Article Text

Abstract
Objective Depression and anxiety are not uncommon in Rheumatoid arthritis (RA). It is increasingly recognised that they are associated with high disease activity and worse disease outcomes. We aimed to examine the frequency of depression and anxiety in an early RA inception cohort and to explore associations with disease-related measures.
Methods The Scottish Early Rheumatoid Arthritis inception cohort recruited newly diagnosed RA patients followed-up 6-monthly. Anxiety and depression were assessed using the hospital anxiety and depression scale. Associations with demographic characteristics and disease-related measures were examined at baseline, 6 months and 12 months.
Results 848 RA patients were included. The prevalence of anxiety and depression at baseline was 19.0% and 12.2%, respectively. Depression and anxiety scores correlated with DAS28 at all time-points (all p<0.0001). In multivariable linear regression, anxiety score at baseline was associated with younger age and Health Assessment Questionnaire (HAQ) score. Anxiety scores at 6 months and 12 months were associated with low body mass index (BMI), baseline anxiety score and current patient global score and HAQ. Depression score at baseline was associated with younger age, being single and HAQ, while depression scores at 6 months and 12 months were associated with male gender (only at 6 months), baseline anxiety and depression scores and current patient global score, HAQ and C-reactive protein (CRP) levels.
Conclusion Depression and anxiety are associated with disease activity, worse functional status and other variables in early RA. There is a close relationship between CRP and depression but not anxiety.
- Arthritis
- Rheumatoid
- Arthritis
- Autoimmune Diseases
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Supplemental material
Supplemental material
INTRODUCTION
Rheumatoid arthritis (RA) is a chronic inflammatory arthritis with both musculoskeletal and systemic features. RA is associated with several physical (eg, cardiovascular) and psychological comorbidities and it is increasingly recognised that depression and anxiety are associated with high disease activity, worse disease outcomes and decreased quality of life.1–6 Most studies investigating the association of RA with depression and anxiety are cross-sectional and performed in patients with established RA of several years’ duration2 4 and/or in patients having received treatment for RA.1 3 The frequency and relationship of psychological factors in early RA has been less studied and may differ from established RA. Here, we examine longitudinally the frequency of depression and anxiety in a large inception cohort of early RA patients and the relationship with demographic characteristics and disease-related measures.
Key messages
What is already known about this subject
Depression is not uncommon in rheumatoid arthritis (RA).
Depression is associated with disease activity and worse disease outcomes in established RA.
What does this study add
There is a close relationship of CRP with depression in RA.
In early RA, depression and anxiety are common, display an improving trend over time and associate with disease activity and worse functional status and outcome.
How might this impact on clinical practice or future developments?
Clinicians should be aware that anxiety and depression are common in early RA and that while treating RA properly appears to help anxiety and depression, this may not be sufficient.
METHODS
Cohort description
The Scottish Early Rheumatoid Arthritis (SERA) inception cohort7 prospectively recruited patients with new-onset RA (ACR-EULAR 2010 criteria) presenting to secondary-care rheumatology centres across Scotland between 2011 and 2015. Participants were treated by their usual rheumatology team as per standard clinical practice. Assessments were recorded at the baseline visit (within 6 months of their diagnosis) and then at 6 months and 12 months follow-up visits. A range of pre-specified features were recorded at the baseline visit and then at 6-monthly follow-up visits. These included demographic (age, gender, body mass index (BMI), current alcohol consumption, smoking, employment and marital status), clinical (tender and swollen joint counts, patient global assessment visual analogue scale (PGA-VAS) for disease activity, treatment being received), laboratory (Erythrocyte Sedimentation Rate (ESR), C-reactive protein (CRP), Rheumatoid factor (RF) and anti-cyclic citrullinated peptides (anti-CCP) status) parameters and disease-related indices (Disease activity score-28 (DAS28) and Health Assessment questionnaire (HAQ)—higher HAQ meaning greater disability). The authors assert that all procedures contributing to this work comply with the ethical standards of the relevant national and institutional committees on human experimentation and with the Helsinki Declaration of 1975, as revised in 2008. All procedures involving human subjects/patients were approved by the West of Scotland Research Ethics Committee (Reference 10/S0704/20). Written informed consent was obtained from all participants.
Study design
The Hospital Anxiety and Depression Scale (HADS) was completed by SERA participants at each visit. As has been previously suggested,8 anxiety and depression were analysed separately each having a score between 0 and 21. The ‘change’ of various scores and parameters (depression score, anxiety score, DAS28, CRP) was the difference between final and baseline values. Results were analysed as continuous variables except when determining the frequency of depression or anxiety. For these, variables were analysed as categorical, using established cut-off scores of ≥11 for probable cases of anxiety and/or depression.8 HADS was also recorded for age-matched and sex-matched individuals (n=58) with similar genetic background who were included as healthy volunteers in SERA cohort. As previously described,7 these were friends of relatives of the RA patients participated in the study.
Statistics
Univariable analyses were performed at baseline, 6months and 12 months. Two-sided Fisher’s exact and Mann-Whitney U tests were used to compare categorical and continuous characteristics, respectively. Wilcoxon matched paired test was used for paired continuous observations. Spearman’s rank correlation coefficient was used for correlations. Benjamini-Hochberg correction was applied for multiple-comparison correction for a false discovery rate of 0.25. Cronbach’s alpha test was used to measure internal consistency for depression and anxiety scales. Multivariable linear regression was performed using the anxiety and depression scores as dependent variables, and as independent variables the features recorded for the participants (see cohort description). These were: demographic (age, gender, BMI, alcohol consumption, smoking, employment and marital status), clinical (tender and swollen joint counts, PGA-VAS, treatment received), laboratory (RF status, anti-CCP status, ESR and CRP) and disease-related indices (HAQ). For depression and anxiety scores at 6 months and 12 months, baseline depression and anxiety scores were also used as independent variables. Collinearity diagnostics, calculating variance inflation factor, were run for all models. Independence of observations were checked using Durbin-Watson test. Homoscedasticity was also checked. Statistical analysis was performed using GraphPad Prism 5.00 (Inc. La Jolla, CA, USA) and SPSS 21.0 (Armonk, NY: IBM Corp, USA).
RESULTS
Patient characteristics
Data from 848 patients with RA were available for evaluation at baseline. Most of the patients (70.0%) were females and their mean±SD age was of 58.27±13.71 years. Their mean±SD DAS28, at baseline, was 4.95±1.41. Baseline characteristics and treatment received for RA during the first 12 months of follow-up time are presented in table 1. At baseline, 81 patients were already treated with psychotropic drugs (eg, serotonin-norepinephrine reuptake inhibitors). During the first 6 and 12 months of follow-up, only 10 and 4 additional patients were commenced on medication for mood disorders.
At 6 months and at 12 months, 691 and 618 RA participants, respectively, were available for evaluation. Comparing participants who continued their follow-up and those who did not, at the 6-month and/or 12-month time-points, there were no significant differences in either the percentages of patients with baseline anxiety or depression (at 6 months; anxiety: p=0.736, depression: p=0.178 and at 12 months; anxiety: p=0.168, depression p=0.157) or in the baseline anxiety or depression scores.
Prevalence of anxiety and depression over time
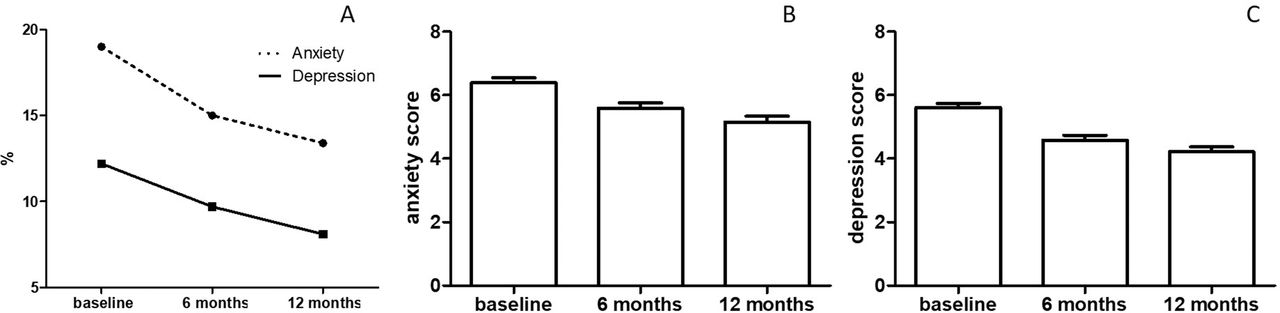
Frequency of anxiety and depression at baseline in early RA were higher than in healthy individuals (anxiety: 19.0% vs 1.7%, p=0.0002; depression: 12.2% vs 1.7%, p=0.009) and displayed an improving trend, over time. In fact, prevalence of anxiety and depression at 6 months was 15% and 9.7% and at 12 months, 13.4% and 8.1%, respectively (figure 1A). Anxiety and depression HADS scores were also highest at baseline and were decreased at 6 months and 12 months. Median (interquartile range—IQR) scores at baseline, 6 months and 12 months for anxiety were: 6.0 (3.0–9.0), 5.0 (2.0–8.0), 4.0 (1.8–8.0), respectively, and for depression were: 5.0 (2.0–8.0), 3.0 (1.0–7.0) and 3.0 (1.0–6.0), respectively. All Wilcoxon matched paired tests (6 months and 12 months, compared to baseline) are statistically significant (p<0.0001) (figure 1B,C). Separate subgroup analysis of the 81 patients who were already treated with psychotropic drugs at baseline indicated that the improving trend for both anxiety and depression was also observed in this group. However, statistical significance was only reached for comparisons between baseline and 12 months (online supplemental figure 1). In general, the internal consistency of the anxiety and depression scales was good. Cronbach’s alpha at baseline, 6 months and 12 months for depression were: 0.834, 0.860 and 0.855, and for anxiety were: 0.865, 0.888 and 0.892, respectively.

{kind=link}
(A) Prevalence of anxiety and depression measured by hospital anxiety and depression scale (HADS) in early rheumatoid arthritis over time from baseline (cut-off ≥11 for both). Longitudinal HADS anxiety (B) and depression (C) scores. Bars and lines represent mean and SEM, respectively. All Wilcoxon matched paired test (6 months and 12 months, compared to baseline are statistically significant, p<0.0001).
Association of anxiety and depression with RA disease activity
Anxiety and depression scores were significantly positively correlated with DAS28 disease activity scores at all time-points (online supplemental figure 2). Correlations were weaker for anxiety compared to those observed for depression scores. In detail, results were as follows: for anxiety; baseline (p<0.0001, r=0.187), 6 months (p<0.0001, r=0.299), 12 months (p<0.0001, r=0.332) and for depression; baseline (p<0.0001, r=0.333), 6 months (p<0.0001, r=0.401), 12 months (p<0.0001, r=0.454). A separate analysis examining the association between anxiety and depression scores with disease activity in the subgroup of patients who were already on treatment with psychotropic drugs at baseline (n=81) showed similar findings.
Supplemental material
Furthermore, baseline anxiety and depression scores correlated with DAS28 scores at 6 months and 12 months (online supplemental figure 3). For baseline anxiety; 6 months (p<0.0001, r=0.230), 12 months (p<0.0001, r=0.217) and for baseline depression; 6 months (p<0.0001, r=0.265), 12 months (p<0.0001, r=0.217). Change (final–baseline values) in the anxiety and depression scores of the patients correlated with change in DAS28 scores at both 6 months and 12 months (online supplemental figure 4). For anxiety; 0–6 months (p=0.001, r=0.160), 0–12 months (p<0.0001, r=0.255) and for depression; 0–6 months (p<0.0001, r=0.291), 0–12 months (p<0.0001, r=0.368). It should be noted that correlation of change in anxiety scores with changes in DAS28 at 6 months was relatively weak.
Supplemental material
Supplemental material
Associations with demographic, clinical and biochemical measures of RA
The demographic, clinical and biochemical features associated with anxiety and depression in the univariable analyses, at the three time-points examined, are presented in tables 2 and 3.
Baseline characteristics of the rheumatoid arthritis patients included in the analysis
Univariable analysis. Variables associated with anxiety and/or depression scores at baseline, month 6 and month 12. All variables are at baseline unless otherwise indicated by ¶. Significant values are highlighted in bold
Anxiety and depression scores for categorical variables presented in table 2
Multivariable linear regression analysis. Variables associating with high anxiety and/or depression scores at baseline, month 6 and month 12. All variables at baseline unless otherwise indicated by‡
Notably, analysing further the association of CRP with depression (but not anxiety) at all time-points, we found that change (final–baseline values) in CRP levels also correlated with change in depression scores at all time-points (0–6 months; P<0.0001, r=0.185 and 0–12 months; P<0.0001, r=0.302).
Multivariable linear regression analysis largely confirmed results from univariable analyses and are presented in table 4 (only parameters that were statistically significant for at least one time-point are presented). The anxiety score at baseline was correlated with younger age and HAQ score (higher HAQ meaning greater disability). At 6 months and 12 months, the anxiety score was associated with baseline anxiety score, lower BMI and higher current HAQ score and PGA-VAS score. The depression score at baseline was also associated with younger age, HAQ and additionally with being single. At 6 months and 12 months, the depression score was associated with baseline depression and anxiety scores as well as with male gender (only at 6 months), current PGA-VAS scores, HAQ scores and CRP levels.
DISCUSSION
Depression and anxiety are important comorbidities in RA and are associated with less favourable disease outcomes and reduced quality of life. The prevalence of depression in our cohort was 13%. The reported frequency of depression in published RA studies ranges between 13% and 56%.9 10 However, investigators examining psychological comorbidities in RA have used different tools to assess this, making it difficult to compare between studies. Our study used HADS, which is highly reliable in the detection of depression in RA.11 A meta-analysis estimated that depression, measured by HADS, occurred in 14.8% of RA patients.10 Anxiety is even more frequent than depression in both our cohort (19%) and the published literature (25–46%).1 3
It is generally recognised that depression and anxiety scores in RA decrease over time, which was also observed in our cohort over the first 12 months following diagnosis.12 13 The reasons for this are currently unclear but several parameters (eg, better control of RA, less inflammation) might contribute. As also observed in our study, depression score is associated with RA disease activity,13 although the direction of this relationship has not been defined14 and causality cannot be inferred from observational studies. Of note, correlations between disease activity and anxiety scores were weaker compared to that recorded for depression scores.
Several studies report that baseline depression and anxiety levels in RA are associated with decreased likelihood of achieving remission,1 3 4 although others have not found this.2 On the other hand, studies in early RA report that higher joint counts at baseline are associated with increased depression at month 6.13 Another study suggested that the HAQ score was the most important predictor of psychological stress in early RA,12 with a variety of other demographic and socio-economical features like occupation and family income to be associated with depression and anxiety in RA.12 In our study, univariate analyses identified a number of factors associated with HADS anxiety or depression scores at all time-points including baseline depression and anxiety scores, unemployment, being single, younger age, HAQ score and increased disease activity measures.
Multiple linear regression analysis indicated that current HAQ scores and baseline depression and anxiety scores were the strongest predictors of depression and anxiety scores. The association between HAQ and depression is consistent with findings from another study using data from SERA cohort, which reported that functional disability at 1-year after RA diagnosis was predicted by depression and anxiety among other factors.15 Similarly, another study examining predictors of depression in a multi-ethnic RA cohort showed that higher HAQ scores were associated with depression.9 Furthermore, in the multivariable analysis in our study, CRP and PGA-VAS were the only measures of disease activity assessed by DAS28 associated with depression.
Notably, CRP was associated with depression but not anxiety at all time-points in univariate analysis and at 6 months and 12 months in the multivariable analysis, suggesting a close relationship between inflammation and depression. This is consistent with a previous cross-sectional study, which reported that CRP was significantly correlated with depression levels in RA.16 Another study of RA patients with DAS28≥3.2 and disease duration between 3 months and 2 years reported higher CRP levels at baseline in patients who had depression compared to those who did not.1
There appears to be a complex interplay between depression and RA, with shared inflammatory pathways postulated.17 It has been suggested that the aberrant immune responses in RA could cause alterations in the central nervous system via neuronal and humoral pathways.17 Notably, Schrepf et al 18 have demonstrated how chronic inflammation in RA has an impact on the brain. Higher peripheral inflammation was consistently correlated with neural connectivity patterns, particularly inferior parietal lobule and medial prefrontal cortex over a 6-month period. The RA-depression immunobiological axis is evidenced by various data. For example, in RA blockade of systemic TNF has beneficial effects on centrally mediated behaviours including mood.19 Further, anti-TNF therapy in RA acutely alters fMRI brain activation.20 21 This aligns with significant overall improvement in well-being, which patients can report often in advance of any objective improvement in their peripheral joint inflammation for example, swollen joints. Said that, as mentioned earlier, in the multiple regression analysis of our study, depression was associated with CRP and PGA-VAS but not with tender or swollen joints count. Our data, especially those showing the relationship between CRP and depression over time support this peripheral blood-neural network link in RA. It also provides a supportive perspective on the increasingly compelling data implicating the immune-inflammatory response in some aspects of the pathophysiology of mental disorders17 notably major depressive disorder.22–24
Herein, we show, as previously reported,13 that anxiety is highly prevalent in early RA. In our study, patient global VAS correlated with anxiety levels, which could partially explain the association between anxiety and worse disease activity outcomes in RA.25 However, in contrast to what we observed for depression in our cohort (as outlined above), anxiety was not associated with CRP, neither in univariate nor in multivariable analysis. The reasons for this are not clear and merit further investigation. It should also be noted that ‘anxiety’ encompasses a heterogenous spectrum of symptoms, ranging from contextual physiological anxiety through to anxiety disorders,26 with some but not others associated with some degree of inflammation.27 A more focused analysis might reveal whether there is an ‘anxiety phenotype’ in RA that is possibly linked with inflammation.
The inverse correlation between BMI and anxiety (but not depression) levels at 6 and 12 months in our study is not surprising, considering that large population studies have shown a U-shape relationship between anxiety and BMI.28 Data from the Rochester Epidemiology Project indicate that anxiety is increased in underweight and obese, but not overweight, people. This association was more pronounced in females.28.Finally, in our early RA cohort, baseline anxiety levels were found to be significantly associated with subsequent anxiety scores, highlighting that anxiety should also be considered in the treatment plan of patients with RA, from the early stages of disease.
Many studies examining psychological comorbidities in RA typically focus on depressive symptomatology and disregard anxiety or describe the psychological burden without distinguishing between depression and anxiety. However, as shown here, there are differences between depression and anxiety, at least in terms of the associating factors in RA, further reinforcing the notion that they should be assessed separately.
We acknowledge that our study has certain limitations. First, consistent with the design of this inception cohort, no data are available for depression, anxiety or disease activity at time-points between baseline and the 6 months and 12 months visits. Given the stable trend of our results, we speculate that it is unlikely that an important finding would have been missed. Similarly, limited data were available for patients followed-up for a longer time period. These, however, are continuously recorded and will be analysed in future studies. Furthermore, the number of healthy individuals is small compared that of RA patients and there may be some differences in the performance of the HADS questionnaire between healthy and RA individuals. Therefore, the differences between these two groups should be interpreted with caution. Finally, although some of the findings have been shown by other studies as well, our early RA inception cohort is one of the largest, examining longitudinally mental health disorders, with a validated tool in these patients.
In conclusion, our study indicates that clinicians should be alert to neuro-psychiatric comorbidity in RA from the earliest stages of the disease when the prevalence and levels of depression and anxiety appear to be highest. While depression and anxiety have been shown to have a negative impact on outcomes in RA, it remains to be determined whether more intense screening and treatment for psychiatric comorbidities, especially in some subgroups of patients (eg, those with high CRP, high HAQ scores) can improve outcomes. Our results also highlight again the link between inflammation and depressive symptomatology. The intertwining of these conditions points to potential common pathophysiology thus opening the possibility of greater mechanistic understanding and thus greater therapeutic opportunity.
Acknowledgments
We would like to thank SERA investigators for their contribution in data collection.
REFERENCES
Footnotes
Contributors GEF: drafting the manuscript, data analysis, data collection. JC: drafting and critically revising the manuscript. AT: drafting the manuscript, data analysis, data collection. MHD: drafting the manuscript, statistical analysis. CP: drafting the manuscript, data collection. DP: data collection, critically revising the manuscript, inception of the study. IBM: data collection, critically revising the manuscript, inception of the study. SS: data collection, drafting and revising the manuscript, inception of the study.
Funding The SERA cohort was supported by joint funding from the Chief Scientist’s Office (award ref ETM-40) and Pfizer.
Competing interests None declared.
Patient consent for publication Written informed consent was obtained from all participants.
Ethics approval All procedures involving human subjects/patients were approved by the West of Scotland Research Ethics Committee (Reference 10/S0704/20).
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement Data are available upon reasonable request. All data relevant to the study are included in the article or uploaded as supplemental information.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.