Article Text

Abstract
Introduction Although patient-reported outcome measures (PROMs) are increasingly used in clinical practice and research, it is unclear whether these instruments cover the perspective of young people with inflammatory arthritis (IA). The aims of this study were to explore whether PROMs commonly used in IA adequately cover the perspective of young people from different European countries.
Methods A multinational qualitative study was conducted in Austria, Croatia, Italy and the Netherlands. Young people with either rheumatoid arthritis (RA), juvenile idiopathic arthritis (JIA), Still’s disease, psoriatic arthritis (PsA) or spondyloarthritis (SpA), aged 18–35 years, participated in semistructured focus group interviews. Thematic analysis was used and data saturation was defined as no new emergent concepts in at least three subsequent focus groups.
Results Fifty-three patients (21 with RA/JIA/Still’s, 17 with PsA, 15 with SpA; 72% women) participated in 12 focus groups. Participants expressed a general positive attitude towards PROMs and emphasised their importance in clinical practice. In addition, 48 lower level concepts were extracted and summarised into 6 higher level concepts describing potential issues for improvement. These included: need for lay-term information regarding the purpose of using PROMs; updates of certain outdated items and using digital technology for data acquisition. Some participants admitted their tendency to rate pain, fatigue or disease activity differently from what they actually felt for various reasons.
Conclusions Despite their general positive attitude, young people with IA suggested areas for PROM development to ensure that important concepts are included, making PROMs relevant over the entire course of a chronic disease.
- patient-reported outcome measures
- qualitative research
- arthritis
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Key messages
What is already known about this subject?
Patient-reported outcome measures (PROMs) have been used for different purposes in routine clinical practice, research and health services management in recent decades, particularly in the field of chronic diseases.
What does this study add?
This is the first study that explores perspectives and views of young people with inflammatory arthritis (IA) on widely used PROMs.
Young people in all countries and disease areas did not feel sufficiently informed about the value of PROMs and the reasons for collecting patient-reported outcomes in addition to clinical outcomes.
From the perspective of young people, commonly used functional assessments seem to be outdated and overlook current relevant issues. These include career planning, caring for others such as children, losing friends, participating in social life (like going out in the evening), being excluded from physical activities at school and university, and using technological devices including smartphones and computers.
Young people considered a large number of functional items too ‘easy’, for example, walking and eating, while other more complex activities in daily life, such as using public transport or preparing meals were missing at all.
How might this impact on clinical practice?
The results of our study will change the use of PROMs in young people with IA in clinical practice and research. In the future, young people with IA should be involved in the adaptation of existing PROMs and the development of new instruments to ensure that important concepts are included, making PROMs relevant over the entire course of a chronic disease.
Introduction
Patient-reported outcomes (PROs) constitute an essential part of health outcomes.1 On an individual level, the measurement of PROs is a crucial component of patient-centred care, building the basis for shared decision-making, patient empowerment, engagement and self-management.2 When used in routine clinical practice, PROs can positively influence the relationship between patients and their healthcare providers.3 4 PROs allow a structured assessment of the type and severity of symptoms that patients experience, as well as the impact of their disease and subsequent treatment on their life. Furthermore, aggregated PRO data can also be used to drive healthcare quality improvement initiatives on an institutional level; and for population health monitoring and reimbursement decision-making on a macro-level.2
Several outcome domains can only be measured in a self-reported manner. Examples are pain, fatigue, functioning in real-life situations and health-related quality of life.2 5 To accurately quantify patients’ experiences, patient-reported outcome measures (PROMs) are used. PROMs are defined as assessments of subjective health outcomes, based on responses provided directly by patients themselves without subsequent interpretation or alteration of the responses by health professionals (HPs) or anyone else.6 In the development and the selection of suitable PROMs, various methodological issues and measurement properties must be considered. These include the reliability, validity, responsiveness and interpretability of the respective instruments.7 8 PROMs have been increasingly applied in routine clinical practice and research in recent decades, particularly in the field of chronic diseases.9 10 In their work on PROs in rheumatoid arthritis (RA), van Tuyl and Michaud11 provided key examples of valid and reliable, commonly used PROMs in rheumatology. However, in order to address the impact of chronic diseases over their entire course, PROMs should be equally applicable and valid across a patient’s lifespan. Otherwise, adaptations for certain age groups may be required.3
In addition to the validity, reliability, responsiveness and acceptability of the measurements, PROMs need to cover what matters to patients.12 While a few studies have been conducted in rheumatology to explore whether PROMs cover the issues important to patients with different chronic autoimmune diseases, none of them focused specifically on young people.13–15 Inflammatory arthritis (IA) affects people of all age groups and PROMs play an important role to determine if a treatment is successful or not. However, to date, it has not been investigated whether PROMs commonly used in IA adequately include the perspectives of young people.
This need was recognised by the EULAR and an international task force on incorporating the perspective of young people with IA into outcomes assessment was established. A qualitative approach was adopted to explore the perspectives of young people with IA on the content and practical use of the most commonly used PROMs in a broader European context.
On this basis, the aims of our study were to explore whether commonly used PROMs in IA adequately cover the perspective of young people with IA from different European countries.
Methods
Study design and participants
A multinational qualitative study was conducted in Austria (AT), Croatia (HR), Italy (IT) and the Netherlands (NL). Young people with IA aged between 18 and 35 years, treated in rheumatology centres, with a disease duration of at least 1 year, and a formal diagnosis of one of three IA disease areas: (1) RA, juvenile idiopathic arthritis (JIA) and Still’s disease; (2) spondyloarthritis (SpA); (3) psoriatic arthritis (PsA), were included in the present study. All participants were contacted by telephone either by local investigators or patient organisations and appointments for participation in focus groups at the local centres or the location of the patient association (in the Netherlands) were made.
Qualitative research typically uses small sample sizes with a diverse range of participants to explore the personal experiences and views of people on a specific topic. Based on earlier studies,12 15 16 disease-specific focus groups were conducted in each country. Data saturation was defined as no new emergent concepts in at least three subsequent focus groups.17 18 In order to determine the number of emergent concepts in each focus group session, data analysis commenced when first transcripts were available and proceeded in parallel to data collection.19
Data collection
HPs and patient research partners (PRPs) co-developed, piloted and finalised the semistructured interview guide.21 It included questions on the perspectives and views of the participants on currently used PROMs which were selected based on a literature review and an online voting process. From 16 PROMs for RA, 19 PROMs for PsA and 15 PROMs for SpA, which were identified in the literature review, the study team in each country ranked the top five most commonly used PROMs based on their own experience. Subsequently, an agreement was made regarding five often used PROMs for each of the disease areas to be provided to the focus group members in printed form as a basis for discussion (table 1). The focus group moderator introduced these PROMs as examples. The interview questions are depicted in online supplemental table 1.
Supplemental material
PROMs selected for discussion in the focus groups
A focus group facilitation guide, including transcription instructions, was provided to support local centres while ensuring data collection was harmonised. The interviews were conducted by trained local investigators with experience in qualitative research data acquisition between March and August 2018, audio-recorded, transcribed verbatim and translated into English. Data coding and initial analyses were primarily undertaken by the first author (EM). During a face-to-face meeting of the EULAR task force members, the concepts were rephrased and organised into a scheme of higher and lower level concepts, with input from the local investigators, PRPs and HPs.
Data analysis
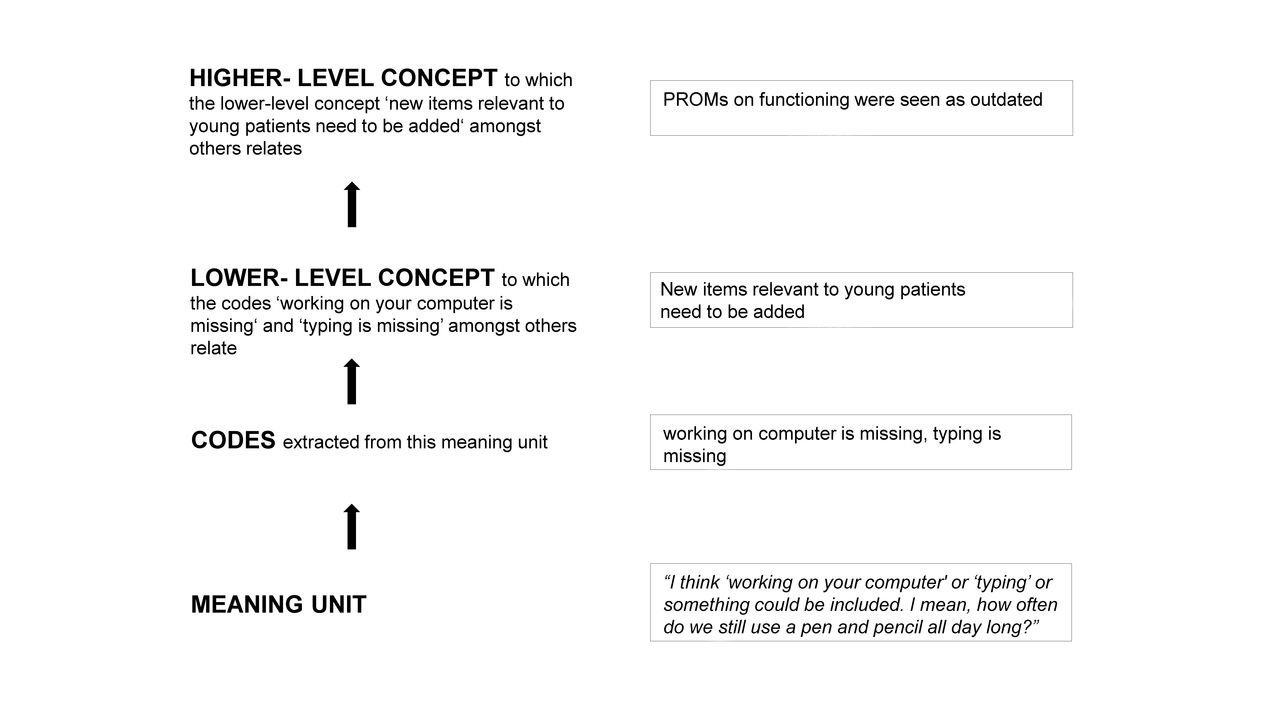
Descriptive statistics were used to summarise the characteristics of participants.22 Thematic analysis of qualitative data followed a modified form of ‘meaning condensation’,23 facilitated by using ATLAS.ti software24 to manage and organise the data. Thematic analysis comprised the following steps (figure 1): all transcripts were screened and read. Queries concerning content were sent to the country teams. Transcripts were then divided into meaning units (defined as specific parts of text, either a few words or a few sentences with a common meaning). Subsequently, initial codes were assigned to the meaning units. Codes could refer to the main topic of a meaning unit, but one meaning unit could also contain more than one code. Associated codes were then grouped into lower level concepts. In a final step, the lower level concepts were summarised into higher level concepts.

{kind=link}
Example outlining the different steps of the analysis from a meaning unit to lower and higher level concepts. PROMs, patient-reported outcome measures.
Rigour and accuracy of the analysis
Several strategies were used to enhance the trustworthiness of the qualitative data.25 Debriefing notes were recorded after each focus group interview. All local investigators who conducted focus groups checked the transcripts against the audio-recordings for accuracy. After analysing all focus group interviews, the results were discussed with researchers of all centres and reviewed by other task force members (PRPs and HPs who were not involved in the analysis of the transcripts). Finally, the consolidated criteria for reporting qualitative research Checklist26 was used to ensure the high quality of reporting the study results (online supplemental table 2).
Supplemental material
Patient and public involvement
PRPs (WO, IB, NC, MK, SS and T-CW) were part of the task force and included in all stages of the study. Furthermore, they will disseminate the results in lay language after publication.
Results
Participant characteristics
Saturation was reached after conducting 12 focus groups (online supplemental table 3), including 53 young people with a mean age±SD of 28±5 years (11 people with RA, 8 with JIA, 2 with Still’s disease, 15 with SpA and 17 with PsA; see table 2). In total, 18 hours and 22 min of discussion were recorded, resulting in 269 pages of transcript.
Supplemental material
Characteristics of participants
A general positive attitude towards PROMs
All participants expressed a general positive attitude towards PROMs and acknowledged their importance in clinical practice. Participants of all focus groups across all diseases described that PROMs had made a meaningful difference in their treatment, in that HPs addressed important issues which impacted on daily life, based on PROMs. Furthermore, PROMs were perceived as useful regarding self-management. One participant described this in the following way:
There are always questions like, ‘How have you been since the last check-up, have there been any changes’. And I like that each time when I am filling out those questionnaires. It is great, because I can be monitored in relation to the previous time. (Female, 22, SpA, Croatia)
Suggestions for adapting PROMs to young people
Forty-eight lower level concepts pertaining to suggested improvement of PROMs from the perspective of young people with IA were organised into six higher level concepts (table 3).
Six higher level and 48 lower level concepts of suggested adaptions of PROMs according to young people with IA
Higher level concept one addressed the need for additional information regarding the purpose of using PROMs. Young people in all countries and disease areas did not feel sufficiently informed about the value of PROMs and the reasons for collecting PROs in addition to clinical outcomes. They thought that they were asked to fill in PROMs because it was commonly done, for study reasons only or to keep them busy while waiting at the outpatient clinic. Participants in all 12 focus groups (100%) described uncertainties regarding the terminology used in the PROMs. They suggested simpler wording or clearer definitions, as young people were often confused, ashamed or even scared in case of difficulties to understand and would not ask for clarification. Some participants also pointed out that the value of PROMs seems limited, if the HPs have no time to discuss the PROM results with them and if the results are not available for all members of the healthcare team.
Furthermore, some participants mentioned that in order to be suitable to young people, some of the items within PROMs would need to be updated to ensure they are relevant for young people in current times (higher level concept two). In particular, this related to the PROMs which address functioning in daily life. A young man expressed it as follows:
I think it’s just an old people’s questionnaires, indeed. Maybe we have kind of an old people’s body, but with this you are really confronted with that. (Male, 22, SpA, the Netherlands)
Moreover, young people considered a large number of functional items too ‘easy’, for example, walking, while other issues related to mobility and physical activity, such as participating in physical activities similar to people without chronic diseases of the same age, or sitting in front of a computer for the entire day, are not covered at all. Likewise, eating was considered too easy, while preparing meals was missing. Some participants explained that reference to ‘easy’ items had incited fear, implying that someone might not be able to walk in later stages of IA.
Interestingly, participants in one focus group (RA/JIA/Still’s disease, the Netherlands) discussed the need for developing different PROMs for people of different ages. In comparison, all other participants suggested to extend the questionnaires to use the same PROMs for younger and older adults.
Issues important to young people should be added and regularly assessed (higher level concept three). These include problems with using technological devices, like smartphones and computers, difficulties with career plans, caring for others (for example, children), loss of friends, social life participation (such as going out in the evening), being excluded from physical activities at school and university, and challenges with regard to sexuality.
The fourth higher level concept referred to planned, erroneous reporting from young people. Some participants mentioned that they had purposely rated their pain, fatigue, disease activity or other symptoms differently from what they actually felt. Some of them had rated better, others worse than the situation had been experienced. The reasons behind this were diverse and included intentions to trigger changes in their disease management, often as an attempt to more accurately demonstrate how they had been feeling since their last visit, or even mirrored undisclosed fears. However, these reports may have a severe impact on an individual’s treatment, independent of the reason. A participant described the following example:
Well, I answer those questions more positively than how it goes, because I'm afraid they might think I'm depressed or something and send me to a psychiatrist. (Female, 25, SpA, the Netherlands)
Higher level concept five focused on individualising PROMs. Participants in the majority of the focus groups expressed that they would like to talk about their personal experience with IA and wished PROMs to be tailored to their individual needs and goals. In addition, length and comprehensiveness of PROMs were included in this higher level concept. Some participants requested that several issues important and meaningful for young people with IA should be adequately addressed in the PROMs and taken up and discussed in the subsequent interactions with interdisciplinary healthcare teams. Some of these participants even questioned the comprehensiveness of PROMs at all, since these tools can never encompass the entire spectrum and the full impact of IA on daily life. This theme was somewhat ambiguous, as other participants criticised the length of some PROMs, contradicting the suggestion of comprehensiveness. Nonetheless, single item scales were seen as insufficient and too narrow in focus, compared with tools which comprehensively assess the impact of a disease in daily life by young people in all countries and disease areas.
The sixth higher level concept covered the desire to use digital technology for data acquisition and access to PROM data. Participants were of the opinion that continuous monitoring could support young people in self-managing their health and well-being. Moreover, participants felt that by using technology, HPs would be more able to share the information about PROs with other HPs involved in the care of young people with IA.
Concepts of all disease areas and all countries
Eighteen (38%) of the lower level concepts were mentioned in all three disease areas and four countries (table 4, concepts in bold). Interestingly, the largest overlap was found in uncertainties regarding the terminology used in the PROMs and the need for clearer definitions and explanations. This concept was mentioned in all focus groups (100%). Consequently, these concepts may represent important generic perspectives of young people regarding PROMs.
Similarities and differences of concepts addressed on a disease specific and country level
Discussion
To our knowledge, this is the first study investigating the perspective of young people with IA on PROMs in a wider European context. Although the use of PROMs was highly valued by young people, participants across all countries and disease groups expressed that PROMs often fail to sufficiently encompass the daily challenges of young people with IA and are often experienced as ‘too easy’, for example, the Health Assessment Questionnaire27 and the Bath Ankylosing Spondylitis Functional Index.28 These PROMs lack more ‘difficult’ items referring to the instrumental activities of daily living29 which are essential for an independent life, especially at a younger age. In this context, item response theory (IRT) and computerised adaptive testing are used for the development of innovative patient-reported instruments, such as the Patient-Reported Outcomes Measurement Information System.30 In their study, Fries et al could show that physical function scales using a common metric or IRT-based items can result in greater responsiveness and precision across a broader range of functioning.31
Some issues were seen controversially, for example, the length/shortness versus comprehensiveness of PROMs or developing age-appropriate PROMs versus using the same PROMs across the life course. Although not all participants shared the same opinion, they agreed to complete PROMs no matter how long it would take, if they were adequately informed about the purpose of using these questionnaires and rating scales. The wish for more information, transparency and clarity regarding the reasons for using PROMs and their advantages in healthcare and research were also reported in previous studies with people of an older age.32–36 Therefore, simple and clear explanations for the use of PROMs can be seen as prerequisites in clinical practice and research to ensure that patients feel confident and provide accurate information.
It is known that chronic diseases influence major life-changing decisions related to social life, education, job, career choice and family planning.37 Participants in our study suggested that topics related to these areas should be discussed on a regular basis at the time of diagnosis and during subsequent follow-up visits with the healthcare team, for which PROMs could also be used. Interestingly, topics like sexuality, intimate relationships, family planning and work were not mentioned in all focus groups, potential reasons being the different cultural backgrounds or the assumption that these topics were not as relevant as others to be raised during consultations. Although it is advisable that private life aspects are increasingly explored among young people with rheumatic and musculoskeletal diseases (RMDs) including IA, sensitivity is required to prevent unnecessary pressure on young people.
Discussing the responses of PROMs together with patients, analysing these responses over time, and including them in shared decisions were highly valued by those participants who had experienced these processes before and were also described in the literature by Fautrel et al and Chewning et al.38 39 However, young people in all focus groups sometimes missed this valuable exchange of information due to time restrictions during consultations. Therefore, some participants in our study suggested using new technology to capture patient-reported data to a larger extent, in order to eventually meet this challenge. For example, patients could complete PROMs ahead of their consultation via a smartphone, tablet or computer, so that the results could be viewed and discussed in clinic. Collecting PROs electronically, as well as sharing and discussing them with healthcare providers in a remote way, might be of great importance during times of a pandemic, such as experienced due to COVID-19.
Many young people participating in our study also wished to talk about their personal experiences with their disease and expected PROMs to be tailored to their individual needs and goals. One outcome measure that is used both in clinical work and research to assess the effectiveness of treatment based on personally relevant goals is the Goal Attainment Scale.40 41 It is often used to define and evaluate personalised patients’ treatment goals that are meaningful to patients in a standardised way.42
Our study enabled us to gain deep insights into the perspectives of young people with IA by means of a qualitative study using focus group interviews in four European countries. We included on purpose researchers and patients from one country from Western (NL), Central (AT), Southern (IT) and Southeastern (HR) Europe in our study to ensure cultural diversity, but also include countries with different healthcare systems. Interestingly, concepts that were important from the participants’ point of view were the same, independent from the country data collected. Our results might thus be transferable to some other countries as well. However, there might still be differences between different countries, especially outside Europe, as only a limited number of countries were involved in our study. Future studies could include other countries and/or other disease areas using a quantitative survey that builds on our results.
To conclude, the results of our study will change the use of PROMs in young people with IA in clinical practice and research. Young people with IA described a substantial potential for improving PROMs. First, optimising the current use of PROMs in their present form; and second, the potential for adapting PROMs so that they meet the current needs of young people. Our study provides the basis for further research in the field of outcomes research, since the assessment of young people’s perspectives should reach beyond the issues covered in PROMs used within rheumatology. Accordingly, young people with IA and other RMD-related conditions should be involved in the development of new PROMs and the potential adaptation of existing PROMs, to ensure that important concepts are included and address the entire course of a chronic disease. In broader terms, our findings may also be relevant to the use of PROMs in the context of other chronic diseases where individual needs, the perception of health and experience of symptoms vary during the course of life.
Supplemental material
Supplemental material
Supplemental material
Supplemental material
Supplemental material
Supplemental material
Supplemental material
Supplemental material
Acknowledgments
We would like to thank all young people who took part in this study for sharing their valuable perspectives. We also thank Dr Elena Picchiassi, Ms Linda van Nieuwkoop, Dr Mirna Reihl and Ms Gordana Maligec for their support in data collection.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Twitter @Stiddyo, @ivan_padjen, @kouloumasm, @ElenaNikiUK, @SimonRStones
Contributors EM, PS, AA, IP, WO, SR, IB, NC, LG, MK, EN, SS, T-CW and TAS were responsible for the study conceptualisation and design. EM, IP, WO and AA conducted the focus groups. Data coding and initial analyses were primarily undertaken by the first author (EM). EM, PS, AA, IP, WO, SR, IB, NC, LG, MK, EN, SS, T-CW and TAS were involved in interpreting the data, writing and reviewing the manuscript. EM was responsible for the visualisation, including tables and figure. WO, IB, NC, MK, SS and T-CW are patient representatives/advocates.
Funding This project was funded by the EULAR; grant number CLI100.
Competing interests PS reports grants from AbbVie, outside the submitted work; IP reports personal fees from Abbvie, personal fees from Novartis, personal fees from Roche, personal fees from Sandoz, personal fees from Sanofi, outside the submitted work; SR reports personal fees from AbbVie, personal fees from Eli Lilly, personal fees from MSD, personal fees from Novartis, personal fees from Sanofi, personal fees from UCB, outside the submitted work; LG reports grants and personal fees from Amgen, grants from Galapagos, grants and personal fees from Janssen, grants and personal fees from Lilly, grants and personal fees from Pfizer, grants from Sandoz, grants from Sanofi, personal fees from AbbVie, personal fees from BMS, personal fees from Biogen, personal fees from Celgene, personal fees from Gilead, personal fees from Novartis, personal fees from Samsung Bioepis, personal fees from Sanofi-Aventis, personal fees from UCB, outside the submitted work; EN reports personal fees from Abbvie, personal fees from Celltrion, personal fees from Gilead, personal fees from Lilly, personal fees from Pfizer, personal fees from Sanofi, outside the submitted work; SS reports personal fees from Actelion, personal fees from CISCRP, personal fees from Janssen, personal fees from Parexel, outside the submitted work; TAS reports grants from AbbVie, grants and personal fees from Roche, personal fees from Sanofi Genzyme, personal fees from Takeda, outside the submitted work.
Patient consent for publication Not required.
Ethics approval The study was approved by the local ethics committees including the Ethics Committee of the Medical University of Vienna, Austria EK Number 2117/2017. All participants were informed about the purpose and procedures of the study and gave their written informed consent in accordance with the Declaration of Helsinki.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement No data are available. This is a qualitative study and therefore the data generated are not suitable for sharing beyond that contained within the report. Further information can be obtained from the corresponding author.