Article Text

Abstract
Objective To explore non-steroidal anti-inflammatory drug (NSAID) and analgesic use in early rheumatoid arthritis (eRA) patients with a favourable risk profile initiating methotrexate (MTX) with or without glucocorticoid (GC) bridging.
Methods Patients with eRA (≤1 year) and favourable risk profile (no erosions, negative rheumatoid factor and anticitrullinated protein antibodiesor low disease activity) in the 2-year CareRA trial were randomised to MTX 15 mg with a step-down GC scheme (COBRA Slim), or MTX without oral GCs, Tight-Step-Up (TSU). Used analgesics were recorded, including frequency, start/end date and indication. Chronic intake (≥90 consecutive days in trial) of NSAIDs, acetaminophen, opioids including tramadol and antidepressants for the indication of musculoskeletal (MSK) pain was considered. Treatments were compared using χ2 and analysis of variance with Holm’s correction for multiple testing.
Results In total, 43 patients were randomised to COBRA Slim and 47 to TSU. At study inclusion, 33/43 (77%) of patients in the COBRA Slim and 32/47 (68%) in the TSU arm had been using analgesics (p=0.5). During the trial, 67 NSAID and analgesics were used for MSK pain in 26/43 (60%) COBRA Slim patients of which 9/43 (21%) daily chronically (DC), while 107 NSAID and analgesics were used in 43/47 (92%) TSU patients, of which 25/47 (53%) DC. The total number of patients on NSAID and analgesics at any time during the study (p<0.01) and chronically (p=0.01) was significantly different between treatment arms. Number of patients on DC NSAIDs was also significantly different (p<0.01) between COBRA Slim 6/43 (14%) and TSU 19/47 (40%).
Conclusion In eRA patients considered to have a favourable prognosis, initial oral GC bridging resulted in lower chronic NSAID and analgesic use.
Trial registration number NCT01172639.
- analgesics
- glucocorticoids
- arthritis
- rheumatoid
Data availability statement
Data are available upon reasonable request. The authors commit to making the relevant anonymised patient data available for a specified purpose approved by the institution and the principal investigator of the CareRA study and with a signed data access agreement.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Key messages
What is already known about this subject?
Early and intensive rheumatoid arthritis (RA) treatment using disease activity as a target for treatment adaptation allows rapid disease control and prevents joint destruction.
Methotrexate (MTX) with glucocorticoid (GC) bridging is recommended by EULAR as first-line treatment for all patients with RA. However, in clinical practice, there is still discussion if this intensive approach is also necessary in patients lacking classical markers of poor prognosis.
What does this study add?
Patients with early RA considered to have a favourable prognosis and receiving initial MTX monotherapy had a significantly higher risk of non-steroidal anti-inflammatory drug and analgesic consumption, even chronically, than those treated with MTX and GC bridging.
How might this impact on clinical practice or further developments?
Early initial intensive treatment should incorporate GC bridging, even in patients considered to have a favourable prognosis.
Introduction
Early, intensive, treat-to-target strategies have improved the clinical outcomes for patients with rheumatoid arthritis (RA).1 2 However, there is evidence that even achieving the target of remission is sometimes insufficient to normalise patients’ quality of life and persistent complaints such as pain remain a challenge.1 Despite European guidelines recommending as first treatment strategy the initiation of disease-modifying antirheumatic drug (DMARD) such as methotrexate (MTX) with a short-term glucocorticoid (GC) course,2 it is debated if this intensive approach is also necessary in patients lacking classical markers of poor prognosis.3 In the Care in early RA (CareRA) trial, we demonstrated that also in patients without erosions, seronegative or with low disease activity, the speed of response was more rapid when treated with MTX plus a step-down-bridge GC scheme compared with MTX therapy without GC, while long-term treat-to-target results were comparable.4–6 However, the potential advantage of intensive therapy on patient important outcomes such as pain and the concomitant use of non-steroidal anti-inflammatory drugs (NSAIDs) and analgesics deserves more detailed study in relation to the clinical response to a treat-to-target approach, taking into account the cumulative need but also the evolution over time.
Therefore, we aim to compare both the extent and dynamics of analgesic use in patients with early RA considered to have a favourable prognosis and treated to target with or without initial GC bridging during the first 2 years in the CareRA trial.
Patients and methods
CareRA was a 2-year open-label investigator-initiated pragmatic superiority randomised controlled trial (EudraCT number: 2008-007225-39) conducted in 13 Flemish rheumatology centres (two academic centres, seven general hospitals and four private practices).
Study population
Patients with recently diagnosed RA (≤1 year) were included and stratified into a low-risk versus a high-risk group based on classical factors of poor prognosis (online supplemental figure 1). This study focuses on the low-risk patients, who had to fulfil at least two of the following three criteria: absence of erosions, negativity for both rheumatoid factor (RF) and anticitrullinated protein antibodies (anti-CCP), or low disease activity score –DAS28CRP≤3.2. Patients in this low-risk group were randomised to either a Tight-Step-Up (TSU) treatment of MTX monotherapy 15 mg/weekly without GC or to COBRA Slim (MTX 15 mg/weekly with step-down GCs, starting with prednisone 30 mg followed by tapering to 5 mg over 6 weeks and stopping at 34 weeks). From week 8 onwards, treatment had to be adjusted in case of insufficient disease control (DAS28CRP>3.2). Overall, around 70% of the participants achieved a status of excellent disease control (DAS28CRP<2.6) after 2 years with a treat-to-target approach.6
Supplemental material
Clinical outcomes
Patients were assessed at screening, baseline and during followed-up at week 8, 16, 28, 40, 52, 65, 78, 91 and 104. Optional visits, if clinically required, could be performed. An electronic case report form (eCRF) was filled out and routinely monitored. Clinical, patient and laboratory parameters were collected at every visit: swollen joint count, tender joint count, patient’s global health assessment (PaGH), physician’s global health assessments, C reactive protein (CRP) or erythrocyte sedimentation rate, health assessment questionnaire, pain and fatigue each on a visual analogue scale (VAS) of 0–100.
Analgesic recording
Analgesics recorded in the eCRF were categorised per type of medication and indication. For this analysis, recorded analgesics will be referred to as ‘use’. NSAIDs, acetaminophen or opioids including tramadol, as well as other neuropathic pain drugs such as antidepressants indicated for musculoskeletal (MSK) pain were considered. Any time period of at least 90 consecutive days for which daily intake of a certain analgesic was documented was considered ‘chronic analgesic use’. Opioids were divided in strong (eg, oxycodone, methadone, fentanyl and sufentanil) and weak (eg, tramadol, codeine, meperidine, tilidine, dextropropoxyphene and piritramide). No formal evaluation of patient compliance (eg, pill count and questionnaire) was performed, but registration of current medication intake was part of the routine evaluation during follow-up as in daily clinical practice.
Treatment adaptations
In both treatment arms, low disease activity (DAS28CRP≤3.2) was used for steering treatment adaptations. Per-protocol adaptations were specified for the first trial year, while the second-year adaptations were left at the discretion of the treating rheumatologist. The first adjustment was an increase in the weekly MTX dose to 20 mg for both arms. Next, 10 mg leflunomide could be added. Further treatment changes could include biological (b-) DMARD initiation. More details on adaptations have been published elsewhere.6
Statistical analyses
Missing data
All randomised patients having taken at least one study medication dose were considered for intention-to-treat analysis. Missing data were assumed to be missing at random and were imputed with multiple imputation (classification and regression trees) by chained equations. Besides the incomplete variables, treatment strategy, centre of recruitment, age, gender, presence of comorbidities, RF, anti-CCP, erosions at baseline and trial completion were included as predictors in the imputation matrix. The number of imputed datasets was fixed to 100, each dataset was analysed and the results were pooled using Rubin’s rules.7 No imputation was done for recorded medication.
Comparison of analgesic use
Chronic intake (≥90 days during the trial) of NSAIDs, acetaminophen or opioids including tramadol and antidepressants prescribed for MSK pain were considered. Comparisons of analgesic use at any timepoint and chronically were performed with χ2.
Comparison of clinical outcomes in patients with or without GC bridging
Comparisons for VAS pain and DAS28CRP between treatment arms cross-sectionally at baseline was performed with analysis of variance (ANOVA), and the evolution during the 2 years was performed with repeated measures (RM) ANOVA and generalised estimating equation (GEE) taking into account time and baseline values. Next, a binary logistic regression for predicting chronic use of analgesics was fitted and controlled for treatment group, VAS pain at baseline, age, gender and presence of comorbidities.
Survival analyses of analgesics
To assess differences between treatment arms from time of diagnosis to the initiation of an analgesic for ≥90 days within the trial, survival curves were computed, and differences were tested with both the Gehan-Breslow-Wilcoxon method, which gives more weight to events at early timepoints and the log-rank test that gives equal weight to all time points. To estimate the independent role of the initial treatment strategy (MTX with or without GC) on chronic analgesic use, a Cox regression analysis was performed accounting for previous analgesic use and VAS pain at baseline.
To account for multiple testing, the Holm-Bonferroni method was used (online supplemental table 1).
All analyses were performed with R V.4.0.0.
Results
Of the 90 patients recruited in the low-risk group of the CareRA trial, 43 were randomised to COBRA Slim and 47 to TSU. Patients had comparable mean and SD in age (51.4±14.4 vs 51.0±14.0), body mass index (25.5±4.3 vs 27.0±4.2) and proportions of females (77% vs 81%), RF positivity (26% vs 23%), anti-CCP positivity (28% vs 23%) and erosions (n=1 vs n=0) (online supplemental table 2). Good retention rates of 87% of patients in TSU (41 out of 47) and 74% of patients in COBRA Slim (32 out of 43) were observed. Missingness for all variables over 2 years ranged from 0% to 39% per different time point and an overall missingness of 9.3%.
Pain and disease activity evolution
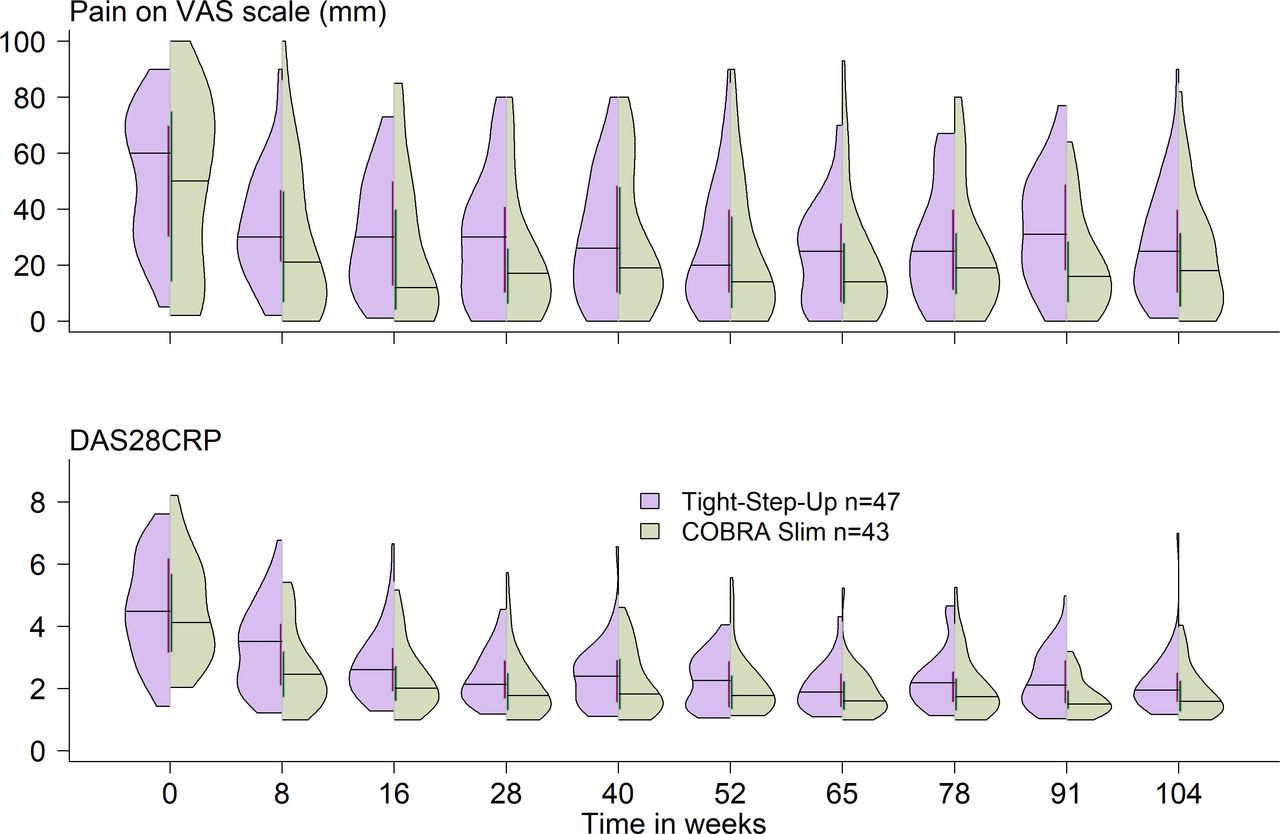
Patients randomised to COBRA Slim had a mean±SD at baseline VAS pain of 48±31 compared with 52±23 for TSU (p=0.57). In terms of disease activity (DAS28CRP), COBRA Slim patients had a mean±SD at baseline of 4.5±2.3, compared with 4.6±1.6 for TSU (p=0.89) (figure 1). Patients from both treatment groups, COBRA Slim and TSU, improve in disease-related measurements such as DAS28CRP, VAS pain, CRP and PaGH early on, but numerically patients in COBRA Slim had a greater improvement. In both treatment arms patients without chronic intake of analgesics seemed to have better outcomes than those with chronic intake for most selected measures at all time points. Data should be interpreted with caution because of the low numbers (online supplemental table 3). The RM-ANOVA, corrected for baseline pain in the model with pain as outcome and corrected for baseline disease activity in the model for DAS28CRP, demonstrated a significant difference for pain (p<0.01) and DAS28CRP (p<0.0001) over the two treatment years between treatment groups. In the GEE models, there was no significant interaction of time with treatment group for pain nor for DAS28CRP. Moreover, the binary logistic regression estimated a 90% (OR 0.10, p<0.001) reduction on the odds of chronic analgesic use when treated with COBRA Slim compared with TSU.

Pain and disease activity in 28 joints with C reactive protein (DAS28CRP) evolution over the 2-year trial per treatment group. Data represented as violin plots. Each ‘half-violin’ represents each treatment group. The shape represents the density estimate of the variable: the more data points in a specific range, the larger the violin is for that range. The horizontal line represents the median and the vertical line the IQR.
Analgesic use at different timepoints and survival analysis
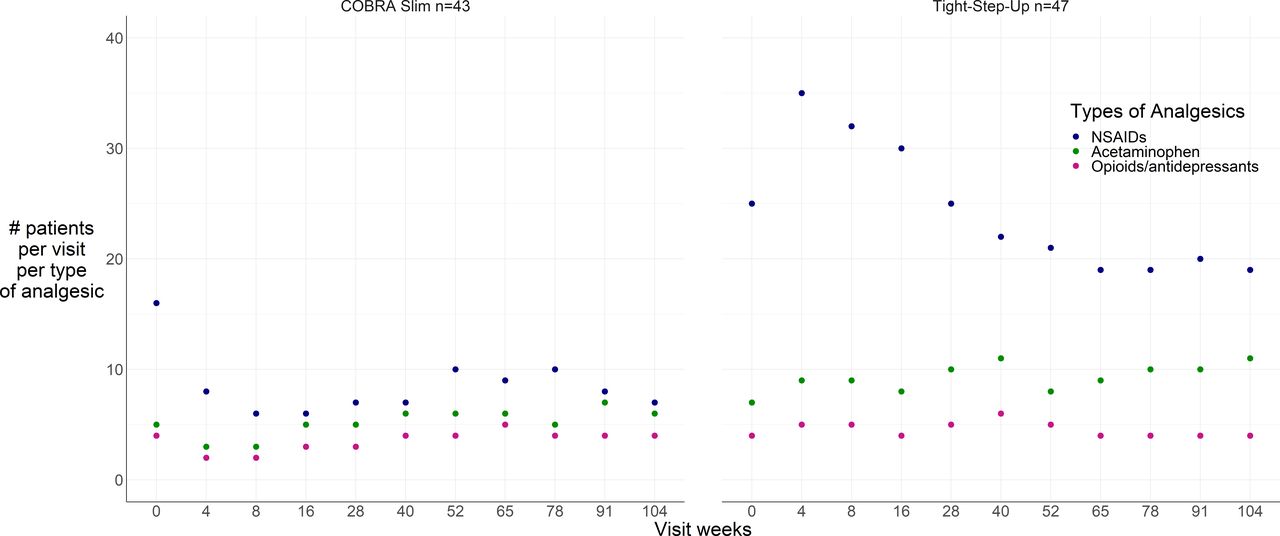
Before the start of the study, 33/43 (77%) of patients in the COBRA Slim and 32/47 (68%) in the TSU arm reported to have been taking analgesics (p=0.5). Cross-sectionally at baseline, 18/43 (42%) patients randomised to COBRA Slim and 28/47 (60%) randomised to TSU used analgesics (p=0.14). During the trial, 26/43 (60%) COBRA Slim patients used a total of 67 analgesics for MSK pain of which 9/43 (21%) daily chronically (DC) and a total of 107 analgesics used in 43/47 (92%) TSU patients of which 25/47 (53%) DC. The total number of patients on analgesics at any time during the study (p<0.01) and chronically (p=0.01) was significantly different between treatment arms. Figure 2 shows the analgesic intake per patient at every visit during the trial. Patients on TSU used more analgesics, especially early in the disease course, compared with patients on COBRA Slim (online supplemental table 4). For daily chronic intake, the number of patients on NSAIDs was also significantly different between COBRA Slim and TSU for daily chronic intake (6/43=14% vs 19/47=40%; p<0.01) (online supplemental figure 2). In COBRA Slim, 2/43 patients took daily chronically acetaminophen+tramadol and 1/43 strong opioid (methadone)+tricyclic antidepressant (nortriptyline). In TSU, 2/47 patients took tramadol daily chronically, and 3/47 combination of: (1) acetaminophen+weak opioid (tramadol), (2) acetaminophen+NSAID and (3) acetaminophen+selective serotonin reuptake inhibitor antidepressant (duloxetine). At baseline, 13 (28%) patients in TSU and 3 (7%) patients in the COBRA Slim group had started an analgesic that was continued daily and chronically (≥90 days). Detailed time of start, mean daily dose and intake time can be found in online supplemental tables 5 and 6. The time to first use of any chronic analgesic (figure 3 and online supplemental table 7) as well as specifically chronic NSAID use was significantly different between treatment arms (online supplemental figure 3). A Cox regression was fitted with the correction for chronic analgesic use already before the trial and VAS pain at baseline. Group differences were maintained. Initiating COBRA Slim (HR 0.17, 95% CI 0.07 to 0.41, p<0.001) and having had no previous chronic analgesic use before the trial (HR 0.11, 95% CI 0.05 to 0.29, p<0.001) were associated with a longer time to initiation of chronic use of analgesics (TTCUA) during the trial. Baseline VAS pain was not significantly associated with TTCUA (HR 1.02, 95% CI 0.98 to 1.04, p<0.01). Overall, this model had a good fit (p<0.001).
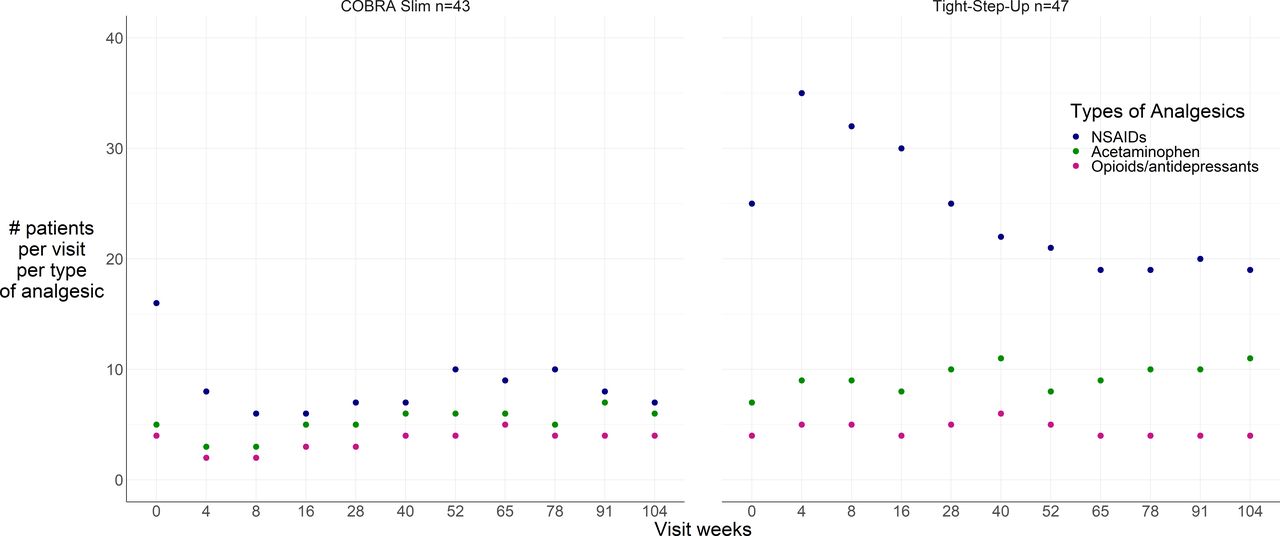
Number of patients taking non-steroidal anti-inflammatory drug (NSAID) or analgesics at any point during the trial per treatment group, per visit and type of medication.

{kind=link}
{kind=link}
{kind=link}
Survival analysis of time to the first recorded use of chronic analgesics with Kaplan-Meier.
Moreover, consecutive (>3 months) use of GCs after the bridging period over the 2 years of the trial was limited, and there was no difference between COBRA Slim (n=5, 12%) and TSU (n=5, 11%).6
Discussion
In this post hoc analysis of the randomised CareRA trial, patients with early RA perceived as having a favourable risk profile who were not initially treated with step-down GC, had a significantly higher use of analgesics (92% vs 60%) and being chronic for a significant proportion of them (53% vs 21%) compared with patients treated with step-down GC. Even when correcting for previous chronic analgesic use and baseline pain, patients treated with MTX and step-down GCs had an 83% lower hazard of using a daily chronic NSAID or analgesic and with no impact on consecutive use of GCs.
Chronic pain and analgesic consumption is a major health issue throughout the world and a huge economic burden for nations.8 In a cohort of 70 929 patients with RA, data collected from Medicare (USA) from 2006 to 2014 showed that in the average rheumatologist’s practice, 40% of RA patients used opioids regularly. In almost half of the patients, at least some opioid prescriptions were written by a rheumatologist, and 14% received opioids that were coprescribed concurrently by more than one physician.8 9 Awareness should also be given to the prescription behaviour of all stakeholders involved, not only the treating rheumatologist but also the general practitioner.10
Regular intake of analgesics both narcotic and non-narcotic comes with risks. NSAIDs are considered fast acting and help to relieve pain and decrease inflammation.11 Associated side effects can be reduced by gradually tapering doses as a patient’s condition improves. However, GCs are a more potent anti-inflammatory medication than NSAIDs, and contrary to NSAIDs, they also have immunomodulatory effects and they have been shown to prevent structural damage.12 Keeping this in mind, we observed patients on TSU had more analgesic use, especially NSAIDs and specifically early in the disease course, compared with patients on COBRA Slim. In contrast, the analgesic consumption before entering the trial was comparable between groups. This suggests that in TSU, analgesics were used instead of GC as bridging therapy in the first few months to alleviate the symptoms of RA. The time at which an analgesic was first taken is quite relevant because rapid introduction of analgesics and NSAIDs related to insufficient disease control in the early phase could lead to more prolonged use despite better disease control at a later stage, which would point to the possibility of an early window of opportunity for pain management in RA. We have seen that more TSU patients started quicker an analgesic which was then continued for a long period of time.
The less pronounced use of NSAIDs, at least during the first 40 weeks, could have been due to the fact that combination therapy of NSAID and GC is in general avoided because of the risk of side effects. To correct for this, we did a sensitivity analysis disregarding the first 40 weeks for categorising chronicity. There were eight patients on chronic analgesics in the COBRA Slim group versus 18 in the TSU group (p=0.04) of which 5 versus 12 were NSAIDs. The less frequent use of NSAIDs and analgesics in COBRA Slim compared with TSU could not be explained by differences in DMARD treatment adaptations throughout the course of the study.6 In terms of analgesic and total strategy cost, we have previously published that it was significantly different between treatment arms, in favour of COBRA Slim along with an increased quality of life.13
EULAR guidelines recommend as a first treatment strategy, in early RA, the combination of MTX with short-term GCs. It is feasible to reach high remission rates and stop GCs completely in the vast majority of patients after induction with GC-based schedules like COBRA Slim as shown in CareRA after 2 years.6 During the 2-year trial, chronic use of oral GCs (daily for more than 3 months) accounted for 11% of TSU patients (5/47) and 12% of COBRA Slim patients (5/43). Mean cumulative prednisone dose during the second year was 151 mg in COBRA Slim patients and 235 mg in TSU patients. Further details are described in the 2-year CareRA report.6 EULAR guidelines differentiate between patients with and without poor prognostics factors, in view of therapeutic decision making in case of insufficient response to the first strategy with MTX and bridging GCs. It remains however still debatable which risk factors are most relevant in this respect. In addition, patients considered to have a good prognosis (RF and anti-CCP negative, no erosions or low disease activity) benefit equally well from GC bridging compared with poor prognosis patients. In the current post hoc study, we demonstrated a higher use of analgesics if the initial scheme does not include GCs, despite the expected good prognosis. However, with a small sample size and without complete certainty of the actual intake but only recorded use of analgesics, caution must be applied when interpreting these findings.
What is more, we should explore and understand the hurdles and opportunities for patients,14 rheumatologists15 and other health professionals16 in the early management of RA with intensive strategies including GCs,17 especially in the context of shared decision making with the patient. The early disease period could probably offer a separate window of opportunity for pain management and especially for avoiding chronic analgesic use. The choice of initial treatment strategy might influence pain management on the long run, even in patients considered to have a good prognosis.
Conclusion
More than 90% of the patients in the TSU group used an analgesic for MSK pain compared with 60% in the group treated with MTX and a step-down GC scheme (COBRA Slim). Chronic analgesic use was more than double in TSU. The earlier and faster disease control in the COBRA Slim treated group seems to diminish the use of NSAIDs and analgesics for a significant proportion of patients, even in chronic use. To benefit maximally from the window of opportunity for treating early RA, intensive remission induction strategies using GCs should be applied even in patients without traditional factors of poor prognosis.
Data availability statement
Data are available upon reasonable request. The authors commit to making the relevant anonymised patient data available for a specified purpose approved by the institution and the principal investigator of the CareRA study and with a signed data access agreement.
Ethics statements
Ethics approval
The study was approved by the leading Ethics Committee of the University Hospitals Leuven after consulting the medical ethics committee of each participating centre (ref s51411) and all study participants gave their written informed consent before inclusion.
Acknowledgments
We would like to show our gratitude to all participating patients, as well as to the investigators and medical staff at all sites. We appreciate the time invested. Furthermore, we are thankful for providing statistical advice to Anikó Lovik.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Twitter @sophie_33pl, @DiederikDeCock
Presented at This work has been previously presented at the American College of Rheumatology’s 2020 conference: https://acrabstracts.org/abstract/patients-with-early-rheumatoid-arthritis-considered-to-have-a-favourable-risk-profile-and-treated-according-to-a-step-up-strategy-have-an-increased-risk-of-chronic-analgesic-consumption/?msg=fail&shared=email.
Contributors PV, RW, AB, SP and DDC made substantial contributions to the conception or design of the study. SP performed the statistical analysis. The manuscript was written by SP, PV, RW, AB and DDC and subsequently revised critically by all the remaining coauthors. All authors were involved in data interpretation and approved the final version to be submitted for publication.
Funding The CareRA trial (EudraCT number: 2008-007225-39) was funded by a Flemish governmental grant (Agency for Innovation by Science and Technology (IWT)). Prof. Dr. Patrick Verschueren holds the Pfizer chair for early rheumatoid arthritis management at the KU Leuven.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.