Article Text

Abstract
Objectives To explore treatment outcomes preferred by patients with early rheumatoid arthritis (RA) and how these change throughout the early disease stage across three European countries.
Methods A longitudinal, qualitative, multicentre study was conducted in Belgium, the Netherlands and Sweden. 80 patients with early RA were individually interviewed 3–9 months after treatment initiation and 51 of them participated again in either a focus group or an individual interview 12–21 months after treatment initiation. Data were first analysed by country, following the Qualitative Analysis Guide of Leuven (QUAGOL). Thereafter, a meta-synthesis, inspired by the principles of meta-ethnography and the QUAGOL, was performed, involving the local research teams.
Results The meta-synthesis revealed 11 subthemes from which four main themes were identified: disease control, physical performance, self-accomplishment and well-being. ‘A normal life despite RA’ was an overarching patient-preferred outcome across countries. Belgian, Dutch and Swedish patients showed many similarities in terms of which outcomes they preferred throughout the early stage of RA. Some outcome preferences (eg, relief of fatigue and no side effects) developed differently over time across countries.
Conclusions This study on patient-preferred outcomes in early RA revealed that patients essentially want to live a normal life despite RA. Our findings help to understand what really matters to patients and provide specific insights into the early stage of RA, which should be addressed by clinicians of different disciplines from the start of treatment onwards.
- Arthritis
- Rheumatoid
- Outcome and Process Assessment
- Health Care
- Qualitative research
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
INTRODUCTION
There is a range of outcome measures for rheumatoid arthritis (RA) available to evaluate disease status and changes under treatment (eg, swollen joint count and patient assessment of pain). Progress in RA treatment was achieved by recognising that patient-preferred outcomes are also clinically important outcomes.1 Although initiatives are being taken to integrate the patient perspective in the outcome measurement of RA,2 3 this remains a challenge in clinical practice. Busy clinicians in modern healthcare systems striving for efficiency may tend to be less open to the patient perspective.4 It is, however, important to consider patient-preferred outcomes when making treatment decisions, since patients with RA may have other or additional priorities and treatment expectations than clinicians.5 Relief of symptoms, mobility and independence are examples of patient-preferred outcomes previously found in qualitative interview studies.6–9
Remarkably, only limited evidence is currently available on what matters most to patients with early RA, while this patient group is likely to have specific outcome preferences related to the early disease stage,10 11 which may also change over time.8 12 A more comprehensive understanding of this patient group’s priorities and treatment expectations is needed to provide care that responds quickly and efficiently to patients’ outcome preferences.
A qualitative interview study in Belgium provided insight into patient-preferred outcomes in early RA, revealing changing outcome preferences in the early stages after diagnosis of RA and treatment initiation and with a return to normality as an overarching patient-preferred outcome.13 The current literature in established RA suggests, however that the local context with its specific cultural characteristics influences how patients evaluate their disease.14 15 Furthermore, variation exists in how rheumatology services are implemented locally, despite international treatment recommendations.16 17 The need for a multinational, longitudinal, qualitative study was met by designing the European Qualitative research project on Patient-preferred outcomes in Early Rheumatoid Arthritis (EQPERA).18 In the present article, we examined the transferability of the Belgian findings and explored treatment outcomes preferred by patients with early RA and how these change throughout the early disease stage across three European countries.
METHODS
Research context
EQPERA involved three countries in Northwest Europe: Belgium, the Netherlands and Sweden. The countries are all ranked highly on the 2018 Euro Health Consumer Index, indicating well-developed healthcare systems.19 Their gross domestic product illustrates significant investments in healthcare.20 They have comparable healthcare systems, although there are minor differences in terms of, for example, clinician referral and the reimbursement of RA treatment.
Study management
A longitudinal, qualitative, multicentre study was independently conducted in each country, following the same research protocol and guided by a local principal investigator (KVdE, EGEM and IL). Data collection and analysis were independently performed by the local research teams in their native language. The steering group of EQPERA consisted of an interdisciplinary team, including nurses (KVdE, EGEM, IL and YvE-H), physiotherapists (AB and ADG), a psychologist (JEV) and a rheumatologist (RW). In each country, at least one patient research partner was involved in the study process as an active team member, supporting the local research team by sharing his/her lived experience with RA. Details on methodology are published in a protocol article.18
Study design
A multinational, longitudinal, qualitative study design was applied. The study design was co-developed with two Belgian patient research partners and included individual interviews at the first time point and focus groups at the second time point. The study was first conducted in Belgium (2012–2013).13 Thereafter, the study design was updated by adding the possibility of individual interviews at t2 and the study was conducted in the Netherlands (2016–2018) and Sweden (2017–2018).21 22 An overview of the study design is shown in figure 1.
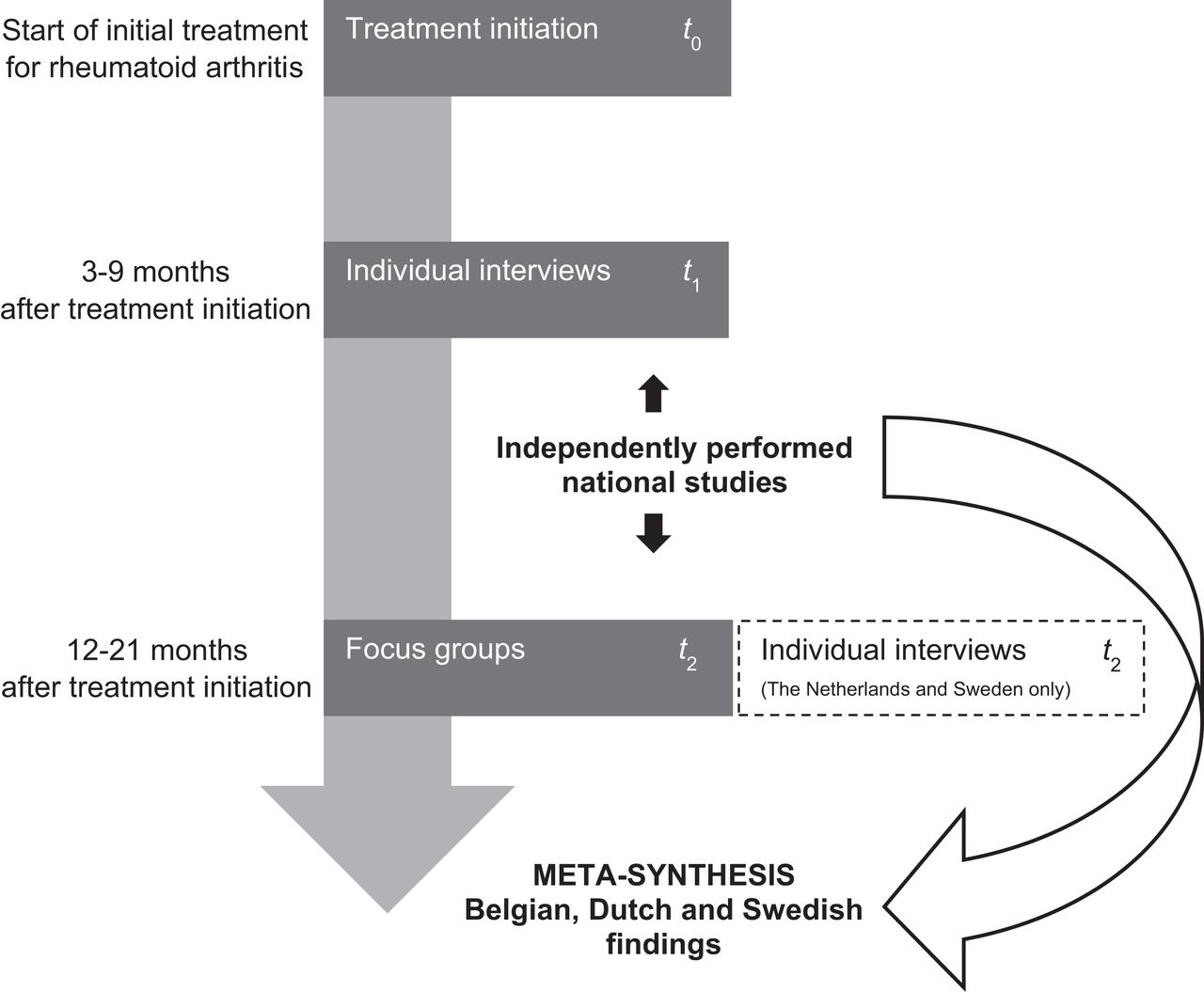
Overview of the study design. t, time point.
Participants
Patients who met the following criteria were eligible for participation: (1) minimum age of 18 years, (2) confirmed diagnosis of RA according to the 2010 American College of Rheumatology/EULAR classification criteria,23 (3) disease duration ≤1 year and (4) treatment initiation 3–7 months ago. Patients were purposefully recruited based on their age, gender and treatment experience to cover a wide range of perspectives. Moreover, patients were recruited from rheumatology centres across different geographic locations in each country. Eighty patients were individually interviewed across Belgium, the Netherlands and Sweden at t1. The sample size was guided by the principles of data saturation.24 Fifty-one patients were interviewed again at t2. Thirty-eight of them participated in a focus group and 13 in an individual interview. A flow chart of participant recruitment is shown in online supplemental file 1. Patients received usual care according to local standards and in respect of the current RA treatment principles of treating early, intensively and to a target of sustained remission or low disease activity.25 26 Patients were interviewed 3–9 months after treatment initiation at t1 and 12–21 months after treatment initiation at t2. Characteristics and treatment details of Belgian, Dutch and Swedish patients are presented in table 1.
Characteristics and treatment details of Belgian, Dutch and Swedish patients, grouped by time point (t1 or t2)
Supplemental material
Data collection
Individual interviews at t1 lasted 15–75 min and were conducted by a local interviewer (KVdE/SM, EGEM and EL/IL). The interviews started by requesting patients to write down keywords regarding their priorities and treatment expectations, before progressing to the open-ended question ‘Which outcomes of your disease and antirheumatic treatment are important to you at this moment?’ and follow-up questions. Outcome preferences were further explored at t2 and patients were additionally inquired about change over time. The 1–1.5-hour focus groups consisted of three rounds that were designed to maximise group interaction.27 A local interviewer from t1 facilitated the focus groups and was assisted by a participating observer. Individual interviews at t2 took place in the Netherlands and Sweden with patients who would otherwise drop out due to personal or practical reasons. Individual interviews and focus groups were audio-recorded, transcribed and anonymised. Interview guides can be found in the protocol article.18
Data analysis
Data collection and analysis were performed simultaneously. Transcripts were analysed by country according to the principles of the Qualitative Analysis Guide of Leuven (QUAGOL), including the constant comparative method.28 An overarching framework of themes and subthemes was identified in each country. The method described by Saldaña helped to discover meaningful changes in patient-preferred outcomes between t1 and t2.29 Patient research partners assisted in data interpretation in each country. Our meta-synthesis was inspired by the principles of meta-ethnography, as practised by Britten and colleagues,30 and the coding process of the QUAGOL, which is based on the principles of grounded theory.28 The key methodological elements were summarised in four steps: describing the findings of each country, recognising differences, similarities and patterns across countries, disentangling these differences, similarities, and patterns, and a fitting test of the meta-interpretations. The local research teams collaborated in a face-to-face consensus meeting to perform the first three steps. Thereafter, step 4 was performed by the local principal investigators (KVdE, EGEM and IL). The meta-synthesis revealed 11 subthemes from which four main themes were identified that together gave meaning to an overarching theme.
RESULTS
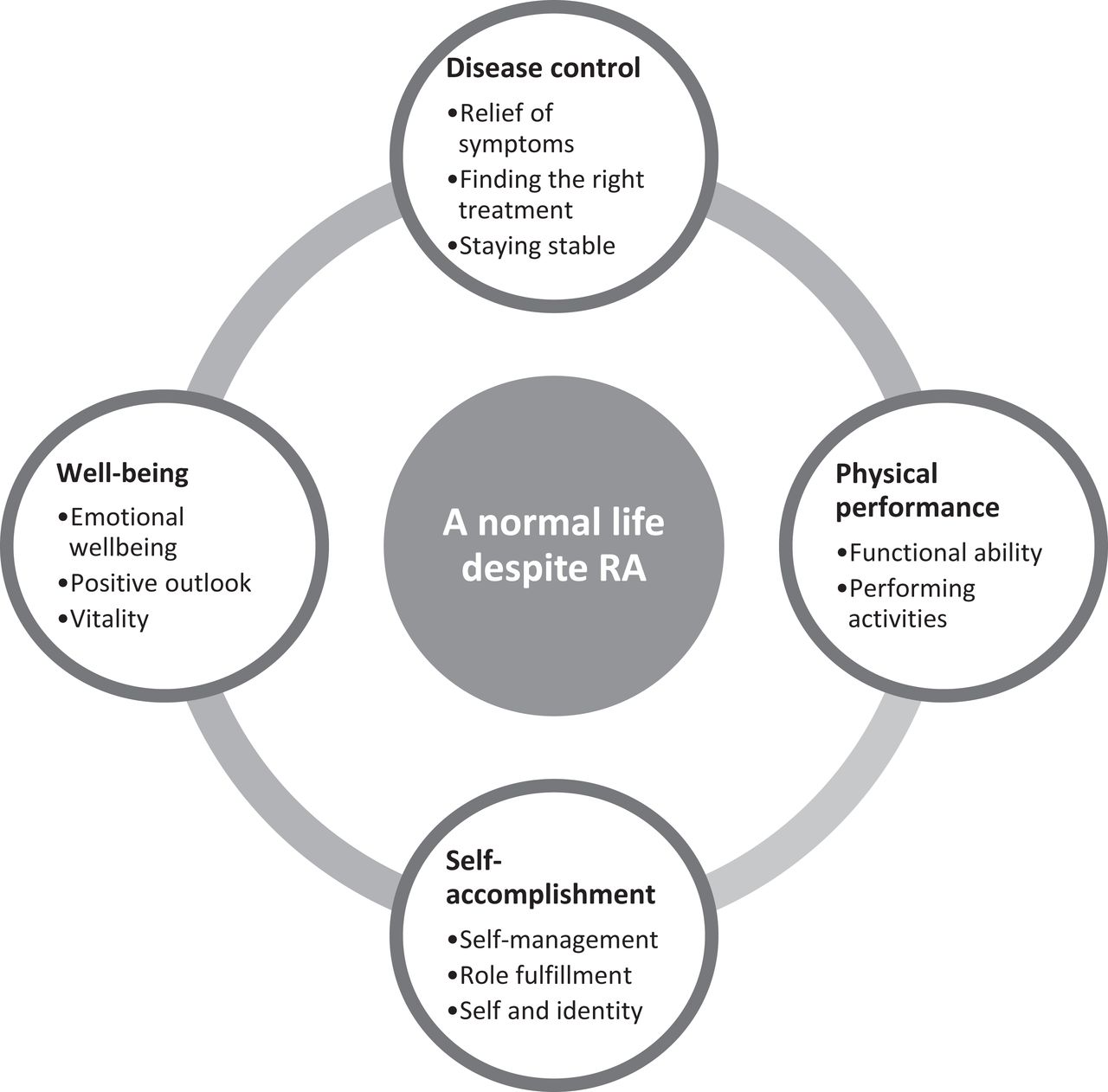
The meta-synthesis resulted in an overarching patient-preferred outcome across countries: ‘a normal life despite RA’. This overarching outcome related to disease control, physical performance, self-accomplishment and well-being, which together describe outcome preferences of patients with early RA (figure 2). Changes in patient-preferred outcomes throughout the early disease stage and differences between countries were described where appropriate.
{kind=link}
{kind=link}
A multinational perspective on patient-preferred treatment outcomes in early rheumatoid arthritis (RA), including an overarching theme, 4 main themes and 11 subthemes.
Normal life despite RA
Patients preferred to live a normal life and maintain everything as it had been before at t1. Patients described this as regaining the health and life they had prior to RA onset as quickly as possible and in its narrowest sense.
‘The treatment is necessary so you can return back to your healthy state before RA was diagnosed. So you can move on in life. So you can say: “I have had these issues, but now I need to have the same quality [of life] again. I am a very healthy person and I can do everything again.” So that is most important to me. To move on in life again.’ (Belgian woman in her 40s, t1)
‘I want to be more like that young girl again […]. Who always saw the funny side of things. Who studied, shared accommodation, and went out with friends.’ (Dutch woman in her 20s, t1)
Patients still preferred a life as normal as possible, comparable to their pre-RA life, at t2. However, they experienced to a greater extent that it was possible for them to live a normal life despite RA.
‘I get my education done, I get the job, I get back.. Or my kids get their mom back. As it was from the beginning. I become more myself.’ (Swedish woman in her 40s, t2)
Swedish patients expressed more threats to their normal life caused by RA at t2 than their Belgian and Dutch counterparts.
Disease control
Relief of symptoms
Patients wanted relief of symptoms (eg, inflammation, pain, swelling, stiffness, fatigue and loss of (muscle) strength) as quickly as possible.
‘But that is what I expect, that I am going to be free from symptoms and with that, everything else, both fatigue and worry and everything, I will come back.’ (Swedish man in his 50s, t1)
Some patients expressed a desire to have no symptoms at all, while others were satisfied with having fewer or less intense symptoms. Pain relief was a major outcome preference for patients across countries because pain limited their functional ability and impeded them from living a normal life. Pain demanded all their attention at t1, diverting their awareness of other symptoms.
‘Getting rid of the damn pain as soon as possible was actually the most important.’ (Belgian woman in her 60s, t1)
Relief of fatigue became an increasingly important outcome for Dutch and Swedish patients at t2, in contrast to the Belgian patients for whom this outcome lost importance over time. Swedish patients experienced fatigue as being more difficult to cope with than pain over time, while Belgian patients felt the opposite. They still feared the intolerable, flaring pain after RA onset.
‘I could survive it if I was not so damn tired. I would rather have pain than be tired. Because I usually say that pain you can ignore, but fatigue, what do you do about it?’ (Swedish man in his 50s, t2)
‘If I feel the way I feel now, yes, I am fine with it, but without pain then.. Yes, I accept the tiredness, then I can go to sleep.’ (Belgian man in his 50s, t2)
‘Indeed, you can manage that, for example by going to bed earlier.’ (Belgian woman in her 50s, t2)
Improved sleep was spoken of by Belgian and Swedish patients at both time points as an outcome preference, which was related to relief of symptoms.
Finding the right treatment
Patients preferred to find the right treatment and restore their health at the earliest opportunity. Dutch patients expressed a desire for receiving medication with a faster onset of action at t1 because they found it difficult to cope with the long wait for a noticeable treatment effect. It was important for patients across countries that medication quickly relieved their symptoms, especially pain. Patients who experienced quick pain relief expressed positive expectations related to disease control. It was important for Belgian patients to have visual proof of disease control (eg, blood test results) to gain additional reassurance. Furthermore, patients from all three countries preferred not to have side effects. This became an increasingly important outcome for Swedish patients at t2 because they experienced side effects as a threat to their ability to live a normal life.
‘Yes, it is a balancing act, so to speak, either pain or medication, so to speak, to find that level. Be pain free and take as little medication as possible.’ (Swedish man in his 40s, t2)
Belgian and Dutch patients on the other hand increasingly tolerated side effects over time, as long as they did not hamper their normal life and the medication effectively controlled their disease. Dutch and Swedish patients were more focused on avoiding long-term adverse effects at t2 compared to Belgian patients. Patients across countries preferred to use the least possible medication, resulting in an outcome preference of dose reduction or tapering with preserved beneficial treatment effect. Swedish patients also focused on effective non-pharmacological treatment, while Belgian and Dutch patients mainly focused on effective pharmacological treatment.
Staying stable
Staying stable, without experiencing disease flares, was preferred by patients across countries at both time points. Some patients expressed a desire to prevent or reduce the risk of joint damage by controlling disease progression.
‘Make sure that my RA does not get worse. I think that is quite important as well. I do not want to… I am now still young with RA. I do not want, for example, to have those deformed hands when I am 30 or 40 years old.’ (Dutch woman in her 20s, t1)
Patients mainly focused on the risk of joint damage at t1 because of better disease control at t2. Preventing or reducing the risk of joint damage was not specifically mentioned by Swedish patients. Belgian patients, in particular, had already experienced disease control at t1 and they hoped to stay stable. Patients across countries feared experiencing flares at t2 and those who had a relapse hoped to regain stability.
Physical performance
Functional ability
Patients preferred to regain their functional ability, especially at t1. Limited mobility affected, for example, their ability to walk, climb stairs and drive a vehicle. Mobility was an important precondition for patients to maintain their independence.
‘Do not take away my mobility because that would leave me with nothing at all!’ (Dutch woman in her 60s, t1)
Patients’ impaired functional ability was often a blow to their self-esteem. Regaining these functions was, therefore, a major outcome preference at both time points. Nevertheless, patients less often mentioned this at t2 because they experienced less functional limitations by then. Their fear of permanent loss of function and subsequent disability diminished accordingly.
‘I do my work independently. Washing, ironing… I do it all back again myself.’ (Belgian woman in her 60s, t1)
Performing activities
It was important for patients across countries to perform activities of daily living (eg, dressing, cooking and going for a walk with the dog), work, hobbies and social activities independently and in the same manner as they had always done. Performing these activities had generally been self-evident prior to RA onset.
‘Walking, climbing stairs, opening a bottle, tying your shoelaces… These are things every normal person is able to do, no?’ (Belgian man in his 50s, t2)
Patients had adjusted to their disease at t2, although they still preferred not to make (m)any changes to their life (eg, pacing activities, using assistive devices and asking for help), only if they had to. Especially Swedish patients were more focused on adopting a healthy lifestyle (eg, exercise, diet and smoking cessation) to regain their former activity levels.
‘To get cured is the greatest wish. But that was the first thing I was told, that you do not. And then you have to try to process and, as I said, the best thing is that I have started working out. That is what is the most positive part.’ (Swedish man in his 50s, t2)
Self-accomplishment
Self-management
Patients wanted to become capable of self-managing the consequences of RA. They wanted to know what they could do themselves to continue living a normal life.
‘And the knowledge and concern go hand in hand. With knowledge, the worry decreases.’ (Swedish man in his 50s, t1)
Self-management became an increasingly important outcome at t2 because patients were clinically more stable and felt more confident to take control by then. For example, they wanted to know how to prevent flares by avoiding triggers. Topics such as exercising, adjusting the work environment and pacing activities also became more important over time. Swedish patients more frequently discussed self-management than their Belgian and Dutch counterparts. Patients across countries expressed a desire to play an active role in making treatment decisions at t2.
Role fulfilment
The ability to fulfil important life roles was a major outcome preference at both time points because this was core to patients’ self-accomplishment. They preferred to engage fully at home and at work, in hobbies and leisure activities, and maintain their relationships with family and friends.
‘If only I can keep going for my walks. That is very important to me. Yes, fine, we all need to work. That is important too. Simple enough. That is number one and then hobbies.’ (Dutch man in his 50s, t1)
Some patients feared to be excluded by others because they were not able to engage fully. The same roles were identified in each country. Dutch and Swedish patients’ workability was discussed as being more important than resuming hobbies and leisure activities in living a normal life, while Belgian patients who still experienced an unstable disease tended to focus less on workability at t2. Maintaining a stable standard of living was an outcome preference especially of interest to Swedish patients.
Self and identity
It was important for patients to be their independent selves at both time points. They preferred to re-establish their predisease identity, which was more of a struggle at t1 than t2. To live a normal life despite RA, patients did not want to identify themselves as a patient, nor wanted to be treated as a patient by the people around them because this affected their sense of self.
‘And now at the general practitioner as well. You find yourself in a risk category because you are now a chronic patient. You get a influenza shot every year. Things like that. You are in a category that you were not in previously and… Yes, well… In itself, that is not so bad, but… It makes me think: I am getting old. […] it really is quite confronting.’ (Dutch woman in her 50s, t2)
Some patients were afraid of being a burden to others, which made them vulnerable to social isolation. It was, therefore, important for them to maintain their independence. Swedish patients, in particular, preferred to maintain their appearance unaffected by RA to re-establish a normalised sense of self.
‘You do not recognise yourself, it is like you have lost part of yourself.’ (Swedish woman in her 40s, t2)
Some Dutch patients experienced ignorance and misunderstanding as a consequence of the invisible nature of RA at t2. They preferred greater recognition and support from other people.
Well-being
Emotional well-being
Patients highlighted the emotional burden of being diagnosed with RA. They preferred to ease negative emotions (eg, anxiety, frustrations and grief) and feel well again.
‘I was desperate because I could not do my household chores no more. I could not do absolutely anything. They had to dress me and that is not easy. I am a person who likes to be busy, who cannot sit still, so, uhm, it is difficult.’ (Belgian woman in her 60s, t1)
For Belgian and Dutch patients, emotional well-being was of greater importance at t1 because they experienced fewer negative emotions at t2. However, worries about the unpredictability of their future were still present. On the other hand, Swedish patients expressed more negative emotions at t2 because they still struggled to deal with the challenges of RA (eg, fatigue and side effects). Patients who experienced a relapse or multiple treatment failures expressed additional emotional distress. Some Dutch patients feared in particular that they would eventually run out of treatment options.
‘And something else that worries me a bit, since I have already tried all of them [medication]… That eventually I will have reached the end of treatment options. […] Will there be anything else left? Or do I start all over again?’ (Dutch woman in her 50s, t2)
Positive outlook
Patients preferred to have a positive outlook despite RA, which was described as facing the future with confidence and having positive perspectives.
‘The first time I heard that I really had RA, I thought: What will happen to me in years to come? What does this mean for my future? Will all of my plans fall apart now or can I just slowly keep doing whatever I have been doing so far?’ (Dutch woman in her 20s, t1)
In order to experience well-being, patients preferred to still be able to make long-term plans and commitments to keep on experiencing or re-experience joy in everyday life. Patients had more positive expectations for the future at t2 because they were less worried and had more disease experience by then. Belgian and Swedish patients also expressed the outcome preference of living a long life, comparable to their peers.
Vitality
Patients preferred vitality, which was described as feeling full of life and energy again. RA drained patients’ energy levels.
‘I want to feel energetic. Energetic and happy.’ (Swedish woman in her 40s, t2)
They expressed a desire to regain their physical and mental drive again to ensure their well-being to live a normal life. Belgian patients especially highlighted this at t1, while Swedish patients' focus on vitality increased over time. Vitality was not mentioned as such by Dutch patients.
DISCUSSION
Our results provide a multinational perspective on patient-preferred treatment outcomes in early RA. We found that, regardless of country of residence, patients essentially wanted to live a normal life despite RA. Many similar patient-preferred outcomes were revealed in Belgium, the Netherlands and Sweden. However, some outcome preferences developed differently over time across countries.
We found that it was of major importance to patients to live their life as normal as possible, which concurs with findings of previous studies in RA.6 8 9 31 However, patients’ definitions of normality changed as their disease experience increased. This result conforms with the concept of ‘shifting normalities’, described by Sanderson and colleagues.32 The added value of our study is the context in which normality was described, namely, over time in the early stages after diagnosis of RA and treatment initiation. We found that patients’ normal life was disrupted after RA onset and patients preferred to return to their predisease life without making (m)any changes. They redefined their notion of what constitutes a normal life over time because they became more familiar with their disease and its consequences. Knowledge about patients’ definitions of normality in the early stage of RA is scarce, yet, crucial for clinicians when supporting patients in disease adjustment and self-management.33
Relief of symptoms, especially pain, was of primary concern to patients across countries after RA onset. Symptom management is thus an important part of care from the perspective of patients with early RA. This does not differ from findings of studies in patients with established RA,7 but patients with early RA specifically highlighted the importance of medication with a fast onset effect and the difficulty of symptom management in case of a delayed treatment response. Furthermore, fatigue was not a main focus of patients with early RA, although relief of fatigue became an increasingly important outcome for Dutch and Swedish patients over time. This finding seems in contrast to studies where patients beyond the early stage of RA consistently emphasised the everyday impact of fatigue on their life.34 Altogether, our results imply that patients’ outcome preferences may change over time, depending on their perceived response to treatment and the stage of RA. This implication should, however, be confirmed or refuted by studies using quantitative research methods.
Another result that adds to the existing body of knowledge about patient-preferred outcomes is that patients with early RA do not want to feel like a patient. Accepting an identity that suddenly includes having a chronic disease was a major issue for patients across countries. Toye and colleagues also described a disrupted self and identity in their meta-ethnography. They pointed out how RA changed who a person was and what he/she had planned to be in the future.35 Patients with early RA preferred to continue being the person they were prior to RA onset, but this was a struggle for them, especially at t1.
We found a few country-specific outcome preferences, indicating that a country’s healthcare system and culture may also influence patient-preferred outcomes in early RA. Most notably, only Swedish patients considered effective non-pharmacological treatment (eg, patient education, physiotherapy, occupational therapy and social work) an important outcome. Swedish patients were probably more familiar with these treatment types since they had consultations with a physiotherapist, an occupational therapist and a social worker 6 weeks after treatment initiation as part of usual care. Another outcome frequently discussed by Swedish patients was self-management, while patients in Belgium and the Netherlands were mostly focused on effective pharmacological treatment. Swedish patients also tended to express a greater negative impact of RA on their emotional well-being than Belgian and Dutch patients. The question arises whether expressing emotions is more common in Sweden. We found that it was only Belgian patients who spoke of proof of disease control as an outcome preference. A possible explanation is that financial incentives are tied to the systematic measurement of clinical outcomes (eg, the Disease Activity Score in 28 joints) in Belgium and it may be that patients noticed clinicians’ focus on these outcome measures, thus making it of greater concern to them. Finally, it should be noted that relief of fatigue became an increasingly important outcome for Dutch and Swedish patients over time, but it did not for Belgian patients. We could not find a plausible explanation for this. Further (quantitative) research is needed to explain country specificities.
We revealed a wide range of patient-preferred outcomes in early RA, which were related to disease control, physical performance, self-accomplishment and well-being. Our findings contribute to a current need in RA treatment, namely, understanding what really matters to patients.36 Integrating the patient perspective in clinical practice is essential for achieving optimal outcomes, since outcomes preferred by patients do not always comply with those measured by clinicians.5 Moreover, outcomes are important indicators for decision-making in RA treatment. By considering patient-preferred outcomes when making treatment decisions, clinicians can strengthen their clinical observations and dialogues with patients. This will enhance person-centred care and facilitate shared decision-making,26 37 which is preferred by the majority of patients.38 After all, clinicians are medical experts in RA, but patients have the lived experience.39
Several strategies were applied to ensure this study’s trustworthiness, such as uniformity in data collection and data analysis training for the local research teams.18 Furthermore, decisions were all made in teams and well documented to prevent researcher bias due to solo interpretations or personal opinions. To support the quality of the independently employed national studies, the local research team used a reporting tool that was based on the consolidated criteria for reporting qualitative research40 41 and the quality criteria suggested by Mays and colleagues.42 Moreover, the local research teams consisted of experienced qualitative researchers as well as patient research partners. Hence, this study on the patient perspective was strengthened at several research phases by the involvement of patient research partners, which is a recommended strategy.43 Two Belgian patient research partners provided feedback on the research question and codeveloped the study design and the data collection method. In each country, patient research partners verified the clarity and understandability of the interview questions and helped with data interpretation and the discussion of the local results. They also approved the patient information and informed consent forms. The robustness of patient-preferred outcomes across countries indicates that our results are relevant to the broader population of patients with early RA in countries with a similar healthcare system and culture. However, we acknowledge that a more diverse group of countries, representing, for example, Southern, Eastern and North European countries, could have supported conclusions about the cultural differences and the transferability of the findings. The selection of the countries was primarily based on achieving a first exploration of patient-preferred outcomes in early RA. A motivated local team with experience in qualitative research and having resources available were selection criteria in view of the feasibility of this longitudinal qualitative study in different countries and different languages. Also, other methodological considerations of this study should be mentioned. Some focus groups were smaller than intended, which could limit rich discussions. It could, however, also make patients feel more at ease to speak out loud and be equally involved in the discussions. Finally, it was a challenge to interview patients at two time points, perhaps because of the early disease stage. Despite efforts made in the study design (ie, adding the possibility of individual interviews at t2 in the Netherlands and Sweden), patients still dropped out at t2.
In conclusion, patients in Belgium, the Netherlands and Sweden have many similarities in terms of which outcomes they prefer throughout the early RA stage. ‘A normal life despite RA’ was an overarching patient-preferred outcome across countries, including outcomes related to disease control, physical performance, self-accomplishment and well-being. This multinational perspective on patient-preferred treatment outcomes in early RA is valuable for clinicians of different disciplines (eg, rheumatologists, rheumatology nurses, physiotherapists and occupational therapists) to implement person-centred care directly from treatment initiation.
Key messages
What is already known about this subject?
Patients with rheumatoid arthritis (RA) may have other or additional priorities and treatment expectations than clinicians.
Patient-preferred outcomes in early RA cannot just be adopted from those in established RA.
What does this study add?
Belgian, Dutch and Swedish patients with early RA have many similar outcome preferences (eg, relief of pain and independence), although country specificities exist.
Patients’ views on outcomes change over time, depending on their response to treatment and the stage of RA.
How might this impact on clinical practice?
Understanding patient-preferred outcomes in early RA is essential to enhance person-centred care and facilitate shared decision-making directly from treatment initiation.
Acknowledgments
We would like to thank the patients who participated in this study for sharing their valuable perspectives and Diederik De Cock and Patrick Verschueren for their contribution to the consensus meeting. Patient research partner Els Binnard contributed to the conception and the study design and Sabrina Meyfroidt (SM) contributed to the data collection of the original Belgian study.
REFERENCES
Footnotes
KVdE and EGEM share the first authorship.
Contributors All authors were involved in drafting the article or revising it critically for important intellectual content and all authors approved the final version to be submitted for publication. Study conception and design: KVdE, EGEM, AB, ADG, YvE-H, JEV, RW and IL. Acquisition of data: KVdE, SM, EGEM, JEV, EL and IL. Analysis and interpretation of data: KVdE, EGEM, EL, AB, ADG, EL, MN, AP, FVdH, YvE-H, GV, JEV, RW and IL.
Funding This work was supported by an unrestricted educational grant of Bristol-Myers Squibb (Belgium), a travel grant from Fonds voor Wetenschappelijk Reuma Onderzoek (Fund for Scientific Research in Rheumatology) (Belgium), the Southern Healthcare Region (Sweden) and the Swedish Rheumatism Association (Sweden).
Competing interests None declared.
Patient consent for publication All patients who participated in this study provided written informed consent.
Ethics approval Ethical approval was sought from the local ethical review boards in each country.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement The data supporting the results reported in the manuscript will not be shared as ethical approval for the study requires that the transcribed interviews are kept in locked files, accessible only to the researchers.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.