Article Text

Abstract
Objectives To evaluate an intervention to reduce the nocebo effect (NE) when switching from the originator infliximab (OI) to the infliximab biosimilar SB2 in chronic inflammatory rheumatic disease (CIRD).
Methods An intervention was built with healthcare professionals (HPs) and a patient representative, based on a systematic review of interventions reducing the NE in musculoskeletal diseases and semi-directed questioning of five patients. Our strategy consisted of training HPs, switch information given by the nurses, a consistent vocabulary. All CIRD patients switched from OI to SB2 were included for the intervention. The primary outcome was the SB2 retention rate (RR) at 34 weeks. Secondary outcomes were the SB2 RR at 12 months, discontinuation rates due to a possible NE and comparison with a historical cohort of CIRD patients receiving the OI and 6 published European cohorts.
Results 45 patients were included from March 2018 (rheumatoid arthritis, n=17, spondylarthritis, n=28). After 34 weeks, the SB2 RR was 91.2%, similar to the historical cohort RR (p=0.41) but higher than the 3 European cohort RRs (p<0.05). At 12 months, the SB2 RR was 84.5% vs 88.4% for the historical cohort (p=0.52). SB2 discontinuation due to a possible NE was 6.6% after 12 months.
Conclusions A tailored communication with a prominent role of nurses reduced the NE in non-medical switches from the OI to SB2 as compared to published results. The RR was similar to the historical cohort RR. The methodology used to construct this intervention may help improve the outcomes of switches with upcoming biosimilars.
- Biosimilar Pharmaceuticals
- Arthritis
- Rheumatoid
- Spondylitis
- Ankylosing
- Infliximab
- atient Care Team
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Key messages
What is already known about this subject?
Owing to cost-effectiveness considerations, health authorities promote switches from originator biologics to biosimilars. Lower retention rates of biosimilas in real life studies compared to double blinded controlled trials have been observed and may be explained by a nocebo effect.
What does this study add?
This study describes an intervention that reduced the nocebo effect when switching from the originator infliximab to an infliximab biosimilar.
How might this impact on clinical practice?
The methodology used in the present study ie, building an intervention after investigation of patient's perspective, and ensuring consitent communication from all healthcare professionnal - may be used for future switches to other biologic agent biosimilars.
INTRODUCTION
Biologic drugs (BDs) have transformed disease outcome for patients with chronic inflammatory rheumatic diseases (CIRDs), but at high cost for healthcare systems.1–3 Since 2014, biosimilar drugs (BSs) -replicas of BDs whose patents have expired, have been developed. Biosimilars meet criteria for similarity in structure, pharmacokinetics and pharmacodynamics plus non-inferiority in terms of efficacy, safety and immunogenicity demonstrated in phase 3 clinical trials.4 Consensus-based recommendations state that biosimilars can be used to treat CIRDs in the same way as their biologic originators.4 Their lower price has become crucial in healthcare saving policies.4 5
Double-blind-randomised control trials (RCTs) assessing a switch from the originator infliximab (OI) to an infliximab BS have reported comparable efficacy, safety and immunogenicity, with no difference in discontinuation rate,6–9 which remained low, from 6.4% to 7.5%. Conversely, discontinuation rates were higher in open-label RCTs (11–36%)9 and even higher for real-life observational cohorts9 (up to 30%), for which most withdrawals were due to subjective or non-specific adverse events/non-specific symptoms (NSAEs/NSSs).10–12 Given the lack of pharmacological explanation for the gap in outcomes between blinded and open studies, the difference may be due to a nocebo effect (NE).10–14 This is supported by reported concerns of patients about the efficacy (40–60%) and safety (35–57%) of BSs15–17 and switches (83–85%).18 Half of healthcare professionals also expressed concerns about switches.19
The NE, an emerging concept in rheumatology,9 is indexed in MEDLINE as ‘an adverse effect occurring with a medical treatment that cannot be attributed to the treatment’s effects’.20 Reducing the NE during switches could enable better BS acceptance, with advantages from an individual and public health point of view.4
Some recommendations,4 5 patients’ claims and ethics21 22 emphasise that no switch to a BS be initiated without patients’ awareness. Some studies implemented appropriate interventions (structured communication strategy, shared medical decision) aiming to reduce patients’ reluctance for the switch, yet without detailing said interventions.10 23 Moreover, risk factors of NE after the switch, hence factors to be addressed in an intervention, have not been identified, so construction of an intervention is more challenging.
Because the healthcare professional–patient interaction affects healthcare outcomes,24 we aimed to build and evaluate the efficacy of an intervention for reducing the NE during a non-medical switch from the OI to its BS SB2, hoping to improve the switch’s efficacy and tolerance. We hypothesised that the intervention would allow a higher BS retention rate (RR) and lower rate of NE/NSAE/NSS as compared with data from a historical cohort and published studies.
PATIENTS AND METHODS
Construction and implementation of the intervention
Step 1: a systematic literature review (inception to 15 November 2018) was conducted to identify risk factors (RFs) and intervention strategies to reduce the NE in musculoskeletal diseases, and more specifically in switches from originators to BSs. The method, flow chart and full results are available in online supplemental materials (online appendix 1, 2 and 3).
Supplemental material
Six studies collected RFs of withdrawal after a switch. However, conclusions could not be drawn because the RFs identified were markers of higher disease activity and treatment failure (online supplemental material, table 1).11–13 25–27
Baseline characteristics of the SB2 cohort and the historical originator infliximab (OI) cohort
Five studies aimed to reduce the NE during switches by an intervention targeted to patients: two studies used a shared decision-making method and a structured communication strategy,10 27 and two used a standardised information.12 23 One study focused on doctor training.26 Only one study compared NSAE/NSS in both switched and historical cohorts but failed to prove an intervention efficacy27 (online supplemental table 2).
Retention rate (RR) at 34 weeks. Comparison with published European cohorts with endpoints at 34 weeks
Step 2: Patient’s perspective: a trained rheumatologist conducted semi-directive interviews with five patients who received intravenous abatacept or tocilizumab for rheumatoid arthritis. Those were not immediately concerned by a switch but might be in the future. The aim was to clarify patients’ knowledge and perceptions of BS, the information needed, and how patients expected the information to be delivered. The interview schedule and patients’ demographics and responses are available in online supplemental materials (online appendix 4). Interviews showed low knowledge of BS, notably their efficacy and tolerance; fear of adverse effects, fear of change, preference for status quo; concerns about whether BSs were different from generic drugs; the need to be allowed to share with the medical team their medical history of side effects, especially those due to generic drugs; needs for support and to be able to decide for themselves, the will to be allowed to resume the biologic originator; and the demand for honest information from health professionals. One of the results was patients’ need to know the perception of and experience with biosimilars of the day-care nurses. The number of patients interviewed was small since the intervention was part of a routine care assessment.
Step 3: Construction of the intervention in a multidisciplinary fashion, based on the results of steps 1 and 2 and patients’ and rheumatologists ‘perception of BSs in published surveys.16–18 29 No qualitative study was found in literature on patients’ perceptions of BSs.
Switch modalities and messaging and vocabulary tools (online appendix 5) were set up during a multidisciplinary meeting including 3 rheumatologists, 1 resident, 1 pharmacist, 3 nurses and 1 patient representative of a patient’s association. During another dedicated meeting, all doctors and nurses involved in switches received training concerning BSs and the NE; they were informed about the results of previous steps and the switch modalities and information available (oral and written).
The switch modality was as follows: on infusion day, before the medical consultation and BS prescription, the day-care nurses provided oral information (a simple sentence mentioning a change of name) and written information (letter, online appendix 6) to patients and answered the questions that emerged according to the pre-determined semantic tools and the patient’s needs. During the medical consultation by the resident or the rheumatologist in charge of the day-care unit (ie, not systematically the patient’s own rheumatologist), information was given according to the same modalities. Upon request, an information booklet on BS developed after step 2 was distributed (online supplemental materials, online appendix 7). If needed, an interview was proposed with a doctor trained in motivational communication. The vocabulary tools focused on similarity between BO and BS, proof of efficacy and safety in wide clinical studies, the strict manufacturing process, and on the knowledge HPs already had on BS: existence of BS for other drugs, use of SB2 in the department for other patients. If patients asked, we insisted on the difference between BS and generic drugs, and explain reasons for a lower price of the BS.
Step 4: Implementation of the intervention: a non-medical switch (ie, not initiated by the patient or the physician) from OI to the infliximab BS SB2 was requested by hospital directors for all patients receiving OI. All patients with CIRD (rheumatoid arthritis [RA], axial or peripheric spondylarthritis [SpA], including psoriatic arthritis [PSA]) currently receiving OI received the support strategy described above and were included. Switches started in March 2018 until every day-care patient was seen at least once; follow-up lasted 1 year. Intervention implementation was not monitored.
Follow-up
Patients were followed up in routine care; treatment change was decided by the rheumatologists in charge. Drug maintenance, side effects and disease activity were routinely assessed at each infusion. Data were analysed from medical records.
Outcomes
The primary endpoint was the RR of SB2 after 34 weeks. Secondary endpoints were the SB2 RR at 12 months; SB2 discontinuations due to NE/NSAE/NSS at 34 weeks and 12 months; comparison of RR and discontinuations due to NSAE/NSS with data from a historical cohort and with RRs from published European studies; and assessment of RFs of withdrawals.
Comparison groups
Because the NE had been revealed in real-life studies vs RCTs, comparison with other real-life studies and cohorts was considered adequate for the study purpose. Therefore, we compared data with that from a historical cohort and the literature. The historical cohort consisted of all patients with CIRD receiving IO at 1 year before the switch in the same rheumatology department. Data were collected from patients’ files.
For comparison with the literature, we used European cohorts with similar follow-up: Tweehuysen et al, 2018,11 Scherlinger et al, 201812 and Avouac et al, 201828 for the primary endpoint; Nikiphorou et al, 2015,14 Boone et al, 2017,10 Glintborg et al, 201713 for the 1-year follow-up.
Definition of NE
For each biosimilar withdrawal, the patient’s file was examined by an independent evaluator to assess NE/NSAE/NSS. In case of doubt, consensus was achieved with a second independent evaluator.
An NE leading to BS withdrawal was defined as lack of efficacy with no objective criteria for increased inflammation (ie, CIRD worsening or end-of-dose wear-off without increased level [CRP] or erythrocyte sedimentation rate [ESR], number of swollen joints, or flare of a concurrent disease [inflammatory bowel disease, uveitis or psoriasis]) or non-objective and non-specific side effects (ie, fatigue, headache, anxiety). NE was retained if the symptoms occurred after the switch and disappeared after a back-switch or change of BD. Criteria for NSAE/NSS in the historical cohort were the same lack of efficacy or subjective adverse events and disappearance after change of BD.
Statistics
The number of patients to include to detect a 50% increase in RR as compared with the only French study of non-medical switches28 was 52 (alpha risk 5%, power 80%). To compare the RR with literature data, we used the χ² test or Fisher exact-test as appropriate. We expressed drug maintenance with Kaplan–Meier curves and applied the log-rank test for univariate comparison between the historical and switch cohorts. For comparing variables between baseline and 1 year after the switch, we used the Friedman test.
For risk factor analysis, we used descriptive statistics and tested significance with the χ² or Fisher exact test as appropriate. For quantitative variables, we used the Student’s t-test or a non-parametric test according to the data distribution. P<0.05 was considered statistically significant.
Patient and public involvement
Patients were involved in the construction of the intervention, not in the recruitment. Results will be shared via conference presentation.
Ethics
This study is an observational study registered at the national agency for drug safety biological research and collections registration service (l’Agence nationale de sécurité du médicament [ANSM]) as part of a search in routine care assessment of the registered and approved patient education programme in the rheumatology department (RCB ID: 2018-A00695-50) and the IT and freedom commission (Commission Nationale Informatique et Liberté; CNIL no. 1734260).
RESULTS
We included 45 patients with a switch from March 2018, who were followed up until August 2019. Initially, no patient refused SB2 treatment. Every patient had a consultation with a rheumatologist (resident or attending) before BS prescription, as part of routine care. No patient required a specific consultation with a rheumatologist to discuss switch beforehand. Only one patient, who described loss of efficacy after the switch was addressed to the rheumatologist trained in motivational communication, but she refused to resume SB2. Three patients were excluded: one for pregnancy, one because follow-up was planned in another hospital and one with SAPHO (synovitis, acne, pustulosis, hyperostosis, osteitis). In the historical cohort, 52 patients were included between December 2016 and February 2018. Baseline characteristics of the cohorts were similar (table 1).
Retention rate
Mean follow-up at first evaluation (34 weeks) was 235 (SD 5.4) and 238 (SD 0) days in the SB2 and historical cohorts. RRs were 41/45 (91.2%) and 50/52 (96.2%) (p=0.41). SB2 RR was significantly higher than in other European cohorts with similar follow-up (p<0.05) (table 2).
NSAE: non-specific side events. NSS: non-specific symptoms. OI: originator infliximab. RR: retention rate. CRP: ESR: erythrocyte sedimentation rate.
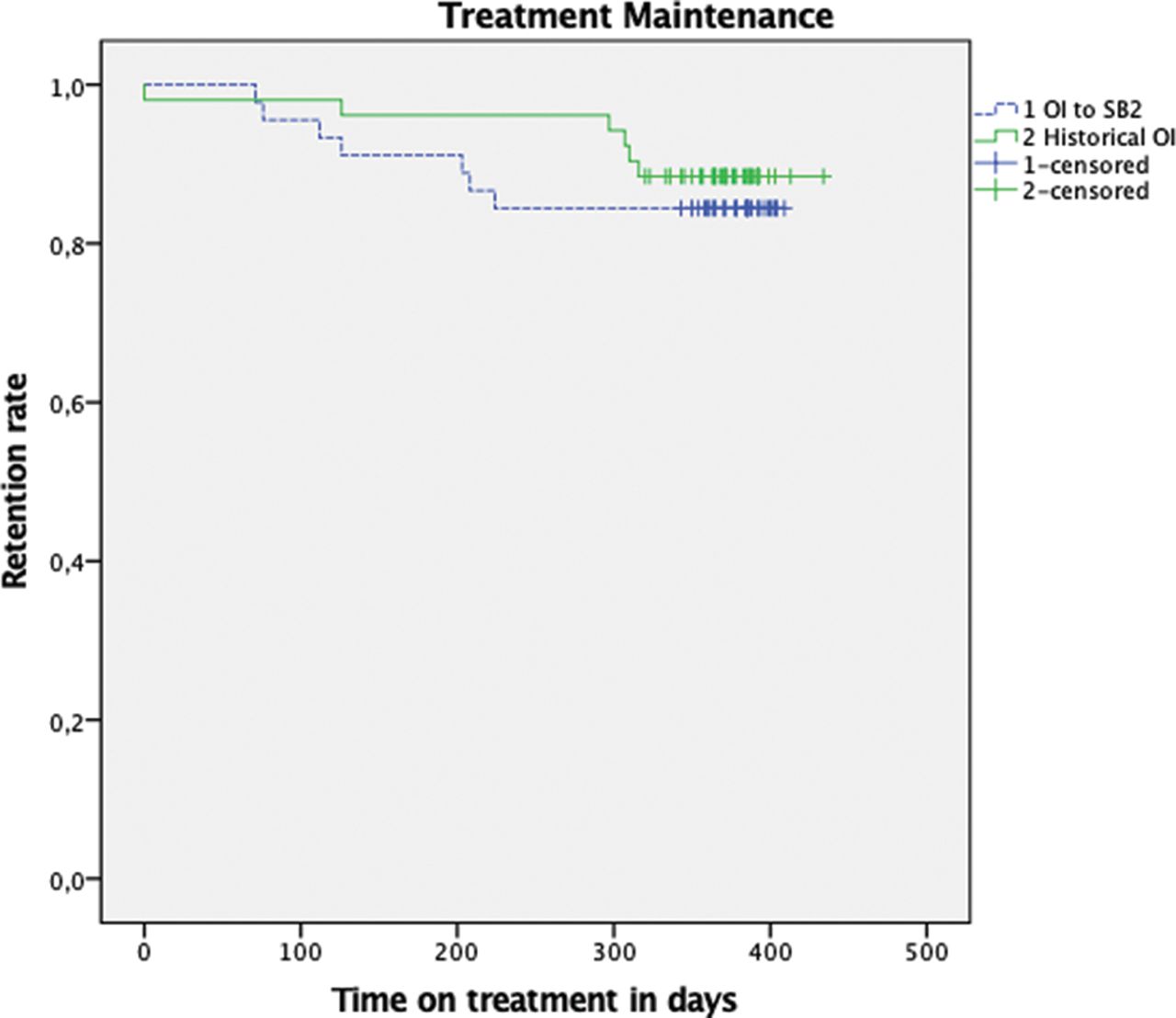
Mean follow-up at 12 months was 368 days (SD 14.6, 95% CI [CI] 339.3-396.8) and 410 (SD 10.8, 388.8-431.2) for the SB2 and historical cohorts. RRs were 38/45 (84.4%) and 46/52 (88.5%). Withdrawal-free survival did not differ between the two cohorts (p=0.520) (figure 1). The SB2 RR did not differ from that of other European cohorts with an endpoint evaluated at 12 months (table 3).
Retention rate 1 years after the switch, comparison with published European cohorts
{kind=link}
Treatment withdrawal-free survival (SB2 in switched cohort and originator infliximab [OI] in historical cohort).
Kaplan-Meier survival curves. Comparison with log-rank test for OI to SB2 and historical OI, p=0.520.
Reasons for OI discontinuation are detailed in table 4.
Reasons for SB2 in switched cohort and historical OI cohort
Efficacy and safety
Patient global score, disease activity score in 28 joints and Bath Ankylosing Spondylitis Disease Activity Index were unchanged between baseline and 1-year follow-up (p=0.316, p=0.369 and p=0.390, respectively); CRP level was significantly higher at baseline than at 1 year (mean 4.5 [SD 78] vs 2.5 [SD 8.7] mg/l, p<0.001). No adverse event causing hospitalisation occurred after the switch.
NE: nocebo effect. NSAE: non-specific side events. NSS: non-specific symptoms. OI: originator infliximab.
Nocebo effect and non-specific adverse events or symptoms
At 34 weeks, withdrawals due to NE/NSAE/NSS were 1/45 (2.2%) in the switch group (table 2) and 1/52 (1.9%) in historical cohort (table 4). At 12 months, withdrawals due to NE/NSAE/NSS were 3/45 (6.6%) in the switch group (table 3), and 1/52 (1.9%) in the historical cohort (table 4). Withdrawals in the SB2 group occurred after 1, 3 and 5 SB2 infusions, respectively. One patient with axial SpA described loss of efficacy, increased pain and fatigue on day 1 of SB2. Another SpA patient reported increased end-of-dose wear-off, and one RA patient had new onset of fatigue. None had synovitis or elevated ESR or CRP level; all symptoms improved after a back-switch to OI.
The number of withdrawals was too small for statistical analysis of risk factors. Baseline characteristics of patients who withdrew SB2 are in table 5.
Baseline characteristics among withdrawers in the 2 cohorts
DISCUSSION
In this real-life observational study, we monitored the efficacy of an intervention to limit NE and improve maintenance after a non-medical switch from OI to SB2. The intervention was constructed after a literature search and semi-directives interviews, which emphasised that patients had low knowledge of BS, needed information on the differences between BS and generics, had fears about their efficacy and tolerance and needed to be supported, with a prominent role of nurses. The intervention was standardised and involved all healthcare professionals. We found a significantly better RR at 34 weeks than that in three published European real-life studies11 12 28 and no significant difference in RR from that for a historical OI cohort. Although the crude RR was higher in the historical cohort, the difference between the switched and historical cohort is low as compared with the other French study with the same data.12
As concluded in our systematic review, interventions to reduce NE were scarce and did not provide positive outcomes as compared with historical cohorts.27 Plus, the intervention methods were seldom available and not precisely described in the literature. Therefore, the present study adds information as to which strategy could be beneficial to patients.
Our structured communication was based on a prior investigation of patients’ needs and perspectives and the inclusion of a patients’ association representative when building the intervention. Interventions in the literature resulted mostly from agreement between healthcare professionals.23
According to patients interviews in step 2, the nurses’ experiences on switches were particularly valued. Although the role of nurses in patient education and management of CIRD is well known,30–32 it had not been investigated for drug switches. Our interpretation is that patients were used to meeting the same nurses for their infusions. Conversely, doctors in the day-care unit change over time, and consultations with the rheumatologist are few. Therefore, patients develop close interactions with nurses, who may not be the same during the switch of sub-cutaneous biologics. Surveys33 have also concluded that nurses possess communication skills and competencies in patient education and qualitative studies have also emphasised that nurses might be ‘easier to talk to’.31
We believe that our results are in favour of including of nurses in the intervention, as the first point of contact in announcing the switch to patients, since none of the patients requested a specific consultation to discuss the switch, in addition to the consultation with the rheumatologist or the resident in charge of the day-care unit.
A non-systematic literature search of the NE when constructing the intervention allowed for a closer insight into its determinants. Negative expectations are a known NE mechanism,34 35 and mistrust in healthcare systems or BSs may participate. Some interventions have used literature data to convince patients of the BS benefits23 and cost-saving interests. However, a quantitative survey in France showed that fears were high for effectiveness (60%) and tolerance (75%,17) Reduced costs generated by the switch would be an incentive in only 20% in this study.17 These findings are consistent with the patients’ answers to the semi-directive interviews made in the department. Strong beliefs exist among patients in all countries that less expensive medication equals lower quality.36 Lower use of generic drugs in France compared to other countries such as The Netherlands or Denmark (30% vs 70% and 44% of market share)37 may indicate a higher mistrust and concerns about generic drugs and drug branding. Of note, studies of NE found that over-communication about adverse events could be counter-productive and fear-generating,38 39 which we considered in the present intervention. Such over-communication started with the dissemination of brief information, which was then intensified upon the patient’s request. In total, appropriate communication including a positive framing and avoiding negative suggestions was used according to prior studies.39 40
Given this tailored intervention, we obtained a good outcome in terms of RR at 34 weeks, which was the primary endpoint, and compared it with the literature and our historical cohort. Assessment at 34 weeks was considered appropriate because the few published intervention studies also had a follow-up at 6 and 7 months. These favourable results were obtained despite the injunction for a non-medical switch imposed by the hospital authority, preventing a shared decision-making process as recommended4 and formally used.10 Although patients could refuse the switch to SB2, we were not sure that the hospital pharmacy could provide OI over time.
At 12-month follow-up, our biosimilar RR did not significantly differ from that from the 3 other real-life published studies.10 13 14 However, comparisons are difficult. Our results are better than in one study (84.5% vs 71.8%), with a lack of statistical significance possibly explained by the small patient sample.14 In another study10, 15% of the patients refused the non-medical switch as compared with none in the present study; only 20% of the patients had CIRD and others had inflammatory bowel diseases. In our study, uncontrolled disease activity was not an exclusion criterion, which may also have favoured a higher withdrawal rate. At 12 months, we found a low NSAE/NSS rate: 6.6% (3/45), vs 15.3% and 12.5% in published studies.10 14 A low number of NE events did not allow for analysis of RFs of the NE. Two of three events occurred after 34 weeks, which contradicts a hypothesis that the NE occurs rapidly after a switch.13 Of note, these two patients retained NSSs after a backswitch to the OI.
The strength of the study is an intervention close to patients’ perspectives. The conclusion of the qualitative step are consistent with international surveys on the patients’ perspective16–18 29 However, although we tried to explore the patients’ opinion on BSs in our department, the small number of patients interviewed may impair the validity of our conclusion on this point since the saturation was not reached, particularly on the role of nurses which has not described so far in literature. The intervention content may differ by countries, but the methodology may be shared to improve switch outcomes, based on contextual considerations. For example, patients may differently favour the role of nurses in switches to subcutaneous BSs, depending on the organisation in other departments or private practice.
Our study has several limitations: we had no control group but rather a historical cohort, with therefore limits in comparability. Moreover, some patients in the switch cohort received the OI in the historical cohort, so statistical comparison between groups was challenging. However, a real-life design was needed to study NE, which had not been identified in RCTs. Another limitation is the low number of patients (45). Nevertheless, our results showed a statistically significant improvement in RR as compared with another French cohort, with a predetermined number of patients to include of 52.28 However, comparison with prior studies is limited by the evolution of the perception of BSs in society (influencing the NE) and better scientific hindsight, allowing for a more assured communication by HPs. Finally, we implemented no control on how the predefined vocabulary was respected. This is a limitation but gives better insight into ‘real life’.
In conclusion, a tailored communication strategy focusing on a trustful relationship between patients and nurses and the implication of a multidisciplinary team showed improvement in outcomes after a switch from infliximab to a biosimilar, by reducing the nocebo effect. The intervention we describe may be useful for future switches of other intravenous BDs. The methodology may be used for developing interventions for all BD switches, focusing on the patient’s perceptive.
Acknowledgments
Dr. Margaux Boisson, Service de rhumatologie du Professeur Cahan, Hôpital Cochin, APHP.
REFERENCES
Footnotes
Contributors FB and CB had the idea of the study. CB and MA were responsible for organising the switch and scheduled meeting. CB was in charge of the semi directive patient interviews and reviewing finished article. JP was responsible for the literature research, for collecting data, statistical analysis and writting of the article.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests FB reports personal fees from Boehringer, Bone Therapeutics, Expanscience, Galapagos, Gilead, GSK, Merck Sereno, MSD, Nordic, Novartis, Pfizer, Regulaxis, Roche, Sandoz, Sanofi, Servier, UCB, Peptinov, TRB Chemedica, 4P Pharma, outside the submitted work. CB reports grants from Fresenius Kabi and Mylan outside the submitted work and was and occasional speaker for Abbvie, MSD, Roche, UCB, Mylan, Sanofi. KL declares personal fees from Novartis and Abbvie, outside the submitted work. SD declares occasional work as co-investigators with Abbvie and Janssen, outside the submitted work.
Patient consent for publication Not required.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement Deindentified patient data are available upon request to the corresponding author. Reuse of data is permitted.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.