Article Text

Abstract
Objectives We examined patient-reported outcomes (PROs) in The Study of Etanercept And Methotrexate in Patients with Psoriatic Arthritis (PsA); a 48-week, phase 3, randomised controlled trial that compared outcomes with methotrexate (MTX) monotherapy, etanercept monotherapy, and MTX+ etanercept in patients with PsA.
Methods Efficacy endpoints included: mean changes from baseline and proportion of patients who reported improvements≥minimal clinically important difference (MCID) at week 24 in treatment groups for Health Assessment Questionnaire-Disability Index, Patient Global Assessment (PtGA), Patient Global Assessment of Joint Pain (PtGAJP) and Medical Outcomes Study Short Form-36 Questionnaire (SF-36) Physical Component Summary (PCS), and Mental Component Summary, and eight domain scores. PROs were analysed as reported (observed), without multiplicity adjustment; therefore, p values are descriptive.
Results At week 24, patients receiving etanercept monotherapy or MTX+ etanercept combination reported greater improvements (p≤0.05) in PtGA, PtGAJP and SF-36 PCS scores compared with those receiving MTX monotherapy. Compared with MTX monotherapy, higher proportions of patients receiving etanercept monotherapy and combination therapy reported improvements≥MCID in PtGA (etanercept vs MTX, p=0.005) and PtGAJP (MTX +etanercept vs MTX, p=0.038). Across PROs, proportions of patients reporting scores≥age and gender-matched normative values at week 24 ranged from 20.8% to 51.0% with MTX monotherapy, 30.9% to 48.8% with etanercept monotherapy, and 30.6% to 52.3% with MTX+ etanercept combination.
Conclusions Patients receiving etanercept monotherapy or MTX+ etanercept reported greater improvements from baseline in several PROs compared with those receiving MTX monotherapy. PROs should be incorporated in discussions between patients and clinicians regarding their treatment choices as they can help determine which treatments are more beneficial in patients with PsA.
- etanercept
- methotrexate
- patient reported outcome measures
- arthritis
- psoriatic
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Key messages
What is already known about this subject?
Patients with psoriatic arthritis (PsA) have lower health-related quality of life compared with the general population, as measured by patient-reported outcomes (PROs). PROs can improve with commonly used treatments for PsA, such as methotrexate (MTX) and tumour necrosis factor inhibitors.
However, few studies exist that have directly compared the therapeutic effect of MTX with a tumour necrosis factor inhibitor on PROs in patients with PsA.
What does this study add?
This study analyzes PRO data captured in a phase 3, randomised controlled trial that directly compared the effect of MTX monotherapy versus etanercept (a tumour necrosis factor inhibitor) monotherapy or MTX plus etanercept combination therapy in patients with PsA who were treatment naïve.
Etanercept monotherapy and combination therapy were more effective than MTX monotherapy for improvement in PROs (and, in many cases, clinically meaningful outcomes were reported) in patients with PsA.
How might this impact on clinical practice?
Improvements in PROs with etanercept may inform decision-making between clinicians and patients with PsA.
Introduction
Psoriatic arthritis (PsA) is a progressive, chronic inflammatory disease with both joint and skin-related manifestations. Patients with PsA can experience a multitude of symptoms including peripheral and axial joint inflammation, enthesis inflammation (enthesitis; inflammation of the areas where tendons or ligaments attach to bones), finger or toe inflammation (dactylitis), nail disease and psoriasis.1 In patients with psoriasis, about 30% develop PsA with an annual incidence of 1%–3%.2–5 Effective disease management requires not only timely diagnosis and treatment but also recognition that PsA can adversely affect patient-reported outcomes (PROs). Previous research suggests that, in general, patients with PsA report worse PRO scores compared with either the general population or patients with psoriasis.6–9 PsA is associated with considerable disease burden including bodily pain and physical function below that of age-matched and gender-matched norms,10 fatigue, increased absenteeism from work, and decreased work productivity.11–14 When assessing the overall clinical value of PsA treatments, PRO measures should be included since health-related quality of life (HRQoL), physical function and global assessments are affected by treatment efficacy, safety, tolerability, dosing frequency and route of administration. Disease-modifying antirheumatic drugs (DMARDs) used to treat PsA such as methotrexate (MTX) and tumour necrosis factor inhibitors (TNFis) can improve PROs related to physical ability, joint pain and mental ability in patients with PsA.9 15 Although MTX, as a monotherapy or in a combination regimen, is widely used to treat PsA, the evidence supporting its use in this disease setting is limited. Further, few randomised controlled trials (RCTs) in PsA have examined PROs when directly comparing MTX with a TNFi or in combination with a TNFi. These include a study that compared MTX monotherapy versus placebo in patients with psoriasis16 and a study that compared MTX monotherapy versus golimumab and MTX combination therapy in patients with early PsA.17
The Study of Etanercept And Methotrexate in Combination or as Monotherapy in Subjects with Psoriatic Arthritis (SEAM-PsA)18 reported that both etanercept monotherapy and combination therapy were statistically significantly more effective than MTX monotherapy by the percentage of patients who were American College of Rheumatology 20% responders (ACR20, primary endpoint) and had Minimal Disease Activity (MDA) (key secondary endpoint) at week 24. Week-48 safety outcomes indicated that no deaths occurred in the study and that the incidences of adverse events and serious adverse events were similar across the three treatment groups.18 Published PRO results with the Health Assessment Questionnaire-Disability Index (HAQ-DI) and the Medical Outcomes Study Short Form-36 Questionnaire (SF-36) showed similar improvements in HAQ-DI and Mental Component Summary (MCS) scores from baseline to week 24 in all three treatment groups.18 However, the SF-36 Physical Component Summary (PCS) score showed greater mean changes from baseline at week 24 in both etanercept groups compared with MTX monotherapy.
Here, we report additional PRO measures from the SEAM-PsA RCT examining the effect of MTX monotherapy, etanercept monotherapy, and MTX plus etanercept combination therapy on PROs that evaluated HRQoL, physical function and global assessments of disease activity, including: HAQ-DI, Patient Global Assessment of disease activity (PtGA), Patient Global Assessment of Joint Pain (PtGAJP) and SF-36 summary and domain scores. By evaluating changes across the 3 groups at week 24 and comparing scores to age-matched and gender-matched normative values (based on the general population without chronic disease), we aimed to examine improvements in PROs.
Methods
Study design and patient population
SEAM-PsA was a 48-week, phase 3, multicentre, international RCT conducted at 124 hospitals/centres/clinics in 17 countries (ClinicalTrials.gov, NCT02376790). Key patient eligibility criteria included age ≥18 years old at screening, active PsA (based on Classification Criteria for Psoriatic Arthritis),19 naïve to etanercept and other biologic agents, no prior use of MTX for PsA (prior treatment with MTX for psoriasis was allowed), ≥3 tender and ≥3 swollen joints (68/66 tender/swollen joint count) at screening and baseline, and an active psoriatic skin lesion ≥2 cm in diameter. Patients were randomised 1:1:1 via an interactive voice-response system to receive: (1) oral MTX (target 20 mg/week) plus subcutaneous placebo weekly, (2) etanercept 50 mg/week given subcutaneously plus oral placebo weekly, or (3) etanercept at 50 mg/week given subcutaneously plus oral MTX weekly (target 20 mg/week). Patients with an inadequate response at or after week 24 (<20% improvement in tender and swollen joint counts from baseline), received rescue therapy with etanercept (50 mg/week) plus MTX (target 20 mg/week) until week 48.
All PROs were evaluated at baseline and weeks 12, 24, 36 and 48. At each visit, PROs were completed before administration of study medication and other study procedures.
The SEAM-PsA trial was conducted in accordance with the Declaration of Helsinki. Written informed consent was obtained from each patient, and each participating site obtained protocol approval by an institutional review board or independent ethics committee. Additional details about the design and eligibility criteria of SEAM-PsA have been previously published.18 20
Outcomes
The primary endpoint of the SEAM-PsA trial was the percentage of ACR20 responders at week 24, and the key secondary endpoint was the percentage of patients with MDA at week 24. These results have been previously published.18
Additional study endpoints included the change in PRO scores from baseline at week 24 in each treatment group by HAQ-DI, PtGA, PtGAJP, SF-36 PCS, MCS and eight individual domains: Physical Function, Role Physical, Bodily Pain, General Health, Vitality, Social Function, Role Emotional, and Mental Health. Exploratory analyses examined the proportion of patients in each treatment group who reported improvements from baseline at week 24≥minimal clinically important differences (MCID; which is the degree of change that is perceptible and clinically meaningful to patients21) in HAQ-DI, PtGA, PtGAJP and SF-36 PCS, MCS and the domains.22–25 We also examined the proportion of patients in each treatment group who reported scores at week 24≥age-matched and gender-matched normative values in HAQ-DI and SF-36 PCS, MCS and domain scores.26 There are no normative values defined for PtGA and PtGAJP.
Statistical analyses
SEAM-PsA was not powered to detect differences between PROs. As such, p values for efficacy endpoints other than the primary and key secondary endpoints were not adjusted for multiplicity and should be considered descriptive. All treatment comparisons were performed using the Cochran-Mantel-Haenszel test with prior use of non-biological DMARDS (non-bDMARDS) and a baseline body mass index (BMI) status (≤30 kg/m2 or >30 kg/m2) as stratification factors. An analysis of covariance (ANCOVA) model that adjusted for baseline BMI status and prior non-bDMARD use compared the treatment differences between the MTX monotherapy group versus the two etanercept-containing groups for changes in PRO scores at week 24 from baseline. Statistical analyses were performed using SAS V.9.4 (SAS Institute).
Results
Patient characteristics
A total of 851 patients completed the study. Baseline demographic and disease characteristics were well balanced across the three treatment groups (table 1). Most patients were Caucasian (90.7%), and mean (SD) age was 48.4 (13.1) years. Most patients were early in the course of their disease, with the mean (SD) duration of PsA of 3.2 (6.3) years (median 0.6 years). Prior MTX for the treatment of psoriasis was received by 4.9% of patients. From weeks 4 to 24, patients in the MTX groups continued a mean MTX dose that was >18.8 mg (median 20 mg).
Demographics and baseline disease activity
Change in PRO scores
An examination of changes in PRO scores from baseline to week 24 indicated that improvements generally occurred across all three treatment groups. For most SF-36 domains, changes from baseline at week 24 were numerically higher in the etanercept groups compared with MTX monotherapy (table 2).
Change in patient-reported outcome scores from baseline at week 24
Treatment differences between MTX monotherapy versus the two etanercept groups by changes in PRO scores at week 24 after adjusting for baseline BMI status and prior non-bDMARD use are shown in table 2. Patients receiving etanercept monotherapy reported greater improvements from baseline in PtGA (p<0.001), PtGAJP (p=0.032), SF-36 PCS (p=0.033) and the domains of Bodily Pain (p=0.034) and General Health (p=0.01) compared with MTX monotherapy. Patients receiving combination therapy reported greater improvements from baseline in PtGA (p=0.012), PtGAJP (p=0.014), SF-36 PCS (p=0.015), Bodily Pain (p=0.007), and Vitality (p=0.05) domains compared with MTX monotherapy.
We generated a spydergram (figure 1) to illustrate how mean baseline and week 24 SF-36 domain scores across treatment groups compared against USA age-matched and gender-matched normative scores matched to the protocol population.27 Published normative values are: HAQ-DI: ≤0.25, SF-36 PCS and MCS: ≥50, and domain scores listed in the figure legend, with missing values not imputed. Figure 1 illustrates how the largest differences between MTX monotherapy and etanercept treatment groups were reported in Bodily Pain, General Health, and Vitality Domains.
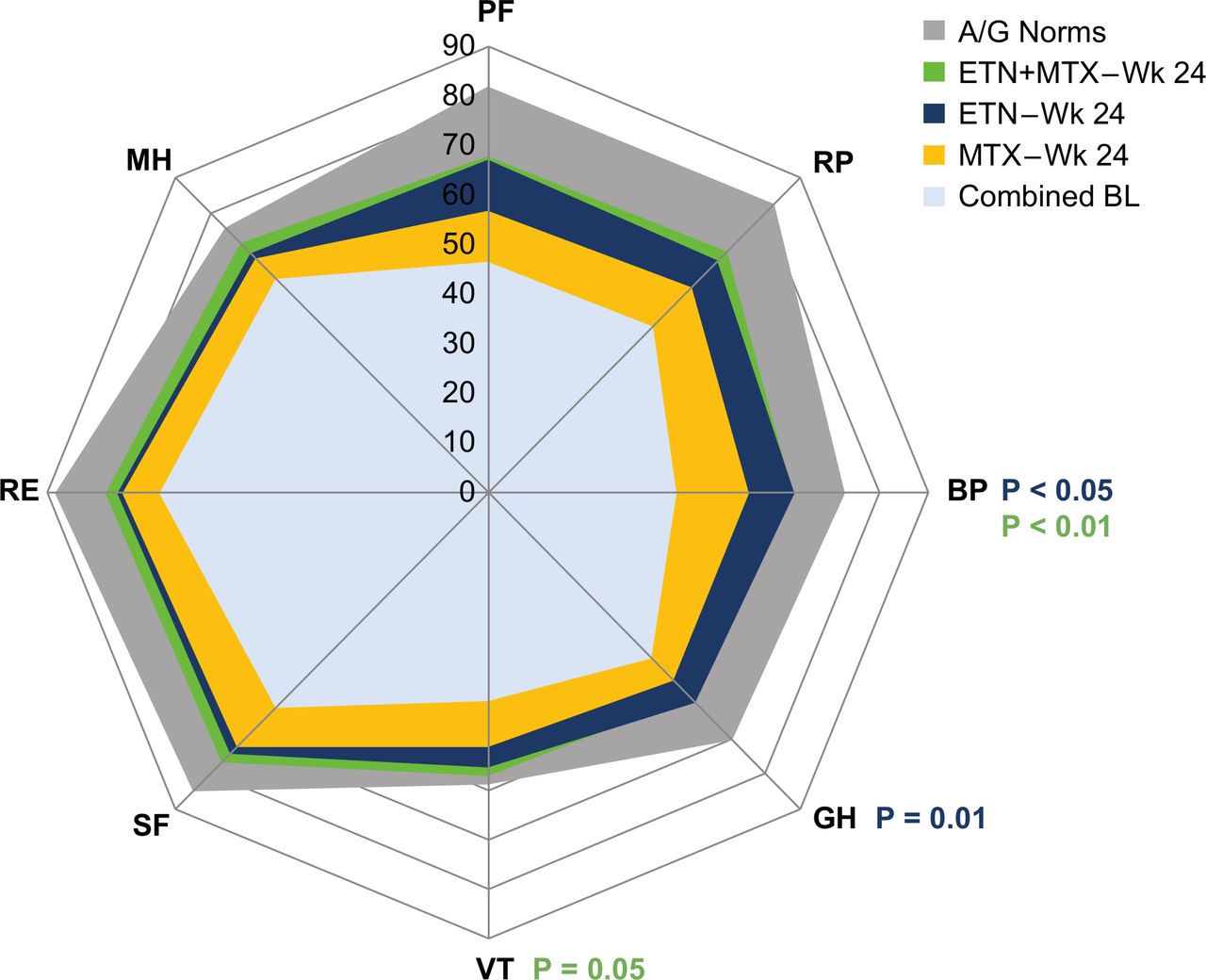
Spydergram of domain scores from baseline to week 24 versus age-matched and gender-matched normative scores. The spydergram was generated using domain raw scores (range: 0–100); age-gender norms in the USA were matched to the study population. The age-matched and gender-matched normative values for the SF-36 domains were: 82.01 for PF, 82.55 for RP, 72.86 for BP, 70.31 for GH, 58.89 for VT, 85.11 for SF, 88.12 for RE and 75.94 for MH. Missing values were not imputed. A higher SF-36 score indicates a more positive health state, so greater positive changes from baseline. P values in red indicate p≤0.05; p values in blue indicate p≤0.01. A, age; BL, baseline; BP, Bodily Pain; ETN, etanercept; G, gender; GH, General Health; MH, Mental Health; MTX, methotrexate; PF, Physical Function; RE, Role Emotional; RP, Role Physical; SF, Social Function; VT, Vitality; Wk, week.
Threshold analyses
Patients reporting improvements in PRO scores at week 24 ≥ MCID
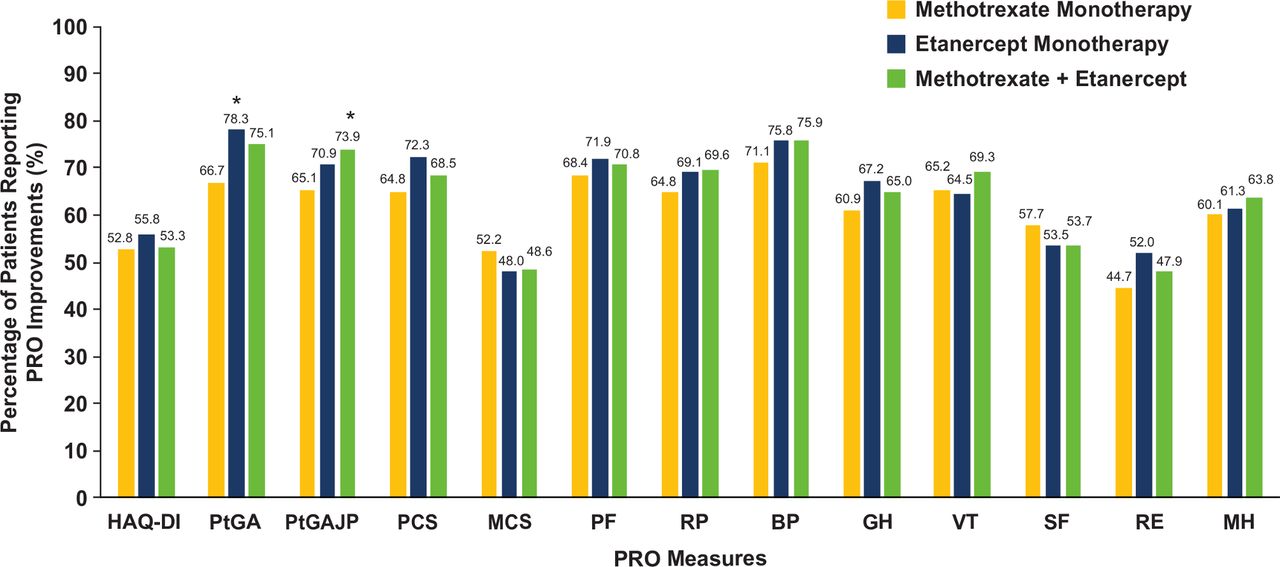
We examined the percentage of patients in each treatment group who reported changes in PRO scores at week 24≥MCID in HAQ-DI, PtGA, PtGAJP and SF-36 PCS, MCS and domains. The etanercept monotherapy and combination therapy groups generally included a higher percentage of patients reporting clinically meaningful changes in PRO scores at week 24 (figure 2) compared with MTX monotherapy. The highest percentages of clinically meaningful improvements were reported in PtGA (66.7% with MTX monotherapy vs 78.3% with etanercept monotherapy, and 75.1% with combination therapy). Analyses comparing across treatment groups generally showed similar proportions of patients reporting changes≥MCID at week 24. Exceptions were higher percentages in both etanercept groups in PtGA (66.7% with MTX monotherapy vs 78.3% with etanercept monotherapy; p=0.005) and PtGAJP (65.1% with MTX monotherapy vs 73.9% with combination therapy; p=0.038; figure 2).
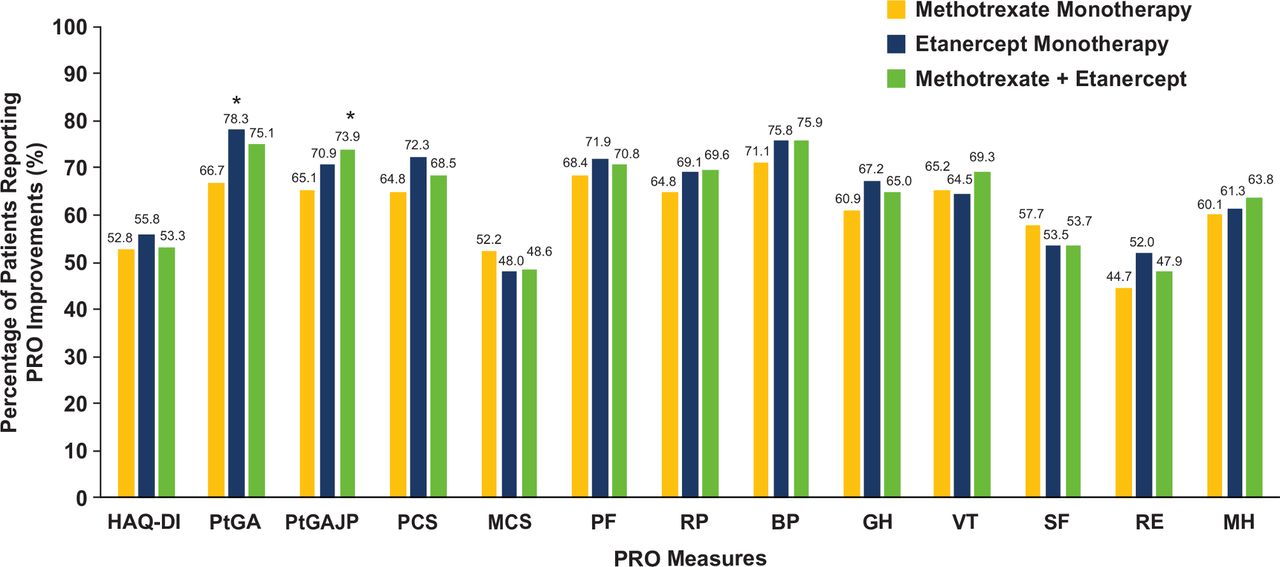
Percentages of patients reporting PRO improvements≥MCID week 24. *P values are descriptive and are for comparison with methotrexate monotherapy. Only p values ≤0.05 are shown. MCID values were change from baseline ≤ –0.35 for HAQ-DI, ≤ –10.0 for PtGA, ≤ –10.0 for PtGAJP, ≥2.5 for SF-36 PCS, ≥2.5 for SF-36 MCS, and ≥5.0 for each SF-36 domain. BP, Bodily Pain; GH, General Health; HAQ-DI, Health Assessment Questionnaire-Disability Index; MCID, minimal clinically important difference; MCS, Mental Component Summary; MH, Mental Health; PCS, Physical Component Summary; PF, Physical Function; PRO, patient-reported outcome; PtGA, Patient Global Assessment; PtGAJP, Patient Global Assessment of Joint Pain; RE, Role Emotional; RP, Role Physical; SF, Social Function; SF-36, Medical Outcomes Study Short Form-36 Questionnaire; VT, vitality.
Patients reporting PRO scores ≥ age-matched and gender-matched normative values at week 24
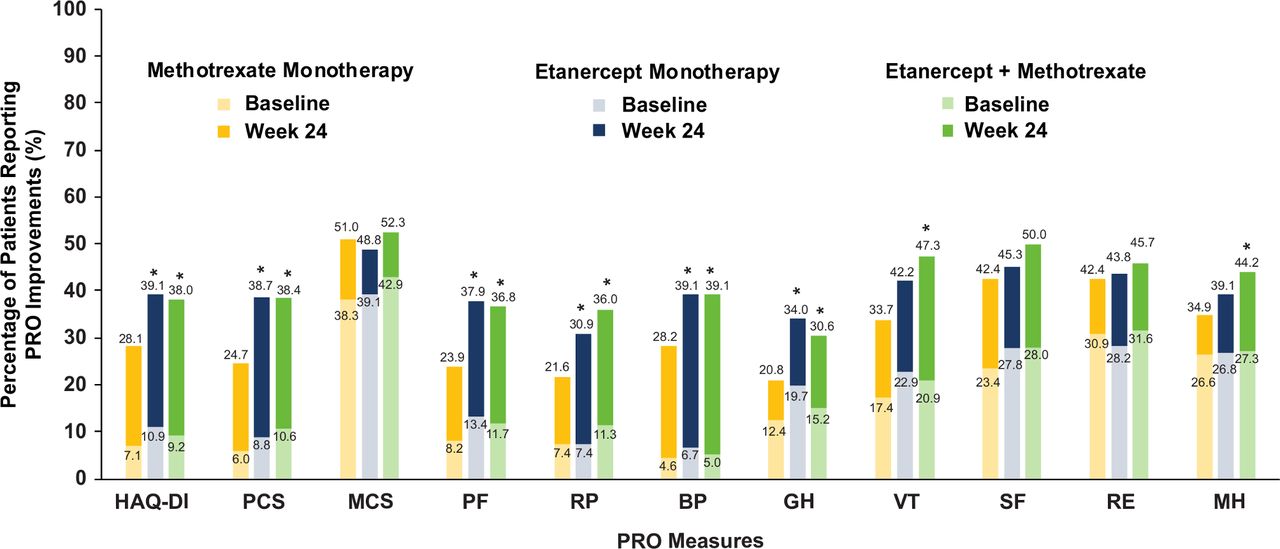
Across PROs, the percentages of patients reporting scores at week 24≥normative values ranged from 20.8% (General Health domain) to 51.0% (SF-36 MCS) with MTX monotherapy, 30.9% (Role Physical domain) to 48.8% (SF-36 MCS) with etanercept monotherapy, and 30.6% (General Health domain) to 52.3% (SF-36 MCS) with combination therapy (figure 3). Higher percentages of patients in both etanercept groups reported scores at week 24≥normative values (p≤0.05) in HAQ-DI, SF-36 PCS, and Role Physical, Bodily Pain, and General Health domains. Numerically, more patients receiving combination therapy reported scores at week 24≥normative values in Vitality and Mental Health domains compared with MTX monotherapy (p≤0.05; figure 3).
{kind=link}
{kind=link}
{kind=link}
Percentages of patients reporting PRO scores ≥normative values at week 24. *P values are descriptive and are for comparison with methotrexate monotherapy at week 24. Only P values ≤0.05 are shown. Normative values were ≤0.25 for HAQ-DI; ≥50 for SF-36 PCS, and ≥50 for SF-36 MCS. Age/gender normalised values for the SF-36 domains were 82.01 for PF, 82.55 for RP, 72.86 for BP, 70.31 for GH, 58.89 for VT, 85.11 for SF, 88.12 for RE, and 75.94 for MH. BP, Bodily Pain, GH, General Health; HAQ-DI, Health Assessment Questionnaire-Disability Index; MCS, Mental Component Summary; MH, Mental Health; PCS, Physical Component Summary; PF, Physical Function; PRO, patient-reported outcome; RE, Role Emotional; RP, Role Physical; SF, Social Function; SF-36, Medical Outcomes Study Short Form-36 Questionnaire; VT, Vitality.
Discussion
Our analyses of the PRO data collected from the SEAM-PsA RCT indicate that patients receiving MTX monotherapy, etanercept monotherapy and MTX plus etanercept all reported improvements in PRO scores at week 24 compared with baseline. Both the etanercept monotherapy and MTX plus etanercept groups reported greater improvements from baseline compared with MTX in PtGA, PtGAJP, SF-36 PCS and Bodily Pain domain. Additionally, the etanercept monotherapy group reported greater improvement in General Health and the combination therapy group greater improvement in Vitality compared with MTX monotherapy. Improvements in PROs reported with etanercept monotherapy and MTX plus etanercept were numerically similar, although this was not statistically evaluated as the trial was not powered for statistical comparison between these two groups.
Reported results indicated that treating patients with PsA with etanercept either monotherapy or in combination with MTX results in greater, more clinically meaningful improvements in PROs compared with MTX monotherapy. Results from the primary and secondary endpoints of SEAM-PsA, for which the RCT analyses were powered, indicate that etanercept monotherapy and combination therapy were statistically significantly more effective than MTX monotherapy by ACR20 responses and MDA at week 24.18 PRO results from these analyses most closely aligned with ACR responses and MDA at week 24 are those examining changes from baseline at week 24 in PtGA, PtGAJP, SF-36 PCS, and General Health domain. These PROs may be most sensitive for capturing how patients with PsA experience their disease.
The internal validity of our study’s results is strengthened due to SEAM-PsA being an active-comparator RCT that directly compared PROs in patients treated with MTX, etanercept and combination therapy. In addition, the active comparator included patients receiving MTX at currently recommended doses (~20 mg/week).28
Results from our study are different from those observed in a phase 3 trial of golimumab in combination with MTX versus MTX monotherapy,17 in which golimumab did not show significant improvements in physical PCS at week 22 (SF-36 PCS score of 50.1 vs 50.7; p=0.543). In our study, etanercept monotherapy or in combination with MTX showed significant improvements in PCS scores at week 24 vs MTX monotherapy (least squares mean change from baseline in SF-36 PCS score of 7.38 and 7.62, respectively, vs 5.68; p≤0.05) for both comparisons. However, similar to observations in our study, the golimumab trial did not find any significant improvements in MCS scores.17
This study has a few limitations. There was no placebo group in the trial. This is important because including a placebo arm could help contextualise the results of this trial with prior RCTs in PsA. It is well known that active comparator trials, without placebo, result in higher responses as all patients have higher ‘expectation bias’, knowing that they are all receiving active treatment.29 30 However, there are ethical issues regarding prolonged placebo exposure in patients with active, especially early disease. Another limitation is that the SEAM-PsA trial was not powered to detect differences between etanercept groups and thus they could not be compared. The most important limitation was the generalisability of our results, as the treatment-naïve population enrolled in this RCT may not reflect the experiences of typical patients with severe or moderate PsA. However, our results are likely most relevant to patients with relatively early, active PsA disease.
Future research in PsA should include active comparators and PROs in their design. In addition, direct comparisons between different treatments could help determine which treatments are more effective in patients with PsA. Considering results from this RCT, PROs should be incorporated in discussions between patients and clinicians regarding their choice of treatment, to incorporate the patient’s perspective. Improvements in PROs reported with etanercept may inform decision-making between clinicians and patients with PsA.
References
Footnotes
Twitter @ervant
Presented at Some of the results described here were previously presented in a poster presentation at the 2019 American College of Rheumatology Annual meeting.
Contributors All authors contributed to the development, analysis, and interpretation of the data.
Funding Linda Rice, PhD at Amgen Inc. and Martha Mutomba on behalf of Amgen Inc. provided medical writing support during the development of this manuscript.
Competing interests VS reports receiving consulting fees from AbbVie, Amgen, Arena, AstraZeneca, Bayer, Bioventus, Bristol Myers Squibb, Boehringer Ingelheim, Celltrion, Corrona, Crescendo/Myriad, EMD Serono, Equillium, Flexion, Genentech/Roche, Glenmark, GSK, Horizon, Inmedix, Janssen, Kypha, Eli Lilly, Merck, Novartis, Pfizer, Regeneron, Samsung, Samumed, Sandoz, Sanofi, Servier, Setpoint, TwoXAR, and UCB. PJM reports receiving grants from AbbVie, Amgen, Boehringer Ingelheim, Bristol Myers Squibb, Celgene, Galapagos, Genentech, Gilead, Janssen, Lilly, Novartis, Pfizer, and UCB; consulting fees from AbbVie, Amgen, Boehringer Ingelheim, Bristol Myers Squibb, Celgene, Galapagos, Gilead, GlaxoSmithKline, Janssen, Eli Lilly, Novartis, Pfizer, Sun, and UCB; speaker fees from AbbVie, Amgen, Bristol Myers Squibb, Celgene, Genentech, Janssen, Eli Lilly, Novartis, Pfizer, and UCB. EM, BS, LL, DC, and GK are employees of Amgen and own stock/stock options in Amgen. JFM reports receiving consulting/investigator fees/honoraria from Merck, AbbVie, Dermavant, Eli Lilly, Novartis, Janssen, UCB, Celgene, Sanofi, Regeneron, Arena, Sun Pharma, Biogen, Pfizer, EMD Sorono, Avotres, Leo Pharma, and Cara Therapeutics.
Patient consent for publication Not required.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement Data are available upon reasonable request. Qualified researchers may request data from Amgen clinical studies. Complete details are available at the following: http://www.amgen.com/datasharing.