Article Text

Abstract
Objective To explore the effect of apps measuring patient-reported outcomes (PROs) on patient–provider interaction in the rheumatic diseases in an observational setting.
Methods Patients in the Swiss Clinical Quality Management in Rheumatic Diseases Registry were offered mobile apps (iDialog and COmPASS) to track disease status between rheumatology visits using validated PROs (Rheumatoid Arthritis Disease Activity Index-5 score, Bath Ankylosing Spondylitis Disease Activity Index score, Routine Assessment of Patient Index Data-3 score and Visual Analogue Scale score for pain, disease activity and skin symptoms). We assessed two aspects of patient–provider interaction: shared decision making (SDM) and physician awareness of disease fluctuations. We used logistic regressions to compare outcomes among patients who (1) used an app and discussed app data with their physician (app+discussion group), (2) used an app without discussing the data (app-only group) or (3) did not use any app (non-app users).
Results 2111 patients were analysed, including 1799 non-app users, 150 app-only users and 162 app+discussion users (43% male; with 902 patients with rheumatoid arthritis, 766 patients with axial spondyloarthritis and 443 patients with psoriatic arthritis). App users were younger than non-app users (mean age of 47 vs 51 years, p<0.001). Compared with non-app users, the app+discussion group rated their rheumatologist more highly in SDM (OR 1.7, 95% CI 1.1 to 2.4) and physician awareness of disease fluctuations (OR 2.0, 95% CI 1.3 to 3.1). This improvement was absent in the app-only group.
Conclusion App users who discussed app data with their rheumatologist reported more favourably on patient–provider interactions than app users who did not and non-app users. Apps measuring PROs may contribute little to patient–provider interactions without integration of app data into care processes.
- patient-reported outcome measures
- outcome and process assessment
- health care
- health services research
Data availability statement
Data are available upon reasonable request.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Key messages
What is already known about this subject?
Pilot studies of apps for measuring patient-reported outcomes (PROs) have found that use of such apps in clinical practice is feasible and acceptable to both patients with rheumatic diseases and their physicians.
What does this study add?
This is one of the first studies to evaluate the effect of apps measuring PROs on quality of care in rheumatic diseases in an observational setting.
Only 55% of app users reported discussing their app results with their rheumatologist.
Patients who used an app and discussed the results with their rheumatologist during clinic visits reported increased physician engagement in shared decision making and following the course of their disease over time, compared with non-app users. However, patients who used an app without discussing the results did not report improvements in these aspects of care relative to non-app users.
How might this impact clinical practice?
When implementing apps or other eHealth tools that measure PROs in clinical practice, offering patients and healthcare providers guidance on how to make use of the PRO information during consultations and in daily life may help to maximise the beneficial impacts of these interventions.
Introduction
Regular monitoring of disease outcomes (including disease activity, progression, and impact of the disease on patient functioning and quality of life) is recognised as important in the management of inflammatory rheumatic musculoskeletal diseases (RMDs).1–5 However, in practice, many patients visit their rheumatologist infrequently6 7 due to limited access to rheumatologists because of geographical or financial constraints or stable disease.8–10 This may contribute to inadequate monitoring of disease outcomes and delays in detecting and treating flares, resulting in increased progression of disease11 and unaddressed residual symptoms of importance to patients.12–14
Patient-reported outcome (PRO) measures are surveys used to assess patient perceptions of symptoms, disease and health status, and quality of life.15 Mobile apps incorporating PROs can contribute to filling the gap between rheumatology visits—patients can use such apps to track disease and health status between appointments, providing increased documentation of disease severity, treatment effectiveness and patient quality of life. This additional information can help guide disease management and treatment decisions and increase physician awareness of patient-perceived health status between visits.4 Disease monitoring apps incorporating PROs have been developed for patients with rheumatoid arthritis (RA), juvenile idiopathic arthritis and lupus.16–20
The Institute of Medicine’s 2001 report, Crossing the Quality Chasm: A New Health System for the 21st Century, identified six areas of priority for improving the quality of care in healthcare systems: healthcare should aim to be safe, effective, patient-centred, timely, efficient and equitable.21 Apps incorporating PROs have the potential to make care in RMDs more patient-centred and effective. Patient-centred care is defined as care that is responsive to patient needs, preferences and values.21 Use of apps incorporating PROs might promote patient-centred care by impacting how patients interact with their rheumatology healthcare providers. Regularly measuring PROs may empower patients to become more involved in their own care and facilitate patient–provider communication and shared decision making (SDM). Sharing PRO information with a rheumatology healthcare provider via an app may also heighten patients’ trust that the provider is aware of changes and fluctuations in their disease over time. Effective care is defined as care that is consistent with evidence-based guidelines and improves health outcomes.21 Use of apps incorporating PROs may increase the effectiveness of care by promoting management of rheumatic diseases that is consistent with the principles of treat to target and tight control of disease.4 5 Apps incorporating PROs can provide more information to guide treatment decisions and to promote timely treatment intensification in response to flares, thus leading to better control of disease activity and improved health outcomes. Currently, evidence on the benefits of apps using PROs in clinical practice is very limited. In this observational study, we evaluated the impact of implementing apps which measure PROs on patient–provider interaction (patient-centeredness of care) and disease management (effectiveness of care).
Patients and methods
The study setting was the Swiss Clinical Quality Management in Rheumatic Diseases Registry (SCQM), which follows patients with RA, psoriatic arthritis (PsA), axial spondyloarthritis (axSpA) and undifferentiated arthritis receiving rheumatology care in Switzerland. The SCQM was created in 1997 to track health outcomes of patients with RA and to support physicians with the management of their patients’ disease.22 Participating providers include university and other large hospitals and private rheumatology clinics. Physicians collect data on patients' disease and overall health status and medications during routine clinic visits; study visits usually occur at least once a year. Starting in 2016, two apps, iDialog monthly and COmPASS II,23 were implemented in the registry as a quality improvement initiative to allow registry patients to document their health status and medication intake between clinic visits. In January 2019, iDialog was replaced with an updated app renamed as MySCQM. New enrolments in ComPASS were halted, but existing ComPASS users could continue to use the same app. Thus, we believe the introduction of MySCQM had minimal impact on the behaviour of app users, since iDialog users were all transitioned to MySCQM and COmPASS users continued to use COmPASS. All participating rheumatologists were informed via email newsletters and the SCQM website about the patient apps, and they were invited to enrol their patients to use the app of their choice. Brochures with information about the apps were sent to physicians to put in waiting rooms and hand out to patients. Patients were informed about the apps and how to use them through their physicians. Patients were also informed about the apps via the SCQM website, and they could contact the SCQM directly to request access to the apps. App use was completely voluntary and patients could stop using their app at any time.
The apps were both compatible with Apple and Android phones. They were web apps, which means they could be used with any browser, on a computer or hand-held device. Reminders for data entry were sent via SMS to users. Both apps assessed disease activity using validated PROs and medication adherence, and provided patients with a graphical display of their disease activity measurements over time (calculated from app entries). Data collected from both apps was integrated into the SCQM database and accessible to physicians during patient visits. After logging in to the SCQM website, physicians could view the patient’s app data plotted on a graph over time with other data regularly collected in SCQM. Physicians could review this data with the patient during consultations. Patients and physicians received no formal guidance regarding interpretation of app feedback or communication about app feedback during consultations. However, it should be noted that physicians were already accustomed to reviewing their patients’ SCQM data in the graphs provided on the SCQM website, and that patients would also be used to answering PRO questions as part of their participation in SCQM.
The apps measured different PROs, but there were certain questions common across all patients, such as the pain Visual Analogue Scale (VAS), patient global assessment VAS, and questions about medication adherence. Details about the characteristics of the two apps are presented in table 1.
Characteristics of the iDialog and COMPASS apps
iDialog solicited monthly data entries from users with the Rheumatoid Arthritis Disease Activity Index-5 (RADAI-5)24 for patients with RA nnd Bath Ankylosing Spondylitis Disease Activity Index (BASDAI)25 for patients with axSpA, and a VAS score for pain, disease activity and skin symptoms for patients with PsA MySCQM (which replaced iDialog in January 2019) measured the same PROs as iDialog, but the new version of the app allowed patients to choose monthly or weekly data entry. COmPASS asked patients to fill out the Routine Assessment of Patient Index Data-3 (RAPID-3)26 weekly. Although the two apps were intended to be completed with different frequencies and used different measures to assess patient symptoms, the apps functioned similarly from the patient’s and physician’s perspective. The authors determined that it would be appropriate to pool data from both apps for this study to ensure an adequate sample size.
Evaluation approach
We hypothesised that use of an app would lead to positive effects on patient–provider interaction and disease management through promotion of patient–provider communication. We evaluated the effect of the SCQM apps on patient–provider interaction and disease management using data from a cross sectional survey and the SCQM database. Survey questions asked about satisfaction with SDM,27 disease management and the apps (see table 2 for key survey questions). Patients’ demographic data and longitudinal data on disease status, health status and medication use were extracted from the SCQM database.
Key survey questions
The exposure of interest was SCQM app use (app use vs no app use). The app use group was further split according to whether patients reported discussing app data with their physician (‘agree’ or ‘completely agree’ with the statement ‘I discussed the app data with my physician’), for a total of three 'treatment' groups: (1) no app use, (2) app only and (3) app+discussion.
During the period included in our analysis, a randomised trial was conducted with the ComPASS app as part of a separate study. In that study, COmPASS users were randomised to one of three arms: (1) patient and physician both receive feedback from patient app entries; (2) patient only receives feedback; and (3) no feedback to patient or physician. For our analysis, COmPASS users randomised to the first two groups were categorised to the app-only or app+discussion groups, depending on whether patients reported discussing app data with their physician. COmPASS users randomised to group 3 (no feedback) were categorised into the app-only group. (A sensitivity analysis was conducted to check whether excluding ComPASS users in group three from the analysis would change the results, since it could be argued that the classification of this group is ambiguous, due to having exposure to the app but also having no access to the app feedback and therefore no possibility for discussing the app results.) In contrast, all iDialog users and their physicians received feedback from patients’ app entries.
For this study, there were two primary outcomes relating to patient–provider interaction: patient satisfaction with SDM and physician awareness of disease fluctuations over time (referred to hereafter as physician disease tracking). SDM was measured using the three-item CollaboRATE instrument,27 a validated patient-reported measure of SDM. Physician disease tracking was assessed with the question ‘How much effort was made to follow the evolution of your health issues over time?’ For each of the survey questions for SDM and physician disease tracking, patients were asked to rate the effort made by the rheumatologist on a 10-point Likert scale (see table 2). For logistic regressions, both SDM and physician disease tracking were defined as a binary outcome=1 if patient gave a maximum rating on the relevant survey questions, or otherwise=0. Since patients tend to give high ratings when asked to evaluate their healthcare providers, we chose this approach (called a top score analysis) to increase variation in the outcomes. This approach has been previously used in the assessment of CollaboRATE scores.28
We also assessed three secondary outcomes relating to disease management: achievement of low disease activity at the most recent SCQM visit, disease activity improvement in the last year of follow-up, and treatment intensification (adding/increasing the dose of a disease-modifying antirheumatic drug) in the last 6 months of follow-up (all were binary outcomes).
Study population
The study survey on patient–physician interaction and app use was administered to all SCQM patients completing an online SCQM questionnaire between February and December 2018 (patients are required to complete the SCQM questionnaire within 2 weeks of their appointment). We analysed survey responses and clinical data collected in the SCQM, focusing on the period between the initial deployment of the apps (1 February 2016) through 1 April 2019. We excluded patients with undifferentiated arthritis, since we lacked measures of disease activity (and were therefore missing two of the study outcomes) for these patients. Patients were included for all analyses for which they had data available on study outcomes (described earlier); app users were included if they answered a survey question about discussing app data with their physician and had used an app for at least 6 months by 1 April 2019. For the analyses of the primary outcomes (SDM and physician disease tracking), patients were eligible for inclusion if they used an app for at least 6 months before the app survey or did not use any app. Patients were excluded if they provided no answer to the survey questions on SDM or physician disease tracking.
For the analyses of secondary outcomes (low disease activity at the last SCQM visit, disease activity improvement in the year before the last visit and treatment intensification in the last 6 months of follow-up), patients were eligible for inclusion if they were followed in SCQM for at least 1 year by 1 April 2019, and had either used an app for at least 6 months before the last SCQM visit or did not use any app. Patients were excluded if they were missing data on disease activity or medications.
Statistical analyses
Analyses were carried out using the R Project for Statistical Computing V.3.4.4. For each individual app user, the follow-up period was defined as the time between first app entry and the most recent SCQM visit up until 1 April 2019. For non-app users, the follow-up period began at the earliest SCQM visit occurring after the first documented app entry (18 August 2015) and ended at the most recent SCQM visit before or on 1 April, 2019. To provide context on the use of the apps, descriptive analyses were performed of app uptake and retention, frequency and duration of use, number of times moderate/high disease activity (MHDAS) was detected by apps and patient attitudes towards apps. We also performed descriptive analyses of the baseline characteristics of analysis subjects. For iDialog users, MHDAS was defined as a RADAI-5 score of >3.0 for patients with RA,24 BASDAI score of >4.0 for patients with axSpA29 or patient global disease activity score of >20 for patients with PsA.30 For COmPASS users, MHDAS was defined as a RAPID-3 score of >6.0 for patients with RA and PsA31 and a RAPID-3 score of >3.33 for patients with axSpA.32
We conducted logistic regressions to compare the groups with respect to the primary and secondary outcomes. For the analyses assessing the secondary outcomes, the z-score of disease activity (Disease Activity Score 28-joint count/BASDAI/physician global disease activity for patients with RA/axSpA/PsA) at baseline was included as a covariate in the logistic regressions to control for the effect of disease activity on the outcomes.33 To balance differences in baseline characteristics (demographic factors, disease and overall health status, and medications) between the three groups, all regressions were weighted using inverse probability of treatment weights based on multinomial propensity scores (PS). PS weighting is one approach commonly used in public policy and health services research that can be used to evaluate differences between groups in an observational setting.34 Covariates thought to have a possible influence on the exposure or outcomes were identified. Covariates for the final PS models were selected by excluding those which were not associated/weakly associated (p>0.05) with each outcome to avoid decreasing the precision of the estimated treatment effects.35 Potential covariates were regressed on each outcome in a multiple logistic regression, and covariates with p>0.05 were removed stepwise until all remaining covariates had p≤0.05; these covariates were then used for each PS model. For a list of covariates included in each PS model, see online supplemental table 1. Missing data on these covariates (see online supplemental table 2) were imputed with multiple imputation by chained equations using the R package ‘mice’.36 Thirty-six multiple imputations were generated. For a list of variables used to impute missing covariates, see online supplemental table 3. PS weights were estimated using the R package ‘twang’,37 then generalised estimating equations was used for robust variance estimation of treatment effects via the R package ‘geeM’.38 The results from each multiply imputed dataset were pooled using Rubin’s rules.
Supplemental material
Results
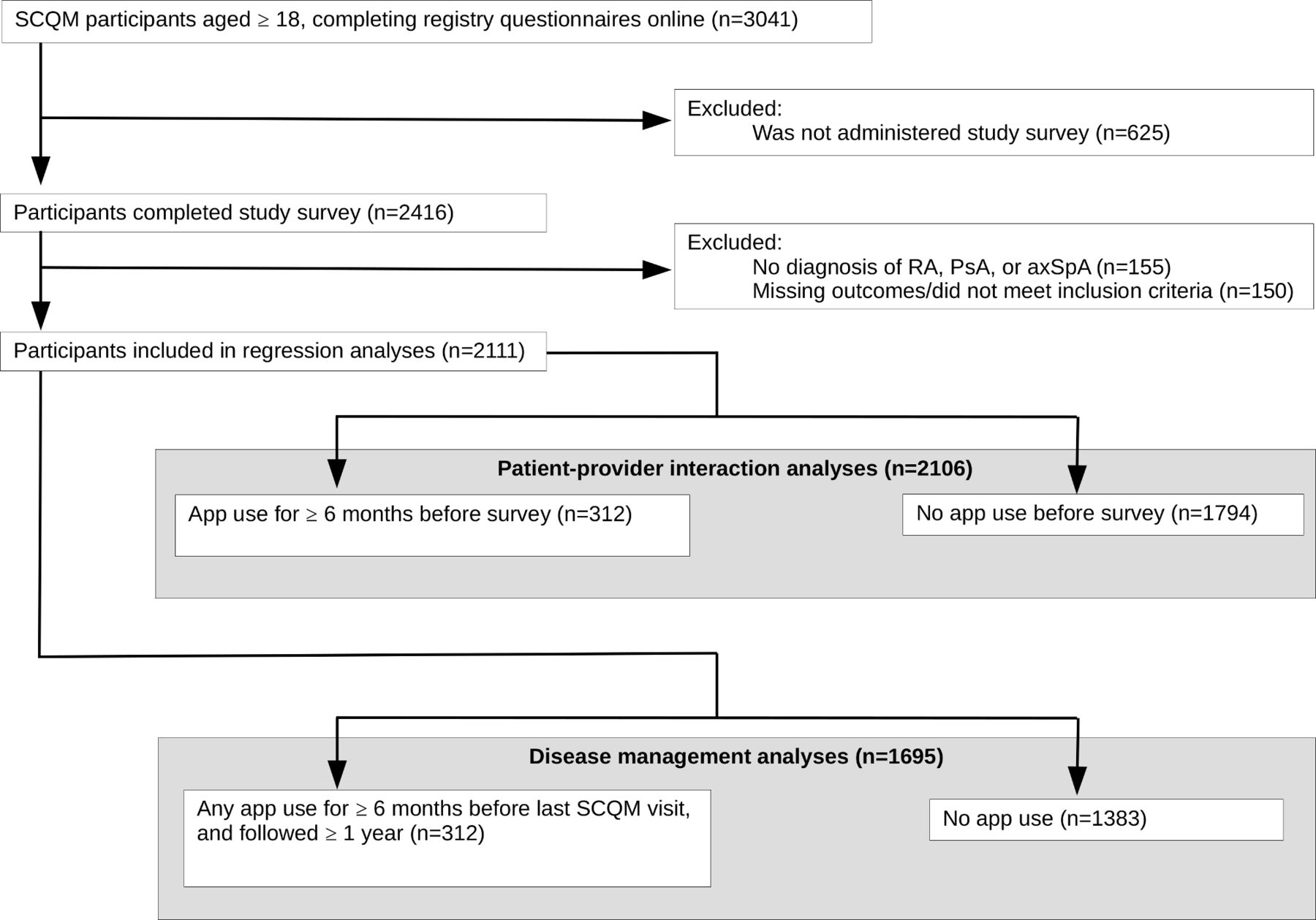
From February to December 2018, 2416 out of 3041 eligible participants (aged ≥18 years and completing online SCQM questionnaires) completed the study survey. Of these, 2011 participants were included in the regression analyses (figure 1 and table 3).
Baseline characteristics of users and non-users of SCQM apps (n=2111)
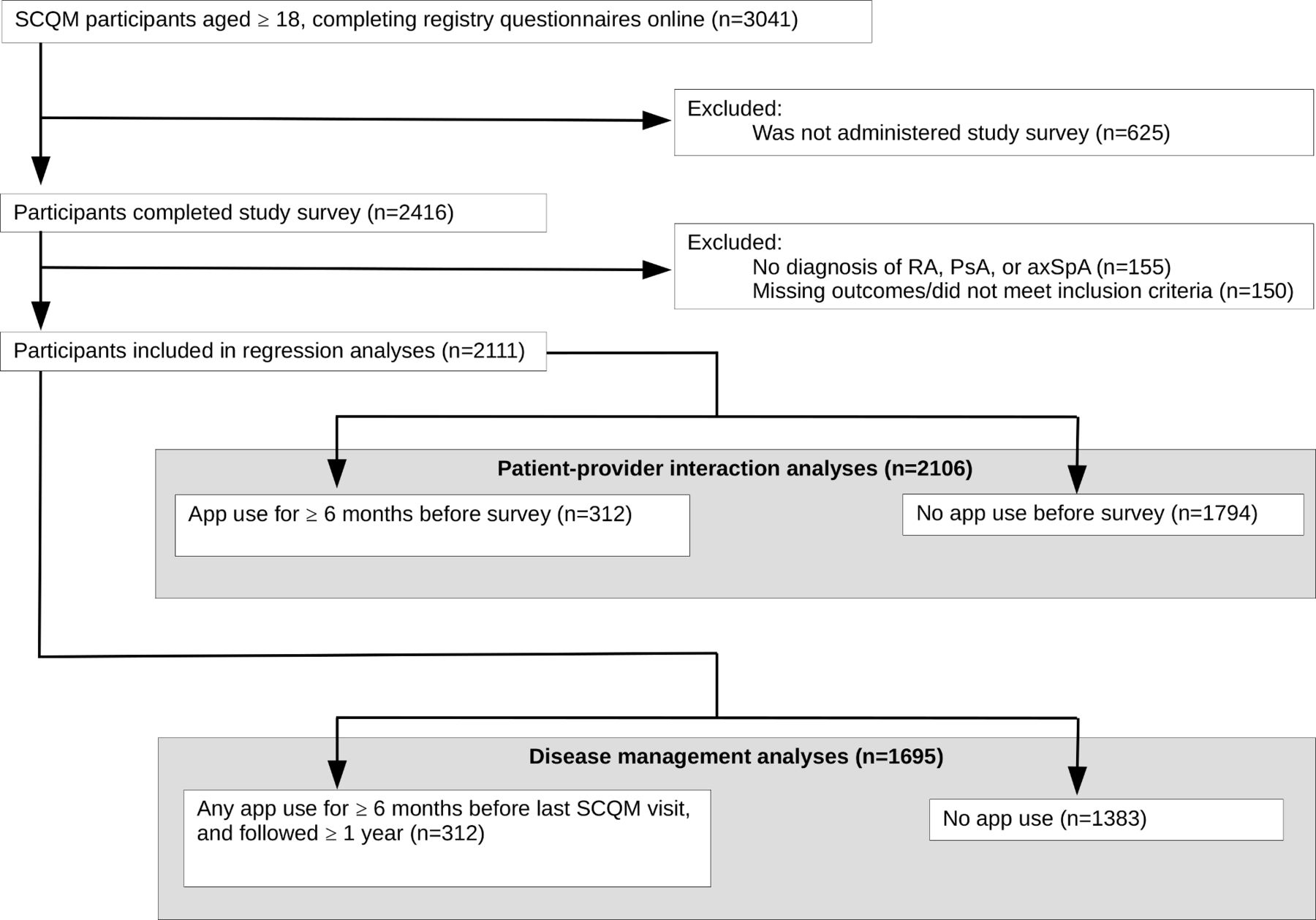
Flowchart for inclusion in regression analyses. PsA, psoriatic arthritis; RA, rheumatoid arthritis; SCQM, Swiss Clinical Quality Management in Rheumatic Diseases Registry.
Compared with SCQM participants excluded from the analyses, those included were younger (mean age of 51.8 vs 55.5 years, p<0.001), had a higher proportion of men (43% vs 38%, p<0.001), had lower proportion diagnosed with RA (43% vs 53%, p<0.001) and had a shorter mean disease duration (10.8 vs 12.1 years, p<0.001).
Out of 2416 survey respondents, 26% used an SCQM app at some point during the 3.8 years between the introduction of the apps and 1 April 2019 (see online supplemental figure 1 for a status plot of app use over time). The median follow-up for each individual patient was 3 years (IQR 2.6–3.3). The median frequency of app use was one time per month (IQR 0.9–1.2), and the median duration was 72 weeks (IQR 25–118). Among all patients who tried apps, 81% had completed an app entry in the 12 weeks before 1 April 2019.
Sixty-six per cent of app users reported MHDAS at least once via their app, corresponding to 39% of all app entries. According to the physician-reported Disease Activity Score with 28 Joint Counts (DAS-28) during the same individual periods of app use, 73% of app users had MHDAS for at least one SCQM visit, corresponding to 47% of SCQM visits. Twenty per cent of app users had at least one app entry indicating MHDAS despite not having had MHDAS documented at any SCQM visits during the same period (online supplemental figure 2).
Respondents in the app+discussion group were more satisfied with apps compared with those in the app-only group. Compared with the app-only group, a greater percentage of users in the app+discussion group found the apps easy to use (72% vs 92%, p<0.001) and understand (83% vs 95%, p=0.004), and were more likely to recommend the apps to others (41% vs 72%, p<0.001) (see table 4).
Satisfaction with SCQM apps
A total of 2111 patients were eligible for inclusion in the regression analyses, including 902 patients with RA, 766 patients with axSpA and 443 patients with PsA (2089 and 1695 patients were eligible for inclusion in the analyses of patient–provider interaction and disease management, respectively; see figure 1 for a flowchart of analysis inclusion). Of these patients, 190 (9%) had a disease duration of 6 months or less at baseline. Among eligible subjects, 17.3% (n=312) used apps, and 55% of app-users (n=162) discussed app feedback with their physician (table 3).
There were 1799 non-app users, 150 in the app-only group, and 162 in the app+discussion group. All groups had a similar sex distribution (43%–45% male). App users were younger than non-app users (mean age of approximately 47 vs 51 years, p<0.001), with a higher proportion of patients with axSpA (43%–47% vs 35%, p=0.011), a higher proportion with low disease activity at baseline (58%–64% vs 51%, p<0.01) and more likely to report confidence in using internet and smartphones (95%–97% vs 88%, p<0.001). Patients aged ≥65 years also used the apps (n=28 or 9% of app users). However, the proportion of elderly among app users was less than among non-app users (9% vs 15%).
The app+discussion group had higher unadjusted rates of satisfaction with SDM (64%, 95% CI 56% to 72%) and physician disease tracking (71%, 95% CI 63% to 78%), compared with non-app users (SDM: 55%, 95% CI 52% to 57%; physician disease tracking: 59%, 95% CI 57% to 62%) (table 5). Differences in the unadjusted rates of disease management outcomes between app users and non-app users were not statistically significant at the p=0.05 level.
Unadjusted rates of outcomes
In adjusted analyses (figure 2), compared with non-app users, the app+discussion group was more likely to be satisfied with SDM (OR 1.66, 95% CI 1.14 to 2.42) and with physician disease tracking (OR 2.00, 95% CI 1.30 to 3.09), whereas the app-only group had similar levels of satisfaction with these outcomes compared with non-app users. Differences in adjusted disease management outcomes between app users and non-app users were not statistically significant at the p=0.05 level. Patients with higher disease activity at baseline were less likely to achieve low disease activity at the last SCQM visit (OR 0.33, 95% CI 0.26 to 0.42), more likely to have improved disease activity by the last SCQM visit (OR 1.20, 95% CI 1.01 to 1.43) and more likely to intensify therapy in the last 6 months of follow-up (OR 1.34, 95% CI 1.09 to 1.65). Sensitivity analyses showed that excluding ComPASS users randomised to receive no app feedback (n=37) did not change the results.

{kind=link}
{kind=link}
Association of app use with patient satisfaction and disease management. *Reference group: no app use.
Discussion
In this study, patients who used an app to document PROs and discussed their app results with their physician reported greater physician engagement with SDM (ie, informing, listening and incorporating patient concerns into decisions) and physician disease tracking than non-app users. In contrast, patients who only used an app but did not discuss results with their physician did not report increased physician effort towards SDM and physician disease tracking compared with non-app users. Our results suggest that merely collecting information about the patient’s disease status between visits does not lead to improved patient–provider interactions. Indeed, satisfaction with physician disease tracking was marginally lower among app users who did not discuss the results, suggesting that app users may be unsatisfied if app data are not addressed during the consultation. Our results suggest that apps measuring PROs can positively impact patient–provider interactions if patients and physicians devote time during consultations to communicating about the data points gathered since the last visit.
Even when patients with rheumatic diseases receive effective treatment, they may continue to experience residual symptoms significantly affecting their quality of life such as pain, fatigue, sleep disturbance, functional limitations, and impacts on mental health and work productivity.12–14 Regular assessment of these aspects of disease impact using PROs can complement clinical assessment of disease activity by promoting physician awareness of patients’ overall well-being. Other apps have been developed for patients with inflammatory arthritis to track their symptoms using the same PROs measured by the SCQM apps, as well as others such as the RA Impact of Disease score (RAID), Health Assessment Questionnaire (HAQ), Modified HAQ (MHAQ), Multidimensional HAQ (MDHAQ), Health Assessment Questionnaire II (HAQ-II), Bath Ankylosing Spondylitis Functional Index (BASFI), Work Productivity and Activity Impairment Questionnaire (WPAI), and self-reported swollen and tender joint counts.5 18 39–42 At the time of writing, there are currently no other published studies of quantitative evaluations of the effects of these apps on patient–provider interactions or disease management. However, pilot studies assessing the feasibility and acceptability of such apps have reported qualitative feedback from patients and physicians.16 39 40 Patients have reported that symptom-tracking apps helped accurately capture fluctuations in their disease over time, which was superior to relying on memory alone.16 39 40 Having a more accurate and thorough record of their symptoms over time also helped provide a starting point for discussions with their physician, making it easier for patients to take an active role in discussions and increasing their confidence about communicating with their physician.16 39 40 Using an app may lead patients to expect that their physician will acknowledge and use their app data in assessment and care.18 Patients also shared concerns that some physicians might not be receptive to incorporating app data into discussions during consultations.39 Physicians in pilot studies felt that having access to patients’ app data helped them to spend less time on history taking and more time discussing patients’ concerns.16 39 Viewing app data prompted physicians to discuss the outcomes that had been measured,39 and they felt it made their assessment more accurate since it was based on the patient’s actual experience over time.18 39
Evaluations of interventions where rheumatology patients are taught to measure their own disease activity or to complete assessments using an online tool suggest that encouraging patients to engage in self-monitoring can facilitate improvements in patient–provider interactions and disease management.43 44 Use of an online self-assessment tool slightly improved patient-perceived patient–physician interaction after 12 months,43 while an intervention training patients to assess their own disease activity using the DAS-28 measure made patients more likely to intensify treatment.44
An important implication of our findings is that when implementing apps to measure PROs, it is critical to plan a mechanism for the new information to be reviewed. Without mechanisms for incorporating new information into decision making by healthcare providers and patients, eHealth interventions are unlikely to improve health outcomes.45 Implementation efforts should support, track and provide feedback on uptake of the app information, since provision of an app alone will not ensure its use. Patient self-monitoring should ideally be combined with setting and reviewing disease management goals, possibly together with a healthcare provider. Some physicians might be concerned about having enough time to review app data during appointments, but our experience and accounts reported in the literature suggest that reviewing app data with patients is quick and easy, and can even facilitate more efficient discussions.39 46 Another important question is whether review of app data during the consultation should be driven by patients or physicians. Relying on patients to take the initiative for discussing app feedback may not be the optimal way to promote use of this information during consultations. Dougados et al44 found that when patients were trained to assess their own disease activity, only 30% discussed their measurements with their physician, and among those who did not discuss their measurements, 14% did not because of reluctance to share the information with their doctor. Providing healthcare providers with guidance that suggests concrete ways of discussing and using app information during consultations may alleviate concerns about using apps and encourage more effective use of apps.
Our study has some limitations. The study was not a randomised trial—although we adjusted for potential confounders of treatment selection using PSs, there could be unmeasured confounders that we did not account for. For example, app users might have had different attitudes towards their health and treatment compared with patients who did not use apps. Not all patients were encouraged to use apps by their physicians; among non-app users, 34% said that they had not been offered an app by their physician. Also, we could not account for possible use of similar non-SCQM apps that might have affected patients' decisions about whether to use an SCQM app or outcomes. Since the study was conducted in the context of the SCQM registry, all patients were already exposed to higher levels of disease monitoring than they might be outside of the registry, potentially weakening the observed effect of the SCQM apps. It is also possible that online users in the SCQM registry might differ from the general rheumatic diseases population in other ways (such as income or educational level) that affected the outcomes observed. Since there were few app users, we have pooled the data from two different apps for our analyses; this may have weakened our results if the two apps actually have a different effect on outcomes. However, this effect appears to be minimal since there were relatively few COmPASS users (84 COmPASS vs 359 iDialog users), and the outcome rates were similar across the two apps. Only 26% of our survey respondents used one of the apps, and only 43%–72% of app users said they would recommend the apps to others; a low level of uptake and satisfaction with the apps might have limited the observed effect of apps on outcomes. Compared with app users, non-app users were older and less confident in using the internet/smartphones for daily tasks. Providing more guidance to patients on using the apps might have increased the uptake among SCQM patients. Lastly, the reader should keep in mind that in this study, no formal guidance was offered to patients and physicians on interpreting and communicating about app feedback, potentially weakening the observed impact of the apps. Apps measuring PROs might be expected to have greater impact on disease management and health outcomes if combined with a more structured self management programme.47
In conclusion, this study demonstrates that apps measuring PROs can improve quality of care (specifically, with respect to SDM and physician disease tracking) in rheumatology, but apps need to be integrated into care processes for optimal impact. Providing patients and healthcare providers with guidance on using PRO information during consultations and in daily life may further increase the beneficial impacts of apps and other eHealth technologies.
Data availability statement
Data are available upon reasonable request.
Ethics statements
Ethics approval
The study was approved by the Cantonal Research Ethics Committee of Geneva, Switzerland (2018–00099).
Acknowledgments
We thank the patients and their rheumatologists for their participation in the Swiss Clinical Quality Management in Rheumatic Diseases Registry (SCQM). A list of participating offices and hospitals that are contributing to the SCQM registries can be found online (www.scqm.ch/institutions). The SCQM is financially supported by sponsors (www.scqm.ch/sponsoren).
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Contributors YS: conceptualisation, methodology, statistical analysis, interpretation of data, writing of the original draft, writing of the review and editing, visualisation, project administration, final approval of the manuscript. DSC: conceptualisation, methodology, interpretation of data, writing of the review and editing, supervision, final approval of the manuscript. AS: data collection and curation, project administration, interpretation of data, writing of the review and editing, final approval of the manuscript. AC, TL, VKJ and UAW: interpretation of data, writing of the review and editing, final approval of the manuscript. AF: conceptualisation, methodology, interpretation of data, writing of the review and editing, supervision, funding acquisition, and final approval of manuscript.
Funding Funding for this study was provided by MSD. The funder played no role in the design or conduct of the study, or in the data analysis. Creation of the iDialog app was funded by MSD, while the COmPASS app was funded by AbbVie. At the time of the study, iDialog was owned by MSD.
Competing interests YS has been a paid speaker for MSD. DC has been a consultant for BMS, Pfizer and AB2BIO; and a paid instructor for Janssen. AC has been a speaker or consultant for Abbvie, Celgene, Eli-Lilly, MSD, Novartis and Pfizer. UAW has received unrestricted grant support by Abbvie and used it for the creation of the COmPASS app. AF has been a speaker or consultant for AbbVie, BMS, Gilead, MSD, Pfizer, Sanofi and Sandoz.
Provenance and peer review Not commissioned; externally peer reviewed.