Article Text

Abstract
Objective To develop a Gout, Hyperuricaemia and Crystal-Associated Disease Network (G-CAN) common language definition of gout, with the goal of increasing public understanding and awareness, and ensure consistent and understandable messages about gout.
Methods A G-CAN working group that included patients, physicians and nongovernmental organisation (NGO) representatives was formed to develop a common language definition of gout for use with the public, media, healthcare providers and stakeholders. A literature search and interviews with patients, healthcare workers and stakeholders informed development of the definition. Following consultation with G-CAN members and partners, the definition was endorsed by the G-CAN board.
Results The G-CAN common language definition of gout describes the epidemiology, pathophysiology, symptoms and impact, risk factors, comorbidities, management and healthcare and workforce considerations. Detailed information is provided to support the content of the definition. After the publication of the English-language version, the definition will be available for translation into other languages by G-CAN members.
Conclusion G-CAN has developed a concise and easily understandable statement describing gout in language that can be used in conversations with the lay public, media, NGOs, funders, healthcare providers and other stakeholders.
- gout
- crystal arthropathies
- epidemiology
Data availability statement
Data are available upon reasonable request.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Key messages
What is already known about this subject?
Despite its high prevalence and impact, gout is understudied and often undertreated.
What does this study add?
The common language definition of gout encompasses key information relevant to gout as determined by a review of the literature, interviews with patients, healthcare workers and stakeholders and consultation with crystal-associated disease network members and stakeholders.
How might this impact on clinical practice or future developments?
This common language definition of gout has been developed to promote consistent, accurate and informative discussion about gout with the public, healthcare workers and stakeholders.
Introduction
Gout is the most common form of inflammatory arthritis affecting adults.1 Despite its high prevalence and impact, gout is understudied and often undertreated.2–4 One mechanism to increase public understanding and awareness, and ensure consistent and understandable messages about a disease, is development of an agreed common language definition. For example, the European League Against Rheumatism (EULAR) and American College of Rheumatology (ACR) developed a common language definition of rheumatic and musculoskeletal diseases (RMDs) to allow consistent use when describing these conditions.5 This short general definition included a general description of RMDs, the causes of disease, the experience of people with the disease and the impact of RMDs.
The Gout, Hyperuricaemia and Crystal-Associated Disease Network (G-CAN) is an international, multidisciplinary collaboration, dedicated to advancing the crystal deposition-associated disorders. In 2019, G-CAN convened a working group to develop a common language definition of gout; a concise and easily understandable statement describing gout in language can be used in conversations with the lay public, media, nongovernmental organisations (NGOs), funders, healthcare providers and other stakeholders. This work followed G-CAN consensus definitions of the disease elements and disease states of gout for technical communications.6 7 Herein, we describe the development and outcome of the G-CAN common language definition of gout project.
Methods
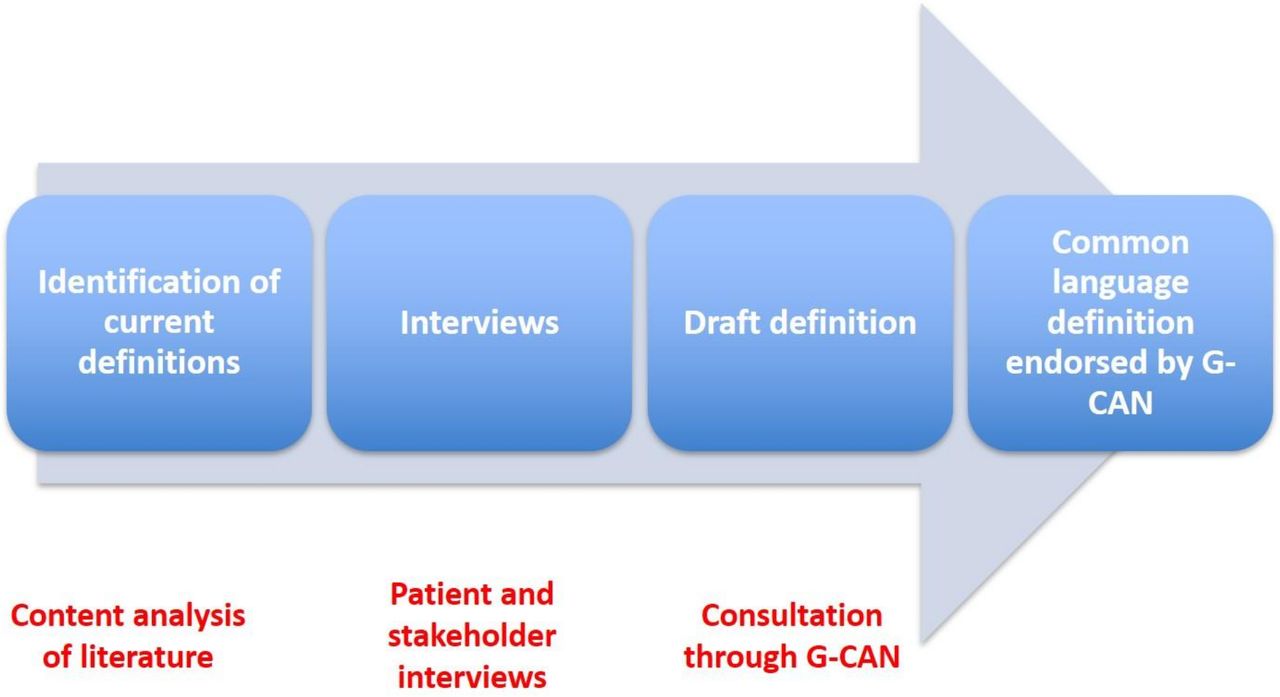
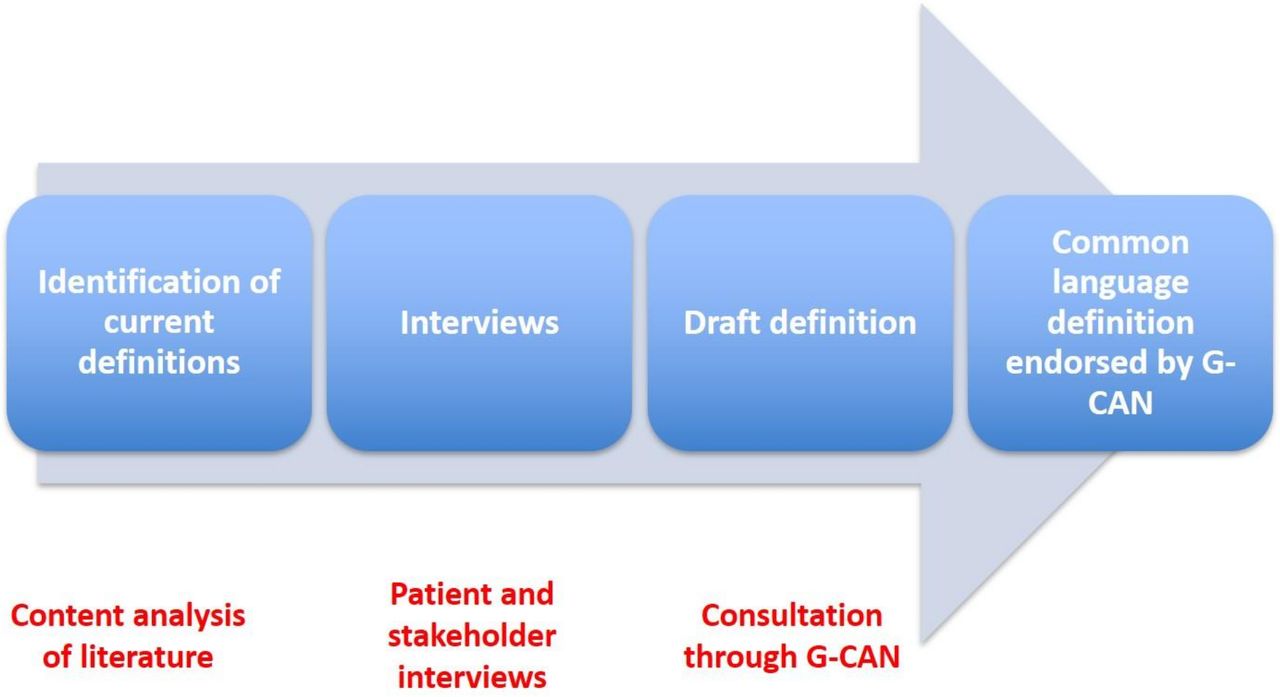
The components and flow of the project are shown in figure 1. The G-CAN working group included patient representatives, a health literacy expert, an NGO representative, a primary care physician, a physician assistant and rheumatologists. A literature review of key aspects of epidemiology, pathophysiology, symptoms, management and impact of gout, including grey literature sources, and interviews with patients, stakeholders and healthcare workers were undertaken to inform the development of the common language definition.
{kind=link}
Development of the Gout, Hyperuricaemia and Crystal-Associated Disease Network (G-CAN) common language definition of gout.
Scope of project
Working group members met to agree on the scope of the common language definition and literature review. It was agreed that the common language definition would be a concise statement written in language understandable to a broad audience and that G-CAN recommended nomenclature, such as ‘gout flare’ would be used.6 It was decided that the final definition would be available for translation into different languages by G-CAN members. The definition will be reviewed and updated as new evidence emerges.
Content analysis of literature
A literature search was undertaken to extract the major aspects of gout described in the literature and review articles about gout from major general medical journals and articles from the grey literature databases. Using the search term ‘gout’, the databases were searched for articles related to the epidemiology, pathophysiology, comorbidities, symptoms, management and impact on patients of gout. Review articles and governmental and NGO reports, documents or guidelines were included. Relevant information was extracted from 93 articles and the key messages for each category (pathophysiology, epidemiology, symptoms, comorbid disorders, diagnostic investigations, management and impact on patients and community) were compiled.
The main factors relating to pathophysiology that were identified in the literature review were that hyperuricaemia, formation of monosodium urate crystals, inflammation and underexcretion and overproduction of urate contribute to the development of gout. The main points related to epidemiology included that gout is common and increasing in prevalence. The main symptoms described in the literature were pain and swelling, and common comorbid disorders were cardiovascular disease, chronic kidney disease, diabetes and hypertension. Management strategies described included urate-lowering therapy and anti-inflammatory medications. The impact of gout included the effects on employment and quality of life, increased healthcare use and impact on physical well-being.
Major articles identified through MEDLINE and recent guidelines relating to the topics of pathophysiology, symptoms, impact on patients, risk factors, comorbidities, management and health and workforce considerations were also summarised to support statements within the definition.
Patient and stakeholder interviews
A total of 19 patients, healthcare workers and stakeholders were interviewed to identify important messages for inclusion in the definition. Patients with gout (n=7) were identified through a clinical research centre. Healthcare workers (n=7, pharmacist, nutritionist, general practitioner, internist, rheumatologist, nurse and podiatrist) and stakeholders (n=5, from an NGO providing patient support and education, a funding body and a government organisation) were identified through professional networks. These individuals were invited to take part in interviews about what should be included in a definition of gout. Participants were asked a set of questions about their experience of gout, what would be important for people to know about gout, how gout impacts on patients and the community and what challenges there are in the management of gout. The interviews were transcribed by the research fellow and analysed using NVivo software to identify the main themes and messages. Interviews were continued until data saturation was reached.
Key messages from the interviews were reviewed by the working group to assist with developing the definition. Key messages patients wanted to communicate about gout included the severity of pain, that it is controllable with treatment, and that it can be related to diet. The effect on ability to work and the importance of receiving appropriate treatment were also emphasised. Healthcare workers and stakeholders identified that it was important to know that gout is related to genetic factors, that recurrent gout flares can be prevented with long-term urate-lowering therapy, that people should not be blamed for having gout, and that the relationship between healthcare provider and patient is important.
Consultation through G-CAN
The results of the literature review and interviews were circulated to all working group members who met on two further occasions by teleconference to agree on a draft definition to be distributed for consultation. This definition was circulated for consultation to all G-CAN members and partners. It was then modified based on the feedback. The subsequent definition was circulated and agreed by the working group, reviewed by patients and lay readers for clarity and sent to the G-CAN board for endorsement.
Results
The key messages from the literature review, interviews, discussion of the working group and feedback from G-CAN members and partners are incorporated in the final definition (box 1).
The Gout, Hyperuricaemia and Crystal-Associated Disease Network common language definition of gout
Gout is a common condition caused by high levels of urate (also known as uric acid) in the body. Having too much urate causes crystals to form in the joints that can result in inflammation and damage. People are usually diagnosed with gout when they have an attack of a very painful arthritis, which can cause difficulty sleeping, walking and working. This is called a gout flare. For most people, gout happens when the kidneys do not remove enough urate from the body, with genetic make-up playing a critical role for some groups. Gout often occurs alongside other health problems such as high blood pressure, heart disease, diabetes and kidney disease, with shared risk factors including being overweight, diet and alcohol consumption. Gout flares are treated in the short term with anti-inflammatory medicines. Long-term daily medicines such as allopurinol decrease the amount of urate in the body and dissolve the urate crystals, resulting ultimately in prevention of gout flares and joint damage. Healthcare workers such as doctors, nurses and pharmacists can help people with gout understand the condition, reduce stigma and work with them to make management choices.
The following commentary provides detailed justification for the text included in the G-CAN common language definition of gout.
Epidemiology
Gout is a common disease with increasing incidence and prevalence, particularly in Western or westernising countries, paralleling the obesity epidemic over recent decades.8–11 There are currently an estimated 41 million people worldwide with gout.10 It is the most common form of inflammatory arthritis,12 estimated to affect about 4% of the population in the USA,13 2%–3% in the 14UK and 0.9%–2.5% in Europe.15 It is more common in men, with a prevalence of 5.2% in men and 2.7% in women.13 This prevalence increased with age to 9.3% of US adults over 60 years, although it can also affect young men.16 17 Gout is rare in women before menopause and does not usually affect children. It is more common in some ethnic groups such as Māori, Pacific Peoples and Taiwanese Indigenous Peoples.18 19 In Aotearoa/New Zealand, Māori and Pacific peoples have 2–3 times the prevalence of gout as non-Māori, non-Pacific peoples20 and the prevalence of gout in Taiwanese Indigenous men and women is 15.2% and 4.8%, respectively, compared with 0.3% in Taiwanese non-Indigenous people.21
Pathophysiology
Hyperuricaemia and deposition of monosodium urate crystals are the key pathophysiological mechanisms leading to the development of gout. Disease stages include asymptomatic hyperuricaemia, asymptomatic deposition of monosodium urate crystals, monosodium urate crystal deposition with gout flares and intercritical gout, and usually later in the disease course (in the absence of urate-lowering therapy), chronic gouty arthritis, tophus deposition and gouty bone erosion.22
Urate is produced mainly in the liver and intestinal cells.23 About two-thirds is excreted by the kidneys and the remainder in the gut.24 When the level of urate is above the saturation point of 6.8 mg/dL (408 μmol/L), monosodium urate crystals form at pH 7.0 and temperature 37°C.25
A gout flare arises when immune cells interact with the monosodium urate crystals, triggering an episode of acute inflammation. The release of the cytokine interleukin (IL)—1β by immune cells is particularly important in driving inflammation in the gout flare.26 Many other proinflammatory mediators also contribute to the gout flare.
Gout is characterised by repeated gout flares with intercritical periods during which the patient is asymptomatic but remains hyperuricaemic with risk of further gout flares.22 Monosodium urate crystals can be found in the synovial fluid during the intercritical period.27 If the hyperuricaemia responsible for gout is untreated, subcutaneous tophi can develop; these nodules are discrete collection of monosodium urate crystals with associated tissue response.6 Tophi can lead to bone erosion and cartilage damage.28
Symptoms and impact
The key symptom of the gout flare is severe joint pain. Qualitative studies of patients with gout show that pain is an important symptom.29 Other symptoms of a gout flare are joint swelling, redness and heat.30 31 Typically, the symptoms develop quickly, often starting at night, peak within 24 hours and resolve within 1–2 weeks.32
Patients commonly experience difficulty mobilising during a gout flare.33 Sleep disorders and daytime sleepiness are also frequently seen.34–37 Work absences are higher in people with gout; a Swedish population-based cohort study reported an average work absentee rate over 3 years of 22% in people with gout compared with 14% of matched population controls.38 Gout also has an impact on family and wider community. Family members may be absent from work or education to care for those with gout.29 There is also a financial impact on the family and on businesses when individuals with gout are absent from work or unemployed, with annual loss of income for patients with severe gout estimated to be up to US$4341 per year.39
Risk factors
Majority of hyperuricaemia is the result of reduced renal clearance of urate,40 which can be due to sex, genetic variations, obesity, insulin resistance, medications and kidney disease.41–48 It can also be caused by overproduction due to high dietary purines or increased cell turnover49 50 and intestinal extrarenal underexcretion.11 51
Genetics plays a major role in hyperuricaemia.52 53 Multiple genes have been identified, which contribute to risk of hyperuricaemia, most of which are involved in urate transport.54 Genome-wide association analysis has identified multiple loci associated with gout including ABCG2, SLC2A9, SLC22A11, GCKR and SLC17A1.41 A missense single-nucleotide polymorphism in ABCG2, which is expressed in the gut, is associated with urate concentration and risk of gout.55
Renal underexcretion of urate is a major mechanism of hyperuricaemia. This can be genetic, mediated by variants of urate transporters such as SLC2A9 and SLC22A11, but may also occur in the context of acquired kidney disease.47
Being overweight or obese is the strongest modifiable risk factor for hyperuricaemia and gout. Obesity raises the serum urate level, through both lowering renal urate excretion and increasing urate production.47 48 56 57 Mendelian randomisation studies have shown obesity to be causally associated with serum urate levels,58–60 and weight loss through bariatric surgery61–63 or dietary intervention leads to reductions in serum urate levels.64–66 A recent Global Burden of Disease analyses of 195 countries and territories between 1990 and 2017 found that high body mass index accounted for 53.4% and 48.6% of the years lived with disability for gout in high-income North America and Australasia.10 Early adult obesity in women was associated with a 2.8-fold increased risk of gout compared with nonobese women in a study using data from the Atherosclerosis Risk in Communities (ARIC) study.67
Higher meat intake (particularly red meat), seafood intake and alcohol consumption are associated with an increased risk of hyperuricaemia,68–70 incident gout71 72 and recurrent gout flares73 74 partly because their high purine content raises urate levels, as demonstrated by short-term metabolic experiments of purine loading in animals and humans.75 76 Healthy cardiometabolic diets such as the Mediterranean or Dietary Approaches to Stop Hypertension diet lowered serum urate in secondary analyses of clinical trials64 77–79 and are associated with a lower risk of incident gout, whereas the Western diet is associated with a higher risk.80
Comorbidities
Gout coexists often with metabolic syndrome (63%)81 and is associated with cardiometabolic–renal comorbidities82 and premature mortality.83 In the USA, 74% of those with gout had hypertension, 71% chronic kidney disease stage ≥2, 53% obesity, 26% diabetes, 14% myocardial infarction and 10% stroke.82 It is associated with increased risk of nephrolithiasis (occurring in approximately 24% of patients with gout).82 84
Management
Treatment of a gout flare should be commenced as soon as possible, with nonsteroidal anti-inflammatory drugs, colchicine or glucocorticoids being first-line options for treatment.85 An open-label randomised trial comparing low-dose colchicine 500 mg three times per day for 4 days with naproxen 750 mg immediately, then 250 mg every 8 hours for 7 days found that there was no difference between the two groups in terms of pain intensity over 7 days although side effects were more common in the colchicine group, mainly diarrhoea and headache.86 Another randomised trial comparing oral prednisone and naproxen for monoarticular gout found that either prednisolone 35 mg once a day or naproxen 500 mg two times a day for 5 days were equally effective, and adverse effects were similar between groups.33 Symptomatic treatment for a gout flare includes immobilisation of the joint and use of cold packs.87 Anti-IL-1β monoclonal antibodies have also been found to be effective for relief of gout flares88 and are generally recommended for patients experiencing gout flares where other drugs have caused side effects or were ineffective.85
Long-term use of urate-lowering therapy leads to crystal dissolution,89 90 resulting in suppression of gout flares,91 92 regression of tophi92 and prevention of progressive joint damage.93 Rheumatology societies strongly recommend urate-lowering therapy for patients with tophi, evidence of radiographic damage attributable to gout or frequent gout flares.85 94 Urate-lowering therapy may also have benefit earlier in the disease course.91 Allopurinol is the preferred and most commonly prescribed first-line urate-lowering therapy.85 95 Second-line treatments include febuxostat, another xanthine oxidase inhibitor, probenecid, a uricosuric agent and pegloticase, a recombinant uricase administered intravenously.
A treat-to-target serum urate approach is recommended by the ACR guidelines85 and EULAR recommendations.94 Serum urate monitoring allows the dose of medication to be titrated to a target serum urate of below 6 mg/dL (360 µmol/L) in those with symptomatic gout and often below 5 mg/dL (300 µmol/L) in those with features of severe gout such as tophi.94
Healthcare and workforce considerations
People with gout experience shame in seeking treatment for gout,96 feel stigmatised that their gout diagnosis is associated with perceptions of dietary and alcohol excess and identify they do not have enough information about gout.97
Approaches that support patient understanding of gout, strengthen primary care and focus on strong relationships between clinician and patient are important in management to enable patients to manage gout and continue urate-lowering therapy. Building health literacy is essential, with one study finding that more than half of patients identified a wish to know more about the cause of gout, treatment goals and long-term treatment.98 A randomised controlled trial found that nurse-led care for patients that focused on providing individualised information and engaging patients in shared decision-making led to a reduction in gout flares and tophi.92 Nurse-led care is associated with greater patient satisfaction and better gout knowledge.99 Other models of care, using a protocolised treat-to-target serum urate approach, have also been shown to be effective. A randomised trial of a pharmacist-led service for patients starting allopurinol for gout found that the intervention led to a higher rate of reaching serum urate goal.100 A programme providing education and support to patients with the use of community support workers (kaiāwhina) was also effective.101
Summary
The common language definition of gout encompasses key information relevant to gout as determined by a review of the literature, interviews with patients, healthcare workers and stakeholders and consultation with G-CAN members and stakeholders. After the publication of the English-language version, the definition will be available for translation into other languages by G-CAN members, using the approach recommended by the International Society for Pharmacoeconomics and Outcomes Research (ISPOR) Task Force for Translation and Cultural Adaptation.102 This concise definition can be used in conversations with the lay public, media, NGOs, funders, healthcare providers and other stakeholders.
Data availability statement
Data are available upon reasonable request.
Ethics statements
Ethics approval
Ethical approval was obtained from the University of Auckland Human Participants Ethics Committee and written consent was obtained prior to the interviews; reference number 024225.
Acknowledgments
We thank Rebecca Snyders Hill, Executive Director, Gout, Hyperuricaemia and Crystal-Associated Disease Network (G-CAN), all G-CAN members who provided feedback during the consultation period, and the G-CAN Board members for review and endorsement. We also acknowledge the contributions of participants in the qualitative interviews.
References
- 1.↵
- 2.↵
- 3.↵
- 4.↵
- 5.↵
- 66.↵
- 7.↵
- 8.↵
- 99.↵
- 10.↵
- 11.↵
- 12.↵
- 13.↵
- 14.↵
- 15.↵
- 16.↵
- 17.↵
- 18.↵
- 19.↵
- 20.↵
- 21.↵
- 22.↵
- 23.↵
- 24.↵
- 25.↵
- 26.↵
- 27.↵
- 28.↵
- 29.↵
- 30.↵
- 31.↵
- 32.↵
- 33.↵
- 34.↵
- 35.↵
- 36.↵
- 37.↵
- 38.↵
- 39.↵
- 40.↵
- 41.↵
- 42.↵
- 43.↵
- 44.↵
- 45.↵
- 46.↵
- 47.↵
- 48.↵
- 49.↵
- 50.↵
- 51.↵
- 52.↵
- 53.↵
- 54.↵
- 55.↵
- 56.↵
- 57.↵
- 58.↵
- 59.↵
- 60.↵
- 61.↵
- 62.↵
- 63.↵
- 64.↵
- 65.↵
- 66.↵
- 67.↵
- 68.↵
- 69.↵
- 70.↵
- 71.↵
- 72.↵
- 73.↵
- 74.↵
- 75.↵
- 76.↵
- 77.↵
- 78.↵
- 79.↵
- 80.↵
- 81.↵
- 82.↵
- 83.↵
- 84.↵
- 85.↵
- 86.↵
- 87.↵
- 88.↵
- 89.↵
- 90.↵
- 91.↵
- 92.↵
- 93.↵
- 94.↵
- 95.↵
- 96.↵
- 97.↵
- 98.↵
- 99.↵
- 100.↵
- 101.↵
- 102.↵
Footnotes
Contributors All authors were part of the steering committee, contributed to the development of the protocol, reviewed all data and the common language definition and approved the final version.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests ND reports personal fees and non-financial support from Abbvie, personal fees from Horizon, Janssen, Dyve, Selecta and Arthrosi, grants from Amgen, grants and personal fees from AstraZeneca and personal fees from Hengrui, outside the submitted work. G-CAN is a global gout research consortium, non-profit, supported at arms length by annual funding support from pharma. In the last 36 months, pharma donor support to G-CAN was provided by Horizon, Astra-Zeneca, SOBI, Takeda, CymaBay, Selecta and LG. RT reports other than from G-CAN, during the conduct of the study; personal fees from Astra-Zeneca, SOBI, Horizon, Selecta and grants from Astra-Zeneca, outside the submitted work. JAS has received consultant fees from Crealta/Horizon, Medisys, Fidia, UBM LLC, Trio Health, Medscape, WebMD, Adept Field Solutions, Clinical Care Options, Clearview Healthcare Partners, Putnam Associates, Focus Forward, Navigant Consulting, Spherix, Practice Point Communications, the National Institutes of Health and the American College of Rheumatology. JAS owns stock options in TPT Global Tech, Vaxart Pharmaceuticals and Charlotte’s Web Holdings, Inc. JAS previously owned stock options in Amarin, Viking and Moderna Pharmaceuticals. JAS is on the speaker’s bureau of Simply Speaking. JAS is a member of the executive of Outcomes Measures in Rheumatology (OMERACT), an organisation that develops outcome measures in rheumatology and receives arms-length funding from 12 companies. JAS serves on the FDA Arthritis Advisory Committee. JAS is the chair of the Veterans Affairs Rheumatology Field Advisory Committee. JAS is the editor and the Director of the University of Alabama at Birmingham (UAB) Cochrane Musculoskeletal Group Satellite Centre on Network Meta-analysis. JAS previously served as a member of the following committees: member, the American College of Rheumatology’s (ACR) Annual Meeting. MJB reports grants from Healthwise, a non-profit, outside the submitted work.
Provenance and peer review Not commissioned; externally peer reviewed.