Article Text

Abstract
Objectives To summarise, by a systematic literature review (SLR), the evidence regarding pharmacological and non-pharmacological therapeutic strategies in difficult-to-treat rheumatoid arthritis (D2T RA), informing the EULAR recommendations for the management of D2T RA.
Methods PubMed, Embase and Cochrane databases were searched up to December 2019. Relevant papers were selected and appraised.
Results Two hundred seven (207) papers studied therapeutic strategies. Limited evidence was found on effective and safe disease-modifying antirheumatic drugs (DMARDs) in patients with comorbidities and other contraindications that limit DMARD options (patients with obesity, hepatitis B and C, risk of venous thromboembolisms, pregnancy and lactation). In patients who previously failed biological (b-)DMARDs, all currently used b/targeted synthetic (ts-)DMARDs were found to be more effective than placebo. In patients who previously failed a tumour necrosis factor inhibitor (TNFi), there was a tendency of non-TNFi bDMARDs to be more effective than TNFis. Generally, effectiveness decreased in patients who previously failed a higher number of bDMARDs. Additionally, exercise, psychological, educational and self-management interventions were found to improve non-inflammatory complaints (mainly functional disability, pain, fatigue), education to improve goal setting, and self-management programmes, educational and psychological interventions to improve self-management.
The identified evidence had several limitations: (1) no studies were found in patients with D2T RA specifically, (2) heterogeneous outcome criteria were used and (3) most studies had a moderate or high risk of bias.
Conclusions This SLR underscores the scarcity of high-quality evidence on the pharmacological and non-pharmacological treatment of patients with D2T RA. Effectiveness of b/tsDMARDs decreased in RA patients who had failed a higher number of bDMARDs and a subsequent b/tsDMARD of a previously not targeted mechanism of action was somewhat more effective. Additionally, a beneficial effect of non-pharmacological interventions was found for improvement of non-inflammatory complaints, goal setting and self-management.
- arthritis
- rheumatoid
- therapeutics
- biological therapy
- occupational therapy
- patient reported outcome measures
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
- arthritis
- rheumatoid
- therapeutics
- biological therapy
- occupational therapy
- patient reported outcome measures
Key messages
This systematic literature review, conducted to inform the Task Force on the EULAR recommendations for the management of difficult-to-treat rheumatoid arthritis (D2T RA), provides an extensive overview of the current literature regarding pharmacological and non-pharmacological therapeutic strategies in D2T RA.
The identified evidence had several limitations: (1) the evidence is indirect as the study population could not be considered as having D2T RA, (2) heterogeneous outcome criteria were used and (3) most studies had a moderate or high risk of bias.
Several biological/targeted synthetic disease-modifying antirheumatic drugs (b/tsDMARDs) were found to be effective in RA patients who failed ≥2 bDMARDs, although generally effectiveness decreased with a higher number of previously failed bDMARDs.
A subsequent b/tsDMARD of a previously not targeted mechanism of action was somewhat more effective in patients who failed ≥1 bDMARD.
Non-pharmacological interventions, especially education, were found to have an additional beneficial effect for improvement of non-inflammatory complaints, goal setting and self-management.
Introduction
Therapeutic strategies for patients with rheumatoid arthritis (RA) have significantly improved over the past decades. However, there is still a substantial proportion of patients that remains symptomatic, even though they have been treated according to the current EULAR recommendations and/or American College of Rheumatology (ACR) guideline for the management of RA.1 2 This patient group is referred to as having ‘difficult-to-treat (D2T) RA’. This disease state is estimated to affect 5% to 20% of all RA patients, depending on the specific definition used.3–5 D2T RA has recently been defined as failure of at least two biological or targeted synthetic disease-modifying antirheumatic drugs (b/tsDMARDs) with different mechanisms of action (MOA), in patients who are still having complaints which may be indicative of active disease and which is perceived as problematic by patient and/or rheumatologist.6 An international survey that was conducted among rheumatologists showed the unmet need for this patient population.7 Consequently, the importance has been acknowledged by EULAR with the approval of a Task Force in charge of the development of management recommendations for D2T RA.
D2T RA is a highly heterogeneous disease state.4 Patients could be symptomatic due to inflammatory activity: for example, refractory disease (having underlying immunologic disease mechanisms driving multidrug-resistant or ‘true’ refractory disease), having active disease because they cannot be adequately treated (ie, having limited drug options because of contraindications, such as comorbidities and/or (risk of) adverse events) or having persistent inflammatory activity due to non-adherence. In addition, patients could be symptomatic due to non-inflammatory factors, for example, concomitant osteoarthritis and fibromyalgia.3 4 8 9 One of the abovementioned factors could be present, although inflammatory activity and non-inflammatory complaints frequently seem to coexist in daily practice.9
Furthermore, in patients with D2T RA, a mismatch in goal setting between patients and healthcare professionals, as well as suboptimal self-management, could negatively impact treatment outcomes and illness perception.10 Patients’ management goals could be unrealistic, for example, aiming to return to all normal activities of daily living, while this is not always achievable because of, for instance, the presence of joint damage. To be able to align treatment goals and to optimise self-management, it will be important to identify mismatches in treatment goals and suboptimal self-management to achieve the most optimal effect from available therapeutic strategies.
Currently, RA management recommendations endorse to switch to another b/tsDMARD in symptomatic patients who failed at least one previous b/tsDMARD and could possibly classify as having D2T RA.1 This therapeutic strategy leads to a trial-and-error approach in patients with D2T RA, as the origin of complaints remains unclear.4 Furthermore, prioritisation of b/tsDMARDs and non-pharmacological interventions are lacking in the current recommendations. Additionally, no recommendations are currently available for RA patients with limited drug options because of contraindications, those with predominantly non-inflammatory complaints (eg, pain, fatigue, reduced function and quality of life), suboptimal self-management, and for those in whom treatment goals are unclear or do not match with the healthcare professional.
Before switching to yet another DMARD, thorough evaluation of the origin of the complaints is needed to be able to choose the most appropriate treatment option. It will be needed to ascertain the diagnosis of RA and to evaluate alternative or coexisting mimicking diseases. Furthermore, it will be important to assess the presence or absence of inflammatory activity. Optimal diagnostic tests for these diagnostic issues are reviewed in a separate systematic literature review (SLR).11
The aim of this SLR was first to explore and summarise pharmacological and non-pharmacological therapeutic strategies in patients with D2T RA that could be used to treat inflammatory activity and non-inflammatory complaints. Furthermore, this SLR focused on the optimisation, and therefore also the identification, of a mismatch in goal setting between patients and healthcare professionals and of suboptimal self-management. This SLR was conducted to inform the EULAR recommendations for the management of D2T RA.
Methods
Research questions
This SLR was conducted following the EULAR Standardised Operating Procedures (SOP).12 Seven clinical questions on therapeutic strategies and the identification of suboptimal goal setting and self-management in patients with D2T RA were proposed by the fellow (NMTR), co-methodologist (PMJW) and postdoctoral fellow (MJHdH), and then approved by the steering committee (GN (convenor), JMvL (co-convenor), DvdH (methodologist), MK (fellow)). At the first Task Force meeting, the questions were discussed, amended and then approved by the whole Task Force.
The clinical questions were focused on pharmacological and non-pharmacological therapeutic strategies for (1a) patients with limited DMARD choices because of adverse events, comorbidities or other contraindications, (1b) patients who failed ≥2 b/tsDMARD with different MOA, (1c) patients with predominantly non-inflammatory complaints; and additionally on (2a) the identification and (2b) optimisation of a mismatch in goal setting, and (2c) the identification and (2d) optimisation of suboptimal self-management. The clinical questions were transformed into epidemiological questions using the ‘Patients, Intervention (index test for diagnostic question), Comparator (reference test), Outcome (PICO) format’ (online supplemental file).13
Supplemental material
Search strategy
The databases of PubMed, Embase and Cochrane were searched for papers in English until December 2019 for search 1 and December 2018 for search 2. Additionally, the conference abstracts of EULAR and ACR were screened, from 2017 until 2019 for search 1 and from 2017 until 2018 for search 2. Advice regarding the set-up of the search strategy was provided by two experienced librarians of Utrecht University (FPW and PHW).
The first search focused on the pharmacological and non-pharmacological therapeutic strategies for RA patients with limited DMARD choices, who previously failed b/tsDMARDs or those with predominantly non-inflammatory complaints. In addition to terms for RA and terms related to therapeutic studies, terms were included for difficult-to-treat disease, adverse events, fatigue, pregnancy and comorbidities that may limit DMARD choices (infections: hepatitis B virus (HBV), hepatitis C virus (HCV), HIV, tuberculosis (TBC); malignancies; lung disease: fibrosis, asthma, chronic obstructive pulmonary disease (COPD); cardiovascular (CV) disease: hypertension, cardiomyopathy; hyperlipidaemia; chronic kidney dysfunction; chronic liver dysfunction; liver enzyme elevation; osteoporosis; diabetes mellitus; thrombosis; depression; anxiety; online supplemental file). Furthermore, terms were included for specific DMARDs, glucocorticoids (GCs), non-steroidal- anti-inflammatory drugs (NSAIDs) and non-pharmacological treatment options. A search limit was set to the last 10 year. In addition, the reference lists of selected papers were manually screened. References published in the year 2000 and later were eligible for inclusion. This cut-off was chosen because of the introduction of bDMARDs around this time and, herewith, the beginning of a new therapeutic landscape regarding available treatment strategies in the field of RA. Moreover, as failure of ≥2 b/tsDMARD with different MOA is part of the D2T RA definition, RA patients could not fulfil the definition before this time point.
The second search focused on the identification and optimisation of suboptimal goal setting and self-management. In this search, terms for RA as well as terms for management goals and self-management were included (online supplemental file). No terms for difficult-to-treat patients were included, as studies in other RA patients were also considered to be relevant as indirect evidence for these specific questions, since limited evidence was expected. Additionally, no terms on specific outcomes were included as many outcomes could be of interest and they may be described in many different ways.
Selection of studies
First, titles and abstracts were screened in duplicate by the fellows (first search: NMTR and MK; second search: NMTR and AH) according to a predefined list of selection criteria (online supplemental file) until the percentage of conflicts was below 5%. In case of conflicts or when in doubt, eligibility was discussed with the co-methodologist (PMJW). Second, all full-text versions of the selected papers were screened in duplicate by the fellows (first search: NMTR, and MK or AH; second search: NMTR and AH). Disagreements were discussed with the co-methodologist (PMJW) until consensus was reached.
Following the EULAR SOP, SLRs of sufficient quality could be selected in addition to original studies.12 The original studies of the selected SLRs were excluded to avoid duplicate evidence. Additionally, the most recent SLR was selected in case of fully overlapping evidence in two or more SLRs.
As evidence for patients with D2T RA specifically was expected to be scarce, for the question on RA patients who previously failed ≥2 b/tsDMARDs with different MOA (1b), it was decided to select papers with patients who failed ≥1 b/tsDMARD. For the question on RA patients with non-inflammatory complaints (1c), papers specifically including patients with active disease, for example, according to composite indices, were excluded and only papers regarding patients with non-inflammatory complaints (reduced function and quality of life, and presence of pain and fatigue) or in unselected populations (ie, not specifically active disease) reporting on these outcomes were selected. Regarding the question on a mismatch in goal setting between patients and healthcare professionals (2a), studies comparing the frequencies of the importance of specific treatment goals between patients and healthcare professionals were also selected, as these may highlight important goals that may not match between patients and healthcare professionals.
Data extraction and quality assessment
Information on study design, patient characteristics, interventions, comparators and outcomes (including relevant descriptive statistics and/or occurrence and association measures) were extracted from the included papers using a predetermined format (online supplemental file).
Risk of bias (RoB) of the original papers was assessed using the Cochrane Collaboration’s risk of bias tool,14 and highest RoB as found was reported here (low, moderate, high). For the questions on the identification of suboptimal goal setting (2a) and self-management (2c), RoB was assessed using the Quality Assessment of Diagnostic Accuracy Studies tool version 2 (QUADAS-2),15 and highest RoB as found was reported (low, moderate, high). For SLRs, ‘A MeaSurement Tool to Assess systematic Reviews version 2’ (AMSTAR-2) was used and overall RoB was reported according to the AMSTAR-2 scoring system (low, moderate, high, critically high).16
Data extraction and quality assessment were performed in duplicate by the fellows (NMTR and AH) until the number of conflicts was below 5%. Disagreements and remaining doubts were discussed with the co-methodologist (PMJW) until consensus was reached.
Statistical analyses
Extracted data were summarised descriptively regarding the main reported or calculable association measures for the therapeutic questions (eg, odds ratio (OR), mean outcome in intervention and comparator group) and the diagnostic evaluations (eg, sensitivity, specificity, likelihood ratio).
Pooling of results was performed in case of sufficient clinical and statistical homogeneity as determined by the steering committee. For the questions on therapeutic strategies for RA patients with predominantly non-inflammatory complaints (1c) and optimisation of self-management (2d), effect sizes (using Cohen’s d) were calculated or extracted to be able to compare results over different outcomes and scoring methods.
Results
Study characteristics
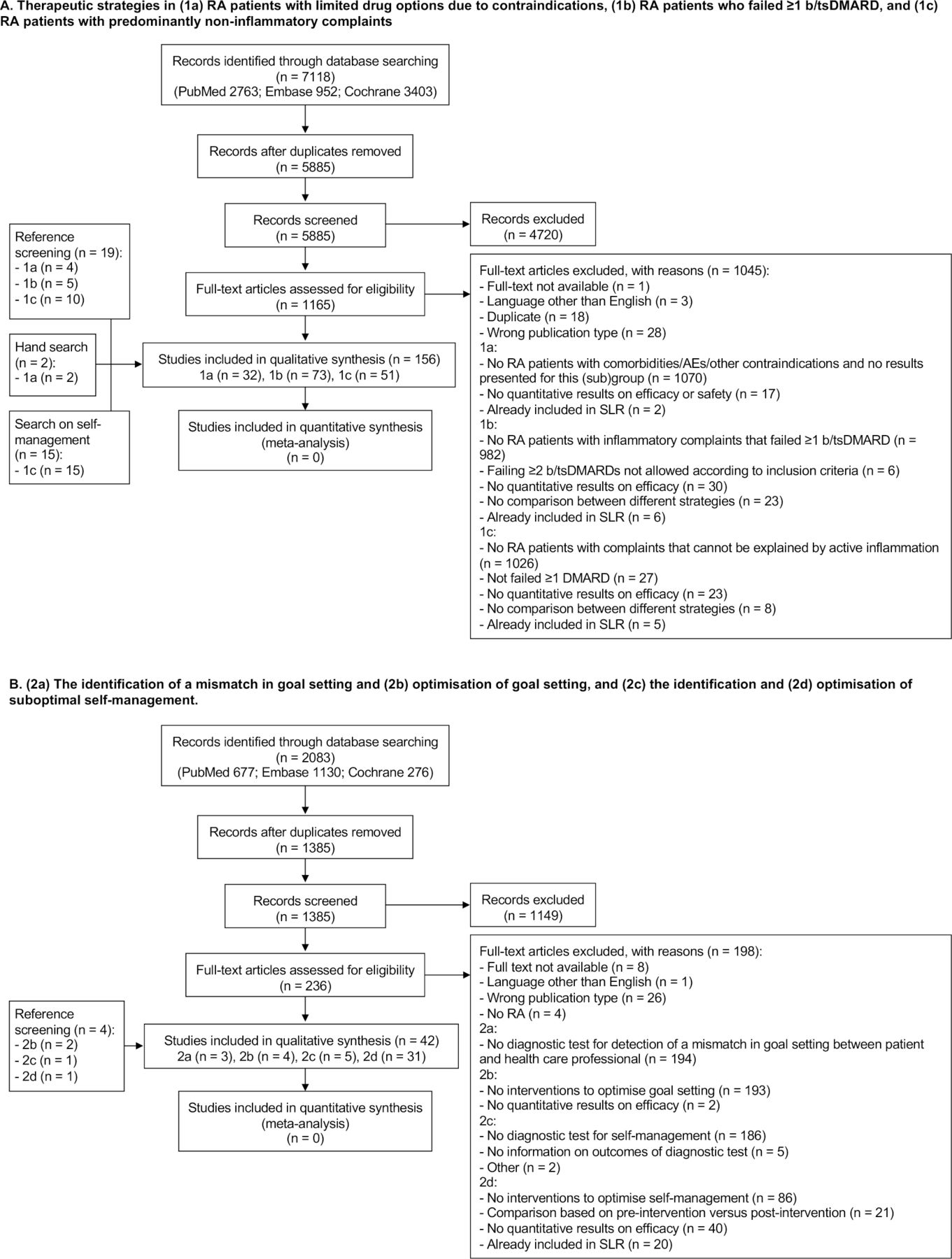
The first search regarding pharmacological and non-pharmacological strategies resulted in 5885 unique papers. After title and abstract screening, 1165 papers were selected for full-text screening and 121 papers were finally deemed eligible for inclusion. Additionally, 36 papers were selected via reference screening and hand search (figure 1A). Thirty-two papers were selected for ttherapeutic strategies in patients with limited DMARD options,17–48 73 for patients who failed ≥1 b/tsDMARD49–121 and 50 for patients with predominantly non-inflammatory complaints.122–171

Flow charts of search and selection of papers. AEs, adverse events; n, number of papers; RA, rheumatoid arthritis; SLR, systematic literature review.
The second search regarding goal setting and self-management yielded 1385 unique papers. Title and abstract screening resulted in 236 papers, and 38 papers were selected for data extraction. Four additional papers were selected via reference screening (figure 1B). Three172–174 and four papers175–178 were selected for the identification and optimisation, respectively, of a mismatch in goal setting between patients and healthcare professionals. Five173 179–182 and 31 papers122 125 126 130–132 135 137 144 145 148 152 153 159 160 162 167 183–196 were selected for the identification and optimisation, respectively, of suboptimal self-management.
None of the studies in search 1 or search 2 included patients with D2T RA specifically, resulting in a lower applicability of the results overall. Heterogeneity in study populations, therapeutic strategies, outcome criteria and association measures prohibited pooling the data in an appropriate way. All quantitative information regarding study characteristics, therapeutic strategies and outcomes are summarised in online supplemental tables 1-7.
Supplemental material
Supplemental material
Supplemental material
Supplemental material
Supplemental material
Supplemental material
Supplemental material
The overall RoB was moderate or high in the majority of studies. Studies were considered as having a high RoB because of their study design (ie, observational studies), subanalyses of randomised controlled trials (RCTs) were performed (not a priori planned or not based on stratified groups) or blinding of participants was not performed (as in the majority of studies regarding non-pharmacological strategies). Studies were assessed as having a moderate RoB, due to insufficient reporting of the randomisation process and/or allocation concealment. Detailed RoB assessment is shown in online supplemental tables 1-7.
RA patients with limited drug options
Thirty-two papers (6 SLRs, 9 RCTs, 17 observational studies; 1 low RoB, 7 moderate RoB, 24 high RoB) were selected comparing efficacy and/or safety of DMARDs in RA patients with limited DMARD options due to a comorbidity and/or another contraindication: HBV, HCV, hepatic disease, pulmonary disease, CV disease, obesity, osteoporosis/osteopenia, renal disease, extra-articular manifestations, pregnancy, psychological disease (online supplemental table 1).17–26 28–41 44–48 No evidence was identified comparing the efficacy and/or safety of DMARDs in RA patients with gastrointestinal disease, HIV, (latent) TBC, malignancies or previously experienced adverse events related to the treatment.
Only the efficacy of infliximab in RA patients with obesity was assessed in more than one cohort of RA patients. In both papers (high RoB), infliximab (3 mg/kg) was found to be less effective in patients with a body mass index (BMI) >30 than in those with BMI <30 (Disease Activity Score assessing 28 joints based on erythrocyte sedimentation rate (DAS28-ESR) remission at 12 months: 0% vs 22.4%, p=0.0128; change in DAS28 ≥1.2 from baseline (BL) until 16 weeks: 58.1% vs 46.7%, p=0.04).33 No differences in RA patients with BMI >30 compared with those with BMI <30 were found for treatment with adalimumab, etanercept or rituximab (in single observational studies: DAS28 based on C reactive protein (CRP) <2.6 at 12 months, adalimumab: 14.8% vs 30.1%, p=0.08; DAS28-CRP <2.6 at 12 months, etanercept: 27.6% vs 36.2%, p=0.44; ACR50 response at 24 weeks, rituximab: 55.7% vs 49.1%–53.4%, not significant).48 In patients with obesity, no studies comparing different treatment options were identified.
Safety of DMARD use in patients with a comorbidity was assessed in an SLR or in more than one cohort of RA patients with HBV, HCV, pregnancy/lactation and in those at risk for venous thromboembolisms (VTEs). In patients with active HBV, a relatively low rate of HBV reactivation was found using bDMARDs in one SLR (of 21 studies, moderate RoB) and two observational studies (high RoB) compared with patients with inactive HBV (tumour necrosis factor inhibitor (TNFi), SLR: 10.7% vs 2.6%; tocilizumab: 0% vs 4.8%; abatacept: 0% vs 0%).20 22 39 The authors of the SLR concluded that antiviral prophylaxis would be recommended in patients with active HBV infection.20
In an observational study (high RoB) in patients with HCV undergoing treatment with TNFi, liver disease developed more frequently compared with patients without HCV (development of liver injury within 1 year: 10% vs 1.23%, p=0.099),34 a difference that did not reach statistical significance in this relatively small sample size (n=101). The authors of the SLR (of 37 studies, high RoB) concluded that the safety profile of TNFi in the setting of HCV infection seemed to be acceptable.18
Evidence regarding safe DMARD use before and during pregnancy and during lactation was found in the 2020 ACR guideline and 2016 EULAR points to consider (of 53 and 319 studies, respectively, moderate RoB).27 42 These recommendations have been based on extensive SLRs and summarise the evidence per DMARD. In patients before and during pregnancy and lactation, no safety issues have been identified for antimalarials, sulfasalazine, azathioprine, ciclosporin, tacrolimus and glucocorticoids. Of bDMARDs, TNFis (especially certolizumab pegol) and rituximab appear without identified safety issues. Three additional papers (1 SLR (of 84 studies, moderate RoB), 2 observational studies (high RoB)) resembled the findings of these recommendations.23 30 36
In the SLR (of three studies on this topic, moderate RoB) regarding the safety of DMARDs informing the 2019 EULAR RA management recommendations, the safety of tsDMARDs in RA patients and especially those at risk for VTEs was summarised.43 In these patients, an increased risk of VTEs was found for tofacitinib and baricitinib, specifically when using the higher doses of 10 and 4 mg, respectively. Evidence on other tsDMARDs is not yet available.
RA patients who failed ≥1 b/tsDMARD
Failure of ≥2 bDMARDs
Nine papers were found regarding the efficacy of b/tsDMARDs in patients who failed ≥2 bDMARDs (7 RCTs (subanalyses), 2 observational studies; 1 moderate RoB, 8 high RoB; online supplemental table 2). In six of these papers, the efficacy of tocilizumab, tofacitinib, baricitinib, upadacitinib and filgotinib, respectively, versus placebo was assessed using ACR20 response at 12 to 24 weeks as an outcome (graphically summarised in figure 2).55 64 72 80 95 120 ACR20 response favoured therapy with b/tsDMARD in all papers. The other study (high RoB) assessed the efficacy of mavrilimumab versus golimumab in a small population of six patients who previously failed two TNFis excluding golimumab (ACR20 response at 24 weeks 66.7% vs 0%).119 In two observational studies (high RoB), the efficacy of an alternative TNFi versus rituximab was assessed and rituximab was found to be more effective (DAS28-ESR at 6 months 4.54 vs 3.91, p=0.021; change in DAS28 from BL until 6 months −0.75 vs −1.31, not significant).53 66
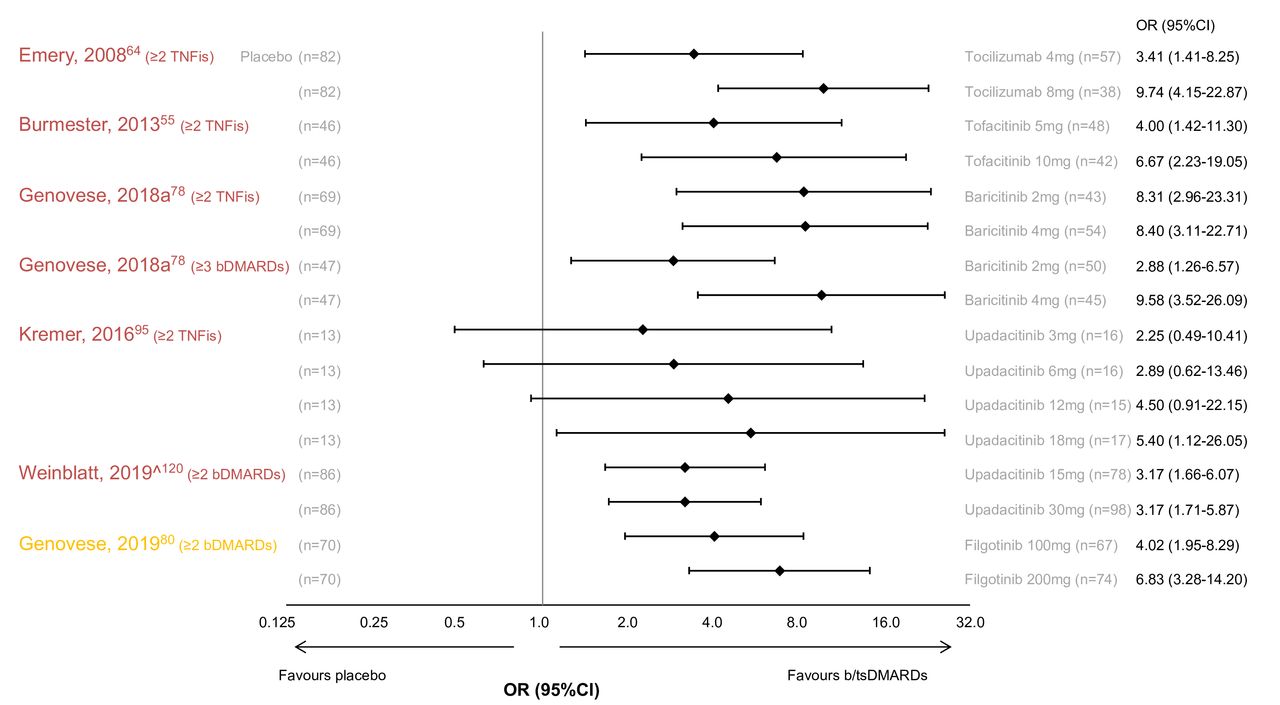
ACR20 response at 12to 24 weeks in RA patients who failed ≥2 bDMARDs. (m)ACR, (modified) American College of Rheumatology; bDMARD, biological synthetic disease-modifying antirheumatic drug; n, number of patients; OR, odds ratio; RA, rheumatoid arthritis; TNFi, tumour necrosis factor inhibitor. Colours of author names according to risk of bias: font in yellow: moderate risk of bias; font in red: high risk of bias. ORs are shown as diamonds and whiskers represent 95% CI.
Failure of ≥1 b/tsDMARD
Thirty-one papers (7 SLRs, 23 RCTs, 1 observational study; 8 low RoB, 16 moderate RoB, 7 high RoB) assessed the efficacy of b/tsDMARDs in patients who failed ≥1 bDMARD versus placebo (online supplemental table 2).50 52 56 57 61 67 68 70–77 79 80 85 92 94 95 97 98 103 104 108 109 111 113 115 116 A significant higher efficacy was found for the following b/tsDMARDs compared with placebo: alternative TNFi, abatacept, rituximab, tocilizumab, ixekizumab, ocrelizumab, olokizumab, sarilumab, secukinumab, sirukumab, tofacitinib, baricitinib, upadacitinib and filgotinib. No benefit in efficacy was found for other bDMARDs compared with placebo, which are not approved for RA (atacicept, fostamatinib and tabalumab).
Thirty-eight papers (7 SLRs, 6 RCTs, 25 observational studies; 2 low RoB, 7 moderate RoB, 29 high RoB) compared the efficacy of different b/tsDMARDs in patients who failed ≥1 b/tsDMARD (online supplemental table 2).49 52 54 58–60 62 63 65 69 75 81–84 87–94 96 97 99–101 106 107 110 112 114 115 117–119 121 Only one study (high RoB) explicitly included a mixed population of patients who failed a bDMARD or a tsDMARD, all other papers only included patients who failed ≥1 bDMARD.69 In 30 of 38 papers, patients explicitly failed a TNFi. Patients failed rituximab in three papers,62 114 117 tocilizumab in two papers,49 100 a non-TNFi in one paper,101 and a mix of TNFis and non-TNFi bDMARDs in two papers.96 110
Six papers (4 SLRs (of 9, 24, 6 and 4 papers (partly overlapping)), 1 RCT and 1 observational study; 3 moderate RoB, 3 high RoB) assessed the efficacy of alternative TNFis versus non-TNFi bDMARDs as a group, in patients who failed a TNFi.52 82 83 94 99 118 Non-TNFi bDMARDs were found to be more effective in two original studies using different outcome criteria (EULAR good/moderate response at 52 weeks 43% vs 60%, p=0.0006 (high RoB)83; change in clinical disease activity index (CDAI) from BL until 1 year −4.81 vs −7.54, p=0.037 (high RoB)118). Two of four SLRs (of 24 and 6 studies (partly overlapping); moderate RoB) concluded that there was a tendency of non-TNFi bDMARDs to be more effective than TNFis, after failure of a TNFi.52 82 94 99
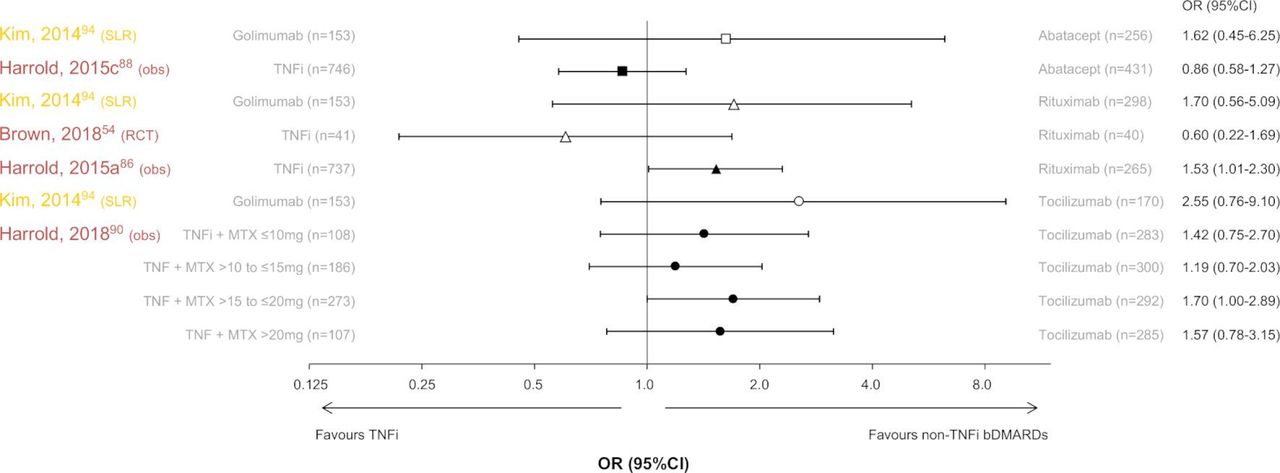
Three papers assessed the efficacy of an alternative TNFi versus abatacept, conflicting results were found regarding the superiority of abatacept in patients who failed a TNFi (1 SLR (of six studies), 1 observational study; 1 moderate RoB, 1 high RoB),88 94 and some advantage was found for TNFi to be more effective than abatacept in patients who failed tocilizumab (1 observational study; high RoB).49 There was a numerical advantage of rituximab to be more effective than TNFi in patients who failed a TNFi in 6 of 10 papers (statistically significant in at least one of the response criteria in 5 papers (2 SLRs (of 24 and 6 studies (partly overlapping)), 1 RCT, 7 observational studies; 2 moderate RoB, 8 high RoB).54 59 65 81 82 86 93 94 107 112 Additionally, there was a numerical advantage of tocilizumab in patients who failed a TNFi in three of four papers (statistically significant in at least one of the response criteria in 3 papers (2 SLRs (of 24 and 6 studies (partly overlapping)), 2 observational studies; 2 moderate RoB, 3 high RoB),82 90 91 94 a numerical advantage of tocilizumab in patients who failed rituximab in 2 of 2 papers (statistically significant in at least one of the response criteria in 1 paper (2 observational studies; 2 high RoB)114 117 and no advantage of TNFi nor tocilizumab in patients who failed a bDMARD (not further specified (1 observational study; high RoB).96 Five of the abovementioned papers reported an (modified) ACR50 response as outcome and are graphically summarised in figure 3.54 86 88 90 94

TNFi versus non-TNFi bDMARDs: (m)ACR50 response at 6 to 12 months in patients with rheumatoid arthritis (RA) who failed ≥1 TNFi. (m)ACR, (modified) American College of Rheumatology; bDMARD, biological disease-modifying antirheumatic drug; mg, milligram; MTX, methotrexate; n, number of patients; obs, observational study; TNFi, tumour necrosis factor inhibitor; SLR, systematic literature review. Colours of author names according to risk of bias: font in yellow: moderate risk of bias; font in red: high risk of bias. ORs are shown as ▀, abatacept; ▲, rituximab; ●, tocilizumab. White symbols represent univariate analyses, black symbols multivariate analyses and whiskers 95% CI.
Six papers compared the efficacy of different alternative TNFis in patients who failed a TNFi and concluded that there was insufficient evidence to prioritise (1 SLR (of 9 studies), 1 RCT, 4 observational studies; 1 low RoB, 5 high RoB).52 58–60 106 121 When directly comparing different non-TNFi bDMARDs, there was a numerical advantage of tocilizumab to be more effective than abatacept in patients who failed a TNFi in six of seven papers (statistically significant in at least one of the response criteria in 3 papers (1 SLR (of 4 studies), 1 RCT, 5 observational studies; 1 moderate RoB, 6 high RoB)).63 83 84 89 91 97 101 Additionally, there was a numerical advantage of tocilizumab to be more effective than abatacept in patients who failed rituximab in three of three papers (statistically significant in at least one of the response criteria in 2 papers (3 observational studies; 3 high RoB)).62 114 117 Furthermore, there was some advantage of tocilizumab to be more effective than rituximab in patients who failed a TNFi (4 papers) or a non-TNFi (1 paper) in five of five papers (statistically significant in at least one of the response criteria in all papers (2 SLRs (of 24 and 4 studies (partly overlapping)), 1 RCT, 2 observational studies; 2 moderate RoB, 3 high RoB)).82–84 97 101 Additionally, a numerical advantage of rituximab to be more effective than abatacept was found in patients who failed a TNFi in three of three papers (statistically significant in at least one of the response criteria in 1 paper (1 SLR (of 4 studies), 1 RCT, 1 observational study; 1 moderate RoB; 2 high RoB)).54 84 97
Three papers compared the efficacy between tsDMARDs and different bDMARDs (2 SLRs (of 4 and 5 studies (partly overlapping)), 1 observational study; 2 moderate RoB, 1 high RoB).69 97 115 There was a numerical advantage of rituximab to be more effective than tofacitinib in patients who failed a TNFi two of two papers, although statistical significance was not reached.97 115 Conflicting results were found regarding superiority in efficacy of the other bDMARDs assessed (TNFi, abatacept, tocilizumab) versus tofacitinib. No studies comparing bDMARDs versus other tsDMARDs were identified nor studies comparing different tsDMARDs.
Comparison of efficacy of b/tsDMARDs between RA patients who previously failed a different number of bDMARDs
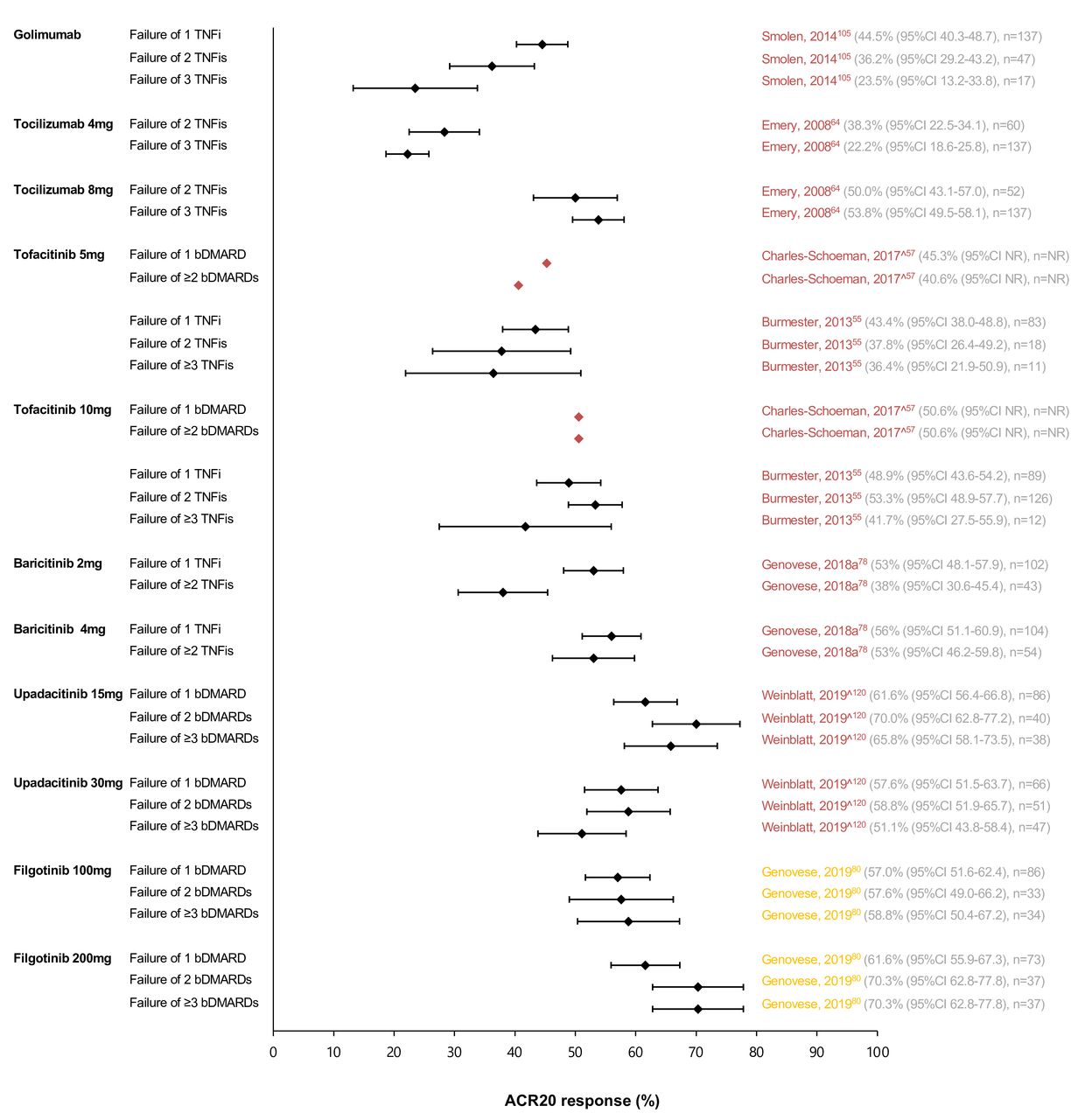
Nine papers compared the efficacy of a b/tsDMARD between patients who previously failed an increasing number of bDMARDs (8 RCTs (subanalyses), 1 observational study; 1 moderate RoB, 8 high RoB; online supplemental table 2).55 57 64 78 80 86 102 105 120 Seven studies used ACR20 response as an outcome, a graphical summary is shown in figure 4.55 57 64 78 80 105 120 For golimumab, tocilizumab 4 mg (intravenous), tofacitinib 5 mg and baricitinib 2 mg, the efficacy numerically decreased with an increasing number of previously failed bDMARDs.55 57 64 78 105 For upadacitinib and filgotinib, this tendency in decreased efficacy was less clear,80 120 as well as for the higher doses of tocilizumab (intravenous), tofacitinib and baricitinib (figure 4).55 57 64 78
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Comparison of ACR20 response at 3 months to 24 weeks in studies comparing RA patients with different numbers of previously failed bDMARDs. ACR, American College of Rheumatology; bDMARD, biological disease-modifying antirheumatic drug; n, number of patients; NR, not reported; RA, rheumatoid arthritis; TNFi, tumour necrosis factor inhibitor; ˆAbstract. Colours of author names according to risk of bias: font in yellow: moderate risk of bias; font in red: high risk of bias. Black diamond with whiskers: OR with 95% CI; red diamond: OR, 95% CIs are not reported.
Two studies reported other response criteria than the ACR20 response. In these studies, the efficacy of abatacept and rituximab also numerically decreased with an increasing number of previously failed bDMARDs (abatacept: change in DAS28-CRP from BL until 6 months, failure of 1 TNFi vs 3 TNFis: −2.1% vs −1.7%, statistically significant (high RoB)102; rituximab: CDAI at 12 months (not corrected for baseline values), failure of 1 TNFi vs ≥2 TNFis: 13.2 vs 18.3, significance not reported (high RoB)87).
RA patients with predominantly non-inflammatory complaints
Fifty papers (21 SLRs (on different topics, although partly overlapping), 27 RCTs, 2 observational studies; 12 low RoB, 11 moderate RoB, 27 high RoB) were found regarding RA patients with non-inflammatory complaints (online supplemental table 3).122–171 Heterogeneous interventions were assessed, while the control intervention was mostly usual care or waiting list. Different outcome criteria were used to assess efficacy. The number of papers with statistically significant benefit of the intervention compared with control per category of intervention and per outcome, including their effect size (if reported or calculable), is shown in table 1.
Papers on therapeutic strategies for non-inflammatory complaints, including effect sizes
Only eight papers specifically selected patients with non-inflammatory complaints (pain: 4 (1 SLR (of 11 studies), 3 RCTs; 1 low RoB, 2 moderate RoB, 1 high RoB)143 151 156 170; fatigue: 3 (3 RCTs; 3 high RoB)137 143 146; psychological problems: 1 (RCT; high RoB)138; difficulties in performing daily activities: 1 (RCT; high RoB)168). Although patients in these studies were selected on the presence of non-inflammatory complaints, DAS28 still ranged from 2.82 to 5.85 (not reported in 3 studies, online supplemental table 3). Therefore, the presence of inflammatory activity could not be excluded. The results of these papers resembled the findings of the other studies, which enrolled an unselected population of RA patients and reported on outcomes regarding non-inflammatory complaints.
Exercise, education, self-management programmes and intensification of patient care were found to improve function. Dietary, psychological interventions and self-management programmes were found to reduce pain, as well as pharmacological interventions (ketoprofen patch and celecoxib). Psychological and self-management programmes were found to reduce fatigue. No (sufficient) benefit in any of the abovementioned complaints was found for alternative medicine, cryotherapy and balneotherapy.
Identification and optimisation of a mismatch in goal setting between RA patients and healthcare professionals
Identification of a mismatch in goal setting
Three studies (all with a cross-sectional design; two high RoB, one qualitative study) were found regarding the identification of a mismatch in goal setting between patients and healthcare professionals (online supplemental table 4).172–174 A diagnostic test to identify a mismatch was not identified. All studies compared two different populations regarding the importance of treatment goals: RA patients and clinicians in two studies, and RA patients with high and low disease activity in the other study. In the qualitative study, patients expressed a desire for clinicians to look beyond clinical markers and to consider patient-reported outcomes.172 In the other study comparing RA patients and clinicians (high RoB), patients and clinicians had the same treatment goals regarding complaints, medication use and daily activity.173 Most treatment goals, such as reduction in inflammation, pain and fatigue, were more frequently scored as important by clinicians (patients vs clinicians: 50% vs 74%, 67% vs 88% and 46% vs 62%, respectively). Only ‘see more/other physicians to help RA management’ was more frequently scored as important by RA patients, although the difference was small (13% vs 9%). In the study comparing RA patients with high and those with low disease activity (high RoB), improvement in arthritis was more frequently scored as important by patients with high disease activity.174 On the other hand, improvement in morning stiffness was more frequently scored as important by patients with low disease activity.
Optimisation of goal setting
Four studies (1 RCT, 3 observational studies; all high RoB) were found regarding the optimisation of goal setting.175–178 All studies used a web-based education tool as the intervention (online supplemental table 5). Different selections of RA patients were included: patients with active disease, patients who were unsure about starting treatment with methotrexate, patients who were starting b/tsDMARDs or an unselected population. RA knowledge improved statistically significantly using the intervention in all studies. In one study, in an unselected population of RA patients, willingness to try a b/tsDMARD was assessed and improved statistically significantly.175 In another study, in patients starting b/tsDMARDs, certainty in choosing a DMARD option was assessed and increased statistically significantly.178
Identification and optimisation of self-management
Identification of suboptimal self-management
Five papers were found regarding the identification of suboptimal self-management: two assessed the importance of factors associated with successful self-management comparing RA patients and clinicians (2 with a cross-sectional design; 1 low RoB, high RoB)173 181 and three assessed a diagnostic measure (1 SLR (of 15 studies), 2 cross-sectional studies; all moderate RoB; online supplemental table 6).179 180 182
In both descriptive studies regarding the importance of factors associated with optimal self-management, most factors were more frequently scored as important by clinicians than by RA patients (eg, a discussion about self-management, more/longer visits, education about psychosocial needs, activities of daily living, sexual concerns).173 181 Patients expressed a desire for a more important role of pharmacists and nutritionists in arthritis education, and for more education on the disease, diagnostic process and nutrition.181
In the SLR regarding diagnostic measures, the Arthritis Self-Efficacy Scale (ASES) and RA Self-Efficacy Scale (RASE) were found to be assessed in more than one cohort of RA patients. Evidence for the RASE suggested that this measure is multidimensional, which is not adequately represented in the scoring. Therefore, ASES was concluded to be the most reliable test, although its methodological weakness was acknowledged by the authors (ie, the content validity and whether it adequately reflects self-efficacy was not explicitly addressed during development).179 In another study, the Modified Rheumatology Attitude Index correlated with the combined questionnaire for functional impairment and quality of life, pain score, patient global assessment and functional impairment questionnaire.180 In a study assessing two cohorts of RA patients, the Brief Resilient Coping scale also significantly correlated with different other measures.182
Optimisation of self-management
Thirty-one papers (7 SLRs (on different topics, although partly overlapping), 23 RCT, 1 observational study; 5 low Rob, 3 moderate RoB, 23 high RoB) were found regarding the optimisation of self-management (online supplemental table 7). No papers specifically selected patients with suboptimal self-management. Different outcomes were found to describe self-management for which different outcome measures were used and heterogeneous interventions were assessed (table 2). The number of papers with statistically significant benefit of the intervention compared with control (mostly usual care or waiting list) per outcome and per type of intervention, including their effect size (if reported or calculable), is shown in table 2.
Papers on the optimisation of self-management, including effect sizes
Improvement in self-efficacy was found using self-management programmes, educational and psychological interventions, exercise programmes, nurse-led follow-up, eszopiclone 3 mg (in RA patients with insomnia) and assistive technology (eye drop dispenser in RA patients with concomitant Sjögren’s syndrome). Psychological interventions were found to reduce anxiety and depression. Education and web-based rehabilitation were found to improve RA knowledge. Benefit of the interventions was also found for other outcomes: self-management programmes and cognitive behavioural therapy to reduce helplessness; self-management programmes to improve autonomous motivation and self-management behaviour and to reduce psychological distress; and psychological interventions to improve coping.
Discussion
In this SLR, evidence is summarised regarding pharmacological and non-pharmacological therapeutic strategies informing the EULAR Task Force in charge of the development of recommendations for the management of D2T RA. Several limitations were found in the selected available evidence. First, no studies were found evaluating therapeutic strategies in patients who fulfilled the definition of D2T RA.6 Therefore, typically, evidence regarding pharmacological therapeutic strategies needed to be extrapolated from studies in patients with active disease who failed at least one bDMARD, which was a TNFi in almost all studies, instead of two b/tsDMARDs with a different MOA as in the definition. Additionally, most studies on non-pharmacological strategies were performed in an unselected population of RA patients instead of in patients with D2T RA with predominantly non-inflammatory complaints, in whom the absence of inflammatory activity could not be ascertained. Second, heterogeneity in patient populations, interventions, comparators and outcome criteria hampered pooling of efficacy outcomes. Third, only very few studies with low RoB were found. Considering these limitations, the results should be interpreted cautiously for patients with D2T RA.
Regarding pharmacological interventions for patients with D2T RA, limited evidence (of low to moderate quality) was found on the efficacy and safety of DMARDs for patients with limited DMARD options due to contraindications regarding obesity, HBV, HCV, pregnancy, lactation and those at risk for VTEs. In patients with obesity, infliximab may be less effective compared with patients with a normal BMI, and adalimumab, etanercept and rituximab may be less affected by BMI.28 33 48 For patients with HBV, TNFi, abatacept and tocilizumab were found to be relatively safe.20 22 39 For patients with HCV, TNFi was found to be a relatively safe treatment option.18 34 For patients before and during pregnancy and during lactation, no safety issues have been identified for several DMARDs, which are described in the 2020 ACR guideline and 2016 EULAR points to consider.27 42 In patients at risk for VTEs, an increased risk of VTEs was found during treatment with tsDMARDs, especially in the higher doses.43 In these patients, other DMARDs may be preferred.
In patients who failed at least two bDMARDs, several b/tsDMARDs (tocilizumab, tofacitinib, baricitinib, upadacitinib and filgotinib) were found to be more effective than placebo.55 64 72 80 95 120 In patients who failed at least one bDMARD, a benefit in efficacy compared with placebo was found for all currently used b/tsDMARDs.52 56 57 67 68 76 77 79 80 85 94 95 97 98 104 108 115 116 Despite this benefit in efficacy compared with placebo, generally, the extent of the beneficial effect of b/tsDMARDs was found to become less when patients failed a higher number of previous bDMARDs.55 57 64 78 86 102 105 This tendency was less convincing for upadacitinib and filgotinib and for the higher doses of tocilizumab (intravenous), tofacitinib and baricitinib.55 57 64 78 80 120 Although this may suggest a preference for these b/tsDMARDs (in these higher doses) in patients with D2T RA, it may also be related to the more recent introduction of these drugs with a novel MOA and the timing of their application in therapeutic strategies. If, for instance, a TNFi would have been applied in patients who previously failed increasing numbers of tsDMARDs, the beneficial effect of TNFi may also have been less dependent on the number of previously failed tsDMARDs. However, for tocilizumab, tofacitinib and baricitinib, the tendency of decreasing efficacy with an increasing number of previously failed bDMARDs was not apparent for their higher doses and only for their lower doses.55 57 64 78 This may indicate that not only their more recent introduction and the novel MOA play a role. Additionally, the studies on tofacitinib, upadacitinib and filgotinib enrolled patients who failed different bDMARDs and not only TNFis.57 80 120 Nevertheless, future studies should assess to what extent this tendency is related to these specific b/tsDMARDs or to the order of their application in therapeutic strategies. Furthermore, a tendency was found for non-TNFi bDMARDs to be more effective than TNFis in patients who failed at least one TNFi, although insufficient evidence was identified to prioritise different non-TNFi b/tsDMARDs.49 52 54 59 65 81–83 86 88 90 91 93 94 96 99 107 112 114 117 118 These findings could indicate that non-TNFi bDMARDs and tsDMARDs may be somewhat more effective in comparison to another TNFi in patients with D2T RA. Specifically, if these non-TNFi b/tsDMARDs are of a previously not targeted MOA.
Regarding non-pharmacological interventions for patients with D2T RA, exercise, education, psychological and self-management interventions were found to be of additional benefit to improve non-inflammatory complaints (mainly functional disability, pain and fatigue).122 125 126 129 132–138 140 144 146–148 152–154 157–160 162 165–167 171 It may be expected that non-pharmacological interventions do not become less effective in patient failing a higher number of previous bDMARDs as much as pharmacological interventions as described above. Therefore, the additional benefit of non-pharmacological interventions might be even higher in patients with D2T RA. However, no formal evidence was found to support this.
Furthermore, education was found to improve goal setting and self-management.175–178 Additionally, self-management programmes, education and psychological interventions were found to improve different aspects of self-management, namely, self-efficacy, anxiety, depression and RA knowledge.122 125 132 137 144 148 152 159 160 162 167 183 185–193 195 Before goal setting between patients and healthcare professionals as well as self-management can be improved, a mismatch in goal setting and suboptimal self-management should be identified. No accurate measures were found to identify a mismatch in goal setting, although patients expressed a desire to take their quality of life goals more explicitly into account.172 ASES was found to be the most extensively studied tool to identify the level of self-management, although validated cut-offs are not available, hampering its use in clinical practice as a diagnostic instrument.179 197
This SLR was aimed to supplement the evidence as summarised for the current EULAR recommendations for the management of RA.1 In the SLR informing the current RA management recommendations, insufficient evidence was found to prioritise different b/tsDMARDs.198 In contrast, in our SLR a tendency was found of non-TNFi bDMARDs to be more effective than TNFis in RA patients who failed at least one TNFi. This difference is explained by the inclusion of observational studies and network meta-analyses in our SLR, while these study designs were specifically excluded from the SLR informing the RA management recommendations. However, we felt it was necessary not to exclude this evidence from our SLR, as direct comparisons in RCTs are lacking in patients with D2T RA. By all means, careful interpretation of the outcomes of these types of studies is warranted, also as results need to be extrapolated to the D2T RA patient population.
Although many therapeutic clinical questions were assessed in this SLR, not all therapeutic strategies for all potential factors contributing to D2T RA have been addressed. At the first meeting of the D2T RA Task Force, treatment non-adherence and lifestyle interventions were also discussed as topics of interest. As there are currently two ongoing EULAR projects related to these issues in patients with rheumatic and musculoskeletal diseases, it was decided to refer to the evidence found in their SLRs for the D2T RA recommendations in consultation with the steering committees of these Task Forces. Therefore, these topics are not included in this SLR.
In clinical practice, the heterogeneity of D2T RA should be considered when choosing the optimal therapeutic strategy for the individual patient with D2T RA. As a myriad of factors may contribute to the D2T RA state,4 9 the therapeutic strategy should be individually tailored and may consist of multiple (pharmacological and non-pharmacological) interventions. Further guidance on this will be provided by the EULAR Task Force on D2T RA in their recommendations for the management of D2T RA, including their interpretation of the clinical implications of the results, which will be published soon.199 Additionally, the heterogeneity of D2T RA should be considered in future studies as not all therapeutic strategies will be useful for all patients with D2T RA. The EULAR Task Force on D2T RA will also provide a research agenda, in which further guidance on topics of interest will be given.199
In addition to the limitations in the evidence that was found, this SLR has some limitations itself. Although an extensive literature search has been performed, relevant papers might have been missed due to the choices that have been made in the search strategy. For the search on pharmacological and non-pharmacological therapeutic strategies, the publication year 2000 was chosen as a cut-off because of the introduction of bDMARDs around this time point. For the subquestion on patients with predominantly non-inflammatory complaints, it was chosen to focus on the often-reported outcomes of function, pain, quality of life and fatigue. For the subquestions on goal setting and self-management, it was chosen to focus on RA patients only, while studies in patients with other chronic diseases may also provide useful information. In our opinion, these choices were mandatory to most efficiently create an overview of the current literature on the most important outcomes in the present therapeutic landscape. Nevertheless, these choices need to be reassessed in case the D2T RA recommendations, and consequently the SLRs, will be updated. Additionally, we chose to report effect sizes to compare results over different outcomes and scoring methods. However, effect sizes were not extractable for all studies, which hampers interpretation and pooling of results. The reported effect sizes varied widely for some outcomes (eg, alternative medicine to improve range of motion: 0.49–14.37), which may indicate publication bias. Although the possibility of publication bias was assessed within the RoB assessment of the SLRs16 and the level of evidence of the recommendations, interpreting this bias, especially with a limited number of studies, is difficult and, therefore, the effect sizes should be interpreted cautiously.
In conclusion, this SLR underscores the scarcity of (high-quality) evidence on the optimal treatment of patients with D2T RA. As D2T RA is a newly defined disease state, all evidence is to an extent indirect. Limited evidence was found on effective and/or safe DMARDs for patients with limited DMARD options due to contraindications. In patients who previously failed bDMARDs, all currently used b/tsDMARDs were found to be more effective than placebo. However, generally, effectiveness of b/tsDMARDs decreased in patients who had failed a higher number of bDMARDs and subsequent b/tsDMARDs of a previously not targeted MOA appear to be more effective. Furthermore, a beneficial effect of non-pharmacological interventions, specifically education, was found for improvement of non-inflammatory complaints (function, pain, fatigue), goal setting and self-management (self-efficacy, anxiety, depression, RA knowledge).
Acknowledgments
We would like to thank M.J.H. de Hair (MJHdH) for her valuable input in the initial phase of this project and F.P. Weijdema (FPW) and P.H. Wiersma (PHW) for their input to the search strategies.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Presented at Parts of this manuscript have been presented at EULAR 2020 (Roodenrijs NMT, Hamar A, Kedves MH, et al. SAT0052 Therapeutic strategies in difficult-to-treat rheumatoid arthritis: preliminary results of a systematic literature review informing the 2020 EULAR recommendations for the management of difficult-to-treat rheumatoid arthritis. Ann Rheum Dis 2020;79:953, and Roodenrijs NMT, Hamar A, Kedves MH, et al. FRI0047 Strategies regarding goal setting and self-management in difficult-to-treat rheumatoid arthritis: preliminary results of a systematic literature review informing the 2020 EULAR recommendations for the management of difficult-totreat rheumatoid arthritis. Ann Rheum Dis 2020;79:595).
Contributors NMTR drafted the clinical questions, performed the systematic literature review including risk of bias assessment, contributed to data analysis and interpretation of data, and drafted the manuscript. AH and MK contributed to the systematic literature review including risk of bias assessment. GN, JMvL and DvdH contributed to interpretation of data and manuscript preparation. PMJW drafted the clinical questions, supervised the systematic literature review including risk of bias assessment, contributed to interpretation of data and manuscript preparation. All authors reviewed and approved the final manuscript.
Funding This project was funded by the European League Against Rheumatism.
Competing interests NMTR, AH, MK and PMJW declare to have no competing interests. GN received fees from Amgen, AbbVie, BMS, Boehringer Ingelheim, Janssen, KRKA, Merck, MSD, Novartis, Pfizer, Roche and UCB; research grants from Pfizer and AbbVie. JMvL reports personal fees from Arxx Tx, Gesyntha, Magenta, Sanofi Genzyme, Leadiant, Boehringer-Ingelheim and Galapagos; grants and personal fees from Roche; grants from AstraZeneca, MSD, ThermoFisher. DvdH received consulting fees from AbbVie, Amgen, Astellas, AstraZeneca, BMS, Boehringer Ingelheim, Celgene, Daiichi, Eli-Lilly, Galapagos, Gilead, GlaxoSmithKline, Janssen, Merck, Novartis, Pfizer, Regeneron, Roche, Sanofi, Takeda and UCB. All competing interests are outside the submitted work.
Patient consent for publication Not required.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement Data are available from the corresponding author upon reasonable request.