Article Text

Abstract
Objective To evaluate the effect of guselkumab on enthesitis and dactylitis in a phase II trial of patients with active psoriatic arthritis (PsA).
Methods This was a phase II, randomised, placebo-controlled, double-blind trial of adults with active PsA (≥3 swollen and ≥3 tender joints and C reactive protein ≥0.3 mg/dL) despite conventional synthetic disease-modifying anti-rheumatic drug, non-steroidal anti-inflammatory drug, and/or oral corticosteroid therapy. Patients were randomised to subcutaneous injections of guselkumab 100 mg or placebo at weeks 0, 4 and every 8 weeks, with placebo crossover to guselkumab at week 24. Dactylitis was scored on a scale of 0–3 on each digit; enthesitis was assessed using the Leeds Enthesitis Index (0–6). Other assessments included American College of Rheumatology (ACR) and Psoriasis Area and Severity Index responses.
Results Of 149 randomised patients, 107 patients had enthesitis (mean score=2.7) and 81 patients had dactylitis (mean dactylitis score=5.7) at baseline. Mean improvements in enthesitis and dactylitis at week 24 were greater in the guselkumab group versus placebo and sustained through week 56. Similar results were observed for the proportions of patients with resolution of enthesitis and dactylitis. At week 56, mean improvements in enthesitis and dactylitis among patients who switched from placebo to guselkumab treatment were similar to those in the guselkumab group. In the guselkumab group, ACR20 responders had greater improvements in enthesitis and dactylitis versus non-responders (week 24).
Conclusions At week 24, the guselkumab group had greater mean improvements in enthesitis and dactylitis and greater proportions of patients with resolution of enthesitis and dactylitis versus placebo. ACR20 response was associated with improvements in enthesitis and dactylitis.
Trial registration number ClinicalTrials.gov: NCT02319759.
URL: https://clinicaltrials.gov/ct2/show/NCT02319759; Registered 18 December 2014.
- Rheumatoid Arthritis
- Disease Activity
- TNF-alpha
- Lupus Nephritis
- Psoriatic Arthritis
- Spondyloarthritis
- Systemic Lupus Erythematosus
- Chemokines
- Arthritis
- Ankylosing Spondylitis
- Anti-TNF
- Treatment
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
- Rheumatoid Arthritis
- Disease Activity
- TNF-alpha
- Lupus Nephritis
- Psoriatic Arthritis
- Spondyloarthritis
- Systemic Lupus Erythematosus
- Chemokines
- Arthritis
- Ankylosing Spondylitis
- Anti-TNF
- Treatment
INTRODUCTION
Psoriatic arthritis (PsA) is a progressive, inflammatory spondyloarthritis that manifests as musculoskeletal and skin disease. Patients with PsA can experience peripheral arthritis, axial disease, dactylitis and enthesitis as well as skin and nail lesions.1 It has been estimated that more than half of all patients with PsA experience dactylitis and/or enthesitis.2 Enthesitis is a more common presentation in PsA as compared with other forms of inflammatory arthritis such as rheumatoid arthritis or ankylosing spondylitis.3
Enthesitis and dactylitis have considerable impact on patients and are considered as important manifestations for treatment goals. In an analysis from the CORRONA Registry, PsA patients with dactylitis and enthesitis had overall greater disease activity compared with patients who did not have dactylitis and enthesitis, respectively, and patients with enthesitis showed greater levels of functional and work impairment compared with patients who did not have enthesitis.4 Additionally, results from a prospective cohort analysis of patients with PsA showed that patients with enthesitis generally have worse radiographic changes both in peripheral joints and the spine than those without enthesitis.5 When developing the composite measure of minimal disease activity (MDA) for PsA, dactylitis and enthesitis were deemed to be critical aspects, while dactylitis was accounted for in the peripheral tender and swollen joint counts, enthesitis scores were added as a separate criterion in MDA.6 Of note, enthesitis and dactylitis are separate disease domains considered in the treatment recommendations from the Group for Research and Assessment of Psoriasis and Psoriatic Arthritis.7
Evidence from animal models and from human imaging studies are contributing to the growing understanding of dactylitis, enthesitis and their linkages and their mechanisms, which may include common initiating factors such as skeletal mechanical strain.8 Interleukin-23 (IL-23) has been shown to be a key upstream regulator in the pathogenesis of psoriasis9 and has been implicated in the development of dactylitis and arthritis features of PsA.10 Guselkumab, a monoclonal antibody targeting the p19 subunit of IL-23, is approved for the treatment of psoriasis.11 12 The efficacy and safety of guselkumab in adult patients with active PsA was also evaluated in a randomised, placebo-controlled, phase II trial.13 Patients treated with guselkumab 100 mg every 8 weeks had significantly greater improvements in the signs and symptoms of PsA, including dactylitis and enthesitis, compared with placebo at week 24, and efficacy was maintained through 1 year in the guselkumab group.13 Here, we report additional comprehensive analyses of the effect of guselkumab on dactylitis and enthesitis in adults with active PsA.
METHODS
Patients and study design
Patient eligibility criteria and details of the study design have been previously described.13 Briefly, adults (≥18 years) were eligible for enrollment in this phase II, randomised, placebo-controlled trial if they had a diagnosis of PsA for ≥6 months before the first study drug administration and met the ClASsification criteria for Psoriatic ARthritis (CASPAR)14 criteria at screening. Patients had to have active PsA, defined as ≥3 swollen and ≥3 tender joints at screening and baseline and a screening C reactive protein (CRP) level ≥0.3 mg/dL, despite current or previous therapy with conventional synthetic disease-modifying anti-rheumatic drugs, oral corticosteroids, and/or non-steroidal anti-inflammatory drugs (NSAIDs). Up to 20% of the patient population could have had previous treatment with one anti-tumour necrosis factor (TNF) agent. Patients also had to have ≥3% body surface area affected by plaque psoriasis at screening and baseline.
Eligible patients were randomly assigned (2:1) to receive subcutaneous injections of guselkumab 100 mg or placebo at weeks 0, 4 and every 8 weeks through week 44. Patients in the placebo group crossed over to receive guselkumab at weeks 24, 28 and every 8 weeks thereafter. At week 16, patients in both groups who had less than 5% improvement in swollen and tender joint counts were eligible for open-label early escape and switch to ustekinumab, at the approved dosage in the local country.
Assessments
The primary endpoint was the proportion of patients achieving a 20% improvement in the American College of Rheumatology criteria (ACR20 response) at week 24. Severity of skin disease was evaluated using the Psoriasis Area and Severity Index (PASI)15; the proportion of patients achieving ≥75% improvement in PASI score was determined. Dactylitis and enthesitis assessments were performed at weeks 0, 4, 8, 16, 24, 28, 32, 44 and 56. Dactylitis was assessed using a scoring system of 0–3 (0=absent, 1=mild, 2=moderate, 3=severe) based on swelling and erythema for each digit, with a combined range of 0–60.16 Enthesitis was evaluated using the Leeds Enthesitis Index, which assesses tenderness in the left and right lateral epicondyle, medial femoral condyle and Achilles tendon insertion by applying enough pressure to blanch the fingernail (total score 0–6).17 Overall, health-related quality of life was assessed using the 36-item Short-form Health Survey (SF-36) Physical and Mental Component Summary (PCS/MCS) scores.
Statistical analysis
Changes in enthesitis and dactylitis scores and the proportions of patients with complete resolution of enthesitis or dactylitis (ie, score=0) were analysed only in patients who had enthesitis or dactylitis, respectively, at baseline. In addition, the presence of dactylitis at each digit (0–20) was summarised. Missing data were imputed using last observation carried forward through week 24. For patients who met the early escape criteria at week 16, the week-16 data were carried forward through week 24. Data were summarised using descriptive statistics. Between-treatment comparisons of change from baseline in enthesitis score through week 24 were performed using analysis of covariance, and between-treatment comparisons of change from baseline in dactylitis score/the number of digits with dactylitis through week 24 were performed using Wilcoxon rank-sum test. Between-treatment comparisons of the proportions of patients with complete resolution of dactylitis/enthesitis through week 24 were performed using the Cochran–Mantel–Haenszel test. In addition, treatment group comparisons of the proportions of tender entheses (lateral epicondyle, medial femoral condyle and Achilles tendon) at baseline with resolution at week 24 were performed using the χ² test. In this analysis, p values were not adjusted for multiplicity and are nominal.
Observed changes from baseline in dactylitis and enthesitis scores at week 24 by ACR20 and ACR50, PASI 75, PASI 90 and PASI 100 response at week 24 were summarised, and p values were calculated using analysis of covariance model among guselkumab-treated patients who had enthesitis or dactylitis at baseline, respectively, and did not discontinue or early escape prior to week 24.
Spearman correlation analyses were performed for changes in dactylitis scores and enthesitis scores and changes in ACR components (swollen (0–66) and tender (0–68) joint counts, pain visual analog scale (VAS), Physician’s Global Assessment VAS, Patient’s Global Assessment VAS, Health Assessment Questionnaire-Disability Index (HAQ-DI), and CRP), SF-36 PCS and MCS scores, and PASI score at week 24 among guselkumab-treated patients who had enthesitis or dactylitis at baseline, respectively, and did not discontinue or early escape prior to week 24.
After week 24, observed data were reported with no imputation for missing data, and patients who met the early escape criteria or discontinued prior to week 24 were excluded from analyses. No formal hypothesis testing was performed after week 24, when all patients were receiving guselkumab.
RESULTS
Patient demographics and disease characteristics at baseline
The baseline demographic and disease characteristics of the overall population have been previously described in detail.13 A total of 149 patients from 34 sites in seven countries were randomised to receive placebo (n=49) or guselkumab (n=100).
At baseline, 107 patients (71.8%) had enthesitis, with a mean enthesitis score of 2.7 (median=2.0); these patients generally had higher mean numbers of swollen joints and tender joints compared with patients who did not have enthesitis at baseline. Prior medication use was similar for patients with and without enthesitis, with the exception of methotrexate (MTX), which was less commonly used by patients who had enthesitis (table 1). Of the patients with enthesitis at baseline, 51 (47.7%) had enthesitis at the lateral epicondyle, 60 (56.1%) had enthesitis at the medial femoral condyle, and 69 (64.5%) had enthesitis at the Achilles tendon insertion.
Baseline demographic and disease characteristics of patients with and without enthesitis
At baseline, 81 patients (54.4%) had dactylitis with a mean dactylitis score of 5.7 (median=4.0); these patients generally had higher mean numbers of swollen and tender joints and higher CRP levels than did patients without dactylitis at baseline. Prior use of anti-TNF agents, MTX and NSAIDs was generally similar for patients with and without dactylitis at baseline (table 2).
Baseline demographic and disease characteristics of patients with and without dactylitis
Changes in enthesitis
Among patients with enthesitis at baseline, the mean reduction from baseline in enthesitis score was greater in the guselkumab group compared with placebo at week 2413; with separation between the treatment groups observed by week 8 (figure 1A). Mean improvement in enthesitis score in the guselkumab group was maintained through week 56 (figure 1B). In the placebo-crossover group, notable improvements in the mean change from baseline were observed 8 weeks after initiating guselkumab therapy at week 24 and were similar to those in the guselkumab group at week 56 (figure 1B).

Mean change from baseline in enthesitis score through week 24 (A) and week 56 (B) and mean change from baseline in dactylitis score through week 24 (C) and week 56 (D). Through week 24, missing data and data for patients who entered early escape were imputed using last observation carried forward (panels A and C); after week 24, no imputation was made for missing data, observed data were used and patients who early escaped or discontinued prior to week 24 were not included in the analysis (panels B and D). GUS, guselkumab; PBO, placebo.
Among those with enthesitis at baseline, the proportion of patients with resolution of enthesitis was also greater in the guselkumab group compared with placebo (p<0.05) at week 24 (figure 2A). In the guselkumab group, the proportion of patients with resolution of enthesitis was maintained through week 56. Among patients in the placebo-crossover group, the proportion of patients achieving resolution of enthesitis was similar to that in the guselkumab group 8 weeks following crossover to guselkumab therapy and maintained through week 56 (figure 2B). When evaluated by individual site (lateral epicondyle, medial femoral condyle and Achilles tendon), improvements were seen both in upper limb and lower limb sites at week 24 in those patients who had tender entheses at those anatomical sites at baseline and did not early escape (online supplementary figure 1).
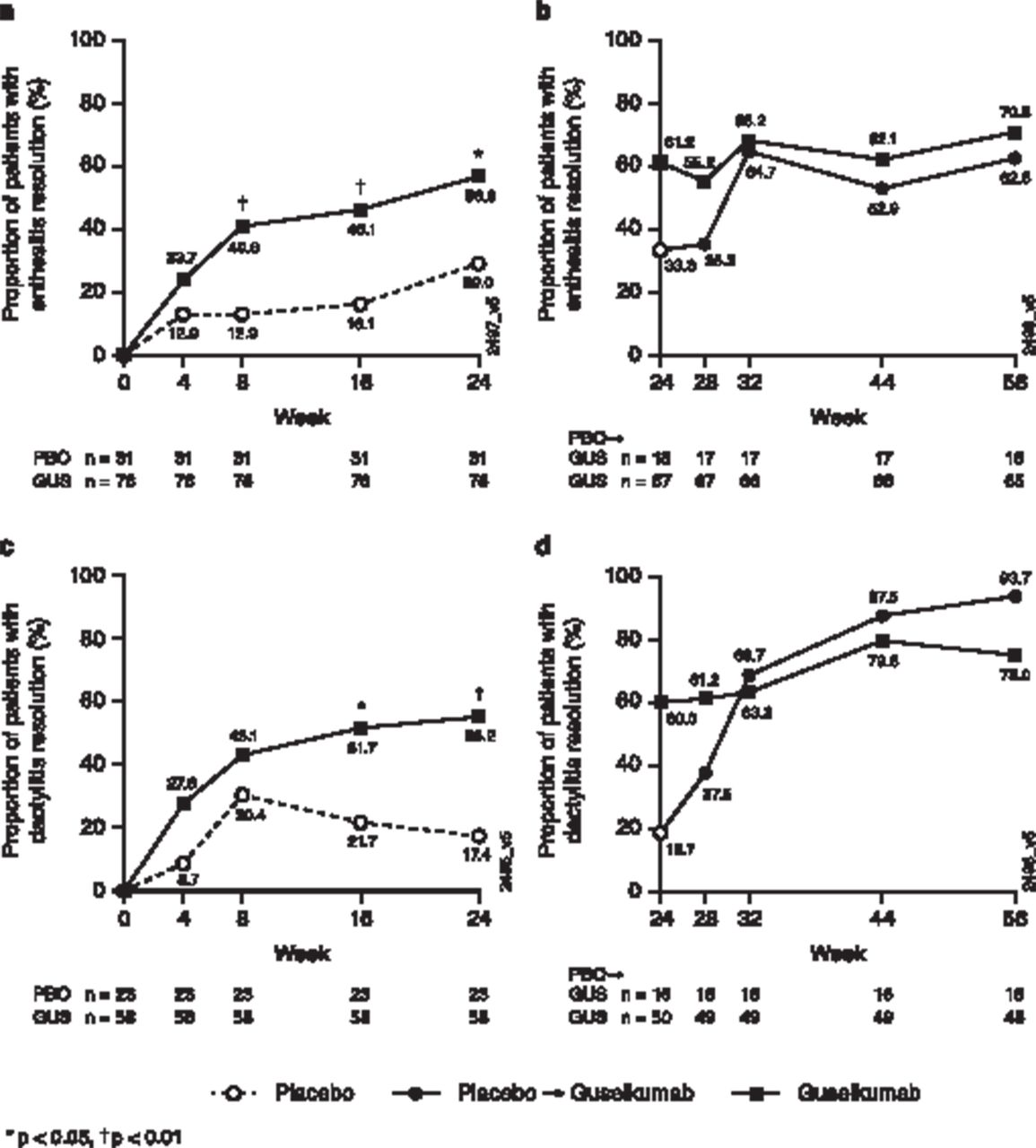
The proportion of patients with resolution of enthesitis through week 24 (A) and week 56 (B) and the proportion of patients with resolution of dactylitis through week 24 (C) and week 56 (D). Through week 24, missing data and data for patients who entered early escape were imputed using last observation carried forward (panels A and C); after week 24, no imputation was made for missing data, observed data were used, and patients who early escaped or discontinued prior to week 24 were not included in the analysis (panels B and D). GUS, guselkumab; PBO, placebo.
Supplemental material
Correlation and association of changes in enthesitis score with improvements in joint, skin and quality of life measures
In the guselkumab group, the mean improvement in enthesitis score was greater for patients who achieved an ACR20 response at week 24 compared with ACR20 non-responders. A similar trend was also observed for ACR50 response after adjusting for baseline factors, while an association between enthesitis improvement and skin response was not consistently seen with PASI 75, PASI 90 and PASI 100 (figure 3A) or changes in PASI score (table 3). Of note, among guselkumab-treated patients, 66.7% (50/75) had improvement in enthesitis score and achieved a PASI 75 response at week 24. Improvements in enthesitis scores in the guselkumab group were moderately correlated with changes from baseline in swollen and tender joint counts, Patient’s Global Assessment, Physician’s Global Assessment and SF-36 PCS and MCS scores (table 3).
Correlations of changes from baseline in dactylitis and enthesitis scores with changes from baseline in other measures of disease activity at week 24 for patients in the guselkumab group

{kind=link}
{kind=link}
{kind=link}
Mean changes from baseline to week 24 in enthesitis score (A) and dactylitis score (B) among ACR20, ACR50, PASI 75, PASI 90, PASI 100 responders and non-responders in the guselkumab group. ACR 20/50, ≥20%/50% improvement in American College of Rheumatology criteria; PASI 75/90/100, ≥75%/90%/100% in Psoriasis Area and Severity Index score. ACR, American College of Rheumatology; PASI, Psoriasis Area and Severity Index.
Changes in dactylitis
Among patients with dactylitis at baseline, the mean improvement from baseline in dactylitis score was greater in the guselkumab group than in the placebo group (p<0.01) at week 24 (figure 1C). Similar results were observed for mean changes from baseline in the number of digits with dactylitis in the guselkumab group compared with placebo (−2.1 vs −0.2; p=0.003) at week 24. Mean improvement in dactylitis score was maintained through week 56 in the guselkumab group (figure 1D). In the placebo-crossover group, noticeable improvements in the mean dactylitis scores were observed 4 weeks after initiating guselkumab therapy (figure 1D).
Among patients with dactylitis at baseline, greater proportions of patients in the guselkumab group achieved resolution of dactylitis at week 24 compared with those in the placebo group (p<0.01; figure 2C). In the guselkumab group, the response rate for resolution of dactylitis was maintained through week 56. Among patients who crossed over from placebo to guselkumab at week 24, the proportion of patients achieving resolution of dactylitis improved following initiation of guselkumab therapy and was maintained through week 56 (figure 2D).
Correlation and association of changes in dactylitis score with improvements in joint, skin and quality of life measures
Among patients in the guselkumab group, patients who achieved an ACR20 or ACR50 response at week 24 had greater mean improvements in dactylitis score compared with non-responders (figure 3B). Mean changes in dactylitis score were similar regardless of PASI 75, PASI 90 or PASI 100 response at week 24 and there was no correlation between changes in dactylitis score and changes in PASI score (table 3). Of note, 66.7% (38/57) of patients treated with guselkumab had improvement in dactylitis score and achieved a PASI 75 response at week 24. Improvements in dactylitis score in the guselkumab group were correlated with improvements in swollen and tender joint counts and HAQ-DI scores at week 24 (table 3). Forty-four patients treated with guselkumab had enthesitis and dactylitis at baseline and available data at week 24; of these, 32 patients had improvements in both enthesitis and dactylitis scores.
DISCUSSION
Enthesitis and dactylitis are important clinical manifestations of PsA and can have substantial detrimental effects on physical function and quality of life. Enthesitis is a key component of developing dactylitis8 18 and, in a previous study, digits with dactylitis had more radiographic joint damage than those without dactylitis.19 To our knowledge, this is the first study to report the effects of treatment with a monoclonal antibody specific to the p19 subunit of IL-23 on enthesitis and dactylitis in patients with PsA.
In this phase II study, patients who received guselkumab had greater improvements in enthesitis and dactylitis scores through week 24, compared with placebo with notable improvements occurring at weeks 8 and 16. The mean changes in enthesitis and dactylitis scores were maintained through week 56 for patients in the guselkumab group. Similar results were observed in the proportions of patients who achieved resolution of enthesitis or dactylitis for patients who were affected at baseline. These improvements were sustained through 1 year.
The Achilles tendon and lateral epicondyle are among the most commonly affected enthesitis sites in patients with PsA and are often affected bilaterally.20 The involvement of the Achilles tendon, in particular, can lead to significant physical impairment and pain21 and is a challenging aspect of treatment in patients with PsA.18 The guselkumab treatment group had improvement in all sites evaluated for enthesitis including lateral epicondyle, medial femoral condyle and Achilles tendon.
It is important to note, however, that clinical assessment of peripheral enthesitis is challenging and may not relate to other, more objective assessments, such as ultrasound of the enthesis. It is also important to note that widespread allodynia may be part of a chronic inflammatory musculoskeletal disorder, and that when the inflammation is abrogated, by whatever means, the allodynia may diminish.22 In practical terms, this may be reflected by improvement in clinical enthesitis scores, independently of any actual improvement in inflammation at the enthesis.23
The IL-23/Th17 axis has been shown to be critical in the pathogenesis of both enthesitis and dactylitis.9 In vivo studies have shown that systemic exposure of IL-23 in a murine model resulted in severe paw swelling as a manifestation of entheseal inflammation.24 Additionally, a recent analysis of entheses of normal human subjects found resident myeloid cells capable of producing IL-23.25 These mechanistic findings have been corroborated with clinical evidence. The results of the ECLIPSA study suggest that enthesitis is sensitive to IL-12/23 p40 inhibition, with a greater proportion of ustekinumab-treated patients having complete resolution of enthesitis compared with those who received anti-TNF therapy.26 Furthermore, preliminary biomarker data from patients in this guselkumab phase II study showed elevations of serum IL-17A and IL-17F at baseline compared with healthy controls, which decreased to levels similar to healthy controls after 16 weeks of guselkumab treatment.27 These results indicate that IL-23p19 subunit inhibition is effective in resolving peripheral enthesitis.
Guselkumab has been reported to significantly improve joint and skin manifestations of PsA.13 In this analysis, improvement in enthesitis was associated with improvements in joint counts, ACR response, and quality of life as measured by SF-36, and improvement in dactylitis was correlated with improvement in joint counts, ACR response, and physical function as measured by HAQ-DI. These results suggest that guselkumab is able to improve multiple domains of disease in patients with PsA and adds to the evidence that enthesitis and dactylitis resolution are important treatment goals.
This was a relatively small, 1-year, phase II trial; however, multiple study sites were included from seven countries. The results reported here are limited by the exploratory nature of these analyses and dactylitis and tender/swollen joint assessments may be confounded. Correlation analyses were also limited due to potential non-linearity of underlying data of various scales used. There is a need to better understand the impact of inhibiting the IL-23 pathway in axial polyenthesitis/osteitis of ankylosing spondylitis; however, spondylitis was not assessed in this study.
CONCLUSIONS
In conclusion, these findings, together with the results previously reported,13 support the contention that IL-23 p19 subunit pathway antagonism is effective for resolving dactylitis and peripheral enthesitis associated with PsA. Further assessment on dactylitis, peripheral and axial enthesitis will be conducted in the ongoing phase III confirmatory studies.
Key messages
What is already known about this subject?
Guselkumab 100 mg was efficacious in reducing the signs and symptoms of psoriatic arthritis (PsA) in adult patients in a phase II study.
What does this study add?
In this study, guselkumab was efficacious in treating enthesitis and dactylitis among adults with PsA. Mean improvements in enthesitis and dactylitis were greater in the guselkumab group than in the placebo group at week 24 and were observed as early as week 8 and week 16, respectively. Greater proportions of guselkumab-treated patients had resolution of enthesitis and dactylitis when compared with placebo, and these response rates were maintained over 1 year. Improvements in enthesitis and dactylitis were correlated with improvements in swollen and tender joint counts. Improvements in enthesitis were also correlated with SF-36 PCS and MCS scores, and improvements in dactylitis were correlated with HAQ-DI improvements at week 24.
How might this impact clinical practice?
Improvements seen with guselkumab treatment in enthesitis and dactylitis, which are an important consideration for treatment of patients with PsA, complement the improvements previously reported in the articular signs and symptoms of PsA. The efficacy of guselkumab on enthesitis and dactylitis in patients with PsA will be further validated in ongoing phase III trials.
Acknowledgments
The authors thank Rebecca Clemente, PhD, of Janssen Scientific Affairs, LLC and Diane Harrison, MD, MPH (consultant funded by Janssen Research & Development, LLC) for writing support.
REFERENCES
Footnotes
Contributors Study design: AD, W-HB, AG, XLX, ECH, PSH. Data collection: XLX, ECH. Data interpretation: PJM, DDG, AD, DGM, PN, W-HB, AG, XLX, SX, ECH, CSK, PSH. Statistical analyses: SX. All authors revised the manuscript and gave final approval for submission.
Funding This study was funded by Janssen Research & Development, LLC.
Competing interests PJM has received research grants or served as a consultant or speaker for AbbVie, Amgen, Bristol-Myers Squibb, Boehringer Ingelheim, Celgene, Eli Lilly, Galapagos, Genentech, Gilead, Janssen Scientific Affairs, Novartis, Pfizer, Sun and UCB.
DDG has received consulting fees and/or grant support from AbbVie, Amgen, Bristol-Myers Squibb, Celgene, Eli Lilly, Galapagos, Gilead, Janssen, Novartis, Pfizer and UCB.
AD reports grants, personal fees and non-financial support from Janssen, during the conduct of the study; grants and medical writing support from AbbVie and Amgen; grants and personal fees from Eli Lilly; and grants, personal fees and medical writing support from Novartis, Pfizer and UCB.
DGM has received research grants from AbbVie, Eli Lilly, Janssen, Novartis and Pfizer and has received honoraria from AbbVie, Celgene, Eli Lilly, Janssen, Pfizer and UCB.
PN has received research funding for clinical trials and honoraria for advice and lectures on behalf of Abbvie, BMS, Celgene, MSD, Pfizer, Sanofi, Roche, Janssen, Gilead, UCB, Novartis, and Lilly.
W-HB has received personal fees from Janssen, AbbVie, Almirall, Bristol-Myers-Squibb, Celgene, Eli Lilly, Janssen, Leo, Novartis and UCB, and grants from Pfizer.
AG has received consulting and/or advisory board fees from AbbVie, Allergan, Avotres Therapeutics, Beiersdorf, Boehringer Ingelheim, Bristol-Myers Squibb, Celgene, Eli Lilly, Incyte, Janssen, Leo, Reddy Labs, Sun Pharmaceutical Industries, UCB, Valeant and Xbiotech, and grants from Boehringer Ingelheim, Incyte, Janssen, Novartis, UCB and Xbiotech.
PSH has received research grants from AbbVie, Janssen and Novartis, and has received honoraria from AbbVie, Amgen, Celgene, Galapagos, Pfizer, and UCB.
XLX, SX and ECH are employees of Janssen Research & Development, LLC, and own stock in Johnson & Johnson, of which Janssen Research & Development, LLC is a wholly owned subsidiary. CSK is an employee of Janssen Global Services, LLC, and owns stock in Johnson & Johnson, of which Janssen Global Services, LLC is a wholly owned subsidiary.
Patient consent for publication Not required.
Ethics approval This trial was conducted in accordance with Good Clinical Practice and the Declaration of Helsinki. The protocol was approved by the Institutional Review Board or ethics committee at each site. All patients gave written informed consent before any study-related procedures were performed.
Data sharing statement Data are available upon reasonable request.
Data availability statement The data sharing policy of Janssen Pharmaceutical Companies of Johnson & Johnson is available at URL: https://www.janssen.com/clinical-trials/transparency. As noted on this site, requests for access to the study data can be submitted through Yale Open Data Access (YODA) Project site at URL: http://yoda.yale.edu.
Provenance and peer review Not commissioned; externally peer reviewed.