Article Text

Abstract
Objectives To compare the construct validity of three presenteeism instruments, using health and economic outcomes as external references, among working persons reporting musculoskeletal complaints.
Methods Data from the prospective Study on Transitions in Employment, Ability and Motivation were used. Presenteeism measurement comprised a global rating of work-ability, and two instruments indicating at-work productivity, and was assessed yearly over 6 years of follow-up. Longitudinal associations between measures of health and subsequent presenteeism, and between presenteeism and subsequent days of sick leave were assessed using generalised estimating equation models. The effect of groups of contextual factors (socio-demographic, lifestyle, personal and work-related factors) was investigated by assessing the change in explained variability.
Results In total, 4523 persons were analysed. The association between physical health and work-ability was stronger than both at-work productivity measures; 10 points increase in physical health (0–100, higher is better) was associated with 0.79 points (95% CI 0.75 to 0.84) better work-ability (0–10, higher is better) in the subsequent year. Besides, work-ability best predicted sick leave; one point higher work-ability was associated with 4 days less sick leave (95% CI −5.09 to −3.63) the subsequent year. Personal factors improved model fit for models on health and work-ability, but conflicting results were seen for both at-work productivity instruments.
Conclusion Work-ability showed higher construct validity against health and economic outcomes as compared to at-work productivity, which shows that work-ability is different to productivity (losses). Personal factors are especially relevant when interpreting the relation between health and work-ability or self-reported quantity of work.
- Epidemiology
- Outcome Assessment
- Healthcare
- Patient Reported Outcome Measures
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
INTRODUCTION
Presenteeism among working persons with rheumatic and musculoskeletal (MSK) diseases is highly prevalent, and several studies related presenteeism to patients’ health outcomes, as well as to an economic impact for the workplace and society.1–3 It has been suggested that the costs of presenteeism exceed the costs due to sick leave (ie, absenteeism) and permanent work disability.4 Although there is still considerable debate on the definition of presenteeism, two main aspects can been distinguished, reflecting (1) the behaviour of attending work while ill and (2) the amount of impact on work when being ill at work.5 6
However, it has been insufficiently recognised that self-reported instruments measuring the amount of presenteeism operationalise presenteeism in different ways. Two broad approaches can be distinguished. While one group of instruments focuses on estimating the economic consequence (eg, the productivity, quantity of work, efficiency, time being not productive), other instruments aim to assess person’s difficulty or ability to perform paid work. This resulted in significant variations of effect sizes between presenteeism instruments and health or economic outcomes.1 5 7 Other reasons for the variation in effect sizes can be attributed to differences in instrument properties (eg, recall period, attribution to overall health or disease-specific restrictions), or the level in which approaches mix the behaviour to attend work with the level and type of impact (ability or productivity) while at work into one instrument.5
Despite the large number of studies reporting on validation and psychometric properties of presenteeism instruments in rheumatology, there are still considerable knowledge gaps. First, few studies directly compared the validity (ie, the degree to which an instrument measures the construct(s) it purports to measure) of different presenteeism instruments.1 8–10 This is relevant, as the different constructs used in available instruments might determine their use in future studies. Although it might be expected that presenteeism instruments addressing ‘work-ability’—as compared to those measuring ‘at-work productivity’—would correlate better with physical and mental health, this has never been formally tested (ie, construct validity). In addition, it is unknown whether constructs differ in their ability to predict subsequent sick leave. Such knowledge is relevant, as it might determine their use in trials and even clinical practice. Second, there is limited evidence regarding the association between different presenteeism constructs and contextual factors (eg, personal or work-related factors). The role of context seems especially important when interpreting work outcome studies.1 11 The aims of our study were twofold: (1) to investigate the construct validity of different approaches to measure presenteeism by associating these instruments with important measures of health and sick leave and (2) to explore the influence of contextual factors on these associations.
METHODS
Data source and sample selection
Study on Transitions in Employment, Ability and Motivation (STREAM) is a prospective cohort study of persons aged 45–64 years in the Netherlands stratified by age and employment status (ie, employed, self-employed and unemployed). From the inception of the cohort in 2010 onwards, participants completed an online questionnaire every year on topics such as work characteristics, health and work productivity. A more detailed description of the STREAM design has been published elsewhere.12 At the time of the fifth time point (2015), a second cohort was initiated and linked to the first one, consisting of employed and unemployed persons aged 45–49 years and employed persons in the other age groups (50–54, 55–59, 60–64 years).
For this study, data from the first time point (2010) until the last available time point (2016) were used. We included persons employed or self-employed at baseline who completed the questionnaires on at least two consecutive time points and reported MSK complaints at ≥50% of the available time points. At each time point, the presence of MSK complaints was assessed and considered present if persons responded positively to at least one of the three options of the following question: ‘Do you have one or more of the following long-standing diseases, conditions or handicaps?’ (a) complaints of the hands or arms (also arthritis, repetitive strain injury (RSI)), (b) complaints of the legs and feet (also arthritis) and (c) complaints of the back or neck (also arthritis, RSI).12
The Medical Ethical Committee of the VU University Medical Center (Amsterdam, the Netherlands) declared that the Medical Research Involving Human Subjects Act does not apply to the STREAM, and indicated to have no objection to the execution of this research under the condition all data would be treated confidentially and stored in secured computer systems.
Presenteeism instruments
A variable addressing work-ability was obtained from the first item of the Work Ability Index, in which persons rate their ‘current work-ability as compared to their lifetime best’ (continuous, range 0–10, higher is better).13 14 In addition, two variables addressing at-work productivity were obtained. One assessing the quantity of work by the first item of the Quality and Quantity-method from Brouwer et al, which asks persons to rate ‘how much work they have done in the last 4 weeks compared to normal’ on days they actually worked (continuous, range 0–10, higher is better).15 And the other, loss of productive time while at work in the past month due to presenteeism, was derived from three items of the ‘Osterhaus-method’ (continuous, range 0–30, higher is worse, not included at the first time point).16 17 To allow comparison of the Osterhaus-method with the other two presenteeism instruments, we standardised the Osterhaus-method by dividing values by three (new range 0–10). A more detailed description of the measurement characteristics of each instrument is shown in table 1.
Characteristics of the three presenteeism instruments used in the STREAM cohort
External measures
Health variables
Physical and mental health were assessed at each time point by the 12-Item Short-Form Health Survey (SF-12), from which a physical component summary score and mental component summary score were calculated.18 To assess vitality, not included in the SF-12, three items from the SF-36 (Medical Outcomes Study 36-item Short-Form Health Survey) were included, allowing computation of a weighted vitality domain score.19 For all three variables, higher scores indicate better perceived health/vitality (range 0–100).
Sick leave
Sick leave days in the past year (0–365) was assessed at each time point by the following open question: ‘How many work days have you, during the past 12 months, been absent due to sickness?’
Contextual factors
At each time point, four domains representing different types of contextual factors were collected, except the socio-demographic factors that were assessed at baseline only.
Socio-demographic factors
Three socio-demographic factors were included: age, gender and educational level.
Age was dichotomised based on the median value (≤55 vs >55 years). Education was categorised into three groups: (1) low (primary school, lower and intermediate secondary school or lower vocational training), (2) medium (higher secondary school or intermediate vocational training) and (3) high (higher vocational training, university or higher).
Lifestyle factors
Lifestyle factors comprised body mass index (in kg/m2), currently smoking (yes vs no) and weekly physical exercise (at least 3 days of intensive physical exercise for more than 20 min or more, yes vs no).
Personal factors
Mastery, that is, the feeling to which a person perceives him/herself to be in control of events, was assessed with the Pearlin Mastery Scale (range 1–5, higher is better). Three different coping styles (ie, active response, avoidant behaviour and seeking social support) were measured using the Utrecht Coping List. Mean values for each coping style were calculated (range 1–4, higher is better). Finally, self-efficacy in relation to work (learning new tasks/new employer) was measured using four newly constructed items based on the guidelines by Bandura et al, and mean values were calculated for each participant (range 1–5, higher is better).12
Work-related factors
Four work-related factors were collected: physical workload (five items, higher is worse), psychological job demands (three items, higher is worse), emotional job demands (three items, higher is worse) and autonomy (five items, higher is better). Mean values for each work-related factor were calculated (range 1–5).12
Statistical analysis
Descriptive statistics were used to report the baseline characteristics of the included participants. Spearman’s ranked correlations were used for testing correlations across the three presenteeism instruments. The longitudinal association between the three presenteeism instruments and the four external measures was tested using autoregressive generalised estimating equation (GEE) models with 1-year time lags, first with no adjustment (‘basic model’), and second with adjustment for a priori selected variables (contextual factors listed earlier). Time-varying variables were modelled as such. The ‘exchangeable’ correlation structure was found to be the most appropriate, in all GEE models, to take into account within-subject correlations over time. Of note, GEE models are considered fairly robust with regard to missing data, and therefore no missing data were imputed. In the analyses exploring the association between health variables (physical and mental health, vitality) and presenteeism, the health variables were modelled as the explanatory variables and presenteeism as the outcome. In the analyses that included sick leave, the three presenteeism instruments were modelled as the explanatory variables and the total days of sick leave in the following year as the outcome. Interactions with age, gender, educational level and physical workload (all at baseline) were tested. Significant interactions (p<0.10) were visualised in a graph, and if considered clinically relevant (>10% difference in slopes), the associations of interest were tested in stratified models. If proven not significant or relevant, variables were included as additional confounders in the adjusted models.
Sensitivity analyses included GEE models assuming a negative binomial distribution for the analyses that included sick leave, which has a right-skewed distribution. Quasi-likelihood under the Independence model Criterion (QIC) was used to gain insight into which domain of contextual factors has the largest impact on model fit (explained variability of the outcome by the model), with lower QICs reflecting better data fit.20 Contextual factors were added as one group from each domain separately to the basic model. P values <0.05 were considered statistically significant. All analyses were done using Stata/SE version 15.1.
RESULTS
Descriptive statistics
A total of 4523 participants were included in our analyses, of which 2986 started in 2010 (baseline first cohort) and 1537 participants in 2015 (baseline second cohort). No clinically important differences on baseline characteristics between the two cohorts were observed (data not shown), and these were therefore combined in all further analyses. The mean number of completed timepoints for the participants in the first cohort was 4.9 (SD 1.4) out of a maximum of six. Participants were on average 53 years old (SD 5.4), predominantly female (54%) and MSK complaints were reported by 3440 (76%) participants at baseline (see table 2). No clinically important differences on baseline characteristics were found between completers and non-completers (data not shown).
Baseline characteristics of the study participants (n=4523)
Mean (SD) values were 7.6 (1.7) for work-ability, 5.7 (2.0) for quantity of work performed and 0.9 (1.6) for the standardised Osterhaus-method at the first available measurement for each instrument and remained stable at the group level across all timepoints (table 2). Correlations between the three presenteeism instruments at each timepoint were significant but weak (r: −0.28 to 0.26).
Longitudinal association between health and presenteeism
Statistically significant interactions between the health variables and the four pre-specified effect modifiers were observed but were not considered clinically important. Thus, all models were fit without stratification. Most longitudinal associations between the health variables and the presenteeism instruments were statistically significant (table 3). However, the associations of all health variables with work-ability were stronger as compared to the other two approaches to assess presenteeism. This was especially clear for the association between physical health and work-ability: an increase of 10 points in physical health is longitudinally associated with an increase of 0.79 points (95% CI 0.75 to 0.84) in work-ability in the subsequent year. Similarly, for the ‘quantity of work’ instrument, an increase of 10 points in physical health is longitudinally associated with an increase of 0.53 points (95% CI 0.47 to 0.60) in the subsequent year, and for the standardised Osterhaus-method, this association was −0.41 (95% CI −0.46 to −0.37).
Longitudinal association between health variables (independent variables) and three presenteeism instruments (outcomes) in working persons reporting MSK complaints (N=4523)
Longitudinal association between presenteeism and sick leave days
All three presenteeism instruments showed a statistically significant association with the number of sick leave days in the subsequent year (see table 4). However, work-ability showed a stronger association with sick leave as compared to the other two approaches; one point better work-ability was longitudinally associated with 4.36 (95% CI −5.09 to −3.63) less days sick leave in the subsequent year. This was 1.85 (95% CI: −2.30 to −1.40) less days sick leave for one point better on the ‘quantity of work’ instrument and 1.49 (95% CI: 0.88 to 2.11) more days sick leave for one point worse on the standardised Osterhaus-method. Sensitivity analyses assuming a negative binomial distribution of the outcome showed similar results (data not shown).
Longitudinal association between three presenteeism instruments (independent variables) and sick leave days (outcome) in the subsequent year in working persons reporting MSK complaints (N=4523)
Contextual factors
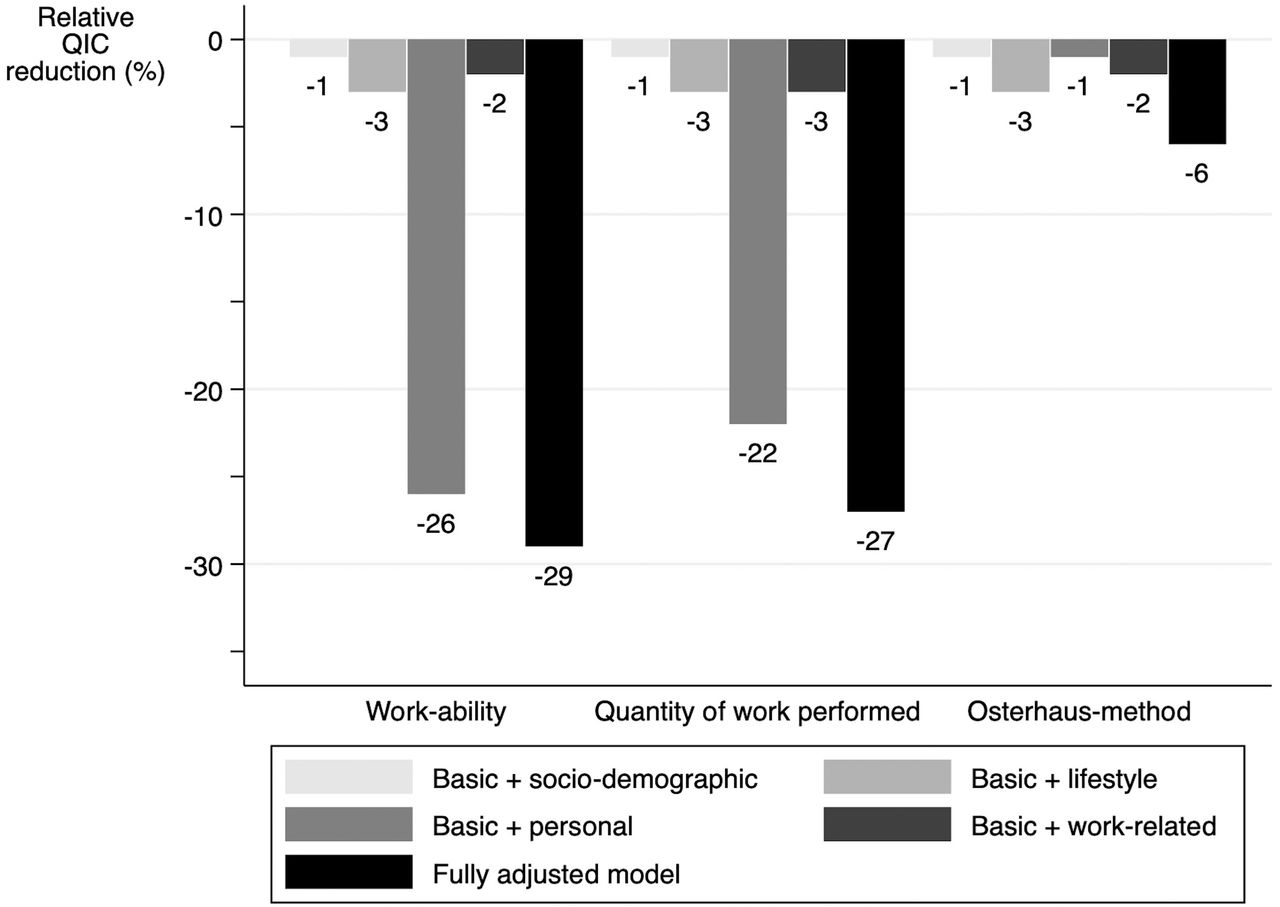
The influence of socio-demographic, lifestyle and work-related factors was small in models exploring the influence of health on subsequent presenteeism, while considerable improvements in explained variability were observed when personal factors were added to the models for work-ability (relative QIC reduction of 26%) or ‘quantity of work’ (relative QIC reduction 22%) (figure 1). The influence of personal factors in the analysis with the standardised Osterhaus-method was negligible (relative QIC reduction 1%).

Comparison of improvement of model fit by adding contextual factors by domain as one group to the models that included all health variables (independent variables) and presenteeism (outcomes), separately for the three presenteeism instruments. Model fit improvement is shown as the relative improvement in QIC as compared to the ‘basic model’ (not adjusted for any contextual factors). Higher relative reduction of the QIC indicates a better model fit. QIC, Quasi-likelihood under the Independence model Criterion.
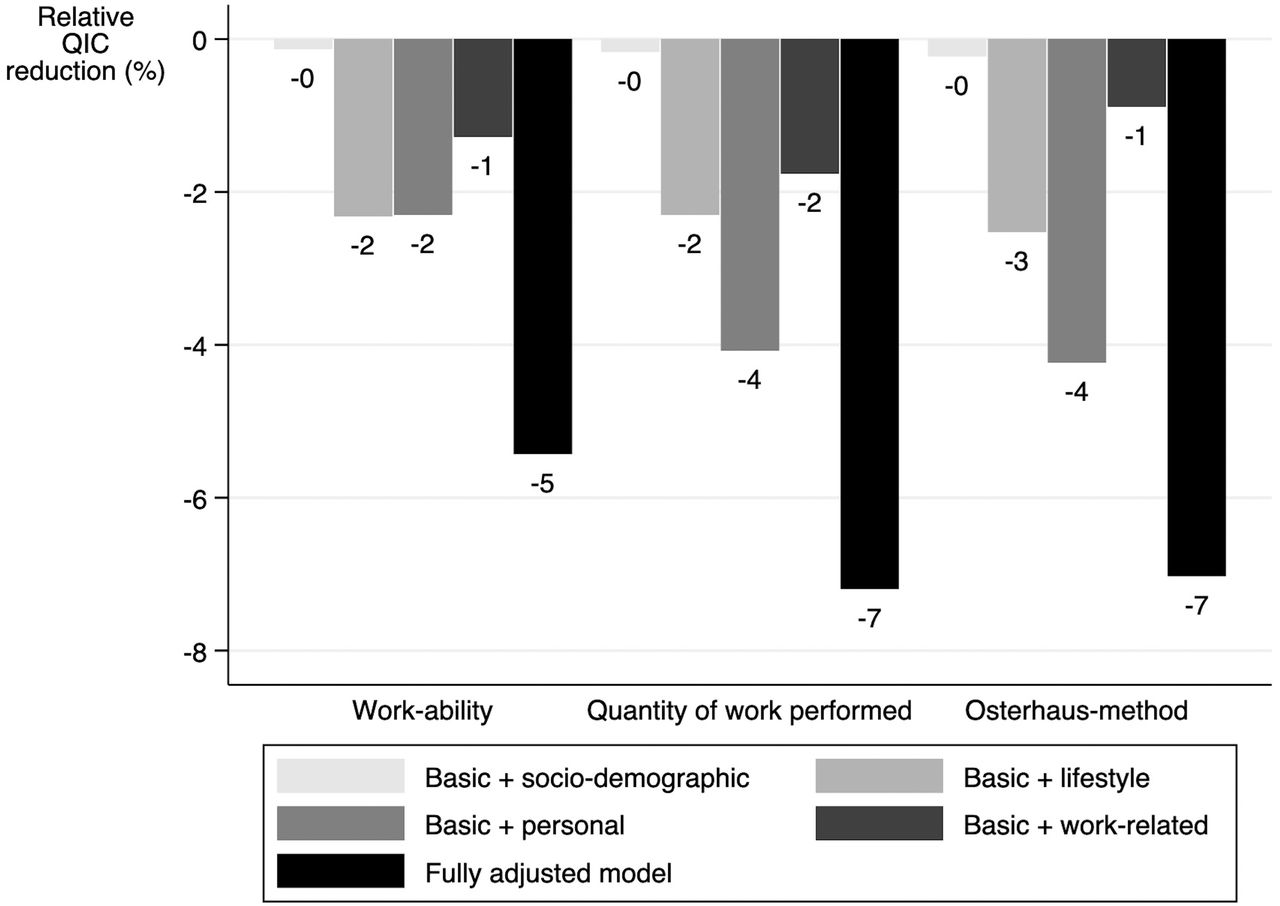
In the models exploring presenteeism as a predictor of subsequent sick leave, improvement in explained variability by any of the contextual factor domains was small (figure 2).
{kind=link}
{kind=link}
Comparison of improvement of model fit by adding contextual factors by domain as one group to the models that included the presenteeism instruments (independent variables) and sick leave (outcome), separately for the three presenteeism instruments. Health variables are not included in these models. Model fit improvement is shown as the relative improvement in QIC as compared to the ‘basic model’ not adjusted for any contextual factors. Higher relative reduction of the QIC indicates a better model fit. QIC, Quasi-likelihood under the Independence model Criterion.
DISCUSSION
This study compares the construct validity over time of three self-reported instruments that measure presenteeism through two different constructs, work-ability and at-work productivity, in working persons reporting MSK complaints. Overall, work-ability showed better longitudinal construct validity against health variables and sick leave as external measures.
Particularly, physical health had a higher impact on work-ability than on both at-work productivity instruments. This finding suggests that, despite the impact of disease on work-ability, persons with MSK complaints mostly succeed to avoid impact on productivity. Our data also confirm that work-ability and productivity are truly different consequences of disease on work, as was also shown by the poor intercorrelation of the three instruments.
In a recent cognitive debriefing study, it was revealed that patients correctly interpret ‘productivity’ as the amount of work accomplished in a specific period of time, while ability relates to the difficulties when performing work.8 Previous studies have shown that different contextual factors have an important impact on presenteeism.21–23 Interestingly, our study shows that personal contextual factors (ie, mastery, coping and self-efficacy) had a larger impact on presenteeism than demographic, lifestyle and work-related contextual factors. These personal factors particularly impacted presenteeism when operationalised as work-ability or quantity of work, while this effect was less evident when presenteeism was measured as loss of productive time while at work (Osterhaus-method).
In this data set, we did not observe relevant effect modification of age, gender, education or physical workload on the relation between health and presenteeism. The absence of relevant effect modification by education or physical workload was somewhat surprising, as it is in contrast to some other studies in MSK disorders.11 24 It is of note that we had no information available on disease duration and we cannot exclude the contextual factors we explored, for example, coping, would have a different role in persons with shorter term opposed to chronic complaints. Also, other work-related factors such as adaptations at work or attitudes of colleagues might have modified the impact of health on presenteeism.
Our results add to the existing body of literature showing that presenteeism is a risk factor for subsequent (long-term) sick leave.25–28 However, in addition, we demonstrate that the impact of health on work-ability is more important than the perceived impact on productivity in contributing to take sick leave. Contextual factors had limited impact on the relation between presenteeism and subsequent sick leave. As discussed earlier, health is an important predictor of presenteeism, and presenteeism is in turn associated with subsequent sick leave. The relation between health and presenteeism is impacted by contextual factors, and therefore, contextual factors likely do not further impact the relation between presenteeism and sick leave. In other words, context is already implicitly included in those presenteeism instruments. This was also the reason not to adjust for the health variables in the analyses with presenteeism and sick leave, as it may lead to over-adjustment.
In the area of MSK and rheumatic disease, Outcome Measures for Arthritis Clinical Trials performed significant work regarding the evaluation of validity and clinimetric characteristics of presenteeism instruments. This previous work has primarily been based on cross-sectional data hampering the understanding of causal relationships with external measures, such as health variables and sick leave.1 The current study fills this knowledge gap by using a large prospective cohort study and including a comprehensive list of questionnaires, contextual factors and sick leave at the same time. The current study pinpoints to the poor intercorrelation and differences in longitudinal construct validity of the different self-reported presenteeism measurement instruments. It also makes clear that, for patients, work-ability is a more relevant measure of presenteeism to be included in clinical trials and can be used when aiming to identify those persons at risk for subsequent (long-term) sick leave.25 However, from an economic perspective, the method by Osterhaus et al is a good choice, because it allows for the calculation of the costs associated with presenteeism based on the self-reported time lost while at work by each person. The frequently used Work Productivity and Activity Impairment Questionnaire, which was not included in this study, has the apparent advantage to measure presenteeism and sick leave in one instrument. However, presenteeism and sick leave appear to be two competing outcomes, which questions the validity of measuring these outcomes in one instrument.
A limitation of this study is that the time interval between two successive time points (ie, 1 year) may have been too large, causing underestimation of the associations between the presenteeism instruments and external measures. Future studies using shorter time intervals between successive time points (eg, several weeks) should be designed to validate our results. Second, the population used in this study was aged 45–67 years and including a younger population in future studies may be interesting, because adverse work outcomes may have long-term consequences and possibly other contextual factors play a more significant role in younger working persons. It would also be interesting to explore the mediating effects of presenteeism in the relation between health and sick leave.
In conclusion, work-ability showed higher construct validity against health and economic outcomes as compared to the two at-work productivity instruments. Our findings suggest that work-ability is not equal to (loss of) at-work productivity and this is likely influenced by contextual factors. Especially, personal factors seem to be relevant when interpreting the relation between health and work-ability. The construct of instrument used in future studies to measure the concept of presenteeism is strongly dependent on the study type and objectives.
Key messages
What is already known about this subject?
Presenteeism among working persons with rheumatic and musculoskeletal diseases is highly prevalent causing a substantial personal and societal burden, and several self-reported instruments exist that aim to estimate the amount of presenteeism.
What does this study add?
This is the first study in musculoskeletal disease directly comparing the construct validity of three instruments, measuring two different constructs (work-ability and at-work productivity) of the concept presenteeism, using a longitudinal design.
Although work-ability and at-work productivity are both constructs that operationalise the concept presenteeism, work-ability better reflects the consequences of health on presenteeism than at-work productivity, and is a better predictor of subsequent sick leave.
How might this impact on clinical practice?
This study supports the work regarding evaluation of validity and clinimetric characteristics of presenteeism instruments performed by OMERACT (Outcome Measures for Arthritis Clinical Trials) and will help determine the use of presenteeism instrument in trials and clinical practice.
REFERENCES
Footnotes
Contributors LvdB designed the study, carried out the analyses and wrote the paper. AS designed the study, contributed to data analysis, data interpretation and writing of the manuscript. GG contributed substantially to the acquisition of the data and writing of the manuscript. RO, GJD and AB contributed to data interpretation and writing of the manuscript. RL contributed to data analysis, data interpretation and writing of the manuscript.
Funding The Study on Transitions in Employment, Ability and Motivation (STREAM) was supported by the Dutch Ministry of Social Affairs and Employment. The funder had no role in the study design, data collection, data analysis, data interpretation or writing of the manuscript.
Competing interests None declared.
Patient consent for publication Not required.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement The data that support the findings of this study are available from TNO Healthy Living (Leiden, the Netherlands), but restrictions apply to the availability of these data, which were used under licence for the current study, and so are not publicly available. Data are however available from the authors upon reasonable request and with permission of TNO Healthy Living (Leiden, the Netherlands).