Article Text

Abstract
Objectives To compare definitions of high disease activity of the Ankylosing Spondylitis Disease Activity Score (ASDAS) and Bath Ankylosing Spondylitis Disease Activity Index (BASDAI) in selecting patients for treatment with biologic disease-modifying antirheumatic drugs (bDMARDs).
Methods Patients from Rheumatic Diseases Portuguese Register (Reuma.pt) with a clinical diagnosis of axial spondyloarthritis (axSpA) were included. Four subgroups (cross-tabulation between ASDAS (≥2.1) and BASDAI (≥4) definitions of high disease activity) were compared regarding baseline characteristics and response to bDMARDs at 3 and 6 months estimated in multivariable regression models.
Results Of the 594 patients included, the majority (82%) had both BASDAI≥4 and ASDAS ≥2.1. The frequency of ASDAS ≥2.1, if BASDAI<4 was much larger than the opposite (ie, ASDAS <2.1, if BASDAI≥4): 62% vs 0.8%. Compared to patients fulfilling both definitions, those with ASDAS ≥2.1 only were more likely to be male (77% vs 51%), human leucocyte antigen B27 positive (79% vs 65%) and have a higher C reactive protein (2.9 (SD 3.5) vs 2.1 (2.9)). Among bDMARD-treated patients (n=359), responses across subgroups were globally overlapping, except for the most ‘stringent’ outcomes. Patients captured only by ASDAS responded better compared to patients fulfilling both definitions (eg, ASDAS inactive disease at 3 months: 61% vs 25% and at 6 months: 42% vs 25%).
Conclusion The ASDAS definition of high disease activity is more inclusive than the BASDAI definition in selecting patients with axSpA for bDMARD treatment. The additionally ‘captured’ patients respond better and have higher likelihood of predictors thereof. These results support using ASDAS≥2.1 as a criterion for treatment decisions.
- spondyloarthritis
- DMARDs (biologic)
- disease activity
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Key messages
What is already known about this subject?
Ankylosing Spondylitis Disease Activity Score (ASDAS) definition of high disease activity is more inclusive than the Bath Ankylosing Spondylitis Disease Activity Index (BASDAI) definition in selecting patients for treatment with biologic disease-modifying antirheumatic drugs (bDMARDs).
Patients fulfilling both the ASDAS and BASDAI definitions of high disease activity respond better to bDMARDs than those fulfilling each alone.
What does this study add?
Patients exclusively fulfilling the ASDAS definition of high disease activity respond better to treatment and have higher likelihood of predictors thereof than those fulfilling both the ASDAS and BASDAI definitions.
How might this impact on clinical practice?
ASDAS ≥2.1 is the most suitable criterion to decide upon treatment start with bDMARDs.
Introduction
Historically, the Bath Ankylosing Spondylitis Disease Activity Index (BASDAI) has been the most widely used measure of disease activity in axial spondyloarthritis (axSpA). In addition to other criteria (eg, the clinician’s opinion and failure of conventional therapy) a value of BASDAI ≥4 is often required, for instance in most clinical trials, to start treatment with biologic disease-modifying antirheumatic drugs (bDMARDs).1 2 However, this definition (BASDAI ≥4) is largely arbitrary. Moreover, BASDAI is solely based on patient-reported outcomes (PRO), does not weigh each variable (individually or collectively) and ignores possible collinearity between the individual items.3 4
The Ankylosing Spondylitis Disease Activity Score (ASDAS) has been more ‘recently’ developed by the Assessment of SpondyloArthritis international Society (ASAS). Different to BASDAI, ASDAS is a composite disease activity instrument which incorporates both objective inflammatory markers such as C reactive protein (CRP) and PROs (back pain, duration of morning stiffness, patient global assessment and peripheral joint pain).5 6 CRP has been previously and consistently shown to predict response to bDMARDs.7–12 Importantly, unlike BASDAI, for which no cut-offs have been validated, four disease activity states were defined and validated for ASDAS: inactive disease (ASDAS<1.3), low (1.3≤ASDAS<2.1), high (2.1≤ASDAS≤3.5) and very high disease activity (ASDAS>3.5).13 14 Over the years, ASDAS has been ‘challenged’ in several independent cohorts and it has consistently shown to perform well in capturing treatment effects.15–18
Despite the above-mentioned advantages of ASDAS over BASDAI in measuring disease activity in patients with axSpA, evidence supporting that ASDAS can possibly replace BASDAI for selecting patients for treatment with bDMARD is still scarce. A previous cross-sectional study in patients with radiographic axSpA (r-axSpA) has shown that ASDAS high disease activity (≥2.1) captures more patients otherwise missed by BASDAI (≥4) (37% patients had ASDAS≥2.1 and BASDAI<4).12 In addition, data from a small prospective cohort study (n=289) has shown that patients who fulfil the ‘ASDAS criterion’ alone (ie, ASDAS≥2.1 and BASDAI<4) respond well to tumor necrosis factor inhibitors (TNFi), although better results were seen in patients fulfilling both criteria (ASDAS≥2.1 and BASDAI≥4).19 These preliminary data suggest that using only BASDAI≥4 as the eligibility criterion for treatment start, as mostly done so far, excludes patients with potential to benefit from therapy with TNFi or eventually with other bDMARDs. Therefore, for the first time, ASAS experts prescribed the use of ASDAS (≥2.1), in addition to BASDAI (≥4), to select patients to start bDMARD treatment, in the recent update on ASAS-European League Against Rheumatism (EULAR) recommendations for the management of axSpA.20 However, evidence favouring ASDAS is still limited and further data are warranted to eventually strengthen or modify this endorsement. We aimed to compare the definitions of high disease activity according to ASDAS and BASDAI in selecting patients for treatment with bDMARDs.
Methods
Patients and study design
In this prospective multicentre cohort study patients (≥18 years old) with axSpA, according to their treating rheumatologists (both treated and not treated with a first bDMARD), registered in Rheumatic Diseases Portuguese Register (Reuma.pt) from June 2008 to May 2018, were included. In addition, patients were required to have complete 6 months of follow-up (ie, baseline, 3-month and 6-month visits), as well as complete data on ASDAS and BASDAI at baseline (‘eligible population’). Reuma.pt is a nationwide clinical register, established and managed by the Portuguese Society of Rheumatology, in which data from patients with various rheumatic diseases, including axSpA, are recorded. A detailed report of the design of Reuma.pt and data management procedures has been published elsewhere.21 For the current study, a dedicated team of researchers from each participating centre was assigned to compare information on a core set of socio-demographic and clinical variables between the central database and the medical records, in order to complete missing information whenever possible. Patients have signed a written informed consent before inclusion.
Disease activity measurements
The BASDAI is composed of six questions (either scored on a numerical rating scale or on a 10 cm visual analogue scale) that assess fatigue (1), spinal pain (2), peripheral joints (3), entheses (4), intensity of morning stiffness (5) and duration of morning stiffness (6). The total BASDAI score is calculated by summing the first four questions and the average of the last two questions and by dividing the result by 5. The score ranges from 0 (no disease activity) to 10 (very active disease). A cut-off of 4 is frequently used to define active disease, but this cut-off level does not have a firm justification.1 2 22
The ASDAS is a data-driven index that combines three BASDAI-PRO-derived questions about spinal pain (1), peripheral joints (2) and duration of morning stiffness (3), as well as the ‘patient global assessment of disease activity’ (4), with either the CRP (ASDAS-CRP) or the erythrocyte sedimentation rate (ESR) (ASDAS-ESR) (5) according to a weighted formula. The ASDAS-CRP is recommended by ASAS, both for use in clinical practice and in clinical trials. The ASDAS has formally validated cut-off levels for disease activity states: an ASDAS value below 1.3 is considered inactive disease, 1.3 or higher and lower than 2.1 low disease activity, between 2.1 and 3.5 high disease activity, and above 3.5 very high disease activity.13 14 22
Demographic and clinical characteristics
The following information were collected: (1) socio-demographic: age, gender, body mass index (mg/m2), smoking status (smoker/non-smoker); (2) clinical and laboratory: disease duration (years), CRP as continuous (mg/dL), Bath Ankylosing Spondylitis Functional Index (BASFI) and the number of comorbidities (which included arterial hypertension, dyslipidaemia, diabetes, cardiovascular diseases, thyroid disease and malignancies); (3) SpA features (used to assess the ASAS axSpA classification criteria) all as ever (ie, current or past) and binary (yes/no): inflammatory back pain (no formal definition), peripheral arthritis, uveitis, inflammatory bowel disease (Crohn’s/colitis), psoriasis, dactylitis, heel enthesitis, good response to non-steroidal anti-inflammatory drugs (NSAIDs), elevated CRP (≥0.5 mg/dL), human leucocyte antigen B27 status (HLA-B27) and familial history of SpA23; (4) imaging: presence of sacroiliitis on pelvic radiographs, according to the modified New York criteria (mNY), and on MRI (both according to the treating rheumatologists/local radiologists)24 and (5) treatment: bDMARDs used (namely infliximab, etanercept, adalimumab, certolizumab pegol, golimumab or secukinumab) and past and current co-medication (NSAIDs, oral glucocorticoids and conventional synthetic DMARDs (csDMARDs)).
Treatment outcomes
Treatment effect was assessed according to ASAS20 (main outcome) and ASAS40 responses, ASAS partial remission (ASAS PR), ASDAS clinically important improvement (ASDAS CII) and ASDAS major improvement (ASDAS MI), ASDAS inactive disease (ASDAS ID) and BASDAI 50 response (ie, improvement of BASDASI of ≥50% and/or absolute improvement of 2 units).21
Statistical analysis
Patients were grouped into four categories according to the cross-tabulation of baseline ASDAS and BASDAI: (1) ASDAS≥2.1 and BASDAI≥4; (2) ASDAS≥2.1 and BASDAI<4; (3) ASDAS<2.1 and BASDAI≥4 and (4) ASDAS<2.1 and BASDAI<4. The probability of fulfilling the ASDAS definition of high disease activity irrespective of the BASDAI definition and vice versa (marginal probabilities) and the probability of fulfilling each definition conditional on the other were calculated. The four disease activity subgroups were compared with respect to baseline demographic and clinical characteristics across all patients included (‘eligible population’). χ2 test was used to test between-group differences for categorical variables and the independent sample t-test or one-way analysis of variance for continuous variables, as appropriate.
Response to treatment at 3 and 6 months was compared across the four disease activity subgroups, in patients starting treatment with their first bDMARD and with complete follow-up data on all above-mentioned response outcomes (‘efficacy population’). Given the observational setting of our study, treatment response was estimated in multivariable logistic regression models, adjusting for factors, selected a priori, that have been shown to influence the response to TNFi and as such might confound the comparisons across subgroups, that is, age, gender, CRP and BASFI at baseline, and expressed as an estimated probability of response (with 95% CI). Patients were considered treatment responders if they met the clinical response criteria at the particular time point of analysis.
All analyses were repeated in patients who, in addition to the clinical diagnosis, also fulfilled the ASAS axSpA classification criteria. Data analysis was performed using Stata V. 14.
Results
Patient characteristics
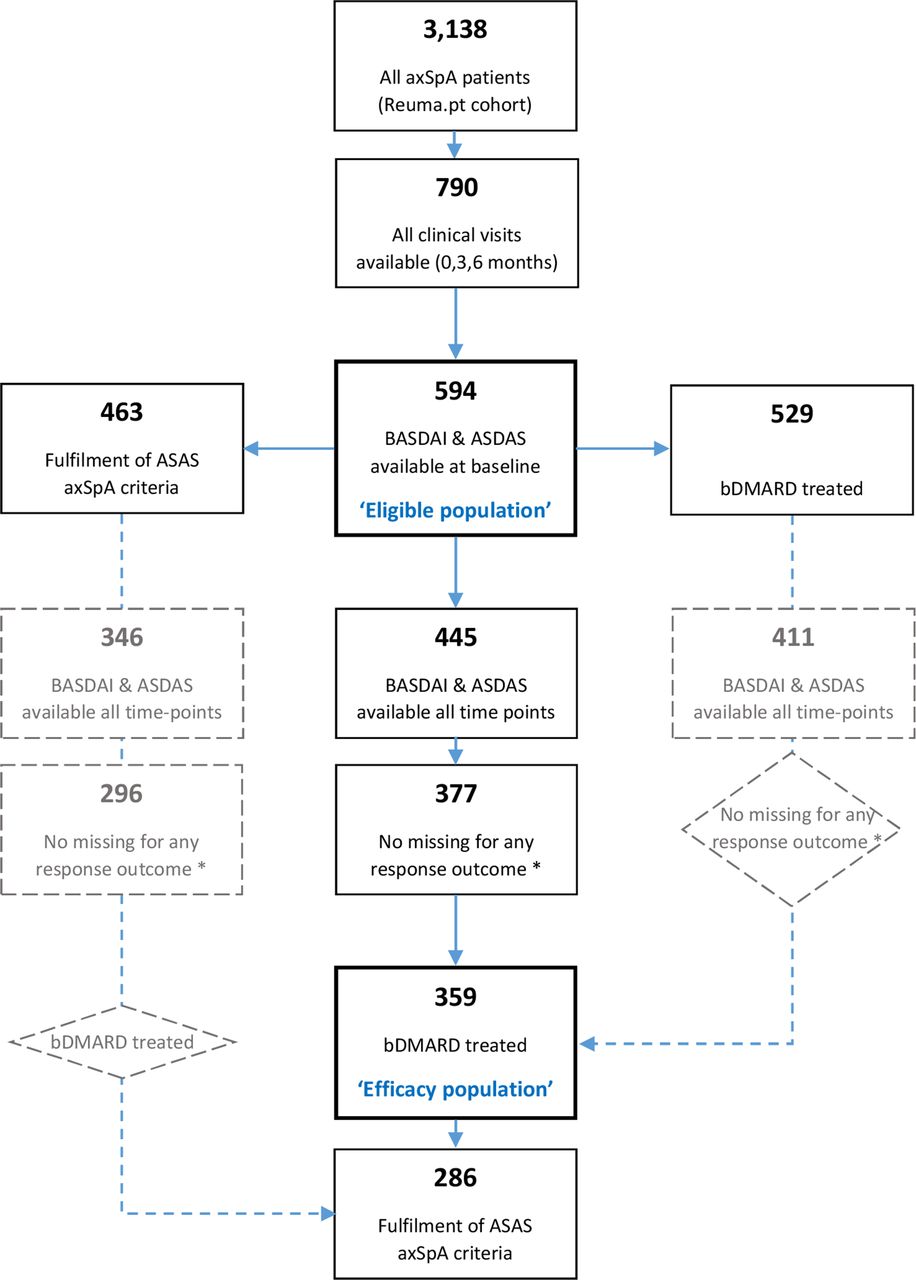
In total, 3138 patients with axSpA were registered in Reuma.pt by the time of database lock (May 2018). From these, 594 fulfilled the inclusion criteria (‘eligible population’) (figure 1). Patients eligible for the study were largely similar to the entire Reuma.pt axSpA population except for higher baseline levels of disease activity and higher number of patients under bDMARD in the former (online supplementary table 1). Out of the 594 included patients 529 were starting their first bDMARD, and out of these 359 had complete data for all response outcomes at every time point (‘efficacy population’) (online supplementary table 2).
Supplemental material
{kind=link}
Flow chart representing sample selection based on inclusion/exclusion criteria and type of analysis. * ASAS20, ASAS40, ASAS PR, ASDAS CII, ASDAS MI, ASDAS ID and BASDAI 50 response. ASAS, Assessment of SpondyloArthritis international Society; ASDAS, Ankylosing Spondylitis Disease Activity Score; ASDAS CII, ASDAS clinically important improvement; ASDAS ID, ASDAS inactive disease; ASDAS MI, ASDAS major improvement; axSpA, axial spondyloarthritis; BASDAI, Bath Ankylosing Spondylitis Disease Activity Index; bDMARD, biologic disease-modifying antirheumatic drugs.
Baseline characteristics are shown in table 1 for the ‘eligible population’ and the ‘efficacy population’. Overall, 55% were men and 67% HLA-B27 positive, with a mean disease duration of 13 years. Patients from the ‘efficacy population’ were largely similar to the ‘eligible population’.
Baseline patient and disease characteristics
Comparison across disease activity subgroups: baseline characteristics
The cross-tabulation between the ASDAS definition of high disease activity (cut-off ≥2.1) and the BASDAI definition of high disease activity (cut-off ≥4), in the ‘eligible population’, is shown in table 2. The probability of fulfilling the ASDAS definition was higher (93%) compared to the probability of fulfilling the BASDAI definition (83%). Most patients fulfilled both definitions (n=487; 82%) and only a minority fulfilled neither (n=39; 7%). The conditional probability of having an ASDAS≥2.1, when BASDAI <4 was much higher than the probability of ASDAS<2.1 among those with BASDAI ≥4 (62% vs 0.8%).
Subgroups according to BASDAI/ASDAS category (baseline)
Compared to patients who fulfilled both (ASDAS and BASDAI) definitions, those who fulfilled only the ASDAS definition were more likely to be male (77% vs 51%) and HLA-B27 positive (79% vs 65%) (table 3). In addition, the levels of CRP were higher (2.9 (SD 3.5) vs 2.1 (2.9) mg/dL) and BASFI was lower (3.0 (2.0) vs 5.6 (2.2)) among patients fulfilling the ASDAS definition only compared to those fulfilling both.
Baseline patient and disease characteristics in the entire ‘eligible population’ and across all subgroups according to BASDAI/ASDAS category
Comparison across disease activity subgroups: response to bDMARDs
Table 4 shows the adjusted response to bDMARDs at 3 and 6 months for the four disease activity subgroups. Overall good response to bDMARDs was observed (eg, ASDAS CII 61% and 66% at 3 and 6 months, respectively). Outcomes were largely overlapping between patients with high disease activity according to the ASDAS definition, irrespective of BASDAI. But for the most ‘difficult’ to achieve outcomes (ie, ASAS PR and ASDAS ID), the likelihood of response was significantly higher in the subgroup fulfilling the ASDAS definition alone compared to the subgroup fulfilling both the ASDAS and BASDAI definitions: ASAS PR at 3 months 61% vs 22% and ASDAS ID at 3 months 61% vs 25%. Patients with ASDAS <2.1 at baseline (regardless of BASDAI) were too few (n=10) to allow a meaningful assessment of treatment effects.
Response to bDMARD in the ‘efficacy population‘ according to the BASDAI/ASDAS category
Sensitivity analysis: patients fulfilling the ASAS classification criteria for axSpA
From the 594 included patients (‘eligible population’), 463 (78%) fulfilled the ASAS classification criteria for axSpA. Out of these, 286 were starting their first bDMARD and had complete data for all response outcomes. These populations showed similar baseline characteristics between each other and the ‘eligible population’ (online supplementary table 3). Results of the sensitivity analyses are similar to the ones from the main analysis (online supplementary tables 4-S6).
Discussion
In this prospective cohort study, we have shown that applying the ASDAS definition of high disease activity (≥2.1) leads to more patients with axSpA being selected to start treatment with bDMARDs, compared to the ‘traditional’ BASDAI definition (≥4). Importantly, the additionally ‘captured’ patients have a higher likelihood of having known predictors of response to bDMARDs, for example, male gender, lower BASFI, higher CRP and indeed respond better, as confirmed by stringent outcomes such as ASAS PR and ASDAS ID. These results support the use of ASDAS≥2.1 as a criterion for treatment decisions in axSpA.
Our results are in line with previous studies also reporting ASDAS high disease activity as more inclusive than BASDAI in the selection of patients with axSpA for bDMARD treatment.12 19 This finding is also in accordance with the overall ‘clinical impression’ that the use of ASDAS expands the spectrum of patients that can benefit from treatment with bDMARDs. Obviously, the consequent relevant question is whether these ‘additional’ patients qualifying for bDMARD treatment really benefit from it, at least as much as those already captured by the BASDAI. Our results do support this claim in two complementary ways: (1) first, the patients fulfilling the ASDAS definition only (ie, ASDAS ≥2.1 and BASDAI <4) show a higher likelihood (compared to those fulfilling both) of baseline (pre-treatment) characteristics that have been consistently shown to be associated with a higher likelihood of response to bDMARDs (ie, male gender, HLA-B27 positivity, elevated CRP and lower level of disability as measured by BASFI)7–12 and (2) second, the patients who fulfil the ASDAS definition only show a similar response to bDMARDs or even better (for the most ‘stringent’ outcomes; ie, ASDAS ID and ASAS PR), compared to patients fulfilling both definitions.
These results must be interpreted considering the study setting. Reuma.pt includes axSpA patients, seen by rheumatologists in daily clinical practice in Portugal since 2008. Already in 2011, the Portuguese recommendations for the use of biological therapies in axSpA for the first time prescribed the use of either ASDAS≥2.1 or BASDAI ≥4 to select patients for bDMARD treatment.25 Although no formal criteria were required in our study, almost all patients fulfilled either the ASDAS and/or the BASDAI definitions at baseline (93% for the ‘eligible population’, data in table 2). In addition, the proportion of patients captured by the ASDAS definition only among patients otherwise not captured (ie, with a BASDAI <4) was impressive: 62% for the ‘eligible population’. This percentage is similar as compared to a previous study in Norway (66%), and even higher if, as done in the latter, we only consider the patients in whom a bDMARD was started, that is, the ‘efficacy population’, with the ASDAS definition only capturing 78% of the patients (data not shown).18 Of note, the use of ASDAS as a criterion to start biological therapy was only considered in the 2016 update of the ASAS-EULAR recommendations for the management of axSpA and is not mandatory in Norway. This suggests that Portuguese rheumatologists not only have been ‘pioneering’ the application of ASDAS for treatment decisions, but also strongly comply with the national recommendations.
As in previous studies, patients starting bDMARD treatment and fulfilling both definitions (ASDAS and BASDAI) had higher pre-treatment disease activity (ASDAS: 3.8 (0.8)) compared to patients fulfilling the ASDAS definition only (ASDAS: 3.0 (0.6)).19 Since high disease activity predicts good response to bDMARDs, higher response rates would be expected in the subgroup fulfilling both the ASDAS and BASDAI definitions. However, this was not what we have found. In fact, for most of the outcomes, the response was largely overlapping between the two subgroups, and for the most ‘stringent’ (ie, ASAS PR and ASDAS ID) response was even higher in the subgroup fulfilling the ASDAS definition only. Despite the fact that the higher likelihood of ASDAS ID and ASAS PR can be, mathematically, explained by lower baseline values of each score individual components (thus, easier to achieve), one alternative and compelling explanation may reside in the higher likelihood of other features also associated with better response, such as male gender, HLA-B27 positivity and lower BASFI that were more common in patients fulfilling the ASDAS definition only.
Our study has some noteworthy limitations. First, the number of ‘eligible’ patients from the overall Reuma.pt cohort is rather small as a result of missing data in the variables of interest (ie, ASDAS and BASDAI), which may limit the external validity of the findings. However, this is a common problem in ‘clinical-practice’ cohorts (registries). Moreover, the ‘eligible population’ is largely comparable to the complete Reuma.pt cohort, except for disease activity which is larger in the former (’eligible population’). This is not unexpected, since the ‘eligible population’ had a larger proportion of patients starting bDMARD therapy. Nevertheless, the response rate in our study is somewhat higher than what is usually seen in clinical trials and also in previous cohorts suggesting possible ‘selection bias’. Notwithstanding, this is unlikely to affect our comparison between subgroups defined by ASDAS and BASDAI disease activity definitions, since this ‘possible bias’ would affect all equally. Second, given the low number of patients we were not able to meaningfully assess the bDMARD efficacy in patients fulfilling neither the ASDAS nor the BASDAI criteria. However, this is merely a reflection of clinical practice and previous studies have already shown that these patients (even if selected by rheumatologists to start biological therapy) respond worse compared with patients fulfilling at least one selection criterion. Third, since almost all patients fulfilling the ASAS criteria were also mNY-positive (86%) we could not investigate whether there were differences between patients with r-axSpA and non-radiographic axSpA (nr-axSpA). Again, this reflects the current clinical practice in our country (where only recently TNFi have been approved for nr-axSpA), but given the extensive literature showing no meaningful differences in disease burden between nr-axSpA and r-axSpA it is unlikely that our results would be different in these patients.25–29
In conclusion, both BASDAI and ASDAS perform well in selecting patients with axSpA for treatment with bDMARDs in daily clinical practice. Ignoring ASDAS as a selection criterion yields an unacceptable number of patients being excluded from an intervention from which they would most likely benefit. Additionally, patients exclusively captured by the ASDAS definition of high disease activity (≥2.1) respond better to treatment and have a higher likelihood of predictors thereof. Therefore, the ASDAS should be at least used in addition to BASDAI, and most likely exclusively, when selecting patients for treatment with bDMARDs.
Acknowledgments
The authors thank patients included in Reuma.pt for their contribution to this study, all rheumatologists involved in data collection and the Portuguese Society of Rheumatology staff for data management.
References
Footnotes
Twitter @R_M_Santiago
Contributors Study concept and design: JM, AS and SR. Statistical analysis and data interpretation: JM, SRM, AS and SR. Data collection: JM, SRM, HS, EVS, FV, JTC, JR, MB, NM, RCM, RR, JLS, MM and RMF. JM prepared the first version of the manuscript. FPS, AFM, NG, JCB and all the previously-mentioned authors collaborated on further data interpretation, revised the manuscript critically for important intellectual content and gave final approval of the version to be published.
Funding This work was supported by a Research Grant from the Investigator-Initiated Studies program of Merck Sharp & Dohme (Grant No. 56078). The sponsor did not interfere with the study question, analysis or interpretation of results. AS is supported by a doctoral grant from Fundação para a Ciência e Tecnologia (Foundation for Science and Technology) (SFRH/BD/108246/2015).
Competing interests AS received speaker fees from Novartis. FPS received speaker/consultancy/research fees from AbbVie, Novartis, MSD, Eli Lilly, Janssen-Cilag, Pfizer, Biogen, Vitória, Roche, Menarini, AlfaSigma, UCB and Medac. HS received speaker/consultancy fees from AbbVie, Eli Lilly, Janssen-Cilag, Novartis and Pfizer. JTC received speaker/consultancy fees from AbbVie, Amgen, Eli Lilly, Janssen-Cilag, MSD, Novartis, Pfizer and UCB. MB received consultancy fees from AbbVie, Amgen, Eli Lilly, Novartis, Pfizer, Janssen-Cilag, Glaxosmithkline, Biogen. Speaker fee: Janssen-Cilag. SR received speaker/consultancy fees from AbbVie, Eli Lilly, MSD, Novartis, Pfizer and Sanofi.
Patient consent for publication Not required.
Ethics approval Reuma.pt has been approved by the ethics committees of the participating hospitals and complies with the Declaration of Helsinki. This specific study has been approved by the Ethics Research Committee of the NOVA Medical School | Faculdade de Ciências Médicas—Universidade Nova de Lisboa (CEFCM), Lisbon, Portugal.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement All data relevant to the study are included in the article or uploaded as supplementary information. Name: Reuma.ptURL: http://reuma.pt/pt_PT/Default.aspx.