Article Text

Abstract
Objective Rheumatoid arthritis (RA) often affects women in their fertile age, and is known to compromise female fertility. Serum anti-Müllerian hormone (AMH) levels are a proxy for the total number of primordial follicles, and a reliable predictor of the age at menopause. Our objective was to study the longitudinal intra-individual decline of serum AMH levels in female RA patients.
Methods Female RA patients from a nationwide prospective cohort (2002–2008) were re-assessed in 2015–2016. Serum AMH levels were measured using the picoAMH assay and compared with healthy controls. A linear mixed model (LMM) was built to assess the effect of RA-related clinical factors on the decline of AMH levels.
Results A group of 128 women were re-assessed at an age of 42.6±4.4 years, with a median disease duration of 15.8 (IQR 12.7–21.5) years. The time between first and last AMH assessments was 10.7±1.8 (range 6.4–13.7) years. Participants represented a more fertile selection of the original cohort. At follow-up, 39% of patients had AMH levels below the 10th percentile of controls (95% CI 31% to 48%), compared with 16% (95% CI 9.3% to 22%) at baseline. The LMM showed a significant decline of AMH with increasing age, but no significant effect of RA-related factors on AMH.
Conclusion AMH levels in RA patients showed a more pronounced decline over time than expected, supporting the idea that in chronic inflammatory conditions, reproductive function is compromised, resulting in a faster decline of ovarian function over time and probably an earlier age at menopause.
- Arthritis
- Rheumatoid
- Epidemiology
- Outcome Assessment
- Health Care
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
INTRODUCTION
Rheumatoid arthritis (RA) is a chronic inflammatory auto-immune disease that often affects women in their fertile age. RA not only affects the joints, but can also cause extra-articular damage, affecting different organ systems.1 2 A prolonged time to pregnancy3 4 and a younger age at which menopause sets in5 6 are both indicators that in women with RA the ovarian function may be compromised as well.
Key messages
Serum anti-Müllerian hormone (AMH) levels are a proxy for the remaining number of ovarian primordial follicles, and as such reflect ovarian function.
Serum AMH levels in this longitudinal cohort of female RA patients revealed that levels decreased more rapidly in patients compared with controls.
The more rapid decline of serum AMH levels in women with established RA indicates that chronic inflammation compromises ovarian function, and may result in an earlier age at menopause.
No significant effect of separate RA-related factors on decline of AMH levels could be identified.
Optimal treatment of chronic inflammatory disease in an early phase may improve long-term women’s health.
The ovarian function depends on both the quantity and the quality of the primordial follicles in the ovaries. At birth, there are approximately 1 000 000 primordial follicles present in the ovaries. This number gradually decreases over time, resulting in about 300 000 remaining follicles at menarche.7 8 During her twenties and thirties, a woman’s follicle pool further decreases, with a slight acceleration in her late thirties and early forties. Finally, the near depletion of the ovarian follicle pool is marked by the cessation of menstruation.9 The last menstrual period in a woman’s life span, that is, the menopause, occurs at a mean age of 51 years. Infertility generally sets in approximately 10 years before a woman experiences menopause.9 This results not only from the decline in number of developing ovarian follicles over time, but also from a decrease in quality of the oocytes maturing within these follicles due to accumulated damage from birth onwards.10
The age at which a woman reaches menopause, as well as the preceding period of decreased fertility and infertility, varies greatly between women.9 At present, the serum level of anti-Müllerian hormone (AMH) is the most reliable predictor for the age at which a woman will enter menopause.11 Although prediction of the actual age at menopause based on a single AMH measurement is still not very precise.11 AMH is a member of the transforming growth factor β family and is produced in the ovary by granulosa cells of early developing follicles.12 In both healthy and subfertile women, there is a strong correlation between serum AMH levels and the number of developing follicles in the ovaries. It has been shown that serum AMH levels become undetectable approximately 5 years before a woman reaches menopause.13
Genes associated with the age of menopause, and more specifically the length of the reproductive life span of a woman, are generally involved in DNA repair and maintenance as well as in the immune system.14 In this way, genes involved in healthy ageing are also predictors for ovarian function. Indeed, a compromised ovarian function has been described in patients with type II diabetes mellitus15 and in young girls with cancer.16 This suggests that an unhealthy soma results in an early decline of ovarian function. It is unknown whether the same holds true for chronic inflammation.14
In women with RA, AMH levels at time of diagnosis have been found to be comparable to those in healthy controls.17 Furthermore, after 6 months of methotrexate (MTX) therapy in RA patients, AMH levels did not differ from those in patients who did not use MTX.17 When analysing women with established RA, AMH levels were indeed lower compared with healthy controls.18 19 However, thus far there have been no longitudinal studies on AMH levels in RA patients. Nor has the effect of disease characteristics on the decline of AMH levels over time been studied.
The objective of the current study was to investigate the intra-individual change in AMH levels over a longer time period in women with RA. We compared serum AMH levels in RA patients with those in controls from the general population, and studied the decline of serum AMH levels in RA patients over time in relation to RA-related clinical factors.
METHODS
Patients
For this observational cohort study, patients were recruited who had participated in the Pregnancy-induced amelioration of RA (PARA) study. The PARA study is a nationwide prospective cohort study, which was performed in the Netherlands in 2002–2010.20 Patients were invited to participate by their attending rheumatologist if they had a diagnosis of RA according to the 1987 ACR criteria,21 and if they were actively trying to conceive or were already pregnant. Patients had to have a good understanding of the Dutch language.20 Patients could participate in the PARA study more than once. For the current follow-up study, patients were contacted when they had given consent to be contacted for future research, and when they had at least one non-pregnant serum sample available (ie, from a preconception visit, or from a visit 6 months postpartum).
The majority of the PARA subjects had been contacted in 2013–2014 for a questionnaire on fertility.22 As a result, addresses were up to date whenever possible. Patients currently living outside of the Netherlands or Belgium were excluded.
Ethical approval
The original PARA study, as well as the current follow-up study, were performed according to the Declaration of Helsinki, and were approved by the Medical Ethics Review Committee of the Erasmus MC.
Data collection
During the original PARA study,20 patients were visited at their homes before, during, and after pregnancy, with the final visit 6 months postpartum. Each assessment consisted of a questionnaire driven interview on disease characteristics and use of medication, measurement of disease activity, and drawing of serum samples.
For the current study, patients received an information letter, and thereafter were contacted by telephone. Patients who gave informed consent, were visited at their home address for blood sampling, and they completed an online questionnaire including questions on menstrual cycle, age at menarche, hormone use, and other possible iatrogenic causes for amenorrhoea, including abdominal surgery and chemotherapy.
Measurements
Disease activity was measured during the PARA study visits using the Disease Activity Score assessing 28 joints (DAS28) for tenderness and swollenness, combined with serum C reactive protein levels.23
Serum samples were stored at −80°C. Serum AMH levels were measured in the samples from all preconception and 6 month postpartum PARA study assessments, as well as in the newly acquired samples from the follow-up visit.
AMH values were measured using the picoAMH assay, provided by Ansh labs (Houston, Texas, USA).24 25 Interassay and intra-assay coefficients of variation were both <5%.
Controls
Serum AMH levels in patients were compared with a group of healthy controls. This international reference cohort existed of 554 healthy adult women, aged 18–47 years, who had a regular menstrual cycle and/or were proven fertile.26 AMH levels in controls were originally reported as measured by the Beckman Coulter Gen II Assay. Therefore, a conversion factor was used to compare AMH levels in the patient group to those in the controls25:

Statistical analysis
Values are presented as mean±SD for normally distributed variables, as median IQR if values were non-normally distributed, and as number (%) for dichotomous variables. The number of missing values are given for each variable.
To approach a normal distribution, AMH levels were log-transformed for analysis. To correct for different distributions of ages between patients and controls at the different time points, AMH levels were compared with controls using analysis of covariance on log-transformed AMH levels with adjustment for age.
Sensitivity analyses were performed by excluding women using combined oral contraceptives, and by excluding women using any steroid sex hormones.
To reduce potential bias in the longitudinal analysis due to missing values, multiple imputation was performed. To incorporate the longitudinal outcome into the imputation procedure, a preliminary linear-mixed model (LMM) with a random intercept and random slope was fitted, using only completely observed covariates, and age as time variable. The random intercept and slope estimated by this model were considered a summary of the outcome, and were added as predictor variables to the imputation models.27
To study the effect of RA-related factors (disease duration, presence of ACPA, presence of RF, presence of erosions, past use of MTX) on the AMH levels, a LMM with random intercept and slope was built, using biological age as time variable. To obtain a more normal distribution of residuals and random effects in the LMM, a square root transformation was applied to the AMH levels. Interactions between ACPA, RF, and erosions, and between age and disease duration, were considered in the model. Pooled results from the 10 multiple imputed datasets are presented.
Since gynaecological age (ie, years since menarche) may more precisely explain the inter-individual difference than biological age, a second analysis was performed using gynaecological age as time variable.
Statistical analysis was performed using Stata SE v14 (College Station, Texas, USA) and R version 3.3.1 (2016, the R foundation for statistical computing; packages used: mice, lme4).
RESULTS
Patients
Serum samples for 128 patients (43% of the original PARA cohort) were available for analysis (figure 1). For two patients no questionnaire data were available for the latest visit, but they were included in the analyses. Baseline characteristics are given in table 1.
Characteristics of women with rheumatoid arthritis who participated in the PARA study and had a follow-up assessment in 2015/2016 (N=128)

Flow chart showing the patients from the original pregnancy-induced amelioration of rheumatoid arthritis (PARA) study that did participate in the current study and were available for analysis.
We compared the 128 study participants to the non-participating subjects (n=167) of the former PARA cohort (table 2). There was a significantly lower percentage of smokers among participants (7%) than in the non-participants (17%) (p=0.013). Furthermore, nulliparity was significantly more common among the non-participants (22%) than in the participants (4.7%) at the end of their final PARA episode (p<0.001). There were no significant differences in age, number of episodes participated in the PARA study, disease duration during the PARA study or current disease duration, presence of ACPA or RF, preconception disease activity during last PARA episode, or disease activity at the last PARA visit (either preconception or 6 months postpartum).
Comparison of participants and non-participants in the follow-up of the PARA study
Of the participants, 41 (32%) women reported amenorrhoea (ie, no menstruation in the preceding 12 months). In 29 women this could be explained by continuous oral contraceptive use (n=3) or the presence of a hormonal intra-uterine device (n=26), and 1 woman had a lactation amenorrhoea. Seven women had had a hysterectomy. In four women (3.1%) the amenorrhoea could not be explained by other causes, and they were considered postmenopausal. Their menopause had been at an age of 39, 44, 44 and 45 years, respectively. Three of them had AMH values below the LoD, and in one patient the serum AMH level was 0.0114 μg/L.
Hormone measurements
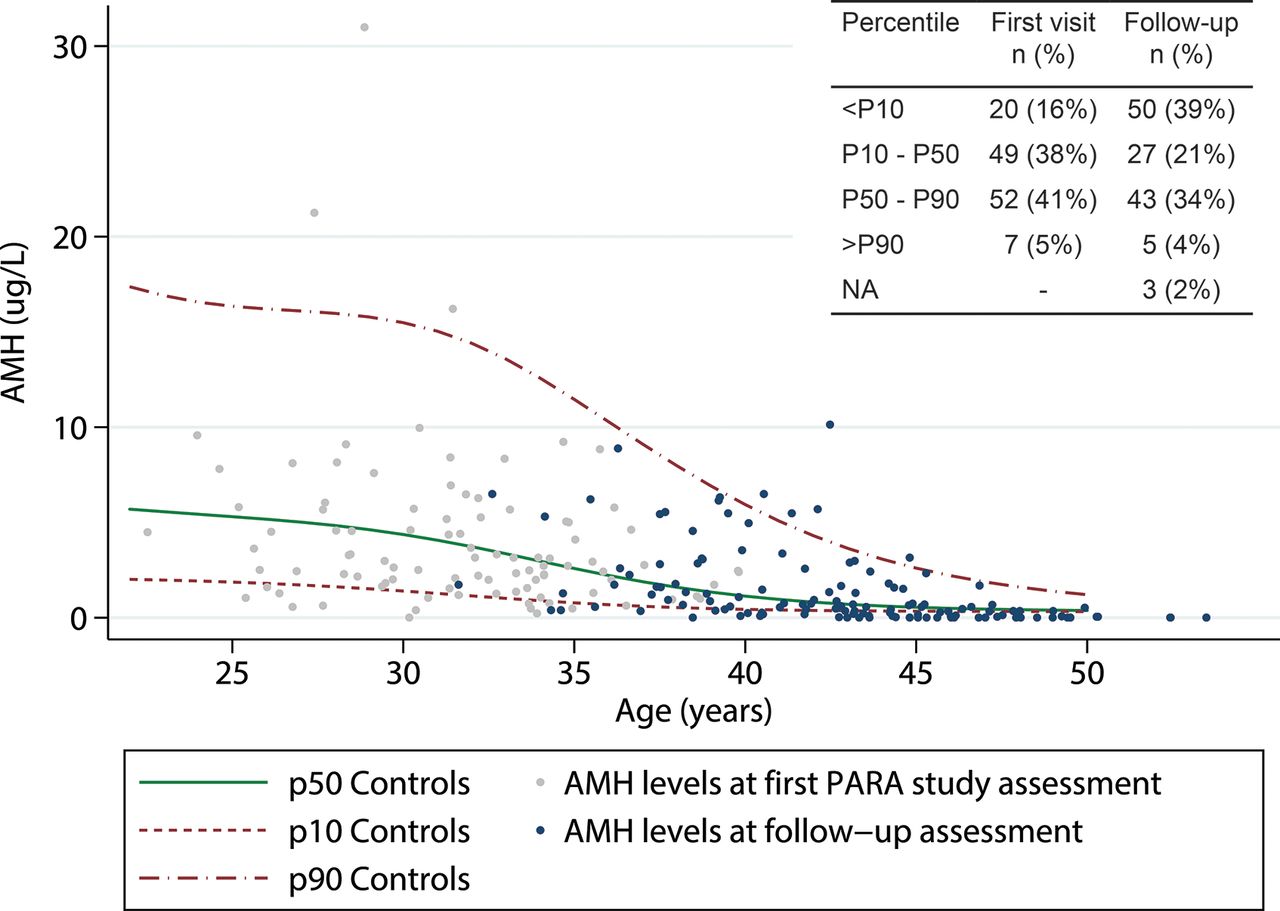
Participant serum AMH levels during follow-up were compared with AMH levels in healthy controls (figure 2). The mean age in controls was 30.6±7.4 years, with a range of 18.0–46.8 years. The age range for patients at the follow-up visit was 31.6–53.5 years. Corrected for age, AMH levels in women with RA at the follow-up visit were significantly lower than those in controls (p<0.001).

{kind=link}
{kind=link}
First and last available serum anti-Müllerian hormone (AMH) levels (μg/L) in women with rheumatoid arthritis who participated in the pregnancy-induced amelioration of rheumatoid arthritis (PARA) study and were visited again after 6.4–13.7 years. The lines represent the 10th, 50th and 90th percentiles of AMH values in healthy controls (Lie Fong 2012).
Looking at the age-specific percentiles, 50 RA patients (39%; 95% CI 31% to 48%) had a serum AMH level below the 10th percentile, compared with 20 patients (16%; 95% CI 9.3% to 22%) at the first available assessment (figure 2). At the follow-up assessment, 3 RA patients were older than 51 years, and as such, their age exceeded the age range of the nomogram (maximum age 51 years).
In RA patients not using oral contraceptives at the follow-up assessment (n=100), the percentage of women with AMH levels below the 10th percentile was 36% (95% CI 27% to 45%). In patients not using any steroid sex hormones at follow-up (n=61), this was 33% (95% CI 21% to 47%).
In table 3, the age-specific AMH percentiles are shown for all RA patients at the first and last measurement, grouped by disease characteristics. At the last assessment, higher percentages of patients with AMH levels below the 10th percentile were seen in ACPA-positive patients vs ACPA-negative patients, in RF positive patients versus RF negative patients, and in patients with erosions at baseline versus those without erosions at baseline. However, these differences were not statistically significant.
Distribution of age-specific percentiles of serum AMH levels in women with rheumatoid arthritis from the PARA study, grouped by serology and erosions
Linear mixed model
For one patient eight measurements were available, four patients had seven measurements, one patient had six measurements, 13 patients had 5 measurements, 50 patients had 4 measurements, 15 patients had 3 measurements and 44 patients had 2 measurements. The intra-individual mean time between the first available AMH measurement and the last was 10.7±1.8 years, with a range of 6.4–13.7 years. The mean age at the first AMH measurement was 31.8±3.8 years, and at the final assessment 42.6±4.4 years.
Repeated measurement analysis using an LMM in the RA patients showed a significant decrease of serum AMH levels with increasing age. None of the RA-related variables (disease duration, presence of ACPA, of RF, or of erosions, MTX use (ever)) did have a significant effect on the AMH levels over time in this group of 128 female RA patients (table 4). Comparing the full model shown in table 4 with a simple model of AMH based on age alone using a likelihood ratio test, did not reveal any significant differences, confirming the findings shown in table 4.
Estimates of linear-mixed model describing the change of serum anti-Müllerian hormone (AMH) levels (applying square root transformation) with increasing age in 128 female RA patients
The additional analysis with gynaecological age as time variable, was performed in the 122 patients that reported their age at menarche. Besides the decline of AMH with increasing gynaecological age, no other variables did show a significant effect. The full model based on gynaecological age was not significantly different from a simple model of AMH based on gynaecological age exclusively.
DISCUSSION
Women with RA had a compromised ovarian function compared with healthy controls, with a considerably larger proportion of women with RA having AMH levels below the age-specific 10th percentile. Assessment of serum AMH levels over time in female RA patients revealed that levels decreased more rapidly in patients compared with controls. Longitudinal analyses did not show any significant effect of RA-related factors on serum AMH levels.
The more rapid decline of serum AMH levels over time in women with established RA may indicate that chronic inflammation compromises ovarian function. The latter may even decline faster than was currently found in women with RA since the participants in this study represented a more fertile selection, with also less smokers, than the original PARA cohort. Since the original PARA cohort was already a relative healthy cohort,20 the true difference between women with RA and the general population may be even larger.
The compromised ovarian function in RA may be a direct effect of cumulative inflammatory damage to the ovaries. Ovarian ageing and inflammation are reported to be linked.28 Although we found no significant association between disease activity and AMH levels in current or previous analyses, there is a relation with ACPA-positivity, which represents patients with on average more active disease, often requiring a more intensive treatment strategy.29 We have previously reported significantly lower serum AMH levels in ACPA-positive patients,19 and in the current study more ACPA-positive than ACPA-negative patients appeared to have AMH levels below the 10th percentile. Furthermore, in the LMM, the negative association of ACPA-positivity with serum AMH levels was present, although non-significant, which may have been due to the lower number of subjects in this study. The present idea among rheumatologists is that ACPA-positive RA may be a different disease than ACPA-negative RA. It is not clear whether the reduced ovarian function is a result of this probably different disease mechanism, or of increased inflammatory damage due to longer periods of high disease activity. However, the lower AMH levels in patients who are ACPA-positive, fit with the overall concept that ACPA-positive RA is a more destructive disease with more extra-articular manifestations.29
Otherwise, there may be a genetic basis for the compromised ovarian function in RA. In genome-wide association studies, not only genes linked to DNA repair and genome maintenance have been related to age at menopause, but also genes linked to immune response seem to determine the timing of menopause.14 Whether RA and early menopause share a common genetic basis, may be the focus of future research.
The current study population was a more fertile selection of the original PARA study, represented by a lower percentage of nulliparity in participants than in non-participants. This is most likely due to the nature of the original PARA study and its first follow-up studies, focusing on pregnancy, childbirth, and the health of the children born during the study. Regular newsletters informed participants of the study outcomes. Several nulliparous women withdrew their consent for future contact. It is assumed this is because of the emotional burden of the regular reminders of their failure to conceive.
Regarding generalisability, we should also consider the recent changes in diagnosis and treatment of RA. Where patients from the PARA cohort were classified as having RA according to the 1987 ACR criteria,21 nowadays RA is often recognised and diagnosed at an earlier stage, when less damage has been done.30 Furthermore, new treatment guidelines have been developed over the last decade, focusing on early combination therapy in a treat-to-target regimen, and the addition of biological disease-modifying antirheumatic drugs such as tumour necrosis factor (TNF) inhibitors for a tighter disease management.31 The next generation of young female RA patients may therefore have a milder course of the disease, with better long-term outcomes. Whether ovarian function and reproductive performance will also benefit from these changes, should be addressed in future studies.
A possible limitation of our study is the use of hormonal contraceptives. Fifty per cent of the current participants used hormonal contraceptives during the follow-up assessment, mainly progesterone releasing intra-uterine devices, or the oral contraceptive pill (OCP). The effect of exogenous steroid hormones on serum AMH levels is still unclear, with several studies reporting no significant effect of exogenous hormones on serum AMH levels, whereas other studies have shown lower AMH levels in users of either OCPs or progesterone-only pills.32–34 Sensitivity analyses excluding women using any of these hormones, still showed one-third of patients having AMH levels below the 10th percentile at follow-up. Therefore, the current use of contraceptives could not explain the decreased long-term serum AMH levels in our study group compared with controls.
Several other factors may affect serum AMH levels, such as smoking and body mass index (BMI). Studies on the effect of smoking on AMH levels report varying results, ranging from no effect35 36 to decreased AMH level in smoking subjects.37 In both the control group and the most recent subject assessments, the smoking status was not assessed. The percentage of smokers among the studied patients was low during the original PARA study, and therefore the impact of smoking on the study results is expected to be minimal.
A higher BMI is associated with lower serum AMH levels.38 BMI was not recorded for the women included in the PARA study, but as reported previously, the median BMI for women 18–42 years in a representative Dutch RA cohort was 24.2 (21.9–28.3).17 Therefore, we assume that the lower AMH levels in the current study are not attributed to higher BMI values.
Both in the patient and the control group, blood sampling was done irrespective of the menstrual cycle day. Fluctuations of serum AMH levels in different phases of the menstrual cycle may be present. Since especially in the lower range of AMH levels cycle fluctuations are not considered to be clinically relevant,39–41 no significant effect on the study results are to be expected.
AMH levels in this study were measured with an ultrasensitive picoAMH assay, whereas the original control samples were not available for reassessment with this assay. The comparison of AMH levels between patients and controls should be considered with caution, since the conversion factor applied to the controls has been developed in another laboratory than the laboratory that performed the measurements with the new assay. Inaccuracy due to the conversion, may give deviating results.25 Furthermore, the currently applied picoAMH assay has a lower limit of detection compared with the Gen II assay that was used for the AMH measurements in controls. Nevertheless, adjusting the very low values in the current patients to the LoD applied in the controls, still resulted in a significantly higher percentage of patients with AMH values below the 10th percentile of controls.
New research questions arise from this study. Future research should focus on the effect of more severe disease, such as in ACPA-positive RA patients, on serum AMH levels. This may be elucidated in larger studies. Furthermore, studying the effect of chronic inflammation on ovarian histology in women with active RA may point towards causal mechanisms of the current findings.
For daily practice, it is important to realise that ovarian function and women’s health are strongly related. Several studies demonstrate the relation of decreasing AMH levels with the occurrence of natural menopause.42–45 Inaccuracy in the individual predictions remains, and therefore AMH measurements are currently only applicable for predictions on group level.46 Nonetheless, this study demonstrates an early decline in ovarian function in women with RA, possibly strongest in women with more severe disease. Rheumatologists should be aware of the adverse health effects of early menopause. Anti-rheumatic treatment should aim for suppression of disease activity to prevent health problems resulting from possible early menopause. Furthermore, in women displaying symptoms of early menopause, referral to a gynaecologist is advised.
In conclusion, serum AMH levels show a faster decline over time in women with RA compared with healthy controls, supporting the idea that in chronic inflammatory conditions, the body is less fit for reproduction. Optimal treatment of chronic inflammatory disease in an early phase may improve long-term women’s health.
Acknowledgments
The authors would like to thank all patients who participated in the PARA cohort and the follow-up studies. Furthermore, we would like to thank all rheumatologists who assisted in the recruitment of patients.
REFERENCES
Footnotes
Contributors All authors contributed to the design of the study, the analysis and interpretation of the data. JB, RJEMD, JMWH, JAV and JSEL contributed to the acquisition of data. All authors contributed to the drafting and critically revising of the work. All authors approved the final version published.
Funding This study was funded by the Dutch Arthritis Foundation (ReumaNederland). The picoAMH assays were generously provided by Ansh Labs (Houston, Texas, USA).
Competing interests JB, JMWH and JAV declare no conflicts of interests. RJEMD has received an unrestricted research grant from UCB Pharma BV. JSEL has received unrestricted research grants from the following companies (in alphabetical order) Ferring, Merck Sharpe and Dome, Merck Serono, Organon, Shering Plough and Serono.
Patient consent for publication Not required.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement Data are available upon reasonable request.