Article Text

Abstract
Objective Many autoimmune diseases share common pathogenic mechanisms; however, there are limited studies quantifying the coexistence of autoimmune diseases and associated conditions in patients with juvenile idiopathic arthritis (JIA). This large US-based study estimated and compared the prevalence of multiple coexisting autoimmune diseases in patients with JIA with a general paediatric (GP) patient population.
Methods This retrospective cohort study was conducted using registry data from the Cincinnati Children’s Hospital Medical Center (January 2010–October 2018). The prevalence of multiple autoimmune diseases was estimated in patients (age <21 years) with JIA and a control group from the GP patient population. Crude prevalences of 26 prespecified autoimmune diseases and associated conditions were compared using Bayesian Poisson regression modelling for each year up to the end of the study period.
Results Overall, 2026 patients were included in the JIA cohort and 41 572 in the GP cohort. Of 26 autoimmune diseases and associated conditions evaluated, 14 (53.8%) had a significantly higher prevalence in the JIA cohort compared with the GP cohort. In total, seven (26.9%) autoimmune diseases or associated conditions had a >20-fold increased prevalence in the JIA cohort compared with the GP cohort.
Conclusion In this study, patients with JIA had a greater prevalence of a large number of coexisting autoimmune diseases and associated conditions compared with the GP population. Physicians should consider coexisting autoimmune diseases in the treatment and management of patients with JIA.
- autoimmune diseases
- arthritis juvenile
- prevalance
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Key messages
What is already known about this subject?
Many autoimmune diseases share common pathogenic mechanisms, and patients with coexisting autoimmune diseases often experience increased disease severity, disability and mortality. There are, however, limited studies quantifying the coexistence of autoimmune diseases in children and young adults with juvenile idiopathic arthritis (JIA).
What does this study add?
This study estimated the prevalence of 26 coexisting autoimmune diseases and associated conditions in this patient population compared with a general paediatric patient population.
Overall, 14 of the 26 autoimmune diseases and associated conditions studied had a statistically higher prevalence among patients with JIA compared with the general paediatric patient population; 7 (26.9%) had a >20-fold increased prevalence in the JIA cohort compared with the general paediatric cohort.
How might this impact on clinical practice or future developments?
Assessment, management and treatment options for patients with JIA should be considered in the context of the increased frequency of other autoimmune diseases and associated conditions present.
Introduction
Juvenile idiopathic arthritis (JIA) is an autoimmune inflammatory arthritis that develops in children <16 years of age, persists for >6 weeks and is of unknown cause.1 It is the most common paediatric rheumatic disease and can lead to joint damage, chronic pain and disability.2 It has a prevalence in the USA of 44.7 cases per 100 000 children.1 3 Seven subtypes of JIA exist, based on features present in the first 6 months of illness: systemic arthritis, oligoarthritis, rheumatoid factor (RF)-positive polyarthritis, RF-negative polyarthritis, enthesitis-related arthritis, psoriatic arthritis and undifferentiated arthritis.4 5 The cause of JIA remains unknown, but it has been related to both genetic and environmental factors.4 6
The National Institutes of Health estimates that autoimmune diseases are the most prevalent diseases in the USA, affecting up to 23.5 million Americans.7 Many autoimmune diseases share common pathogenic mechanisms.8 The presence of coexisting autoimmune diseases in patients with rheumatoid arthritis (RA) has been noted to lead to increases in disease severity, disability and mortality.9 In addition, coexisting conditions in patients with JIA (including coexisting autoimmune diseases) have been shown to negatively impact quality of life and increase disability and mortality.10 11 Similar results were shown in studies that evaluated the coexistence of other autoimmune diseases in patients with multiple sclerosis and psoriasis.12 13 There are limited published studies quantifying the occurrence of other autoimmune diseases in children and young adults with JIA, the majority of which are case reports or studies with small numbers of patients.11 14–26
The aim of this study was to estimate and compare the prevalence of 26 coexisting autoimmune diseases and other associated conditions in children and young adults with JIA with those of a general paediatric (GP) patient population.
Methods
Study design
This was a retrospective cohort study conducted using electronic medical registry data from the Cincinnati Children’s Hospital Medical Center (CCHMC; Cincinnati, Ohio, USA) from 1 January 2010 to 1 October 2018. CCHMC is a 600-bed paediatric hospital that handles more than 1.3 million patient encounters annually.
Patients
Children and young adults aged <21 years who had at least one clinic visit at CCHMC were included. The JIA cohort consisted of patients who had at least two occurrences of International Classification of Diseases, Ninth or Tenth Revision, Clinical Modification (ICD-9-CM and ICD-10-CM) diagnosis codes for JIA. The JIA diagnosis date was recorded as in the patient encounter or discharge diagnosis date. If multiple dates were present, the earliest one was used. The GP cohort included all children seen at the CCHMC. To confirm a coexisting autoimmune disease or associated condition, the diagnosis code for 1 of the 26 predefined coexisting autoimmune diseases and associated conditions under investigation (online supplemental table S1) was noted. Autoimmune diseases included in the definitions for JIA subtypes (eg, psoriasis, spondyloarthritis), and those that could be misdiagnosed as JIA (eg, systemic lupus erythematosus) or are known complications of JIA (eg, uveitis) were not included in the list of associated autoimmune diseases. In patients with JIA with one of the following conditions, which are commonly present in other rheumatic diseases and may have led to an initial misdiagnosis of JIA, all subsequent visit diagnoses were reviewed for a diagnosis of another rheumatic disease: chronic glomerulonephritis, myositis, pulmonary fibrosis, interstitial lung disease and Sjögren’s syndrome/sicca syndrome. As a result of this more intense review of these diagnoses, one patient diagnosed with JIA was excluded, as the arthritis was determined to be part of the known manifestations of a subsequently diagnosed genetic syndrome. The GP cohort excluded patients with diagnosis codes for JIA. No other exclusion criteria were applied.
Supplemental material
Outcomes
The crude prevalence (reported as X cases per patient-year) of each of the 26 autoimmune diseases and associated conditions were compared in the JIA and the GP cohorts during the last year of the study period.
Statistical analysis
Descriptive statistics were used to analyse baseline demographic information, coexisting conditions and medication use for the patients with JIA.
Bayesian Poisson regression modelling27 was used for estimating and comparing prevalence rates for each of the autoimmune diseases and associated conditions in the JIA and GP cohorts at the end of the study period. The prevalence rates and corresponding 95% confidence limits for the autoimmune diseases in the two cohorts are reported.
The study was conducted in accordance with the International Society for Pharmacoepidemiology guidelines for good pharmacoepidemiology practices,28 applicable regulatory requirements and the principles of the Declaration of Helsinki. This article does not contain any new studies with human or animal subjects performed by any of the authors. The study protocol was reviewed and approved by the Institutional Review Board (IRB) of the Cincinnati Children’s Hospital (IRB #20180346) and a waiver was provided stating that patient informed consent was not required for this study.
Results
Patient disposition and baseline characteristics
Of the children and young adults with at least one clinic visit (n=253 554), a total of 2026 patients with JIA and 41 572 patients with at least one prespecified autoimmune disease or associated condition were identified from January 2010 to October 2018. Of the 2026 patients included in the JIA cohort, 1333 patients were included in this analysis. Reasons for exclusion were: missing diagnosis date (n=163) and ≥21 years of age during the last year (n=678) (patients could have more than one reason for exclusion). Baseline demographic and disease characteristics of patients with JIA included in the study are presented in table 1. In this table is a comparison of patients with JIA with and without an additional autoimmune disease or associated condition; the patients with JIA with an additional autoimmune disease or associated condition were significantly older at JIA onset and diagnosis when compared with those without an additional autoimmune disease or associated condition. Furthermore, patients with JIA with an additional autoimmune disease or associated condition were prescribed significantly more non-biological and biological disease-modifying antirheumatic drugs (DMARDs), corticosteroids and non-steroidal anti-inflammatory drugs, which may indicate more severe disease. In addition, there was a significant difference in the JIA subtypes between the two groups.
Baseline demographics and clinical characteristics of the overall population with JIA, the population with JIA with at least one additional autoimmune disease or associated condition (JIA+) and the population with JIA without an additional autoimmune disease or associated condition (JIA–)
Prevalence of autoimmune diseases and associated conditions
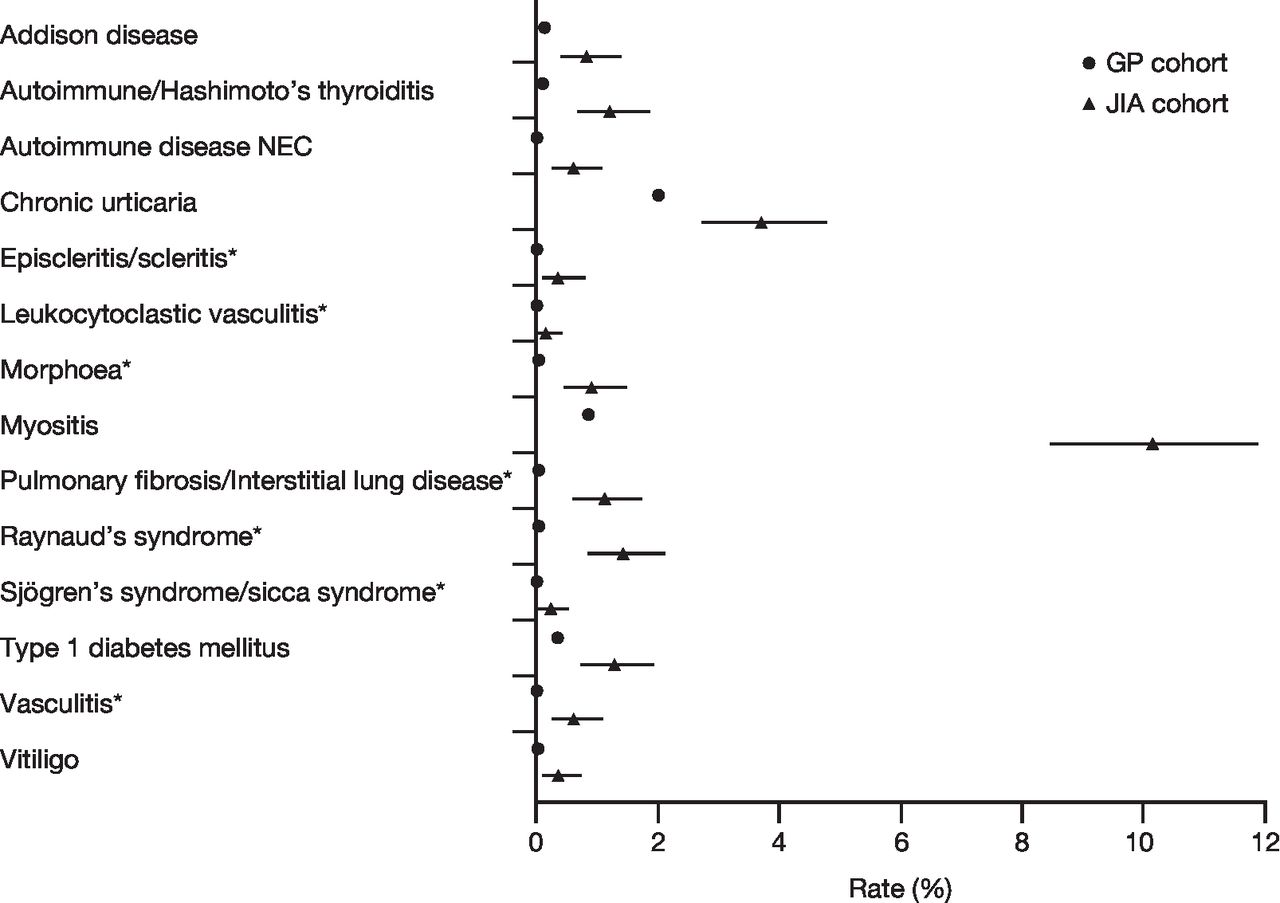
The prevalences (over the last year) of the 26 autoimmune diseases and associated conditions in both cohorts are shown in table 2. Out of 26 evaluated, 14 (53.8%) had a significantly higher prevalence in the JIA cohort compared with the GP cohort (figure 1). These 14 diseases in order of increasing fold difference were: chronic urticaria, type 1 diabetes mellitus, Addison disease, vitiligo, autoimmune/Hashimoto’s thyroiditis, myositis, autoimmune disease not elsewhere classified, morphoea, episcleritis/scleritis, Raynaud’s syndrome, pulmonary fibrosis/interstitial lung disease, vasculitis, Sjögren’s syndrome/sicca syndrome and leukocytoclastic vasculitis. There were seven autoimmune diseases or associated conditions (26.9%) that had a >20-fold increased prevalence in the JIA cohort compared with the GP cohort. These seven diseases in order of increasing fold difference were: morphoea, episcleritis/scleritis, Raynaud’s syndrome, pulmonary fibrosis/interstitial lung disease, vasculitis, leukocytoclastic vasculitis and Sjögren’s syndrome/sicca syndrome.
Prevalence over the last year and relative risk for the entire study duration for all 26 autoimmune diseases and associated conditions investigated in patients with JIA compared with the GP population
{kind=link}
Significant results from Bayesian Poisson analyses on prevalence comparisons: JIA cohort versus GP cohort. Data are prevalence estimates with 95% confidence intervals. *>20-fold increased prevalence in the JIA cohort compared with the GP cohort. GP, general paediatric; JIA, juvenile idiopathic arthritis; NEC, not elsewhere classified.
Overall, 19% of the patients with JIA and 5% of the GP population had at least one autoimmune disease or associated condition. In patients with JIA, 16% had one, 2% had two and <1% had three or more autoimmune diseases or associated conditions. The autoimmune disease and associated conditions according to JIA subcategory are shown in online supplemental table S2.
Discussion
The results from this large US-based study of multiple autoimmune diseases demonstrated that of the 26 autoimmune diseases and associated conditions studied, approximately 54% were significantly more common in children and young adults with JIA compared with the GP patient population.
Currently, there are limited publications quantifying the occurrence of other autoimmune diseases in children and young adults with JIA, and the majority of those published are case reports or studies involving one or a small number of selected autoimmune diseases.11 15–26 Our results are supported by a retrospective review of medical records in an Italian hospital that found that there was a high incidence of new autoimmune diseases in patients (aged 0–21 years; n=79) affected by JIA, with autoimmune thyroid disease being the most common coexisting autoimmune disease.14 Additionally, a longitudinal population‐based study showed that JIA appeared to increase the risks for development of RA, systemic lupus erythematosus, ankylosing spondylitis, psoriatic arthritis and Sjögren’s syndrome in adulthood.29 Furthermore, some studies involving a small number of patients or select autoimmune diseases also support our findings with increases in autoimmune thyroid disorders (n=15115; n=5316; n=66)19 and type 1 diabetes mellitus (n=12 269)23 noted in patients with JIA.
Similar studies have reported an increased risk of coexisting autoimmune conditions in patients with an existing autoimmune condition. A cross-sectional study using a US administrative healthcare claims database found that patients with RA have more coexisting autoimmune diseases than patients with osteoarthritis, suggesting a relationship between RA and other autoimmune diseases.9 Furthermore, a retrospective cohort study that investigated the association between psoriasis and 21 common autoimmune diseases found that patients with psoriasis were more likely to have one or more other autoimmune diseases compared with the general population, with the strongest association being with RA.12 In patients with multiple sclerosis, a systematic review and meta-analysis of the incidence of autoimmune disease found that the most prevalent autoimmune conditions were psoriasis (7.74%) and thyroid disease (6.44%).13 In addition, a study investigating the association between myasthenia gravis and coexisting autoimmune disease found that 24% of patients with myasthenia gravis had a coexisting autoimmune disease; of these, autoimmune thyroid disease was the most common (16%).30
The genetic basis of autoimmune diseases, including involvement of common genes, may explain the clustering of certain autoimmune diseases.31 A genome-wide association study showed that patients with paediatric autoimmune disease had higher heritability estimates than those with non-immune-mediated disease (paediatric-onset epilepsy), and that of the paediatric autoimmune diseases, JIA was one of the most highly heritable.31 A registry study also found that higher proportions of patients with JIA versus other autoimmune diseases had first-degree relatives with any autoimmune disease.32 A study conducted in Italy found that ~50% of patients with JIA had at least one relative with an autoimmune disease and that there was a high incidence risk of new autoimmune diseases in patients with JIA; however, the study was not able to predict which patients would develop autoimmune diseases, what disease would occur and at what time the disease would develop.14
The current study has some limitations. First, as seen in studies using electronic health record data, the patient population is dynamic. In this analysis, we assumed that patients only departed the database due to transition into adult care, but they may have also departed as they were no longer being cared for at CCHMC. Although the GP population was recruited from the same socioeconomic groups and geographical location as the JIA cohort, this is a single-centre study and findings may not be generalisable to other ethnic populations and geographical locations, as the risk for developing an autoimmune disease is known to be influenced by both genetic and environmental factors.4 6 Autoimmune diseases are characterised by heterogeneous clinical presentations, and sometimes complex definitions and multiple ICD-9-CM diagnosis codes; as such, classification bias may exist. Potential differences in the severity of the autoimmune disorders were not evaluable on the basis of the information captured in the registry evaluated in this study. Also, some of the diseases listed, such as myositis, can have aetiologies other than autoimmune, and this study did not include only those thought to be autoimmune in origin.
Children and young adults with JIA have a more pronounced prevalence for a large number of other autoimmune diseases and associated conditions compared with the GP population. Physicians should consider the presence of other potential autoimmune diseases in the initial work-up and ongoing evaluation of patients with JIA. In addition, the design and analyses of future studies investigating the development of additional autoimmune diseases and associated conditions following treatment in patients with JIA should incorporate the inherent increased risk of other autoimmune diseases in this population. This inherent increased risk for other autoimmune diseases in patients with JIA also complicates the assessment of the risk for certain treatments to induce one of these autoimmune diseases as a complication of treatment. Certainly in this study, patients with an additional autoimmune disease or associated condition were significantly more commonly treated with non-biological and biological DMARDs.
Acknowledgments
Professional medical writing and editorial assistance was provided by Claire Line, PhD, at Caudex and was funded by Bristol Myers Squibb.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Contributors DJL, BH, CC, STA-H, TAS and HIB were involved in study conception and design. DJL, BH, CC, STA-H and HIB were involved in acquisition of data. DJL, BH, CC, STA-H, TAS and HIB were involved in the analysis and interpretation of data. All authors were involved in drafting the article or revising it critically for important intellectual content, and all authors approved the final version to be submitted for publication. All authors had full access to all of the data in the study and take responsibility for the integrity of the data and the accuracy of the data analysis.
Funding This study was funded by Bristol Myers Squibb.
Competing interests DJL’s institution, Cincinnati Children’s Hospital Medical Center, has received consulting fees and/or honoraria for the work of DJL from Abbott, Amgen, AstraZeneca, Boehringer Ingelheim, Celgene, F. Hoffmann-La Roche, GlaxoSmithKline, Novartis, Pfizer, Takeda, UBC and Wyeth Pharma. DJL has served on speakers’ bureaus for Bristol Myers Squibb and Genentech and has served on data and safety monitoring boards for Forest Research and the NIH-NIAMS (<$10 000). TAS was an employee and shareholder of Bristol Myers Squibb at the time of the analysis (a former employee at present). HIB received grant/research support from Bristol Myers Squibb and Pfizer (>$10 000); served as a consultant for Bristol Myers Squibb, GlaxoSmithKline, Janssen, Lilly, Novartis, Pfizer, Roche and Sanofi; and served on speakers’ bureaus for Novartis and Roche (both >$10 000).
Patient consent for publication Not required.
Ethics approval The study was conducted in accordance with the International Society for Pharmacoepidemiology guidelines for good pharmacoepidemiology practices, applicable regulatory requirements and the principles of the Declaration of Helsinki. This article does not contain any new studies with human or animal subjects performed by any of the authors. The study protocol was reviewed and approved by the Institutional Review Board (IRB) of the Cincinnati Children’s Hospital (IRB #2018-0346) and a waiver was provided stating that patient informed consent was not required for this study.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement Data are available upon reasonable request. Bristol Myers Squibb policy on data sharing may be found at https://www.bms.com/researchers-and-partners/independent-research/data-sharing-request-process.html.