Article Text

Statistics from Altmetric.com
Within the health technology assessment framework,1 an economic evaluation compares health technologies in terms of their costs, clinical effectiveness, side effects, impact on health-related quality of life and impact on organisations. It involves the choice of the ‘best alternative’ to which a (new) technology is compared, the comparison of the benefits and consequences between strategies balanced against the difference in costs and the choice of the economic perspective. This article presents an introduction to steps to implementing a health economic evaluation, based on the health economics literature2 and guiding principles such as the Consolidated Health Economic Evaluation Reporting Standards statement, which has been proposed3 to standardise the conduct and reporting of health economic evaluations, with examples specific to rheumatic diseases.
An economic comparative assessment requires an explicit statement of the broader context for the study, and a description of the disease in question. This includes justification for choices to be made, the values important to guide the judgement of decision makers and its relevance for health policy or clinical practice decisions.
Trial-based economic evaluation
Cost–effectiveness analyses compare new technologies, such as a drug treatment or an orthopaedic surgery, with standard care, by calculating associated health effects and costs, at best using data from a randomised clinical trial. The incremental cost–effectiveness ratio (ICER) is routinely used to express the cost–effectiveness of one treatment over another in the form of a ratio, as costs per health effect gained.
ICER =
Cost of new treatment– Cost of standard care
Effectiveness of new treatment– Effectiveness of standard care
––––––––––––––––––––––––––––––––––––––––––––
As such, the ICER provides the cost of an additional unit of health (eg, days with pain relief, reduced level of disability, fracture avoided) gained when substituting the old with the new technology.
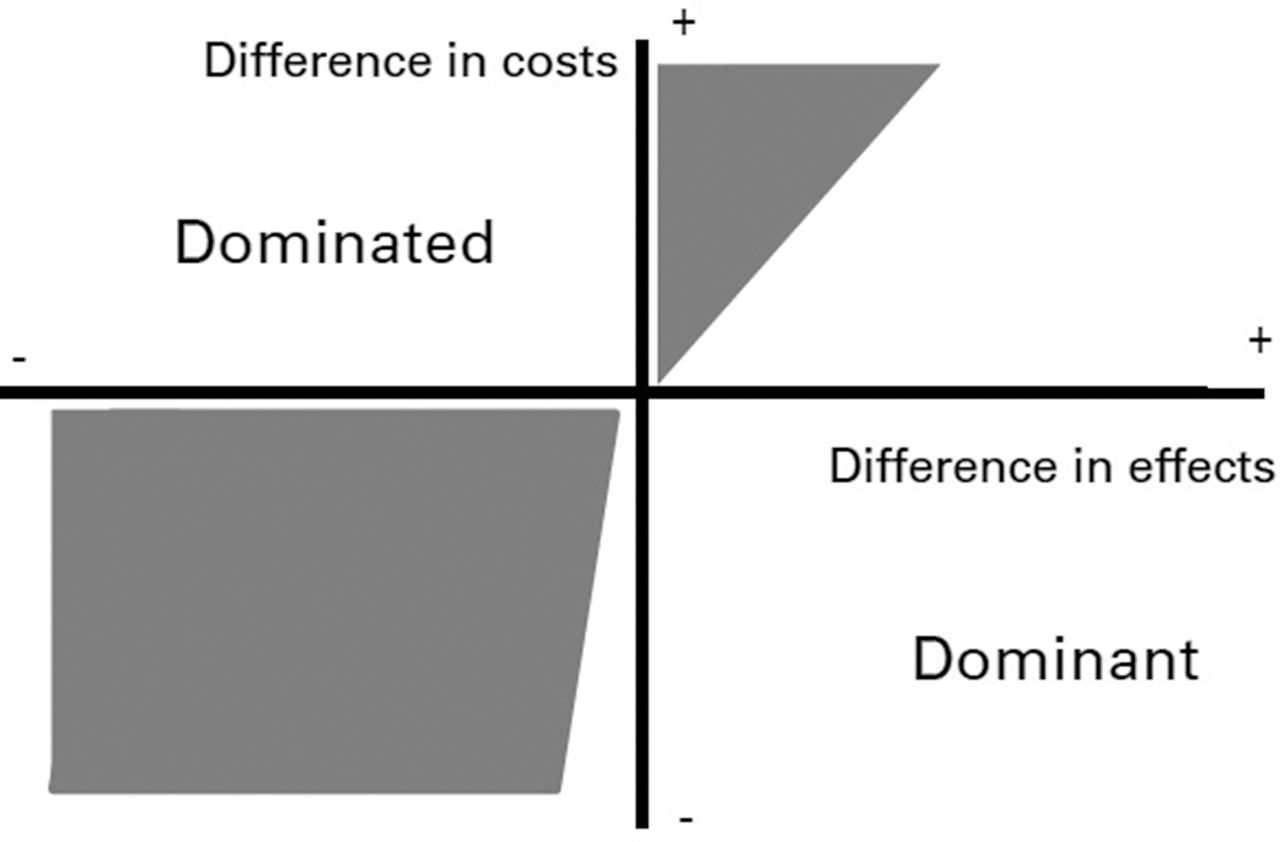
The ICER is best explained on the cost–effectiveness plane (figure 1) where four possible outcomes can be observed.
{kind=link}
Cost–effectiveness plane.
If the new strategy has higher costs and provides lower effect (upper left quadrant), it is rejected. It is said to be dominated.
If the new strategy has better effect at lower cost (lower right quadrant), it is accepted and considered to be dominant.
Decision-making is less straightforward when considering the secondary diagonal on the plane.
Where the costs are lower but the health effects are lower as well (lower left quadrant), we can ask how large the money-saving would have to be to accept the loss in effectiveness (a threshold efficiency frontier), for example, when taping biologic disease-modifying antirheumatic drugs (bDMARDs) in rheumatoid arthritis (RA) or spondyloarthritis.
At the opposite (upper right quadrant), when a new treatment provides better health at higher cost, the question is how much money could be spent to access the gain in health (a threshold efficiency frontier), for example, when introducing bDMARDs in established RA.
These lines within each of those two quadrants determine where the deal will be acceptable in white, or unacceptable in grey.
Model-based economic evaluation
This type of analysis requires a lot of information, including on health outcomes, their valuation, health events, and resource use and costs. In some situations, not all relevant information can be gathered in clinical trials, for example, when comparing the long-term morbidity or mortality outcome of a new drug to current standard treatment in osteoarthritis. Not only would such a trial be very costly it would also delay market access. Developing a simulation model that involves extrapolation of observed short-term data over time can help address this gap in the data. Types of decision analytic models include state transition models and discrete event simulations—the latter are more complex as they allow for modelling individual patients rather than a cohort (and these are often used in modelling of RA).4 Recently, a discretely integrated condition event simulation proved to be a more flexible alternative to track the course of RA according to treatment, including switches to further lines in a selected sequence, while taking into account patient heterogeneity with multiple events over time.5 Such models can be implemented in Microsoft Excel, typically in combination with Visual Basic for Applications, or other software packages such as R. A useful guide to how to implement a model in Excel can be found in Briggs et al. 6 To ensure transparency of such a model-based economic evaluation, a clear description of the reasons for choice of decision analytic model used and a presentation of the model structure and assumptions are recommended.3
The use of registry data could be a valuable source since several biological registries have been developed that include health outcomes such as disease activity or physical functioning. The link with claims database (providing data on health resource utilisation and sick leave), where possible, would contribute very comprehensive information on healthcare consumption.
Economic perspective
Keeping in mind an economic evaluation is mainly used to inform decisions at a national level, it is rarely ‘universal’ as it will be performed within a specific setting, location, country, and thus account for aspects relevant to the system in which the decision needs to be made.7 An economic evaluation is conducted from a specific perspective. This perspective determines the type of costs and benefits that are included in the analysis. Treatments may be reimbursed by health insurance or funded by a national health system. Therefore, the national health insurance/system perspective is interested in costs in terms of tariffs reimbursed to patients, to health professionals and to hospitals or other institutions taking care of the patients and health benefits for the patients in question. The hospital perspective considers what hospitals have to pay for delivering a health service, that is, mainly personnel and equipment. From the patient perspective,8 economic considerations include what the patient has to pay after all costs covered by insurances have been reimbursed, namely the out-of-pocket costs. Finally, the most comprehensive societal perspective is invoked where all expenditures generated by healthcare technology are taken into account for various payers. This also accounts for productivity losses when people are forced to leave work because of their arthritis condition. Another example is genetic diagnostic processes that involve many stakeholders from private and public sectors whose costs may not be reimbursed by public or private health insurance.
Comparators
When assessing a new health technology, the relevant comparators need to be identified. Therefore, it is necessary to describe the interventions or the strategies being compared and to state why they are chosen. For instance, for patients with RA, what represents standard care when the intervention is a new biological therapy? There are several valid choices of comparators: other biological treatments that are already recommended, a standard treatment, such as methotrexate, or a ‘do–nothing’ option (best supportive care) that all other interventions can be compared against. Including all of them provides a clearer picture of the RA treatment landscape and enables cross-validation between past and future evaluations.
Choice of health outcomes
A clear description of the health outcome considered and a justification of their relevance will help putting the interpretation of the economic assessment in context. The valuation of health benefits depends on the nature of the economic comparison.1 2 In addition to a generic health outcome, such as the quality-adjusted life-year, it may be informative to include a condition-specific health outcome in the analysis, by which different technologies can be compared.
The different types of economic evaluation can be distinguished by the outcomes considered in each: whether the alternatives provide the same health benefit (cost minimisation analysis), or differ by health events or health states observed by health professionals (eg, achieving sustained remission, avoiding an osteoporotic fracture, avoiding a side effect) or reported by patients (eg, number of days with pain, of decrease points on a 0–10 scale of fatigue) (cost–effectiveness analysis), combines the effect of two outcomes about health and time (cost–utility analysis) or when health benefit may be quantified in monetary terms (cost–benefit analysis).
Cost estimates
The cost assessment, whatever the perspective taken, uses opportunity cost, which describes the value of the achievable benefits forgone by funding one technology, which comes at the expense of another.2 Its assessment consists of several steps including identification of resources, measuring quantity of resources used and doing the exercise of valuing and costing these.9 It may differ between the strategies compared.
Time horizon
An appropriate time horizon takes into account the time and duration of use of the new health technology and the duration for which costs and benefits will continue to arise (such as effects beyond discontinuation or survival gains), for example, a lifelong time horizon of a new DMARD in RA aims to capture short- and longer-term effect on health and costs, including potential long-term side-effect or benefits.
Discount rate
Muennig explains that ‘medical interventions […] often result in decreased future medical costs that must be accounted for in present-day terms. Humans have a tendency to place a lower value on future events than on events that occur in the present. This phenomenon is called discounting’10 and this can be applied to costs and outcomes alike, although different jurisdictions have different guidance on what discount rate to use and whether the same is to be used for costs and health effects.
Limitations to running economic analysis
Health economic evaluation relies on comparisons of alternatives in terms of costs and health outcomes. However, in some situations, economic evaluations can have serious limitations and even provide little contribution, for instance (1) when a treatment is demonstrated very effective with a small sample size, because small sample will not allow an analysis of cost and effectiveness related variables with sufficient reliability; (2) when treatment effect is documented with too short follow-up which precludes any long-term assessment of both effect and cost; and (3) when clinical trials use outcomes that are inadequate for economic analysis, for example, in a trial evaluating a new treatment of osteoporosis with bone density increase as an outcome, where bone density change incurs no cost per se and cannot easily be related with a meaningful outcome for patients; here, the probability of fracture would be better suited. However, such issues can be addressed in appropriate uncertainty analysis.
In conclusion, a health economic analysis represents a strict methodological approach that helps decision makers to make the best choices among various new technologies to gain the maximum of health with the same amount of (available) money.
Footnotes
Acknowledgements This manuscript was written in support of the preparation of the EULAR health economics in rheumatology course.
Contributors FG prepared the first draft of this manuscript with input from MdW, BF, SG, MJ and AB. All authors approved the revised version.
Competing interests None declared.
Patient consent for publication Not required.
Provenance and peer review Not commissioned; externally peer reviewed.