selection. EBM, evidence-based medicine. * Reasons for exclusion included: patient population (n=11); interventions (n=5), comparators (n=1), outcomes (n=55), study design (n=50), other (n=83); in some cases, more than one reason were recorded. ** Breakdown by source: Ovid (Embase/Medline/EBM) (n=127), conference searching (n=55), other and hand searches (n=55), clinical trials databases (n=1).
Of the 50 studies identified in the SLR, 25 were eligible for inclusion in the NMA of the full population (ie, sensitivity analysis and safety analyses) and 22 of these were eligible for inclusion in the base-case NMA of the bDMARD-naïve population. For the majority of bDMARDs, one or two randomised controlled trials were identified (table 2). The number of trials included in each network (ie, evaluating ACR, PsARC or PASI end points) may be less than the number of eligible trials because not all studies provided data for all three efficacy end points at the required time point or in a format suitable for analysis. Similarly, not all treatments were included in each network. For the bDMARD-naïve population at weeks 12‒16, ACR response rates were reported in all 22 trials, PASI response rates in 17 studies and PsARC in 13 studies. The likelihood of occurrence of bias in most studies was deemed to be low for domains of performance bias, attrition bias and reporting bias, but the risk of bias was unclear for selection bias, detection bias or other sources of bias.
Overview of randomised controlled trials included in the networks evaluating clinical efficacy in bDMARD-naïve patients with PsA
If there were no data reported specifically for bDMARD-naïve patients in a study (abatacept, apremilast, certolizumab pegol or secukinumab (both dosage regimens)), data from the full study population of patients with active PsA (regardless of prior bDMARD therapy) were used.
Network meta-analysis
For the NMA, the fixed-effects models provided the best fit and are presented for all efficacy outcomes plus SAEs and DAEs; random-effects models are presented for TEAEs and all-cause discontinuation. As noted earlier, ACR, PsARC and PASI results presented here are from the analysis of weeks 12‒16 data in the bDMARD-naïve population of patients with PsA, with a sensitivity analysis of week 24 data in the overall population of bDMARD-naïve and bDMARD-experienced patients. Safety data presented are for the overall population. As most previously published NMAs in PsA have not included ixekizumab, results for this IL-17A antagonist are highlighted in this section.
ACR responses
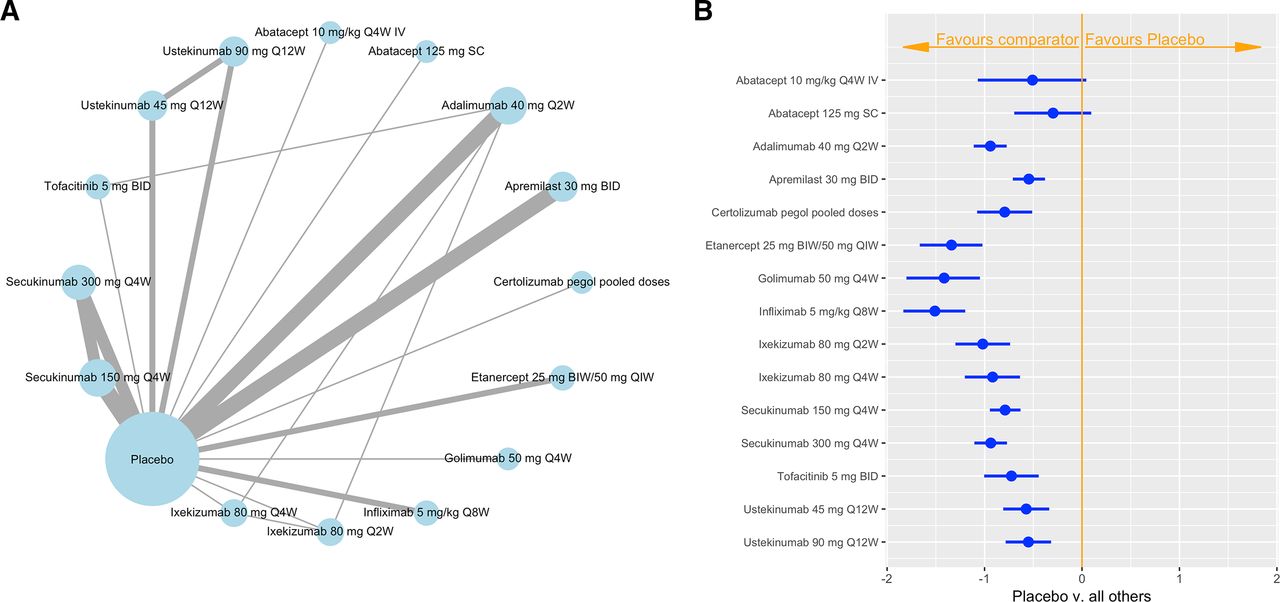
The ACR network for the bDMARD-naïve population included 22 studies and 16 treatment regimens. The ACR network diagram is shown in figure 2A, with lines weighted according to the number of studies included in the respective comparison. With the exception of the two abatacept regimens, all treatments had a statistically greater chance of achieving any ACR score (ACR20, ACR50, ACR70) than placebo (figure 2B). Infliximab was the most effective agent, followed by golimumab and etanercept; these agents were statistically superior to most other treatments, although golimumab and etanercept were not superior to ixekizumab 80 mg every 2 weeks (Q2W). Ixekizumab 80 mg Q2W was statistically superior to abatacept subcutaneous (SC), apremilast and both ustekinumab schedules. Ixekizumab 80 mg Q4W was statistically superior to abatacept SC, apremilast and ustekinumab 90 mg Q12W. Both schedules of ixekizumab did not significantly differentiate from abatacept intravenous, adalimumab, certolizumab pegol, secukinumab and tofacitinib. An additional forest plot with ixekizumab 80 mg Q4W as the active reference is provided in online supplementary figure 1.
Supplemental material
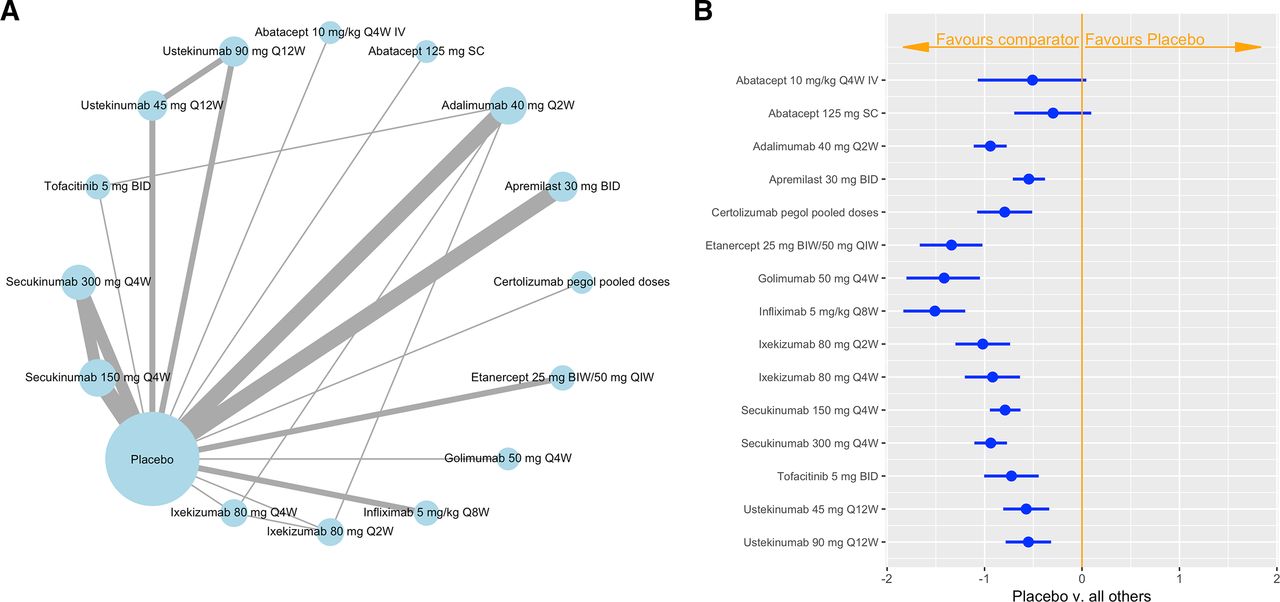
Network diagram (A) and forest plot of treatment differences on the standard normal scale (B) for ACR response at weeks 12–16 among bDMARD-naïve patients with active PsA (placebo as the reference). In the network diagram, line thickness is weighted according to the number of studies included in the respective comparison between treatment regimens or between drug and placebo (indicated by each line connecting circles). Circle size is weighted according to the total number of studies with the treatment regimen or placebo. ACR, American College of Rheumatology; bDMARD, biologic disease-modifying antirheumatic drug; BID, two times per day; BIW, twice weekly; IV, intravenously; PsA, psoriatic arthritis; QxW, every x weeks; SC, subcutaneously.
PsARC response
The PsARC network for the bDMARD-naïve population included 13 studies and 12 treatment regimens, the most frequently studied agent being adalimumab (figure 3A). All treatments had a statistically greater chance of achieving a PsARC response than placebo (figure 3B). The best performing treatments were golimumab, infliximab and etanercept, which were statistically superior to most other agents, including both regimens of ixekizumab. Ixekizumab 80 mg Q2W was statistically superior to tofacitinib. There were no other statistically significant differences between ixekizumab and adalimumab, apremilast, certolizumab pegol and secukinumab. An additional forest plot with ixekizumab 80 mg Q4W as the active reference is provided in online supplementary figure 2.

Network diagram (A) and forest plot of odds ratios (B) for PsARC at weeks 12–16 among bDMARD-naïve patients with active PsA (placebo as the reference). In the network diagram, line thickness is weighted according to the number of studies included in the respective comparison between treatment regimens or between drug and placebo (indicated by each line connecting circles). Circle size is weighted according to the total number of studies with the treatment regimen or placebo. bDMARD, biologic disease-modifying antirheumatic drug; BID, two times per day; BIW, twice weekly; IV, intravenously; PsA, psoriatic arthritis; PsARC, psoriatic response criteria; QxW, every x weeks; SC, subcutaneously.
PASI response
The PASI network for the bDMARD-naïve population included 17 studies and 14 treatment regimens, the most frequently studied agents being adalimumab, apremilast and secukinumab (figure 4A). With the exception of abatacept and etanercept, all treatments had a statistically greater chance of achieving any PASI score (PASI50, PASI75, PASI90 and PASI100) than placebo (figure 4B). The greatest benefit was observed for infliximab, but it was not superior to ixekizumab 80 mg Q2W and Q4W, respectively, which was the next best performing therapy. The probability of ixekizumab 80 mg Q2W achieving PASI50, PASI75, PASI90 and PASI100 was 88.6%, 73.3%, 54.7% and 38.0%, respectively. Corresponding probabilities for ixekizumab 80 mg Q4W were 87.2%, 70.9%, 52.0% and 35.4%. Both schedules of ixekizumab were statistically superior to abatacept, adalimumab, apremilast, certolizumab pegol, etanercept, secukinumab 150 mg, tofacitinib and ustekinumab. An additional forest plot with ixekizumab 80 mg Q4W as the active reference is provided in online supplementary figure 3.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Network diagram (A) and forest plot of treatment differences on the standard normal scale (B) for PASI at weeks 12–16 among bDMARD-naïve patients with active PsA (placebo as the reference). In the network diagram, line thickness is weighted according to the number of studies included in the respective comparison between treatment regimens or between drug and placebo (indicated by each line connecting circles). Circle size is weighted according to the total number of studies with the treatment regimen or placebo. bDMARD, biologic disease-modifying antirheumatic drug; BID two times per day; BIW, twice weekly; IV, intravenously; PASI, Psoriasis Area and Severity Index; PsA, psoriatic arthritis; QxW, every x weeks; SC, subcutaneously.
Meta-regression on baseline risk
Meta-regression analysis was conducted to control for baseline risk. In general, meta-regression results suggested that the standard unadjusted NMA results for clinical efficacy end points might be favouring treatments in studies with smaller placebo response rates—infliximab, golimumab and etanercept—and underestimating the benefit of ixekizumab, certolizumab pegol, tofacitinib and secukinumab.
Adverse events and discontinuation
Safety parameters evaluated in the overall population of bDMARD-naïve and bDMARD-experienced patients included TEAEs, SAEs, DAEs and discontinuation for any reason. The TEAE network included five studies and six treatments (both regimens of ixekizumab, adalimumab, certolizumab pegol, infliximab and placebo). No treatment had a statistically higher or lower chance of a TEAE than placebo, and there were no statistically significant differences between any of the active therapies included in this assessment. The SAE network was much larger, including 22 studies and 16 treatments, although the number of SAEs in each study was low, resulting in a high level of uncertainty regarding the estimated treatment effects. No treatment had a statistically higher or lower chance of an SAE than placebo. Ixekizumab 80 mg Q2W had a statistically higher chance of an SAE than golimumab, but there were no other statistical differences between ixekizumab and other therapies.
The DAE network was also relatively large, with 22 studies and 16 treatments, but the number of DAEs in each study was low and, consequently, there was a high level of uncertainty in results. Apremilast was the only treatment with a statistically higher chance of a DAE than placebo, whereas ustekinumab 45 mg Q12W and ustekinumab 90 mg Q12W had a lower chance of a DAE than placebo. Both schedules of ustekinumab were superior to ixekizumab 80 mg Q2W, although there were no other statistically significant differences between ixekizumab and active therapies. The all-cause discontinuation network included 18 studies and 15 treatments, and no treatment had a statistically higher chance of discontinuation than placebo. Some treatments (adalimumab, etanercept, ustekinumab 45 mg Q12W and ustekinumab 90 mg Q12W) had a statistically lower chance of discontinuation than placebo. There were no statistically significant differences between ixekizumab and other treatments.
Sensitivity analysis
A sensitivity analysis was conducted for the ACR and PASI networks using efficacy data at week 24 for the overall population of bDMARD-naïve and bDMARD-experienced patients. For both of these networks, results of the sensitivity analysis were generally similar to those of the base-case analyses.
The ACR responses included 17 studies and 16 treatments. All treatments had a statistically higher chance of achieving any ACR responses than placebo, and the magnitude of benefit was the greatest for infliximab, followed by golimumab. Both regimens of ixekizumab were statistically superior to once-weekly abatacept 125 mg SC and ustekinumab 45 mg Q12W. In addition, ixekizumab 80 mg Q4W was statistically better than ustekinumab 90 mg Q12W. There were no statistically significant differences between ixekizumab and other treatments.
The PASI response included 14 studies and 15 treatments. With the exception of the two abatacept regimens, all treatments had a statistically higher chance of achieving any PASI score (PASI50, PASI75, PASI90 and PASI100) than placebo. The magnitude of benefit was the greatest with infliximab, followed by golimumab and ixekizumab 80 mg Q2W. Both of the ixekizumab regimens were statistically superior to both of the abatacept regimens, etanercept and secukinumab 150 mg Q4W. Ixekizumab 80 mg Q2W was also statistically superior to adalimumab, certolizumab pegol and secukinumab 300 mg Q4W.
Discussion
Our SLR identified 50 randomised controlled trials for possible inclusion in the NMA that evaluated the efficacy and/or safety of bDMARDs and/or targeted synthetic DMARDs in patients with PsA. This NMA is in line with other reviews and indirect comparisons conducted over the past 2 years,10–14 27–30 and it is one of the most comprehensive NMAs to date, including a broad range of comparators relevant for healthcare decision-making as well as the commonly investigated outcomes in PsA, such as ACR, PsARC and PASI response rates. It was also comprehensive in terms of safety outcomes, including TEAEs, SAEs, DAEs and all-cause discontinuation, and the variety of interventions included.
NMAs evaluating the clinical efficacy of competing interventions at weeks 12‒16 in bDMARD-naïve patients with PsA included a network of 22 studies for ACR, 17 trials for PASI and 13 studies for PsARC. The number of different treatment regimens evaluated was 16 for ACR responses, 14 for PASI response and 12 for PsARC response. In terms of chronological development, these bDMARDs ranged from early agents such as etanercept and infliximab to recent treatments such as ixekizumab, secukinumab and tofacitinib (table 1). Almost all treatments were statistically superior to placebo in each of these networks, the exceptions being abatacept in the ACR and PASI networks, and etanercept in the PASI network. Infliximab, golimumab and etanercept were the most effective treatments in the ACR and PsARC networks. For ACR, ixekizumab 80 mg Q2W was significantly better than abatacept SC, apremilast and both ustekinumab regimens; ixekizumab 80 mg Q4W was significantly better than abatacept SC, apremilast and ustekinumab 90 mg Q12W. For PsARC response, the three best performing agents (golimumab, infliximab and etanercept) were statistically superior to most other agents including both regimens of ixekizumab. Ixekizumab did not statistically differentiate from the other therapies, with the exception of ixekizumab 80 mg Q2W being statistically superior to tofacitinib. In the PASI network, the greatest benefit was observed for infliximab, followed by ixekizumab 80 mg Q2W and Q4W, respectively. Both regimens of ixekizumab were statistically superior to most other treatment regimens, except for golimumab and secukinumab 300 mg Q4W. Results of the sensitivity analysis (ACR and PASI networks) in the overall population at week 24 were generally similar and therefore support the base-case results. Analysis of safety end points in the overall population did not identify any concerns regarding the use of ixekizumab compared with other treatments for PsA.
Several recent NMAs have also evaluated the comparative efficacy of various bDMARDs in PsA,10–14 although we believe that our analysis takes a broader perspective. In particular, our analysis included all approved bDMARDs and targeted synthetic DMARDs, whereas other recent NMAs focused on only a selection of agents, such as IL antagonists. Indeed, as mentioned earlier, the number of different treatment regimens evaluated for ACR, PsARC and PASI responses ranged from 14 to 16. In addition, we considered all studies in a systematic way, and we analysed and extracted data in a consistent and transparent manner. In general, other NMAs showed statistically superior results with active treatment versus placebo and few or no statistically significant differences between active treatments, and in this regard results were broadly similar to those of our NMA.
As was the case in other NMAs in this area,10–14 our NMAs were limited to some extent by the scarcity of available clinical trial data in bDMARD-naïve patients with active PsA. Although the efficacy of most bDMARDs was evaluated in at least two placebo-controlled trials, only one placebo-controlled trial was available for abatacept, certolizumab pegol and golimumab. The limited clinical trial data is also reflected in the relatively wide 95% CrI values across the analyses. Additionally, for some bDMARDs (abatacept, apremilast, certolizumab pegol and secukinumab) in some studies, data were not reported specifically in bDMARD-naïve patients, which necessitated including the overall population of bDMARD-naïve and bDMARD-experienced patients from those studies. For example, in the trial with secukinumab, randomisation was stratified by previous anti-TNF therapy, with a planned enrolment of ≈60% anti-TNF-naïve patients.31 Results of a pre-planned exploratory analysis showed that the magnitude of ACR and PASI response rates was generally higher in the anti-TNF-naïve patients than in those who had previously received anti-TNF therapy.30 Therefore, if prior biologic exposure is an effect modifier for these treatments, the NMA results may not be representative of the treatment effect in a pure bDMARD-naïve or bDMARD-experienced population.
The number of studies per pairwise comparison in each NMA network was generally small. This meant that random-effects models were occasionally difficult to fit. Fixed-effects models were usually the best fit by DIC assessment, which indicates that even when it was not possible to use a pure bDMARD-naïve population there was no evidence of substantial between-study heterogeneity, and in most cases fixed-effects results are presented. However, there may still be undetectable heterogeneity in the network that cannot be adjusted for, which would mean that the treatment effects from the fixed-effects models are too precise, and 95% CrI values may be wider than reported. For similar reasons, although an assessment of inconsistency was performed, and no inconsistency was identified, there were only a small number of closed loops comprised of a few studies. There may still be undetectable inconsistency in the network that could introduce heterogeneity and bias in the results. Also, as noted earlier, meta-regression results generally suggested that the standard unadjusted NMA results for clinical efficacy end points might be favouring treatments in studies with smaller placebo response rates (infliximab, golimumab and etanercept) and underestimating the benefit of ixekizumab, certolizumab pegol, tofacitinib and secukinumab. However, the overall quality of the data from the trials included in the NMAs was generally good in terms of randomisation, blinding and intent-to-treat analyses.
Direct H2H studies generally provide the highest level of evidence.32 As the number of direct comparators is typically limited in practice, NMA can be used to complement the direct evidence to allow for an assessment of comparative efficacy across a broader range of relevant alternative therapies.32 In December 2018, the randomised, open-label phase 3b/4 SPIRIT H2H study was completed, demonstrating superiority of ixekizumab versus adalimumab in bDMARD-naïve patients at 24 weeks for the primary end point of simultaneously achieving ACR50 and PASI100.5 In addition, ixekizumab showed non-inferiority to adalimumab in achieving ACR50 and superiority in PASI100 response. Despite differences in the design of the H2H study compared with the studies included in the NMA, the findings of this study corroborate the results of the NMA and allow for consistent interpretation.
Conclusion
In conclusion, results of this NMA confirm the efficacy and acceptable safety profile of bDMARDs, including ixekizumab, in patients with active PsA. The TNF-α inhibitors infliximab, golimumab and etanercept were the most effective agents for ACR and PsARC responses (ie, joint symptoms), although there were relatively few statistically significant differences between other treatments in these networks. With respect to PASI response (ie, skin symptoms), infliximab and ixekizumab were the best performing therapies. Although the base-case analyses comparing efficacy across three networks (ACR, PsARC and PASI) focused on bDMARD-naïve patients at 12‒16 weeks, results of a sensitivity analysis in the overall mixed population of bDMARD-naïve and bDMARD-experienced patients at week 24 were generally similar and support the robustness of the base-case results. Ixekizumab generally performed well in all three networks, particularly for PASI response, for which only infliximab provided a numerically greater magnitude of benefit in the bDMARD-naïve population. The results of this NMA are consistent with the recently completed H2H study comparing ixekizumab with adalimumab.
Acknowledgments
The authors would like to acknowledge Greg Plosker and Karen Goa (Rx Communications, Mold, UK) for medical writing assistance with the preparation of this manuscript, funded by Eli Lilly.
References
Footnotes
Contributors AR-W was involved with the interpretation of the data. RP and CW were involved with the design of the work, as well as the analysis and interpretation of the data. GB was involved with the design of the work, as well as the acquisition, analysis and interpretation of the data. GK and CS were involved with the design of the work and the interpretation of the data. SK, DN and SH were involved with the conception and design of the work, as well as the interpretation of the data. SL-L was involved with the conception of the work and the interpretation of the data. All authors contributed sufficiently to the work and provided critical revision of the manuscript for important intellectual content. All authors give their approval for the manuscript to be submitted and published in RMD Open and agree to be accountable for all aspects of the work.
Funding This study was funded by Eli Lilly and Company.
Competing interests AR-W has received honoraria for conferences and as a scientific expert from Abbvie, Amgen, Biogen, BMS, Janssen, Lilly, MSD, Novartis, Pfizer, Roche, Sandoz, Sanofi and UCB. RP and GB are full-time employees of Adelphi Values Ltd, and CW of their cooperation partner, Clarostat Consulting Ltd, who were commissioned by Eli Lilly and Company to conduct the analysis for this work. SL-L, GK, CS and SH are full-time employees of Eli Lilly and Company, receive a salary and own company stock. DN and SK were full-time employees of Eli Lilly and Company during the inception of the work.
Patient consent for publication Not required.
Ethics approval None.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement All data relevant to the study are included in the article or uploaded as supplementary information.