Article Text

Abstract
Total hip and total knee arthroplasty) remain important interventions to treat symptomatic knee and hip damage in patients with rheumatoid arthritis, with little change in utilisation rates despite the increasingly widespread use of potent conventional synthetic disease-modifying anti-rheumatic drugs (csDMARDs) and targeted DMARDs including Janus kinase inhibitors and biologics. The majority of patients are receiving these immunosuppressing medications and glucocorticoids at the time they present for arthroplasty. There is minimal randomised controlled trial data addressing the use of DMARDs in the perioperative period, yet patients and their physicians face these decisions daily. This paper reviews what is known regarding perioperative management of targeted and csDMARDs and glucocorticoids.
- Corticosteroids
- Methotrexate
- Orthopedic Surgery
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
INTRODUCTION
The standard of care for patients with rheumatoid arthritis (RA) is to gain control of the disease by escalating or changing disease-modifying anti-rheumatic drug (DMARD) therapy until remission or low disease activity is achieved. Currently, most patients with RA are receiving one or more conventional synthetic DMARDs (csDMARDs) or a combination including a targeted therapy to achieve this goal.1 The treatment of RA has changed substantially over the past decades. In 1986–1989, 1% of patients with RA used methotrexate as the first‐line csDMARD and approximately 2.5% of patients with RA were on a combination of two csDMARDs.2 By 2006–2011, 70% of patients were on methotrexate, and 22.5% of patients were on combinations of two to three csDMARDs or a csDMARD and a targeted DMARD.2 3 By 2013–2016, 50% of patients with RA undergoing arthroplasty were on targeted DMARDs, 80% were on methotrexate or other csDMARDs and 32% were receiving glucocorticoids at the time of joint replacement surgery.3 While use of both conventional and targeted DMARDs has increased, and the rates of upper extremity and small joint surgery have decreased, the rates of total hip (THA) and total knee arthroplasty (TKA) have not.2 4 In one recent study using propensity matching and adjusting for disease activity, tumour necrosis factor inhibitor (TNFi) use was not associated with decreased rates of THA or TKA.5 Therefore, patients with RA continue to undergo THA and TKA, despite high utilisation of targeted and csDMARDs and glucocorticoids, which most patients are taking at the time of surgery. A careful thorough medical evaluation is also essential in these patients but will not be addressed in this paper.6 This paper provides an overview of the current data supporting perioperative management of targeted and csDMARDs and glucocorticoids and the current recommendations for perioperative medication management. The majority of the data presented comes from studies of patients with RA undergoing joint replacement.
RISK OF INFECTION
Medication management at the time of surgery seeks to balance the risk of infection attributed to targeted and csDMARDs against the risk of flares of inflammatory disease.7 8 Patients with RA have an increased risk of infection in general, and this risk is increased in patients treated with certain immunosuppressants, including glucocorticoids, and in patients with severe or active disease.7 9–11 Risk associated with disease activity is especially relevant since most patients have active disease at the time of arthroplasty, with a mean Disease Activity Score-28 (DAS28) Erythrocyte Sedimentation Rate of 3.7, indicating moderate disease activity, despite a mean disease duration of almost 15 years.3 The majority of prosthetic joint infections (PJI) occur during the first 1–2 years after surgery, with an overall incidence of 1.55%, and are attributed to infections introduced at the time of surgery or as a result of delayed wound healing; the incidence of late infections is significantly lower at 0.46%.12 Patients with RA have a 50–80% greater risk of PJI than patients with osteoarthritis, and also have greater risk beyond the early period.9 13 14 For the purposes of perioperative management, however, early infections are most relevant since delayed infections are more commonly related to subsequent episodes of sepsis or bacteremia and are not expected to be influenced by perioperative medication management decisions.15
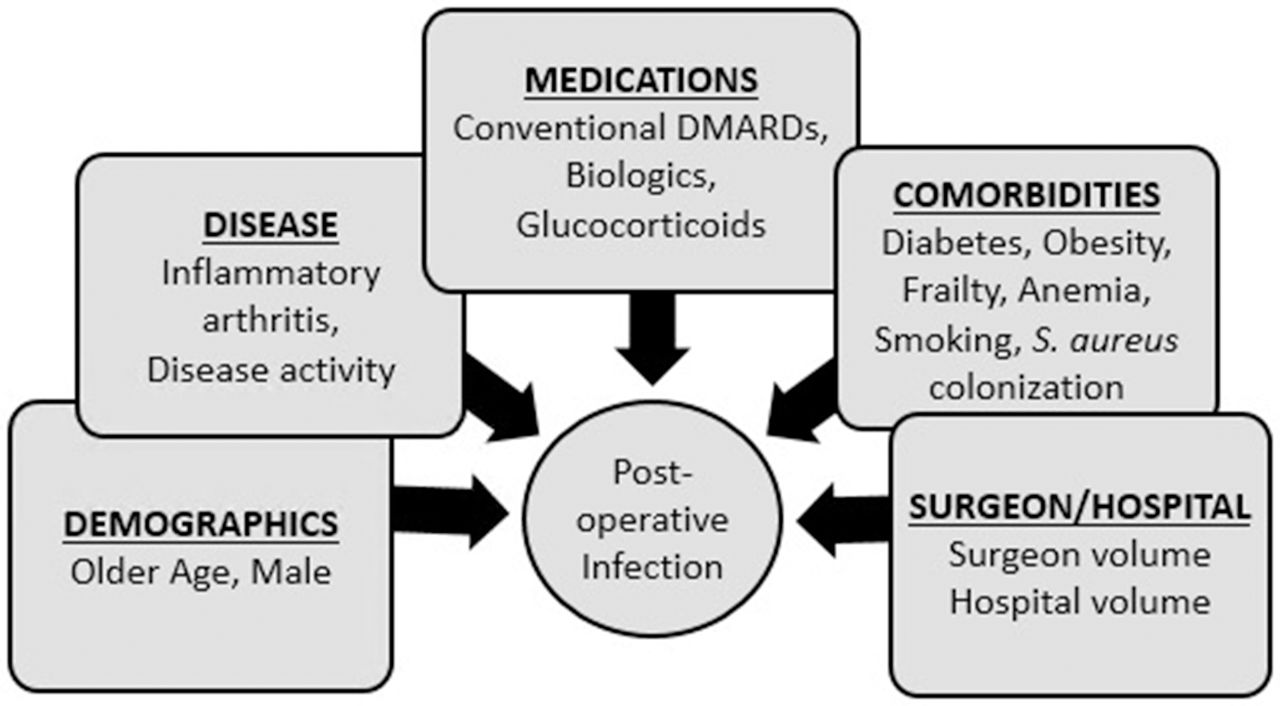
Multiple other factors contribute to infection risk, such as age, comorbidities (eg, obesity, smoking, diabetes) and the volume of surgeries performed by the hospital and surgeon (figure 1).16 Risks for infection are additive. For instance, there is a fourfold increase in the risk of PJI with a body mass index (BMI)>40 kg/m2 (OR 4.13, 95% CI 1.3 to 12.88; p=0.01). If the patient with a BMI>40 kg/m2 is also an active smoker, the risk is higher (OR 7.52, 95% CI 1.69 to 33.4, p=0.04). Staphylococcus aureus colonisation is increased in patients with RA on biologics (OR 1.80, 95% CI 1.007 to 3.22, p=0.04) and S. aureus colonisation increases the risk of PJI (OR 2.36, 95% CI 1.13 to 4.88, p=0.02).17 If the colonised patient is also a smoker with a BMI≥30 kg/m2, the risk increases further (OR 12.76–66.16, p=0.017).18 While medication management around the time of surgery is of particular interest because of the potential for intervention, it is important to remember that infection risk in patients with RA is multifactorial.

Risk factors for postoperative infection. DMARDs, disease-modifying anti-rheumatic drugs; S. aureus, Staphylococcus Aaureus.
POSTOPERATIVE FLARES
Flares are common after THA and TKA; 63% of patients with RA report a flare within 6 weeks of surgery, and a third were rated as severe by those with flares.3 19 Patients who reported flares had higher disease activity than those without and a similar pattern as patients who had not undergone surgery, and patients in both surgical and non-surgical groups self-manage their flares and rarely consult their rheumatologist.20–22 Patients describe flare events as severe and disabling, and flares are associated with radiographic progression.21 23 However, using a measure commonly used to assess THA and TKA outcomes, the Hip Disability (HOOS) and Knee Injury OA Outcomes Scores (KOOS), flares in the post-operative period were not an independent risk factor for pain and function measured at 1 year after surgery.24 Baseline DAS28 predicted 1-year HOOS/KOOS pain and function; each 1 unit increase in DAS28 worsened 1-year pain by 2.41 (SE=1.05, p=0.02) and 1-year function by 4.96 (SE=1.17, p=0.0001), suggesting that active sustained disease is a greater problem than flares.24 In addition while numerically more flarers used targeted DMARDs, stopping them did not predict flares, and continuing methotrexate in this cohort was not protective.3 Optimisation prior to surgery should include controlling RA disease activity when possible. Moreover, when a patient panel comprised patients with RA and juvenile arthritis were convened to advise the American College of Rheumatology (ACR) and the American Association of Hip and Knee Surgeons (AAHKS) in the formulation of a guideline for perioperative medication management, they were unanimous in their opinion that any potential increase in infection risk was worse than a flare of their disease.24 25 Taken together, these data suggest that flares in the postoperative period may not be linked to medication management and that patients prioritise the risk of infection over flares after arthroplasty. Table 1 summarises the medications in current use in rheumatology practice and recommendations included in the ACR/AAHKS Guideline.26
Medications included in the American College of Rheumatology/American Association of Hip and Knee Surgeons Guideline for the Perioperative Management of Antirheumatic Medication in Patients With Rheumatic Diseases Undergoing Elective Total Hip or Total Knee Arthroplasty*
TNF INHIBITORS
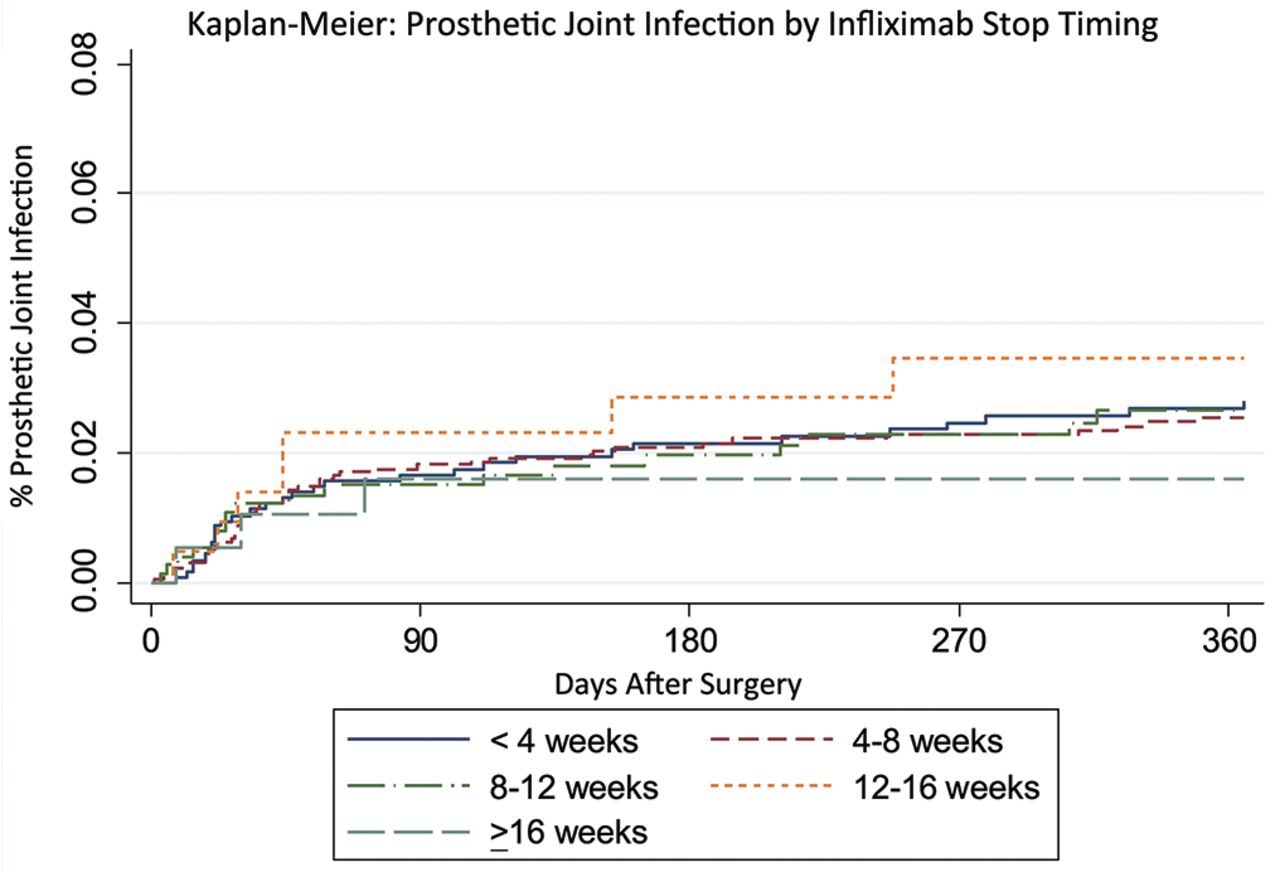
Patients receiving TNFi have an increased risk of infection,11 and studies have demonstrated that patients undergoing TKA or THA who receive TNFi were at an increased risk of infection compared to those with no TNFi exposure.11 27 Using pooled data in a meta-analysis representing 3681 patients with and 4310 without a recent exposure to TNFis at the time of surgery, the TNFi exposed group had higher risk of developing a surgical site infection compared with patients not exposed to TNFi (OR 2.47, 95% CI 1.66 to 3.68. p<0.0001).28 However, the included studies compared those whose disease was severe enough to treat with a TNFi compared with those who were likely to have milder disease, and disease activity and severity are also risk factors for infection.7 29 30 Administrative data sets contain billing data for TNFi infusions that permits the time between the TNFi dose and surgery to be accurately determined and compared, so equivalent groups could be analyzed. There was no increase in infection within 30 days of surgery in patients who received infliximab <4 weeks prior to surgery compared to 8–12 weeks (propensity adjusted OR 0.90, 95% CI 0.60 to 1.34). Similarly, there was no increase in the rate of PJI in patients receiving infliximab infusions <4 weeks versus 8–12 weeks (3.1 vs 2.9 per 100 person-years, HR 0.98, 95% CI 0.52 to 1.87) (figure 2).31 Using the Danish arthroplasty registry and linking to the DANBIO rheumatology register that contains information about RA disease and severity and biologics use, patients with RA had an increased risk of PJI (confounder adjusted sub-HR (SHR)=1.46 (1.13–1.88)).30 However, treatment with biologic DMARDs did not significantly increase PJI risk (SHR=1.61 (0.70–3.69)).30 Moreover, a meta-analysis demonstrated that postoperative infection risk was not decreased in those patients stopping TNFi prior to orthopaedic surgery.32 Less data exist for other surgery types, many of which may be associated with higher risks of complications. One study of patients with inflammatory bowel disease undergoing abdominal surgery found an increased rate of infectious complications (although not serious infections) in patients receiving a TNFi,33 but a similar study found that use of biologics use was not associated with wound complications and that the timing of biologics before surgery was not associated with outcomes.34 Whether data in patients undergoing abdominal surgery to treat an inflammatory gastrointestinal condition are applicable to patients with RA is uncertain. A recent study using administrative data evaluated patients with RA undergoing hip fracture repair, abdominopelvic surgery, or cardiac surgery and found no increase in the risk of 30-day readmission, hospitalised infection, pneumonia or wound complications in patients receiving a TNFi or in patients receiving a non-TNFi targeted DMARD compared with patients receiving methotrexate without one of these therapies.35 Similar to what has been seen in studies of arthroplasty, the timing of infliximab infusions prior to surgery was not associated with adverse outcomes.35

Kaplan-Meier curves comparing incidence of prosthetic joint infection in patients with RA undergoing total hip or knee arthroplasty based on the time between the last infliximab infusion and surgery (infliximab stop time)31 (Reproduced with permission). RA, rheumatoid arthritis.
While it remains uncertain whether interruption of a TNFi before surgery can improve postoperative outcomes, the ACR/AAHKS guideline for patients undergoing elective TKA and THA achieved consensus between the surgeons, rheumatologists and infectious disease specialists, recommending that all biologics be withheld for a short duration with surgery planned for the end of the dosing cycle. This recommendation assumes that high doses of medications suppress the immune system more than lower doses and that the dosing interval better reflects the duration of immunosuppression that the blood half-life. Medications can be restarted at approximately 14 days after surgery when the wound has healed, sutures and staples are out, there is no swelling or drainage and there are no clinical signs of infection.26
OTHER TARGETED DMARDS
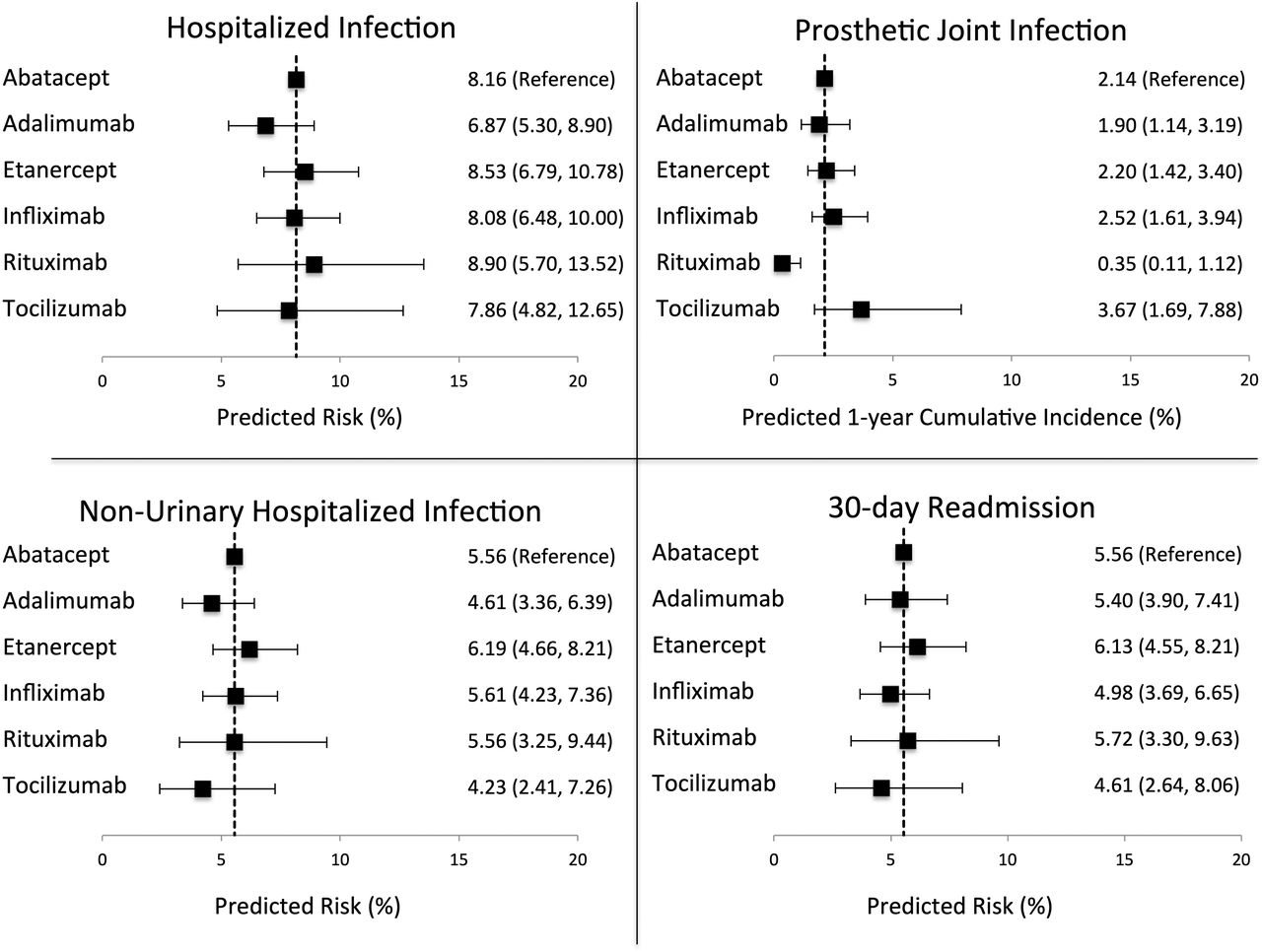
Less data exist to inform management of other targeted DMARDs. An administrative claims study examining 1958 patients with RA receiving abatacept infusions before arthroplasty found no difference in postoperative infection in patients who received abatacept 4–8 weeks (one dosing interval) versus <4 weeks before surgery (OR 0.93 (0.65–1.34) for 30-day hospitalised infection, HR 1.29 (0.62–2.69) for PJI within 1 year).36 A previous registry described low infection risk for abatacept treated patients and no relationship between time from infusion to surgery.37 An additional study using the same data sources examined a cohort of 9911 patients with a prescription or infusion of abatacept, adalimumab, etanercept, infliximab, rituximab or tocilizumab who underwent THA or TKA and found no difference in hospitalised infection, PJI or readmission between the biologics (figure 3).38 Although the study cohort contained few rituximab- and tocilizumab-treated patients, registries have provided additional data. Data from patients treated with tocilizumab who underwent surgery were collected from a routine care registry. The mean interval between surgery and the last tocilizumab infusion was 4.94±1.74 weeks, with few complications reported.39 However, surgeons may not be aware of the direct effect of tocilizumab on the C reactive protein and blunting of the temperature curve, requiring greater vigilance in diagnosing infection postoperatively.40 A total of 201 patients in a rituximab registry underwent surgery, 58% were orthopaedic procedures and 9 patients (6.7%) had complications. There was no significant difference in the median interval between the rituximab infusion and surgery for patients with complications (6.43 months (IQR 4.46–7.6 months)) and without (6.49 months (IQR 3.91–8.74 months)) (p=0.99). Included cases were few, and no information regarding immunoglobulin levels was available.41 As low immunoglobulin levels increase infection risk, measuring immunoglobulin levels prior to surgery and replacing when low may be more relevant in mitigating infection risk than extending the interval between surgery and the rituximab infusion.42 For non-surgical patients with RA in the National Databank for Rheumatic Diseases, there was no difference in the risk of serious infections in 7210 patients receiving TNFis compared with 1676 patients on non-TNFi biologics.43 There is little information regarding patients receiving Janus kinase inhibitors such as tofacitinib undergoing arthroplasty, although again in non-surgical studies, infection risk seems comparable to that seen with biologics.44

Associations between the type of biologic a patient was receiving and risks of postoperative outcomes from inverse probability weighted models31 (Reproduced with permission).
The similarity in infection risk among the biologics has led to the recommendation to plan surgery at the end of the dosing cycle and minimise the time the medications are withheld, as for the TNFis.26 Given the short half-life of tofacitinib, recommendations were to withhold treatment for 7 days before surgery.
METHOTREXATE AND OTHER csDMARDS
Methotrexate, the anchor drug in RA, was studied in a randomised controlled trial of patients with RA undergoing elective orthopaedic surgery, with 388 patients randomised into three groups, and complications including infections or revisions compared between groups. In Group A (continued methotrexate), 2% of patients had complications, 15% of Group B (withheld methotrexate) and 10% of 228 patients in Group C (were never on the drug) had complications. Flares were also significantly lower in Group A.45 In addition, the overall safety profile of methotrexate has recently been confirmed in a non-rheumatic disease population of diabetics and those with metabolic syndrome, with no difference in serious infections (HR 1.02, 95%CI 0.69 to 1.50) and little difference in infection risk overall (HR 1.15, 95%CI 1.01 to 1.30).46 Finally, methotrexate increases the levels of adenosine, and studies in animal models demonstrate that adenosine engages receptors on cells and promotes wound healing, adding a theoretical framework to support the continuation of methotrexate at the time of surgery.47
There is little surgical safety data for other csDMARDs, such as sulfasalazine, hydroxychloroquine or leflunomide. A retrospective study of 367 joint surgeries in 204 patients with RA, most of whom were treated with csDMARDs, demonstrated no increase in surgical site infection, and sulfasalazine appeared to decrease infection in another study.48–50 Given the overall safety profile of the csDMARDs, the ACR/AAHKS perioperative management guideline recommends continuing these medications through surgery.26
Other immunosuppressants such as azathioprine, mycophenolate, cyclosporine and tacrolimus are used more commonly in autoimmune rheumatic diseases other than RA (such as systemic lupus erythematosus). These therapies may be associated with greater infection risk than methotrexate, but there are very little data on how these treatments might affect postoperative infection risk. One Medicare study of 3339 solid organ transplant patients undergoing arthroplasty who were frequently treated with one or more of these therapies had a greater risk of pneumonia, sepsis and periprosthetic infection compared to controls (2.4% vs 1.0%), but the specific contribution of immunosuppression to this risk could not be determined.51 Given this uncertainty, ACR/AAHKS guidelines recommend continuing these therapies with severe systemic autoimmune disease (in whom the risk of stopping therapy would be high) and stopping therapy for 1 week prior to surgery in patients with more mild disease, in consultation with the patients treating rheumatologist.26
GLUCOCORTICOIDS
Glucocorticoid therapy is widely used in rheumatic diseases. Overall, 65% of patients with RA receive glucocorticoids, and a recent surgical series revealed that 87% of patients undergoing THA or TKA were given glucocorticoids at the time of surgery.3 52 Infection is a well-known risk for patients with RA outside the surgical setting, for whom the risk of serious infection is greatest in those with active disease, or with a high exposure to glucocorticoids. In a study using a model of glucocorticoid use that incorporates information relevant to patients with RA about duration, intensity and timing of glucocorticoid exposure,7 43 53 high levels of both recent and cumulative glucocorticoid use increased infection risk (OR 1.33, 95% CI 1.22 to 1.45, p<0.001). Glucocorticoids have also been shown to be associated with greater infection risk in patients with RA undergoing arthroplasty, especially at higher doses. In one study, the risk for infection was higher with a glucocorticoid dose >15 mg.54 In a study of patients with RA undergoing elective THA and TKA using large insurance data sets that include both infusion and prescription data, glucocorticoids were associated with a dose-dependent increase in postoperative risk for PJI and serious infection. Propensity-weighted models showed that use of more than 10 mg of glucocorticoids per day (vs no glucocorticoid use) resulted in a predicted risk for hospitalised infection of 13.25% (95%CI 9.72% to 17.81%) (vs 6.78%) and a predicted 1-year cumulative incidence of PJI of 3.83% (95%CI 2.13% to 6.87%) (vs 2.09%).38 In addition, using data from a rheumatology registry linked to an arthroplasty registry revealed that glucocorticoid exposure was a risk factor for PJI (HR 2.87, 95% CI 1.12 to 7.34), and both glucocorticoids and increasing disease activity measured as DAS28 (HR 1.49, 95% CI 1.01 to 2.20) were risk factors for mortality.30 Glucocorticoids at doses >5 mg/day were also a risk factor for postoperative mortality or readmission in a study of patients with RA undergoing hip fracture, abdominopelvic or major cardiac surgery.31 These data suggest that minimising glucocorticoids in the months before elective surgery may improve outcomes and that delaying elective surgery may be appropriate in some situations, especially for patients receiving high doses of glucocorticoids.
Long-term glucocorticoid therapy cannot be abruptly stopped during a physiologic stress such as surgery, however, out of concern for adrenal insufficiency causing hypotension and even death. The question for clinicians is whether to administer supraphysiologic doses (‘stress dose steroids’) at the time of surgery to prevent adrenal insufficiency or continue the usual dose; however, stress dosing, or supraphysiologic doses meant to mimic the response to stress, remains prevalent.55 There are little data to guide the need for stress dosing. In a systematic review that included seven observational cohorts and two randomised controlled trials and included 315 patients and 389 operations, there was no haemodynamic difference between those receiving stress dosing compared with those who did not, and measuring cortisol levels was not helpful.55 Given the potential for an increase in infection risk and little data to support its use, the ACR/AAHKS guideline recommends giving only the usual daily dose of glucocorticoids on the day of surgery for adults receiving chronic steroids for their rheumatic condition at the time of elective TKA and THA.26
CONCLUSION
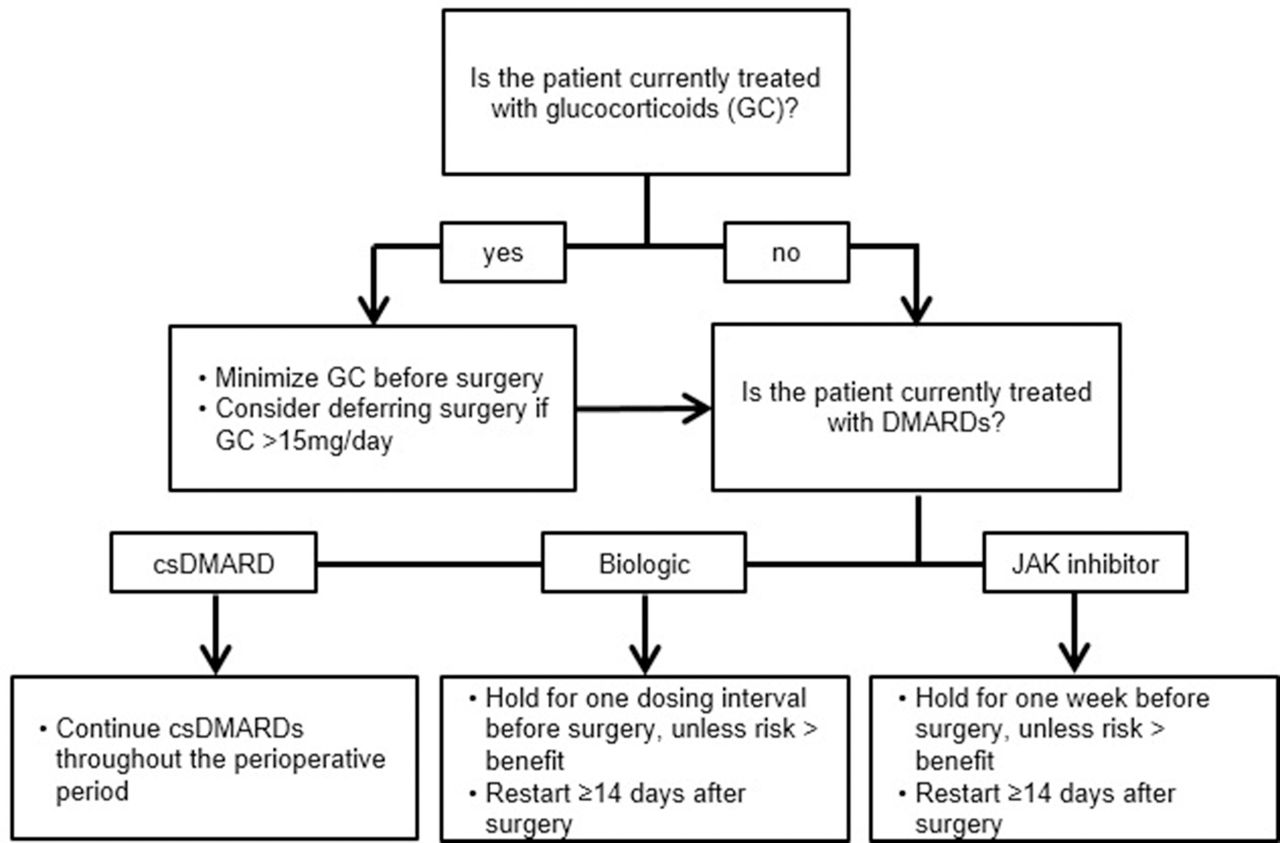
Patients with RA continue to undergo and benefit from THA and TKA, and the majority receive csDMARDs, glucocorticoids or targeted therapies at the time of surgery. A general approach to perioperative management before elective THA and TKA is summarised in figure 4. Current practice supports continuing csDMARDs through surgery. Glucocorticoids should be tapered to at least less than 15 mg prior to surgery, and lower if possible. At the time of surgery, glucocorticoids should be continued at their presurgical dose rather than using ‘stress doses’. While observational studies have not shown clear differences in the rate of postoperative infection in patients who stop biologics before surgery, concerns remain given known risks associated with these therapies; performing surgery at the end of the biologic dosing cycle and restarting at approximately 2 weeks after the wound has closed achieved consensus support from the guideline development panel of the ACR/AAHKS.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Flow diagram outlining approach to perioperative management of immunosuppression in patients with rheumatoid arthritis undergoing elective hip or knee arthroplasty. csDMARDs, conventional synthetic disease-modifying anti-rheumatic drugs38 (Reproduced with permission).
Key messages
Arthroplasty use remains prevalent for patients with rheumatoid arthritis (RA), and the majority are receiving biologic and conventional DMARDs and glucocorticoids at the time of surgery.
Risk of surgical site infection including prosthetic joint infection is multifactorial for patients with RA and includes active RA, smoking, comorbidities, glucocorticoids and immunosuppressive therapy.
Flares of RA are frequent after arthroplasty, and the link to medication management is not established; patients tend to prioritise avoiding infections over risking flares.
Current studies of the interval between a biologic infusion and surgery have not demonstrated a differential infection risk for patients receiving recent versus remote infusions.
REFERENCES
Footnotes
Funding The authors report grants from Bristol-Myers Squibb, personal fees from AbbVie, Expert witness testimony, grants and personal fees from Novartis, and personal fees from American College of Rheumatology, outside the submitted work.
Competing interests SMG has consulted for Novartis and UCB, and has research funding from Novartis, Pfizer and Horizon Pharma. MDG has consulted for AbbVie and has research funds from Bristol Meyers Squibb.
Patient consent for publication Not required.
Disclaimer The views expressed in the submitted article are of the authors’ own and are not an official position of the institution.
Provenance and peer review Commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.