Article Text

Abstract
Objective Non-pharmacological interventions support patients with connective tissue diseases to better cope with and self-manage their diseases. This study aimed to map existing evidence on non-pharmacological interventions in patients with systemic lupus erythematosus (SLE), systemic sclerosis (SSc) and mixed connective tissue diseases regarding content, feasibility and potential suitability in an e-health setting.
Methods A literature search was performed in eight different databases in July 2020. The intervention’s content was extracted using the ‘Better reporting of interventions: template for intervention description and replication (TIDieR) checklist and guide’. A Sankey diagram and descriptive statistics were used to analyse the data and illustrate the relationships between the interventions.
Results Of 8198 identified records, 119 papers were eligible. One hundred and four of them (87.4%) were conducted between 2000 and 2020, mainly in the USA (SLE n=24 (21.2%), SSc n=16 (14.2%)), Brazil (SLE n=8 (7.1%), SSc n=5 (4.4%)) and Italy (SLE n=0 (0%), SSc n=12 (10.6%)). Fifty-two studies (SLE n=24 (21.2%), SSc n=28 (24.8%)) used multicomponent interventions. The single interventions were physical exercises (SLE n=16 (14.2%), SSc n=17 (15.0%)), coaching/counselling (SLE n=11 (18.0%), SSc n=0 (0%)) and education (SLE n=2 (1.8%), SSc n=3 (2.7%)). Primary outcomes focused on physical function (SLE n=1 (0.9%), SSc n=15 (13.3%)), mouth opening in SSc (n=4 (5.9%)) and physical capacity (SLE n=2 (1.8%), SSc n=1 (0.9%)). No interventions for mixed connective tissue disease were found.
Conclusion There was a great variety in the intervention’s content due to differences in body structure, activity limitations and participation restrictions in SLE and SSc. These results highlight the need for personalised, multicomponent, non-pharmacological interventions, which could be delivered as e-health interventions.
- physical therapy modalities
- occupational therapy
- nursing
- lupus erythematosus
- systemic
- scleroderma
- systemic
Data availability statement
Data are available upon reasonable request.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
- physical therapy modalities
- occupational therapy
- nursing
- lupus erythematosus
- systemic
- scleroderma
- systemic
Key messages
What is already known about this subject?
Persons suffering from autoimmune connective tissue diseases (CTD), such as systemic sclerosis (SSc), systemic lupus erythematosus (SLE) and mixed connective tissue diseases (MCTD), experience limitations in physical and mental function, activities of daily life and participation, also leading to a reduced quality of life.
What does this study add?
Consistent with the people’s limitations in their daily routines, various non-pharmacological interventions/programmes exist for SSc and SLE. We did not find non-pharmacological interventions for MCTD.
The most common interventions included patient education, self-management, physical activity/exercise and advice regarding a healthy lifestyle.
How might this impact on clinical practice or further developments?
Multicomponent, non-pharmacological interventions in people with CTDs should be personalised to increase effectiveness.
Multicomponent e-health interventions target the different needs of patients with CTDs.
E-health settings allow patients easier access to specialised health professionals.
Introduction
Connective tissue diseases (CTDs), such as systemic sclerosis (SSc),1 systemic lupus erythematosus (SLE)2 and mixed connective tissue diseases (MCTD),3 are rare chronic autoimmune diseases of unknown aetiology which affect several organ systems, such as the skin, heart, lungs, kidneys, joints, muscles and blood vessels.4 5 Consequently, people with CTDs experience fatigue, pain, reduced mobility/range of motion, shortness of breath and decreased physical function. Thus, CTDs often lead to activity limitations, participation restrictions, psychosocial and economic consequences and reduced health-related quality of life.6–10
Non-pharmacological interventions support patients with CTDs, to better cope with and self-manage their diseases, thereby increasing their quality of life. Non-pharmacological interventions are most commonly delivered by health professionals in rheumatology,11 and several studies have been conducted to establish their effectiveness. For instance, recent reviews demonstrated that being physically active and performing exercises positively impacts fatigue in people with SSc and SLE.12–15 However, these reviews focused only on a specific type of intervention (eg, exercises12–14) or restricted the study designs (eg, included only randomised controlled trials (RCTs)15). Research of interventions using other study designs, such as case studies or qualitative studies, is under-represented in these reviews. To date, a comprehensive overview of different non-pharmacological interventions is lacking. Furthermore, given the small number of patients with SLE and SSc (1–5 individuals per 10.000)16–18 and their particular needs, health professionals who are experts in CTDs are often not easily accessible for these patients especially in rural areas.19 20 Consequently, telehealth interventions or remote consultations with experts have been previously suggested.21 22 Besides, the current COVID-19 pandemic has even more increased the need for remote healthcare. However, telehealth or other remote interventions in CTDs have not yet been explicitly covered in any of the current reviews.
To define the term e-health, we used the definition of the WHO and the description of the term ‘telemedicine’ as defined in the Medical Subject Headings terms by PubMed. The WHO defines e-health as the ‘use of information and communication technologies (ICT) for health’.23 Telemedicine is defined as the ‘Delivery of health services via remote telecommunications’.24 Both definitions include interactive consultative and diagnostic services and comprise terms such as ‘mobile health’, ‘m-health’, ‘telehealth’ and ‘e-health’.
The objective of this study was to map the existing evidence of non-pharmacological interventions in patients with SLE, SSc and MCTD regarding content, feasibility and potential suitability in an e-health setting.
Materials and methods
We conducted a scoping review25 using the guidelines of the Joanna Briggs Institute’s (JBI) approach to evidence-based healthcare methodology to map and describe the content of existing non-pharmacological interventions applicable for patients with SSc, SLE and MCTD. In the second step, we conducted an analysis to provide some insights of effectiveness. Our findings are reported according to the ‘PRISMA Extension for Scoping Reviews (PRISMA-ScR): Checklist and Explanation’.26 The protocol of this scoping review was published on researchgate.net (DOI: 10.13140/RG.2.2.22193.43363).
Search strategy
An initial search, limited to PubMed and CINAHL, was performed (by VR, RF, EJFS) to identify the first articles on this topic to develop a search strategy. In the second step, this search strategy was used to conduct an adapted and more extensive query in eight different databases: MEDLINE (PubMed), EMBASE (OVID), CINAHL (EBSCO), PsycINFO (ProQUEST), the Cochrane Database of Systematic Reviews, OTSeeker, PEDro and SciELO (online supplemental file 1). Further, members of the research group were consulted by email to identify additional grey literature or research that had not been found through the database query. Reference lists of identified papers were searched for any additional relevant articles subjected to the same screening and selection process. There were no exclusions of papers based on publication date.
Supplemental material
Study selection and inclusion criteria
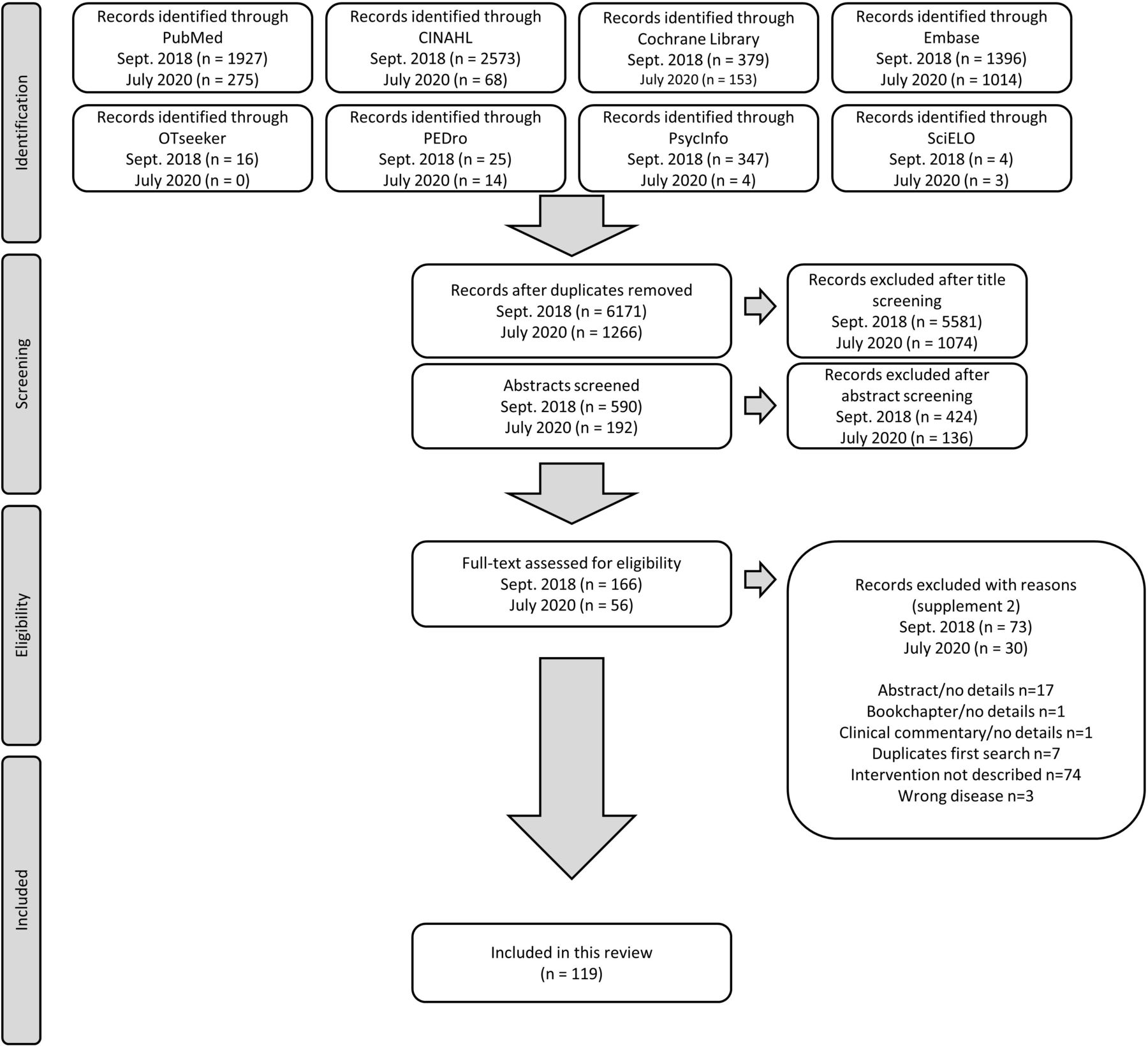
All identified studies/articles/reports in the queries were uploaded into EndNote and duplicates removed. The selection process had two phases. First, two researchers (VR, RF) independently screened the titles whether they met inclusion/exclusion criteria or not, followed by screening the abstracts. A third researcher (TAS) assessed possible disparities in selecting these titles and/or abstracts. Second, the full texts for all selected publications were retrieved and read (VR, EJ). When in doubt whether a paper met the inclusion/exclusion criteria, a third researcher (TAS) was asked to assess the paper and the decision was made by consensus. According to the PRISMA-ScR,26 reasons for the exclusion of full-text studies are provided (online supplemental file 2). The results of the selection are presented in a Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) flow diagram (figure 1).
Supplemental material

Flow chart of the search and selection process performed in September 2018 and updated in July 2020.
The following inclusion criteria guided the selection of publications. Following the JBI,25 the PCC (participants, concept and context) mnemonic and study design were used to screen the studies.
Participants
Studies were included in this scoping review if participants in the study had a diagnosis of SSc, SLE or MCTD.
Concept
Studies were included if any non-pharmacological, non-surgical intervention (such as exercises, education, psychosocial intervention, etc) was investigated (either the development and/or the evaluation of a non-pharmacological intervention). The intervention had to be described in sufficient detail (at least content and setting) to be included.
Context
This scoping review considered all contexts (home care, community services, primary healthcare, hospital settings, etc).
Types of studies
Any quantitative (experimental study/observational) research designs and any qualitative study/design assessing participants’ perspectives on interventions were included. Theoretical studies were excluded.
Data extraction
Study characteristics were extracted using a data extraction form as indicated by the methodology for scoping reviews developed by the JBI.25 The described interventions were further extracted using the ‘Better reporting of interventions: template for intervention description and replication (TIDieR) checklist and guide’.27 Two reviewers (VR, EJ) extracted the data independently. Any disagreements that arose between these reviewers were resolved through discussion until consensus was reached.
Assessment of risk of bias and descriptive analysis
The quality of retrieved RCTs was assessed using the ‘RoB 2: a revised tool for assessing the risk of bias in randomised trials’28 (online supplemental file 3). Other study designs were used to extract information on the intervention’s content but not analysed further regarding risk of bias.
Supplemental material
Due to the heterogeneity of the studies included in this review, we descriptively summarised them.25 We calculated the weighted arithmetic mean of participant age to consider the number of participants in each study in relative weighting. In addition, we used a Sankey diagram to illustrate the relationships between different studies and study characteristics graphically. In a world map, we showed the frequencies of the countries in which the studies were conducted. To summarise and display descriptively the effects of the interventions on outcomes, we created a table in which we listed the interventions in rows and the outcomes in columns. We assigned the studies to the respective combinations of interventions and outcomes (numbers shown indicate the respective study, the colour represents whether the primary outcome was significant between groups (green), significant within groups (yellow) and not significant (red)).
Results
In total, 8198 records on non-pharmacological interventions were identified from the databases. After exclusion of duplicates and title/abstract screening, 226 studies were analysed in full text. One hundred and nineteen papers comprising 113 studies (six studies were published in two articles each29–40) were used for this scoping review. The PRISMA flow chart of the study selection is depicted in figure 1. Following the RoB 2,28 4 out of 42 retrieved RCTs (published in 44 papers) had a low risk of bias, 16 moderate and 22 high (online supplemental file 3). To provide a comprehensive overview of the various forms of intervention, we prepared a detailed summary of the individual study characteristics and interventions (online supplemental files 4 and 5).
Supplemental material
Supplemental material
Study characteristics
Participants
In 58 of the 113 studies (51.3%), the participants were diagnosed with SLE and in 55 (48.7%) with SSc. We did not find any paper dealing specifically with MCTD and non-pharmacological interventions. In total, 5140 people were included (n=4687 (91.2%) female, n=332 (6.5%) male, n=121 (2.3%) gender not reported41–46). However, the authors of one study43 did not report the number of the patients included. Of the participants, 3484 were diagnosed with SLE (intervention groups (IG) n=2664 (77.6%), control groups (CG) n=820 (22.4%)), 1632 with SSc (IG n=1055 (66.7%), CG n=577 (33.3%)) and 58 persons were healthy controls. The allocation of 24 patients diagnosed with SSc in the experimental group and CG of Freedman et al 47 was not reported. The weighted mean (SD) age of patients with SLE was 42.0 (SD±6.8) years (weighted mean age IG 42.3 (SD±6.7); CG 41.4 (SD±6.9)) and 54.8 (SD±4.9) for patients with SSc (IG 54.3 (SD±5.1); CG 55.7 (SD±4.3)). In seven studies, the authors did not report the participant age.42 44 48–52
Date and location of publications, study designs
The majority of the studies were published between 2011–2020 (SLE n=36 (31.9%), SSc n=39 (34.5%)) and 2001–2010 (SLE n=16 (14.2%), SSc n=13 (11.5%)). Forty of all the studies were published in the USA (SLE n=24 (21.2%), SSc n=16 (14.2%)), 13 in Brazil (SLE n=8 (7.1%), SSc n=5 (4.2%)), 12 in Italy (SLE n=0 (0%), SSc n=12 (10.6%)), 10 in Canada (SLE n=5 (4.4%), SSc n=5 (4.4%)) and 8 in the UK (SLE n=3 (2.7%), SSc n=5 (4.4%)) (figure 2). Of the 113 studies, 42 (SLE n=24 (21.2%), SSc n=18 (15.9%)) were RCTs, 20 (SLE n=10 (8.8%), SSc n=10 (8.8%)) were one-group pre/post-test design, 13 (SLE n=7 (6.2%), SSc n=6 (5.3%)) were quasiexperimental studies and 12 (SLE n=2 (1.8%), SSc n=10 (8.8%)) were single-case studies. These study designs and other characteristics are graphically displayed in the Sankey diagram (figure 3).
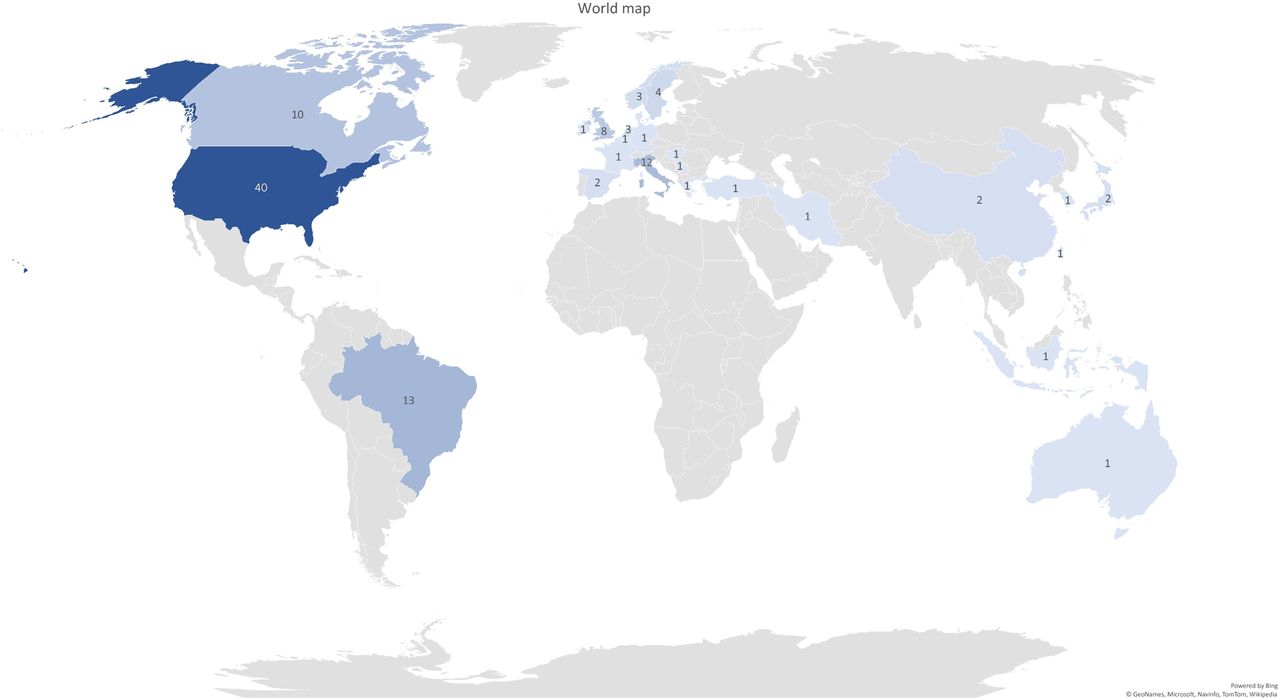
World map evidence representation. This graph shows the frequency of the countries in which the published studies were conducted.
{kind=link}
{kind=link}
{kind=link}
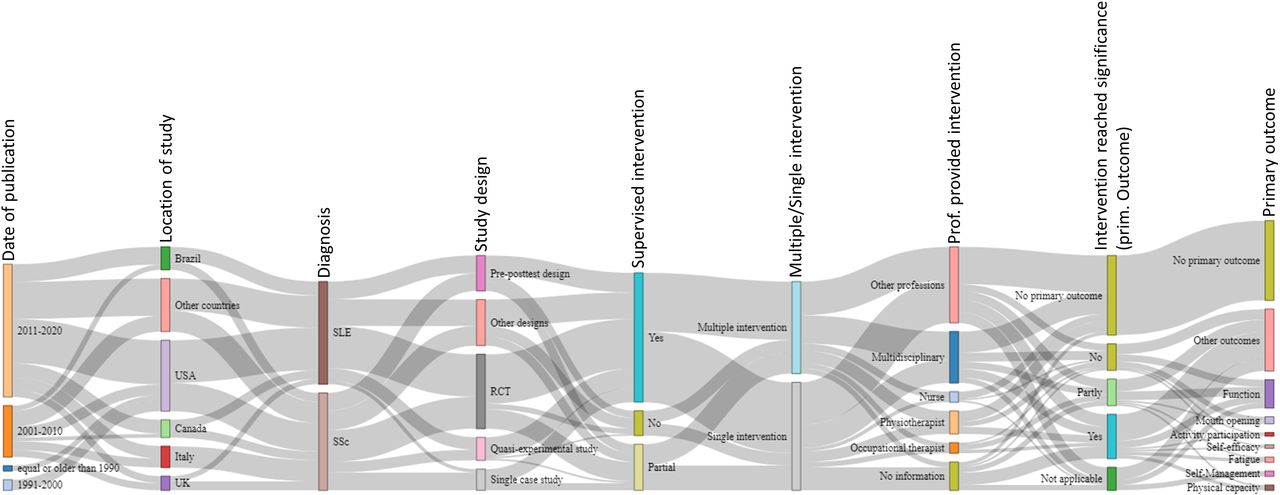
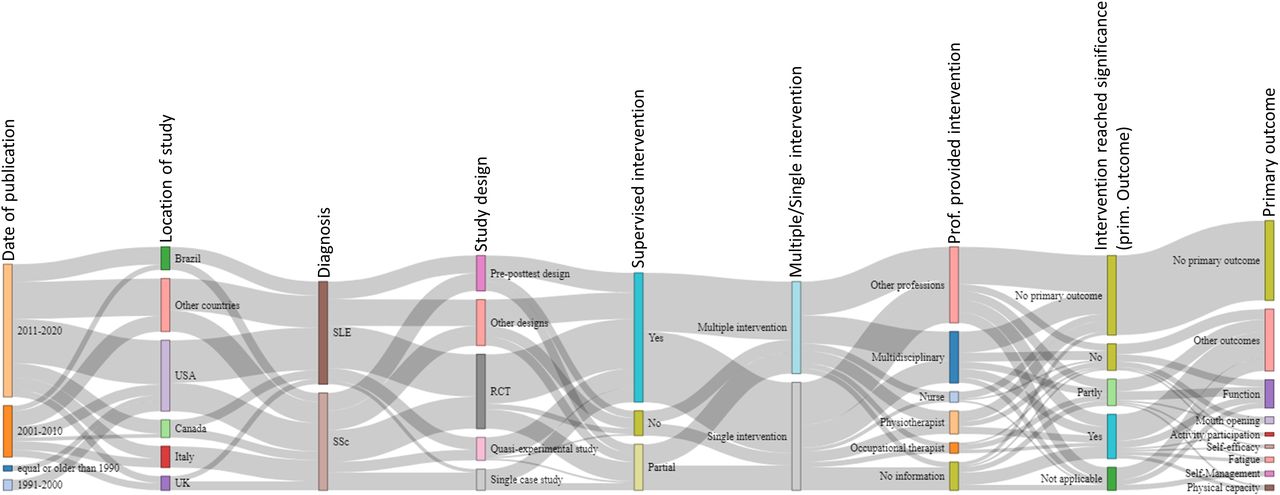
Sankey diagram. This diagram illustrates relationships between different studies and study characteristics graphically. The bars show the study characteristics that were compared between the studies. The grey lines between the bars are reflecting the congruencies and differences between the different studies. The wider the grey connection lines are, the more congruency exists. RCT, randomised controlled trial; SLE, systemic lupus erythematosus; SSc, systemic sclerosis.
Health professionals providing interventions
In 29 (25.7%) of the 113 articles, the interventions were performed by multidisciplinary teams. The other study interventions were performed by physiotherapists (SLE n=6 (5.3%), SSc n=7 (6.2%)), occupational therapists (SLE n=1 (0.9%), SSc n=5 (4.4%)), nurses (SLE n=4 (3.5%), SSc n=2 (1.8%)) or other health professionals (n=43 (38.1%)). In nine studies (8.0%), the interventions were performed by patients/peers (eg, peer counselling). In 16 studies (SLE n=6 (5.3%), SSc n=10 (8.8%)), the authors did not provide clear information on the profession of the health professionals delivering the intervention.7 33 46–48 53–63
Interventions, outcomes, effectiveness
In 52 of the 113 studies (SLE n=24 (21.2%), SSc n=28 (24.8%)), the researchers used multiple or multicomponent interventions to treat their patients, and in 61 studies (SLE n=34 (30.1%), SSc n=27 (23.9%)) single interventions. Of the 61 studies including a single intervention, 33 (SLE n=16 (14.2%), SSc n=17 (15.0%)) included exercises, 11 (SLE n=11 (9.7%), SSc n=0 (0.0%)) coaching/counselling (eg, goal setting, nutrition counselling, peer counselling, physical activity counselling), 5 (SLE n=2 (1.8%), SSc n=3 (2.7%)) education (eg, self-management strategies, cope with the disease) and 4 (SLE n=4 (3.5%), SSc n=0 (0%)) cognitive–behavioural interventions. In the 45 studies (39.8%; including 12 RCTs) where the authors did not clearly define a primary outcome, multiple outcomes and measurements to evaluate the effect of their studies were used (online supplemental file 4). Of the 113 articles found, in 68 (60.8%) a primary outcome was defined. The most frequent primary outcomes were physical function, such as range of motion or hand functioning (SLE n=1 (0.9%), SSc n=15 (13.3%)), mouth opening (SLE n=0 (0%), SSc n=4 (3.5%)), physical capacity (SLE n=2 (1.8%), SSc n=1 (0.9%)), fatigue (SLE n=3 (2.7%), SSc n=0 (0%)) and self-management (SLE n=1 (0.9%), SSc n=2 (1.8%)). As the primary outcome is of utmost importance to decide on the overall result of the study,64 65 we included only these in further analysis of the results. Of the 68 articles, 38 described studies with CG (RCT n=30 (44.1%), quasiexperimental designs n=8 (11.8%)). The studies including a CG and defining a primary outcome are displayed in tables 1 and 2. In these tables, the heterogeneity between the study interventions, outcomes and results becomes apparent. In SLE, 10 of the 19 RCTs (52.6%) showed a significant positive effect. In SSc, it was 7 out of 21 (33.3%). The outcomes were very different and varied greatly.
Interventions/outcomes in studies for people with SLE
Interventions/outcomes in studies for people with SSc
Setting and tailoring the intervention to the patient’s needs
In the 113 articles, 98 (86.7%) of the interventions were either partly (SLE n=5 (4.4%), SSc n=21 (18.6%)) or completely supervised (SLE n=46 (40.7%), SSc n=26 (23.0%)). Supervised in this context refers to face-to-face communication or contact. Partly supervised interventions had an initial face-to-face component, or direct support was provided at the beginning of the treatment. In the course of treatment, this support was constantly reduced. Only 15 of the study interventions (SLE n=7 (6.2%), SSc n=8 (7.1%)) were designed and used as full-distance intervention programmes.38 42 52 66–76
In total, 52 (SLE n=32 (28.3%), SSc n=20 (17.7%)) of the interventions were tailored to the patient’s needs and 29 (SLE n=16 (14.2%), SSc n=13 (11.5%)) to the patient’s physical condition/fitness. ‘Tailored to the needs of the patient’ in this context means that either individual coaching/counselling as part of the intervention or that the measures taken were adapted to the patient’s life situation. ‘Tailored to the patient’s physical condition/fitness’ were interventions, mainly exercises, that were adapted to the patient’s personal ability/capacity, but not to the patient’s life circumstances or preferences. The interventions in 21 studies (SLE n=3 (2.7%), SSc n=18 (15.9%)) were not tailored. In nine (SLE n=5 (4.4%), SSc n=4 (3.5%)) studies, the authors did not provide information on tailoring or individualisation of the interventions. Of the 15 studies where distance intervention programmes were used, only 4 (26.7%) were tailored to the patient’s needs, 2 (13.3%) to the patient’s physical condition/fitness and 8 (53.3%) of the interventions were not tailored.
Discussion
This scoping review with a descriptive analysis provides a comprehensive overview of non-pharmacological interventions for people diagnosed with SLE and SSc regarding content, feasibility and potential suitability in an e-health setting. CTDs impact people’s lives in multifaceted, complex ways. Thus, there is no single non-pharmacological intervention that can simultaneously help these patients reduce pain and fatigue, increase physical function (eg, range of motion, grip strength) and enhance health-related quality of life and cope with the disease. Consequently, the use of multicomponent interventions, regardless of whether in an e-health setting or not, seems essential and clinically relevant. Education, counselling and/or exercises were part of most of the interventions described. In systematic reviews of exercise/physical activity, it has been shown that being more physically active reduces, for example, fatigue, pain and depressive symptoms in people with SLE.77
On purpose, we did not exclude papers based on countries (where the studies were conducted) or publication date to avoid limiting ourselves to intervention types that are culturally specific or that might have changed over time. Our results show that the majority of articles (87.4%) were published between 2000 and 2020. Potential reasons might be the generally increased number of studies on non-pharmacological interventions after 2000 and the growing focus on facilitating more active involvement of patients in managing their healthcare. Thus, interventions requiring active participation, such as patient education, instructions for self-management, physical activity/exercise and advice regarding a healthy lifestyle, have been created and evaluated for feasibility and/or effectiveness.
Most of the interventions described in the studies were either partly or entirely supervised by healthcare providers and/or patients/peers (n=98 (87%)). Thus, these interventions’ feasibility and suitability in an e-health setting are questionable and should be evaluated in further studies. Non-pharmacological interventions are associated with low adherence rates because they often involve lifestyle modifications and require changes in behaviour and daily routine habits, which are challenging to achieve.78 Therefore, interventions that have been developed in a supervised setting cannot be transferred to an unsupervised setting without further validation.78 79 It might be possible that the supervision per se is an important trigger for the people with CTDs to adhere to the treatment and, hence, reach a good/better clinical outcome.
The studies in our review which included tele/e-health interventions focused mainly on patient education and information and were not individually tailored to patients’ needs. In 2021, we would potentially consider a larger variety of interventions suitable for e-health, including supervised non-pharmacological interventions, such as physical exercises, functional training, activity pacing advice, etc. We assume that this is partly due to the fact that the COVID-19 pandemic has substantially advanced the tools, but also our skills in digital healthcare delivery. However, we need to consider equity and access to technologies to not exclude certain groups of people systematically.
People with CTD experience specific clinical manifestations of their disease, and therefore certain limitations in everyday life. To account for this individuality, the interventions should be tailored to the patient’s needs.80 In our results, 81 (72%) of the described face-to-face interventions showed such a tailored approach. However, only 7 out of 15 (47%) e-health programmes were tailored, which indicates a need for development of innovative tools and strategies to facilitate personalisation of these interventions. Artificial intelligence applications might facilitate that e-health interventions become smart. For instance, based on some patient’s characteristics or responses, specific contents might be available or not.
The scoping review methodology allowed us to focus on the content, feasibility and potential suitability in an e-health setting. Compared with a classical analysis of RCTs, the strength of a scoping review is the possibility to include a heterogeneous body of literature, conveying a large number and variety of patients with such particular clinical conditions that would otherwise not be available. By descriptively mapping the content of the studies, we were able to identify research gaps and bring together literature from different disciplines, including intervention programmes with emerging evidence.25
The Sankey diagram analysis shows that in most studies the interventions were partially or fully supervised. Furthermore, it highlights that studies on SSc and SLE are balanced in numbers, but studies on non-pharmacological interventions in people with MCTD are entirely lacking. However, Sankey diagrams do not present meaningful differentiations or comparisons as the widths of the connection lines are similar. Consequently, it was difficult to depict the associations between specific interventions and their outcomes in the diagram. For this purpose, we used the representation in table form. In the tables, we directly contrasted outcomes and types of interventions which is another way to represent knowledge gaps or research needs visually. For example, tables 1 and 2 show that exercise as a single intervention was evaluated in several studies focusing on different outcomes. Other non-pharmacological programmes and interventions were assessed in each case with different outcomes. Because of this heterogeneity, it is difficult to compare the studies and effects with each other. For instance, a self-management programme was assessed only in relation to quality of life but not in relation to other outcomes.45 Further research is needed in this area to make more reliable statements about effectiveness and efficacy.
However, we acknowledge that our review has certain limitations. We focused only on SLE, SSc and MCTD. Furthermore, conclusions on efficacy cannot be made with a scoping review design. While we used a comprehensive search strategy, we excluded studies that did not describe or evaluate a specific intervention. The qualitative studies that we found did not evaluate or describe interventions. They were almost all preliminary studies focused on developing an intervention. Thus, they were excluded because they did not meet the inclusion criteria.
Conclusion
Our results underscore the complexity of treating people with non-pharmacological interventions in CTDs such as SLE and SSc. An interdisciplinary approach tailored to the patient’s needs is essential to support people with SLE and SSc holistically and comprehensively. Education, counselling/coaching and (promoting) exercises/physical activity are important parts of non-pharmacological interventions in people with SLE and SSc and are also suitable for e-health interventions.
Data availability statement
Data are available upon reasonable request.
Ethics statements
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Twitter @FerreiraRJO, @EduardoJFSantos
Contributors VR, TAS, CB and CvdE wrote the manuscript. VR, RJOF, EJ and EJFS performed the search strategies and selected the studies. VR and EJ assessed the risk of bias of RCTs and extracted the data of all studies, and synthesised the results. TAS, CB and CvdE reviewed the processes and excluded articles and tailored the synthesis reports. All other authors suggested and agreed upon the research questions, read the report prior to the manuscript, discussed the results and made contributions to the text. All authors approved the final version of the manuscript.
Funding This project was funded by EULAR (project number HPR038).
Map disclaimer The inclusion of any map (including the depiction of any boundaries therein), or of any geographic or locational reference, does not imply the expression of any opinion whatsoever on the part of BMJ concerning the legal status of any country, territory, jurisdiction or area or of its authorities. Any such expression remains solely that of the relevant source and is not endorsed by BMJ. Maps are provided without any warranty of any kind, either express or implied.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.