Article Text

Abstract
Objectives Investigate if low cardiorespiratory fitness (CRF) was associated with and acted as a mediator of excess all-cause mortality rate in persons suffering from rheumatoid arthritis (RA) compared with the general population.
Methods All-cause mortality was analysed using Cox regression modelling in patients with RA (n=348) and controls (n=60 938) who took part in the second (1995–1997) and third (2006–2008) waves of the longitudinal population-based Trøndelag Health Study in Norway. A mediation analysis was performed to investigate if excess relative risk of mortality in RA was mediated by low estimated CRF (eCRF).
Results During the follow-up until 31 December 2018 (mean 19.3 years), the mortality rate among patients with RA (n=127, 36.5%) was higher than among controls (n=12 942, 21.2%) (p<0.001). Among controls and patients with RA, 51% and 26%, respectively, had eCRF above the median for their age and sex (p<0.001). The final Cox model included RA status and eCRF, adjusted for hypertension, body mass index, smoking, cholesterol, diabetes and creatinine. eCRF below median for sex and age category was associated with increased mortality (p<0.001). The total excess relative risk of mortality in patients with RA was 28% (95% CI 2% to 55%, p=0.035), in which RA itself contributed 5% and the direct and indirect contributions of low eCRF accounted for 23%.
Conclusions Low eCRF was an important mediator of the increased all-cause mortality rate found in RA. Our data indicate that patients with RA should be given advice to perform physical activity that increases CRF, along with optimised treatment with antirheumatic drugs, from the time of diagnosis.
- arthritis
- rheumatoid
- epidemiology
- outcome assessment
- health care
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Key messages
What is already known about this subject?
Low cardiorespiratory fitness (CRF) is independently associated with all-cause mortality in the general population.
Patients suffering from rheumatoid arthritis (RA) have increased mortality rates compared with the general population.
What does this study add?
Participants with RA had a 28% excess relative risk of mortality compared with controls in the large population-based Trøndelag Health Study.
In mediation analysis, RA itself contributed 5% and the direct and indirect contributions of low estimated CRF accounted for 23% of this excess mortality risk.
How might this impact on clinical practice?
Together with optimal medical treatment, both information and implementation of strategies for improving CRF should be introduced early in the management of RA to reduce the risk of premature mortality.
Introduction
Rheumatoid arthritis (RA) is a common chronic systematic rheumatic disease affecting joints, tendons, bursae and internal organs including the cardiovascular and respiratory systems.1 In Norway, RA has a prevalence of 768/100 000 (women 1003/100000, men 513/100 000).2 The prevalence of RA is quite stable around the world, around 0.5%–1%.1
Patients with RA often show more unfortunate cardiovascular risk profiles, with higher frequencies of the metabolic syndrome and smoking compared with the general population.3 4 In addition, chronic inflammation in RA is regarded as an important contributor to accelerated atherosclerosis leading to increased cardiovascular disease (CVD) that eventually leads to increased rates of premature death in RA.5–11 There are indications that improved medical treatment with new biological disease modifying antirheumatic drugs (DMARDs) and targeted synthetic DMARDs in addition to use of conventional DMARDs at higher doses and an earlier disease stage led to reduced inflammation,12–14 which in turn has contributed to reduced mortality in patients with RA in short-term studies.15 16 However, robust evidence of improved survival rates in long-term studies in persons with RA is lacking.17
There is strong evidence that the cardiorespiratory fitness (CRF) level affects cardiovascular health, and low CRF is a stronger predictor of adverse cardiovascular outcomes than traditional risk factors.18 CRF is measured as a person’s maximum oxygen uptake (VO2max), and is now regarded as a clinical vital sign.18 Exercise training, particularly at high intensities, leads to improved CRF.19 CRF is, therefore, an important modifiable risk factor because it may be improved by increasing relevant physical activity (PA).20
Studies have shown that patients with RA have reduced CRF compared with the healthy population,21–23 whereas PA interventions that improve CRF are associated with increased function and reduction of cardiovascular risk in RA.24 25
The gold-standard method to measure VO2max is by cardiopulmonary exercise testing (CPET) either on a treadmill or bicycle ergometer.18 With gradually increasing workload, oxygen expenditure increases until the oxygen ventilation curve flattens as the person reaches physical exhaustion. VO2max is the measured level of oxygen ventilation at this point. CPET is a resource-intensive method. Various mathematical models have therefore been developed to estimate VO2max (eCRF) without the need for a physical test.18 26–28 One example is the eCRF equation developed by regression analysis with the CPET results from 4260 participants in the third wave of the Trøndelag Health Study (HUNT3) as the dependent variable. The predictors in this model are age, gender, resting heart rate and waist circumference, as well as information about frequency, duration and intensity of PA performed by the participants.26
High eCRF can counteract the increased cardiovascular risk factor clustering caused by long sedentary time,29 and in one study the risk of acute myocardial infarction (MI) in women was inversely associated with the level of eCRF.30 In addition, several studies have shown that eCRF serves as an independent predictor of mortality in the general population.28 31 32 A previous study showed that a 3.5 mL/(min x kg) higher eCRF was associated with a 21% lower HR for CVD mortality in both men and women.31
Despite the strong association between low CRF and mortality found in the general population, evidence is still lacking for importance of the same association in patients with RA. To our knowledge, no population-based studies have analysed CRF level in relation to excess mortality in an RA population. Focus so far has rather been on medication reducing inflammation to prevent excess mortality in RA, and thereby perhaps overlooking the potential additional importance of low CRF as a mediator of increased mortality rates in RA. The hypothesis of this study was that low CRF contributes to the increased mortality in patients with RA compared with the general population. The aims were to investigate if low eCRF was associated with and acted as a mediator of increased all-cause mortality in patients with RA, using data from a large population-based cohort.
Methods
Participants
HUNT is a longitudinal population-based health study using an open cohort design. All present inhabitants ≥20 years of age in the northern region of Trøndelag county in Norway are invited to each wave of the study, independent of whether they have previously participated in HUNT. In this study data from the second (HUNT2, 1995–1997, n=65 202, 69.5% of invited) and third (HUNT3, 2006–2008, n=50 787, 54.1% of invited) waves were used.33 Data from the first wave (HUNT1, 1984–1986) could not be included because there was no question regarding RA. All participants in HUNT provided written informed consent.
Based on information in hospital case files, a previous study identified those with a valid RA diagnosis (n=546) out of all participants in HUNT2 and HUNT3 who self-reported RA.2 The standardised 2010 American College of Rheumatology/European League Against Rheumatism (EULAR) classification criteria for RA were used during diagnosis validation.34 Those with uncertain RA, given an RA diagnosis after HUNT3 and/or having psoriatic arthritis, juvenile inflammatory arthritis, ankylosing spondylitis or other forms of inflammatory arthritis, were excluded. Following exclusion of participants with missing variables for eCRF calculation, 348 patients with RA (235 women and 113 men) and 60 938 controls were included (figure 1).
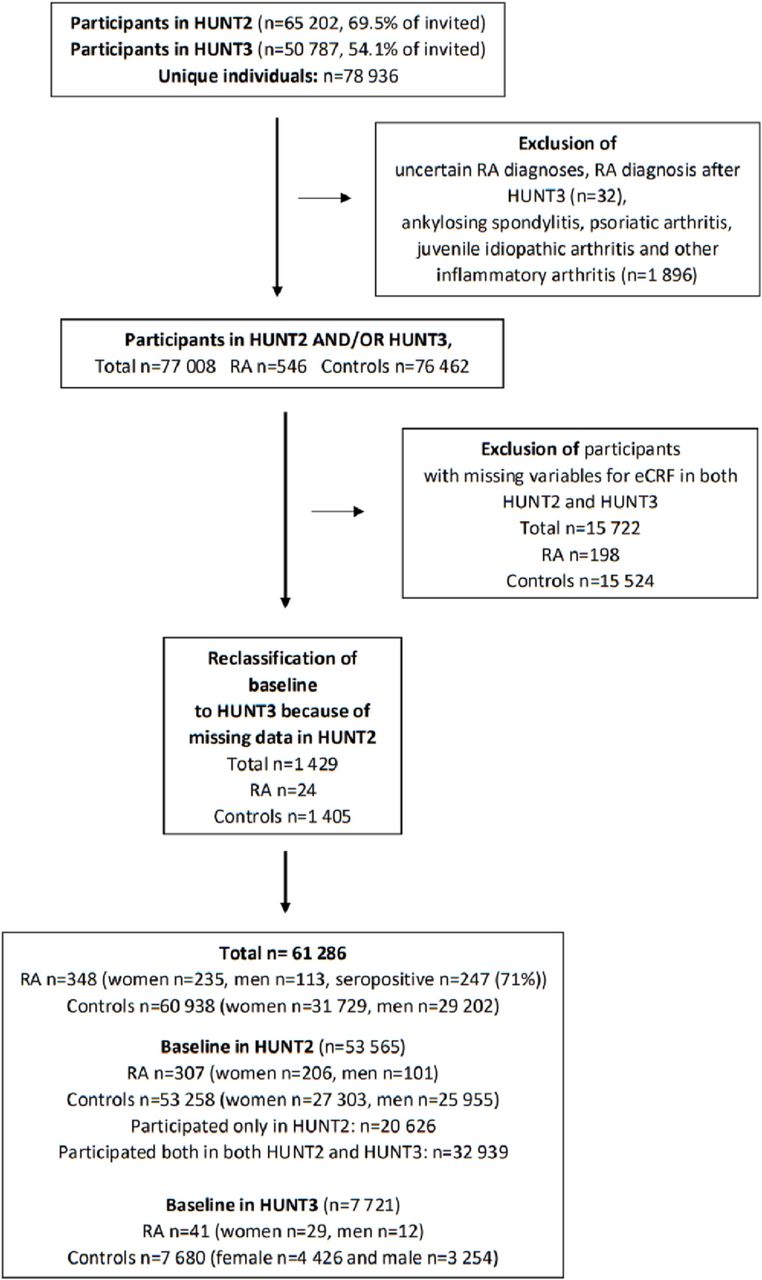
Recruitment to the study. All inhabitants ≥20 years of age are invited to participate. eCRF, estimated cardiorespiratory fitness; HUNT2 and HUNT3, the second and third wave of the longitudinal population-based Trøndelag health study; RA, rheumatoid arthritis.
Variables
The following variables and definitions were used: eCRF (mL/(min x kg)) in controls and patients with RA was calculated as previously described and detailed in online supplemental data 1.26–28 Body mass index (BMI) was divided into three categories: <18.5, 18.5–24.9, >30.0 kg/m2; hypertension (yes/no): systolic blood pressure ≥140 and/or diastolic blood pressure ≥90 mm Hg and/or self-reported use of antihypertensive medication; previous CVD (yes/no): self-reported stroke and/or angina and/or MI; smoking: self-reported never, previous or present smoking; diabetes (yes/no): self-reported diabetes and/or the use of antidiabetic medication and/or having a non-fasting blood-glucose level >11 mmol/L; creatinine (µmol/L); total cholesterol (mmol/L); seropositive RA: presence of rheumatoid factor and/or anticitrullinated peptide antibody; duration of RA: three categories: <3 years, 4–9 years and ≥10 years.
Supplemental material
Data from HUNT2 and HUNT3 were linked with the Norwegian Cause of Death Registry,35 which registers information about all deaths of Norwegian citizens in Norway or abroad.
Patient and public involvement
There was no direct patient and public involvement (PPI) involvement in the design of this study. Two PPI representatives will help select and design material for dissemination of results to their peers and patient groups.
Statistics
Data are given as counts and percentages or mean with SD. P values <0.05 were regarded significant. Statistical analyses were performed using Stata (V.15.1, StataCorp). Normal distribution of continuous variables was evaluated using histograms.
Because HUNT2 and HUNT3 took place approximately 11 years apart, baseline characteristics of the participants could have changed between them. Baseline comparisons for patients with RA and controls were therefore performed separately for HUNT2 and HUNT3, using χ2 tests or t-tests.
In brief, the associations of RA and low fitness were analysed using Cox regression. Adjustments for potential confounders were added in steps to better permit evaluation of whether the associations found for RA and low fitness were independent from each other and from the adjustment variables. To investigate the total excess relative risk of mortality in RA and whether it was mediated through low fitness, a Cox regression-based mediation analysis was performed. The details of the analyses are described in the following paragraphs.
All-cause mortality in patients with RA and controls was analysed employing Cox proportional hazard regression modelling in several steps as detailed below. Age was used as the time variable, thereby ensuring that participants were compared with other participants of the same age in all models. This design safeguards against introducing bias due to age differences between patients with RA and controls. The analyses were stratified by sex, and entry was the date for the first participation in HUNT (baseline), that is, either HUNT2 or HUNT3. For those who participated twice, the first observation with complete data for the fully adjusted model (Step 3) was considered the baseline observation; thus those who took part in both HUNT2 and HUNT3 but had missing variables for HUNT2 were included with their baseline defined as HUNT3. For participants in both HUNT2 and HUNT3, relevant variable values were updated in HUNT3. Participants were followed from their baseline until they died, or observation ended on 31 December 2018.
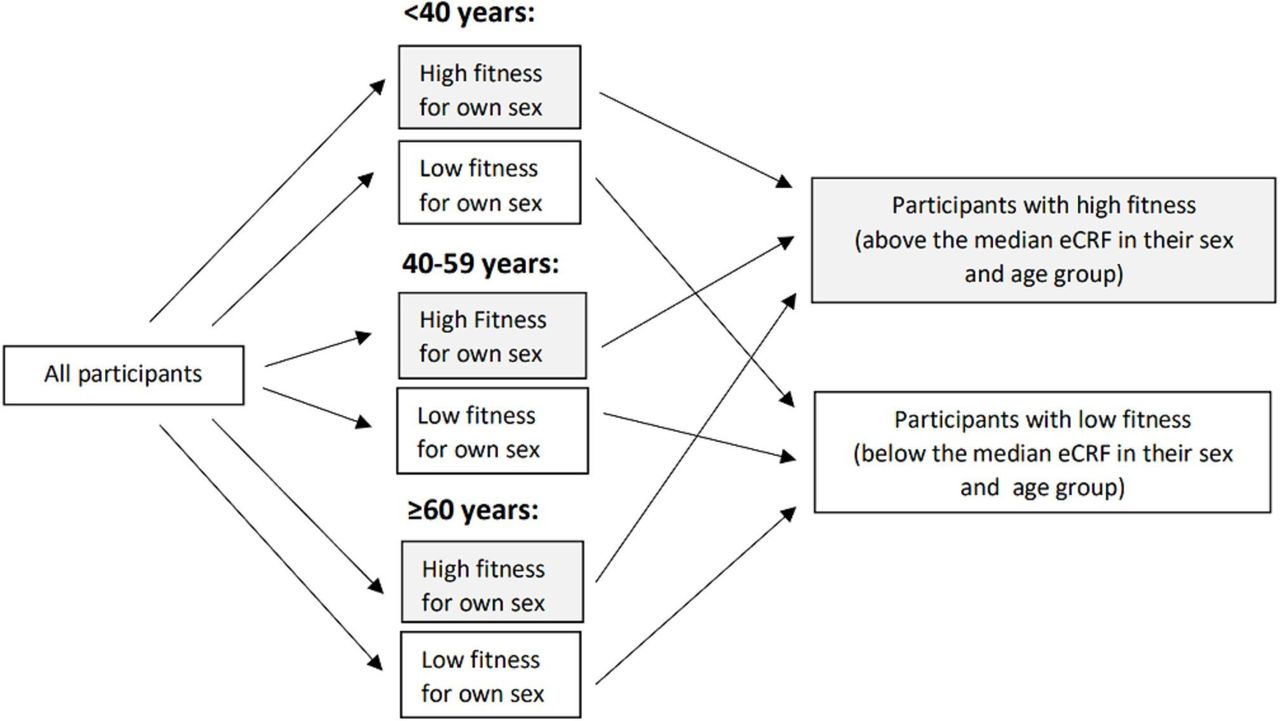
In the main analysis, eCRF was categorised as above or below the median for each participant’s sex and age group (<40 years, 40–59 years, ≥60 years, variable denoted eCRF-dichotomous, using eCRF above the median as reference group) (figure 2). This was done because fitness is strongly associated with age and significantly higher in men than women. Using eCRF-dichotomous in the main model had two reasons: The Step 3 Cox model was directly comparable to the model used to test eCRF as a mediator of excess mortality in RA (second study aim), for which using more than two eCRF categories was not possible; and because there is some variability in measured CRF compared with eCRF.

Categorisation of fitness level above or below median eCRF for their sex and age group. eCRF, estimated cardiorespiratory fitness.
The first analytic step (Step 1) consisted of univariable models for RA status (yes/no) (Step 1a) and eCRF-dichotomous (Step 1b) for the relevant age group and sex, respectively. Step 2 was a bivariable model including both RA status and eCRF-dichotomous. Step 3 was a multivariable model including RA status, eCRF-dichotomous and the following adjustment variables: hypertension, BMI, smoking status, total cholesterol, diabetes status and serum creatinine. They were chosen based on published associations with mortality.
Because missingness was very low (table 1), the analysis was performed on complete cases. The proportional hazard assumption was evaluated using Stata’s phtest based on Schoenfeld residuals. For models with violation of the proportional hazard assumption, a corresponding flexible parametric survival model was fitted. If the HRs (mean with 95% CI) were similar, the Cox models were considered acceptable. Linearity of continuous variables was evaluated using Martingale residuals. Models were compared using the Akaike and Bayesian information criteria (AIC and BIC), where a lower numerical value indicates better fit.
Baseline characteristics*
Two sensitivity analyses for the Step 3 (adjusted) model were performed to ascertain whether dichotomisation of eCRF introduced bias. First, categorisation was performed in tertiles for each participant’s sex and age group (variable denoted eCRF-tertiles, using the higher eCRF tertile as reference group). Another sensitivity analysis used eCRF as a continuous variable, denoted as eCRF-continuous. A third sensitivity analysis included adjustment for previous CVD in addition to the adjustments used in the Step 3 model.
To investigate whether an increased mortality rate in RA is mediated by low eCRF, we performed a mediation analysis using the Stata package med4way.36 In this Cox regression-based analysis, the total effect on mortality of having RA is calculated as the total excess relative risk of mortality. This excess risk was then split into three paths and the mediator effect of eCRF was calculated fixing eCRF-dichotomous to low, that is, below the sex-specific and age-specific median. In other words, the mediation analysis sought to answer the following question: How much of the association of RA with all-cause mortality is mediated by low eCFR? The three different paths were the controlled direct effect of RA on all-cause mortality (ie, when all other variables are adjusted for), the pure indirect effect of RA via eCRF below the median, and the portion attributable to interaction between RA and eCRF below the median when all other variables are adjusted for (figure 3). The mediation model used Cox regression based on the Step 3 (adjusted) model above. eCRF was not used as a continuous variable in the mediation analysis because there is no clear definition of what the relevant value of eCRF would be at which to analyse the mediation effect. As a sensitivity analysis, the mediation analysis was also performed after inclusion of previous CVD as an additional adjustment variable.

{kind=link}
{kind=link}
{kind=link}
Mediation model. (A) The model is based on the Step 3 adjusted Cox regression model and shows how much of the association of RA with all-cause mortality was mediated by low fitness (eCRF below median). (B) Details from results of the mediation analysis. eCRF below median, estimated cardiorespiratory fitness below the sex-specific and age-specific eCRF median using age groups <40 years, 40–59 years or ≥60 years.
Results
The baseline characteristics and results from comparisons between patients with RA and controls for participants with baseline in HUNT2 (RA n=307, controls n=53 258) and HUNT3 (RA n=41, controls n=7680) are presented in table 1. BMI was not significantly different between patients with RA and controls for participants with baseline in HUNT2, but the patients with RA with baseline in HUNT3 had significantly higher BMI than controls. Baseline total cholesterol was significantly higher in patients with RA than controls in HUNT2, but not in HUNT3. Higher frequencies of patients with RA were smokers or previous smokers in HUNT2, and had hypertension or previous CVD compared with controls at both baseline time points (table 1).
Out of 348 patients with RA, 247 (71.0%) were seropositive, 93 (26.7%) were seronegative and 8 (2.3%) had unknown serologic status. RA disease duration (<3 years, 4–9 years and ≥10 years) was 27.9%, 49.7% and 19.8%, respectively, and 2.6% lacked information about the duration of RA.
Mean follow-up was 19.3 years (min. 0.2 to max. 23.4 years), during which 13 069 participants died. The all-cause mortality rate was significantly higher among patients with RA (n=127, 36.5%) compared with controls (n=12 942, 21.2%) (p<0.001). Among controls and patients with RA, 51% and 26%, respectively, had baseline eCRF above the median for their age and sex (p<0.001).
Low fitness was strongly associated with mortality in both groups. Of the 127 patients with RA who died, only 4% (n=5) belonged to the high fitness category, in contrast to 8.8% (n=12 942) of the controls (p=0.054). Total time at risk was 1 158 878 person years, that is, 5596 person years for patients with RA and 1 153 281 person-years for controls.
Detailed results from the stepwise Cox regressions and sensitivity analyses are given in table 2.
Results from Cox regression analyses for all-cause mortality
In the univariable Step 1 Cox analyses, either having RA (p=0.036) (Step 1a) or having eCRF below the median (p<0.001) (Step 1b) were associated with increased mortality. In the bivariable Step 2 model with RA and eCRF-dichotomous, RA status became non-significant (p=0.12) whereas eCRF below the median remained significant (p<0.001). This finding is compatible with the hypothesis that part of the excess mortality risk of RA in the univariable model was in fact explained by the lower eCRF among patients with RA compared with controls. Following adjustment for hypertension, BMI, smoking, total cholesterol, diabetes and creatinine in the Step 3 model, eCRF below the median remained significant (p<0.001) (table 2). The sensitivity analyses showed that results and model fit using eCRF-dichotomous in Step 3 (AIC=213 717.9 and BIC=213 829.7) were comparable to models using eCRF-tertiles (AIC=213 714.4 and BIC=213 835.5) and better than eCRF as a continuous variable (AIC=213 768.0 and BIC=213 879.8). Inclusion of adjustment for previous CVD in the third sensitivity analysis had minimal influence on the Cox regression results (table 2).
Some adjustment variables violated the proportional hazard assumption. However, the coefficients hardly changed when using a flexible parametric survival model instead, so the Cox models were considered acceptable.
Results from the mediation analysis are given in figure 3. The results showed that having an eCRF below the sex-specific and age-specific median if one suffered from RA acted as a mediator for mortality, which explained 23% (4% plus 19%) of the total increased risk of all-cause mortality of 28%. Thus, the effects of low eCRF exceeded the isolated contribution of RA itself of 5% in this setting. In the sensitivity analysis with additional adjustment for previous CVD, the total increased risk of all-cause mortality was 27%, of which 21% were explained by having an eCRF below the sex-specific and age-specific median. Thus, previous CVD had little influence on the results.
Discussion
This study showed that patients with RA had significantly increased long-term all-cause mortality rates compared with controls. When adjusting for other risk factors for mortality, the excess relative risk of 28% was partly associated with the RA disease itself, but the major part, that is, 23%, was mediated by low eCRF combined with the interaction between RA and low eCRF. The contribution of the interaction to the total increased relative risk of mortality was not significant (p=0.077), but this is likely a false-negative result due to low power because very few of the patients with RA who died had eCRF above the median. However, residual confounding due to missing adjustment variables cannot be excluded. Because eCRF is modifiable, results from this study are particularly interesting as increasing PA that leads to improved CRF may translate to reduced mortality rates in patients with RA.
Already at the turn of this century, tests of physical function (ie, walk test and grip strength) in addition to patient-reported measures reflecting physical function (ie, the modified health assessment questionnaire and the patient global assessment) were described as predictors of mortality, whereas radiographic change, RF positivity and inflammation markers were not.37–41 In the following years, new treatment strategies like ‘Treat to target’ with new drugs have been in focus.12 42 An unintended consequence might be that registration of inflammation levels and radiographic changes may have been performed almost at the expense of other outcomes like CRF and other measures of physical function.
New and better drugs increase quality of life, reduce inflammation and radiographic change, and thereby help patients with RA exercise; however, drugs alone do not increase CRF. There is no doubt that higher CRF is associated with longer survival in the general population,18 28 31 43 and the present study gives evidence that this also applies to patients with RA. Thus, increasing fitness may be an important tool for reduction of preterm mortality, counteracting the increased age-related decline in eCRF described in RA.44 In addition to early medical treatment, encouragement and information about suitable PA and exercise training, in particular at high intensity,24 should therefore be an obligatory part of RA treatment strategies from the time of diagnosis.
An increasing focus on PA is reflected in the latest 2017 EULAR recommendations for PA in arthritis. They state that arthritis patients should follow the same recommendations for PA as the general population and that PA in RA is safe.45 46 Perhaps because of lacking evidence, The EULAR recommendations for prevention of CVD recommend PA because it might reduce inflammation and prevent CVD, but CRF and related terms are not mentioned.47 The present finding that low eCRF clearly acts as a mediator of excess mortality in RA contributes to the evidence supporting improvement of CRF as an important tool for preventive care also in patients with RA.
Some studies have indicated that the mortality gap between patients with RA and the general population is narrowing.15 16 However, comparison of RA populations diagnosed in different time periods using different criteria and various follow-up strategies may result in a false impression of a narrowing mortality gap.6 Cigarette smoking is associated with earlier debut of seropositive and more severe RA and is a well-known risk factor for atherosclerosis and increased mortality rates.4 48 One may ask whether the overall observed reduction of smoking in most industrialised countries has a more positive effect in patients with RA compared with the general population and is possibly contributing to narrowing of the mortality gap. However, low eCRF remained a strong risk factor for mortality in our study after adjustment for smoking and other variables associated with mortality and CVD.
Access to lifestyle-related and other relevant adjustment variables in HUNT, and the long follow-up should be regarded as strengths of our study. The low number of patients with RA may represent a weakness, but the very large population-based control group reduces selection bias and thereby improves the validity of the results.
Another strength of the present study is that RA diagnoses were confirmed from medical records and not based on self-report or diagnostic codes in various registries.2 Given that many of our study participants were diagnosed with RA several years ago and that their eCRF was not recently updated, it may be argued that the findings are no longer relevant. A previous study from our group found that patients with RA who performed CPET in 2017 were deconditioned compared with the healthy population and use of various conventional and biological DMARDs was not associated with CRF.21 The results are therefore probably relevant for today’s RA population as well, even if there have been large changes in medication and treatment strategies.
Using eCRF instead of the measured CRF from CPET may be regarded as a limitation of this study. However, using CPET may introduce selection bias, as those more used to PA may be more motivated for participation. Using eCRF calculated from other data makes it possible to include a wider range of participants. Furthermore, performing CPET in such a large population-based study would have been practically and economically impossible.
Because HUNT has an open cohort design, participants in our study had different baselines. This permitted inclusion of more participants and thereby provided higher statistical power, as well as the possibility of updating the data for those who participated twice. However, we cannot exclude that studying participants having different baselines could have influenced the results.
In conclusion, this study showed that low CRF was an important mediator of the increased mortality found in patients with RA. In addition to optimal medical treatment, focus on improvement and follow-up of CRF should be an integral part of standard treatment of RA already from the time of diagnosis.
Acknowledgments
The HUNT Study (Trøndelag Health Study) is a collaboration between the HUNT Research Centre (Faculty of Medicine and Health Sciences, NTNU-Norwegian University of Science and Technology), the Nord-Trøndelag County Council, the Central Norway Health Authority and the Norwegian Institute of Public Health.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Contributors Study conception and design: MHL, MH, UW and VV. Acquisition and analysis of data: MHL and VV. Interpretation of data: MHL, MH, UW and VV. Drafting the manuscript: MHL and VV. Revising the manuscript critically for important intellectual content: MH, UW and VV. All authors approved the final version of the manuscript.
Funding This project was funded by a grant to Marthe Halsan Liff from The Central Norway Regional Health Authority, allocated via The Liaison Committee for Education, Research and Innovation in Central Norway (2016/29014).
Competing interests None declared.
Patient consent for publication Not required.
Ethics approval Approval for HUNT was obtained from the Norwegian Data Safety Authorities and the Norwegian Department of Health. The Regional Committee for Medical and Health Research Ethics approved the present study (4.2009.1068 and 2018/1149), which was performed in compliance with the Declaration of Helsinki.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement Data may be obtained from a third party and are not publicly available. Data from HUNT are available on reasonable request from the HUNT Research Centre (www.ntnu.edu/hunt/data), following approval from the Regional Research Ethics Committee. However, restrictions apply to the availability of the data for the present paper, which were used under licence for the current study and are not publicly available in accordance with Norwegian law.