Article Text

Abstract
Aim The objective was to examine the prevalence of atherosclerotic cardiovascular disease (ASCVD) and its risk factors among patients with RA with diabetes mellitus (RA-DM) and patients with RA without diabetes mellitus (RAwoDM), and to evaluate lipid and blood pressure (BP) goal attainment in RA-DM and RAwoDM in primary and secondary prevention.
Methods The cohort was derived from the Survey of Cardiovascular Disease Risk Factors in Patients with Rheumatoid Arthritis from 53 centres/19 countries/3 continents during 2014–2019. We evaluated the prevalence of cardiovascular disease (CVD) among RA-DM and RAwoDM. The study population was divided into those with and without ASCVD, and within these groups we compared risk factors and CVD preventive treatment between RA-DM and RAwoDM.
Results The study population comprised of 10 543 patients with RA, of whom 1381 (13%) had DM. ASCVD was present in 26.7% in RA-DM compared with 11.6% RAwoDM (p<0.001). The proportion of patients with a diagnosis of hypertension, hyperlipidaemia and use of lipid-lowering or antihypertensive agents was higher among RA-DM than RAwoDM (p<0.001 for all). The majority of patients with ASCVD did not reach the lipid goal of low-density lipoprotein cholesterol <1.8 mmol/L. The lipid goal attainment was statistically and clinically significantly higher in RA-DM compared with RAwoDM both for patients with and without ASCVD. The systolic BP target of <140 mm Hg was reached by the majority of patients, and there were no statistically nor clinically significant differences in attainment of BP targets between RA-DM and RAwoDM.
Conclusion CVD preventive medication use and prevalence of ASCVD were higher in RA-DM than in RAwoDM, and lipid goals were also more frequently obtained in RA-DM. Lessons may be learnt from CVD prevention programmes in DM to clinically benefit patients with RA .
- arthritis
- rheumatoid
- hypertension
- lipids
- cardiovascular diseases
- atherosclerosis
Data availability statement
No data are available. All data relevant to the study are included in the article or uploaded as supplementary information. The data were pseudonymised by each centre before transferred to the data handling centre at Diakonhjemmet hospital, where it is stored on a central server. The data handling manager is Joe Sexton (joesexton0@gmail.com) and the data centre leader is Anne Grete Semb (a-semb@diakonsyk.no).
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Key messages
What is already known about this subject?
Clinical audits as the Survey of Cardiovascular Disease Risk Factors in Patients with Rheumatoid Arthritis can be applied to monitor data recording and management, measure clinical performance against guideline standards and inform appropriate treatments to improve quality of care in routine practice.
Both patients with rheumatoid arthritis (RA) and diabetes mellitus (DM) are associated with a doubled risk of atherosclerotic cardiovascular disease (ASCVD) compared with the general population.
What does this study add?
The diagnosis of hypertension and hyperlipidaemia was more common among patients with RA with DM than patients with RA without DM.
Among patients with RA with DM, the prevalence of ASCVD was doubled compared with patients with RA without DM.
Appropriate preventive cardiovascular disease (CVD) medication was more widely used and lipid targets more often obtained among patients with RA with DM compared with those without DM.
How might this impact on clinical practice or further developments?
Lessons may be drawn from CVD prevention programmes in DM to benefit patients with RA.
Introduction
The prevalence of diabetes mellitus (DM) is approximately 9% of the world’s adult population, although there are large geographical variations from as low as 2.5% (Republic of Moldovia) to 17% (Egypt).1 2 Furthermore, related to physical inactivity, unhealthy diet and obesity, the prevalence of diabetes is increasing in all age groups. The increased risk of cardiovascular disease (CVD) in patients with DM is well recognised, and there are specific guidelines for CVD prevention and risk factor management in such patients.3
Rheumatoid arthritis (RA) is the most common inflammatory rheumatic disease and is, like DM, associated with increased risk of CVD which is not fully explained by traditional CVD risk factors.4–6 This increased risk in patients with RA may be comparable to that of patients with DM.7 Prevention of atherosclerotic cardiovascular disease (ASCVD) in patients with RA is advocated both by the European League Against Rheumatism8 and other recent recommendations.4 Despite these efforts, ASCVD prevention in patients with RA was noted to be incomplete across the world in our international audit, Survey of Cardiovascular Disease Risk Factors in Patients with Rheumatoid Arthritis (SURF-RA),9 which was motivated by the clinical experience of inadequate CVD risk factor recording and CVD preventive medication use among patients with RA in many countries.
Patients with RA have a high comorbidity burden, and one of the most common comorbidities in RA is DM.10 Compared with the general population, the prevalence of DM among patients with RA seems to be increased,11 although there are conflicting reports.11–15 The increased risk of type 2 DM (T2DM) may be due to lifestyle-related factors such as physical inactivity and overweight, but also related to glucocorticoid use. Concomitant DM among patients with RA is a problem, because these patients have more ASCVD, depression, renal failure and hospital stays compared with patients with RA without DM.16 In patients having both RA and DM, the risk of CVD is nearly tripled.7
Little is known about how DM affects ASCVD risk factor screening and management in patients with RA. Our objective was to examine the prevalence of ASCVD and its risk factors in patients with RA with and without DM, and to evaluate their lipid and blood pressure (BP) goal attainment in primary and secondary prevention based on the results from the large international audit SURF-RA.
Methods
The data in SURF-RA were derived from already established clinical cohorts, as well as from prospective recording in cardiology and rheumatology clinics, between 2014 and 2019. Patients aged >18 years with clinically diagnosed RA were eligible for inclusion. Participating centres were divided into Western Europe, Eastern Europe, North America and Asia.
The following RA-related variables were recorded: rheumatoid factor and anti–citrullinated protein antibody positivity, inflammatory markers including C reactive protein (CRP) and erythrocyte sedimentation rate (ESR), use of antirheumatic medication, as well as Disease Activity Score using 28 joints with ESR. CRP, ESR and lipid values were analysed according to each centre’s laboratory standards.
The presence of self-reported established CVDs, including coronary heart disease (CHD), stroke, peripheral arterial disease, atrial fibrillation and heart failure were registered by the physician in the data collection sheet. The following self-reported risk factors of CVD: smoking, physical activity, known diagnoses of hypertension, hyperlipidaemia and DM, as well as the most recent CVD risk factor measurements including BP, weight, height and waist circumference, were also recorded in the data collection sheet. Lipids, glucose and glycosylated haemoglobin A1c (HbA1c) were recorded if there were measurements within 1 year of examination. We lacked information on fasting status prior to lipid measurements, and both fasting and non-fasting lipid values may have been included. For general CVD risk screening, fasting status has been shown not to influence the prognostic value of blood lipids.17 The use of lipid-lowering agents, antihypertensive treatment and anti-diabetic medication was recorded. Glucose levels or HbA1c were not included in the DM definition, since the rationale was to identify only cases in which DM had been diagnosed and thus necessary preventive measures should have been taken.
The treatment goal of antihypertensive treatment was set at <140/90 mm Hg for patients without DM and <140/80 mm Hg for patients with DM according to the prevailing guidelines at the time of the survey.
At the time of the survey, the European Society of Cardiology recommended that low-density lipoprotein cholesterol (LDL-c) goal should be ≤2.5 mmol/L for patients at high risk of CVD and ≤1.8 mmol/L for patients with established ASCVD.18
To reflect primary and secondary CVD prevention, comparisons of CVD risk factors and their management between patients with RA with and without DM were made separately for those with and without ASCVD (CHD, stroke or peripheral artery disease). To evaluate BP and LDL-c target attainment in primary prevention, we compared patients with RA with and without DM and without known ASCVD but who were using lipid-lowering or antihypertensive medications.
Summary statistics are presented as means or medians, with SD or IQR. To compare independent samples for continuous variables, we used Mann-Whitney U test, and for categorical variables, the χ2 test was applied. Data handling and statistical analyses were performed with R V.4.0.3 (R Foundation for Statistical Computing, Vienna, Austria).
Results
Of the total SURF-RA cohort (n=14 504), we included cases with no missing data on age, sex, presence of DM or ASCVD. Cases with no recorded diagnosis of DM but recorded use of insulin or oral antidiabetic medication were excluded (n=83). The total study cohort comprised 10 543 individuals from 19 countries across three continents. The proportion of patients from different world regions and ethnic groups is shown in table 1. RA-related factors and use of antirheumatic medication are shown in online supplemental table 1.
Supplemental material
Characteristics and medications of patients with rheumatoid arthritis (RA) with or without atherosclerotic cardiovascular disease (CVD) and with or without diabetes mellitus (DM)
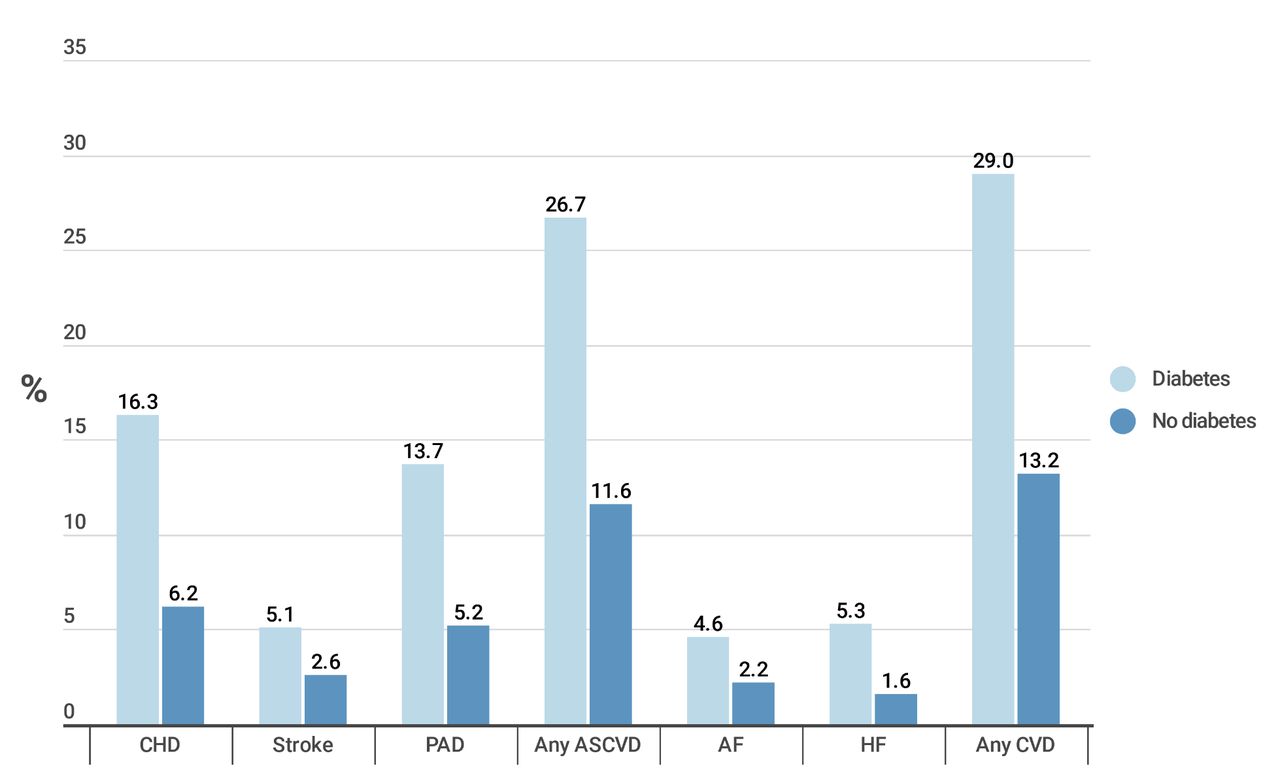
In most countries, 8%–15% of patients with RA had concomitant DM (figure 1). A total of 27% of the patients with RA with DM had ASCVD compared with 12% of patients with RA without DM (figure 2). CHD, stroke, peripheral artery disease, atrial fibrillation or heart failure were all more common among patients with RA with DM compared with patients with RA without DM. The total study population was divided into those with a diagnosis of ASCVD (n=1434) and those without (n=9109).

Percentage of patients with RA with concomitant diagnosis of diabetes mellitus by country. The number over the bars are %. RA, rheumatoid arthritis.

Prevalence of cardiovascular diseases (CVDs) among patients with rheumatoid arthritis with diabetes mellitus (n=1381) and without diabetes mellitus (n=9162). AF, atrial fibrillation; ASCVD, atherosclerotic cardiovascular disease; CHD, coronary heart disease; HF, heart failure; PAD, peripheral artery disease.
Patients with RA without ASCVD
Among the patients with RA without ASCVD, there were 1012 cases who had concomitant DM and 8097 cases who did not. There were no differences in sex distribution, but patients with DM were slightly older than those without DM (table 1). The most common type of DM was T2DM (91.4%), while 49 patients (4.8%) had type 1 DM and 38 (3.8%) had no record of DM type. Only 386 (38.1%) of patients with RA with DM had a measurement of HbA1c within 1 year before the survey inclusion (median (IQR) HbA1c 50 (42–61) mmol/mol) (table 2). Among the patients classified as not having DM, only 1179 (14.6%) had a measurement of HbA1c within the previous year, and a small proportion of them had elevated HbA1c as a sign of either impaired glucose regulation with HbA1c of 42–47 mmol/mol (n=100) or undiagnosed DM with HbA1c 48 mmol/mol or higher (n=17).
Cardiovascular disease risk factors among patients with rheumatoid arthritis (RA) with or without atherosclerotic cardiovascular disease (CVD) and with or without diabetes mellitus (DM)
The proportion of patients with a diagnosis of hypertension, hyperlipidaemia, use of lipid-lowering or antihypertensive agents was higher among patients with RA with DM than among those without (table 1). Patients with RA with DM had on average higher body mass index (BMI) and they were less often moderately or more than moderately physically active than those without DM (table 2). Patients with RA with DM were less frequently current smokers than patients with RA without DM (13% vs 17%).
Lipid measurements were available in 65% of the patients with DM and in 55% of patients without DM (table 2). Levels of LDL-c, high-density lipoprotein cholesterol (HDL-c) and total cholesterol were lower in the DM group, whereas triglycerides were higher compared with patients with RA without DM. Overall, patients with RA with DM and without ASCVD, but on lipid-lowering treatment for primary prevention purposes had lower LDL-c compared with patients without DM, and this difference was statistically significant in subpopulations from Western Europe, Eastern Europe and North America (figure 3A).

{kind=link}
{kind=link}
{kind=link}
(A–D) Treatment target attainment for LDL-c and systolic BP among patients with RA with or without diabetes in primary prevention and secondary prevention by world regions. (A) LDL-c level in RA cases without ASCVD but with lipid-lowering agents for primary prevention. (B) LDL-c level in RA cases with ASCVD and in need of secondary prevention. (C) Systolic BP among patients with RA with antihypertensive drug treatment but no ASCVD. (D) BP among patients with RA with ASCVD. Red dashed lines depict commonly used treatment targets. Differences between patients with or without DM were compared with Mann-Whitney U test. The boxplots represent the distribution of measurements, with median as the black horizontal line in the middle of the box, IQR from 25th (Q1) to 75th (Q3) percentiles as the height of the box, and whiskers as Q1−1.5*IQR and Q3+1.5*IQR. Outliers are represented by grey dots. ASCVD, atherosclerotic cardiovascular disease; BP, blood pressure; DM, diabetes mellitus; LDL-c, low-density lipoprotein cholesterol; RA, rheumatoid arthritis.
BP measurements were available for 77% of the patients with RA with DM and 70% of the patients with RA without DM (table 2). Systolic BP was slightly higher among patients with RA with DM compared with those without (median difference 5 mm Hg), whereas diastolic BP was lower. We also compared systolic BP of patients with RA with and without DM receiving antihypertensive medication (figure 3C), and observed no significant differences.
Patients with RA with ASCVD
Of the patients with RA with ASCVD, 369 had concomitant DM and 1065 did not. There were no significant differences in age, sex or distribution across world regions in patients with ASCVD with and without DM (table 1). Of the patients with RA with DM, 352 (95.4%) had T2DM, 12 (3.3%) had type 1 DM and 5 (1.4%) unknown type. Only 46.3% had a measurement of HbA1c within 1 year prior to survey inclusion (median (IQR) HbA1c of 49 (42–58) mmol/mol) (table 2). Of the patients classified as not having DM, only 13.3% had a HbA1c measurement within a year, and there were 21 cases with HbA1c of 42–47 mmol/mol and 3 cases with HbA1c above the diabetic threshold (48 mmol/mol or higher). Of ASCVD subtypes, CHD/stroke/peripheral artery disease was present among 61.0%/19.2%/51.2% of the patients with RA with DM versus 53.5%/22.2%/44.4% of the patients without DM, respectively (figure 2).
Proportions of patients with a diagnosis of hypertension, diagnosis of hyperlipidaemia and use of lipid-lowering or antihypertensive drugs including beta-blockers and ACE-inhibitors/angiotensin receptor blockers were higher for the patients with RA with ASCVD and DM compared with those without DM (table 1). Of note, of the patients with RA with ASCVD but no DM compared with patients with RA with ASCVD and DM, only 53% versus 72% respectively reported use of statins. Patients with RA with ASCVD and DM had higher BMI than patients without DM (table 2). There were no significant differences in physical activity level or smoking status.
Lipid measurements were available in 73% of patients with DM and in 65% of patients without DM with ASCVD (table 2). Comparable to the data on patients without ASCVD, levels of LDL-c, HDL-c and total cholesterol were lower whereas triglycerides were higher among those with DM compared with those without. Overall, neither the majority of patients with RA with ASCVD with DM nor without DM reached the treatment target of LDL-c <1.8 mmol/L in any of the world regions (figure 3B). On average, LDL-c levels were closest to the treatment target in North America and highest in Eastern Europe. Overall, patients with DM had lower LDL-c compared with patients without DM, and the difference was statistically significant in subpopulations from North America, Eastern and Western Europe (figure 3B).
BP measurements were available for 87% of the patients with DM and 83% of the patients without DM. Diastolic BP was slightly but statistically significantly lower among patients with DM compared with patients without DM (table 2). For the majority of patients across world regions, systolic BP was under the commonly used treatment target of 140 mm Hg (figure 3D). No consistent differences in systolic BP between patients with or without DM were noted.
Discussion
To our knowledge, this is the first report comparing ASCVD risk factors, prevention and attainment of guideline-recommended treatment targets in patients with RA with and without DM. The major finding in this audit was that the treatment results for primary and secondary ASCVD prevention were superior in patients with RA with DM compared with patients with RA without DM. This was especially reflected in the higher proportion of patients with RA with ASCVD and DM reaching their lipid goals compared with patients with RA with ASCVD but without DM. Furthermore, screening of many CVD risk factors, especially hypercholesterolemia and DM or pre-diabetes, among patients with RA was inadequate and needs to be improved globally. Our findings highlight the importance of raising awareness of the increased risk of CVD in patients with RA, which can be achieved by information campaigns directed at patients and their spouses and all categories of healthcare personnel.
In this large audit of ASCVD and its risk factors in patients with RA, we have shown that patients with RA with DM have more than two times the frequency of ASCVD compared with patients with RA without DM. The increased risk of myocardial infarction in patients with RA has been known for decades and was reported by Holmqvist et al6 to be increased by 40% compared with the general population, despite the overall reduction in ASCVD since the 1970s. Furthermore, in line with our findings, a Danish nationwide cohort study including patients from 1997 to 2006 has reported a roughly doubled myocardial infarction incidence rate among patients with RA with DM compared with those without.7 We point out that our contemporary data imply that this increased ASCVD risk linked to the combination of having both RA and DM has not improved since then.
Despite the knowledge of the increased risk of ASCVD in patients with RA, their CVD risk factors often remain underdiagnosed and they receive poorer CVD prevention than general population.19 20 We found that patients with RA with DM more often used lipid-lowering and antihypertensive medications compared with their counterparts without DM, regardless if they had ASCVD or not. This may reflect the well-developed CVD preventive programmes in patients with DM. This patient group has specialised clinics, nurses, information materials and screening routines in many countries, although there may be variations in medical handling of DM across geographical regions. Despite the fact that statins are safe and effective among patients with RA,21 22 an alarmingly low proportion (roughly 50%) of patients with RA without DM but with ASCVD used statins, and only a quarter reached the LDL-c target of ≤1.8 mmol/L. This could be related to clinical inertia, and warrants attention to initiation and adherence of lipid-lowering treatment. Also among the general population, CVD risk factors are strikingly common, and primary and secondary prevention are often inadequate.23–25 A European 18-country observational study of patients using lipid-lowering agents showed that the 2016 LDL goals were attained by only 22% and 45% of the very high-risk primary and secondary prevention patients, respectively.23 In the EUROASPIRE V study across 27 countries, 29% of patients with CHD reached LDL target of <1.8 mmol/L.24
The prevalence of diagnosed DM in patients with RA across countries varied mostly from 8% to 15%, although there were a few exceptions with DM prevalence as low as 2%. Our findings are comparable to results from other RA cohorts from Italy15 (DM prevalence 13.6%) and the USA (10.4%).26 However, reflecting poor risk factor monitoring, HbA1c measurements were found in only less than one out of six patients with RA without DM, and thus we speculate that undiagnosed DM may be a considerable problem among patients with RA. Widdifield and colleagues have reported that only half of the individuals with RA were screened for CVD risk factors, including HbA1c.27 Importantly, an association between RA and undiagnosed DM has been reported by a German cross-sectional study.28 Of note, we found 20 patients without known diabetes but with diabetic HbA1c (range 48.6–58.5 mmol/L, median 49.7), suggesting that HbA1c levels slightly over the diabetic threshold may not always receive attention.
The low frequency of lipid measurements in our survey reflects poor CVD risk factor management. This may be due to insufficient knowledge among health personnel,29 and due to diffusion of responsibility for CVD risk evaluation between general practitioners, cardiologists and rheumatologists. The higher lipid goal attainment in patients with RA with DM may be related to the high focus on prevention of microvascular and macrovascular complications beyond glycaemic control in DM care, which is emphasised in DM treatment guidelines3 30 31 and is well-implemented in primary care settings. Among patients with DM, CVD risk management may be taken care of by primary care physicians, internists or endocrinologists, whereas for patients with RA, CVD risk management is mostly carried out by primary care physicians or rheumatologists.32 This may also explain why pharmacological secondary prevention, including lipid-lowering drugs, beta-blockers and ACE-inhibitors/angiotensin receptor blockers, was more frequent among the patients with RA with DM compared with those without. In addition, presence of DM may increase adherence to statins.33
The treatment goal of antihypertensive treatment was set at <140/90 mm Hg for patients without DM and <140/80 mm Hg for patients with DM according to the prevailing guidelines at the time of the survey, which is a modest approach compared with the most recent European guidelines on hypertension, which define different targets depending on age and side effects.34 Surprisingly, based on single measurements BP was well controlled in patients with RA. This is in contrast to patients with RA from a US report, where 40% had BP >140/90 mm Hg,14 and to large populations with established CHD such as in Eurospire V survey (42% had BP >140/90 mm Hg) and in SURF-CHD survey (40% not at BP target).24 35
There are several limitations of a survey such as SURF-RA. First, the variations of the recorded prevalence of ASCVD risk factors across the three world continents may reflect the various settings for such risk factor recording. For example, the risk factors reported from North America were mostly extracted from primary care patient records, while SURF-RA centres in Western Europe were mostly rheumatology outpatient clinics and some cardiology outpatient clinics. Some of the data were extracted from pre-existing registries, which may explain the differences in missing data across the geographic regions. The rates of missing data on CVD risk factors highlight that, even in rheumatology centres with a focus on CVD prevention, the screening and recording of these crucial clinical variables are incomplete. This underlines the importance of increasing the awareness of this clinical field. The centres participating in the audit were either invited through the ATACC-RA network (www.atacc-ra.com) or invited through conference contacts. Therefore, the representativeness of the cohorts in relation to nations, ethnic groups or geographic regions is not complete. In addition, the number of patients included from the various regions differed, with more patients recruited from North America and Western Europe. Another limitation is that we used the treatment goals of European recommendations in evaluating treatment target attainment across world regions. Medication adherence was not evaluated and this may have influenced goal attainment. Participating centres did not share standardised instruments for measurements, for example, same BP monitors, height and weight measuring scales and laboratory measurements. Despite these limitations, clinical audits are valuable tools for improving clinical performance in implementing guideline-recommended procedures.
Conclusion
The use of CVD preventive medications and the presence of ASCVD was higher in patients with RA with DM than in patients with RA without DM. Lipid goals were also more frequently obtained in patients with RA with than without DM in both primary and secondary prevention. Based on this survey, special attention is needed to ensure that patients with RA with ASCVD reach their lipid goals. Data from the SURF-RA indicate that CVD prevention in DM is better implemented compared with patients with RA, and lessons may be drawn from the existing CVD prevention programmes in DM to enhance CVD prevention among patients with RA.
Data availability statement
No data are available. All data relevant to the study are included in the article or uploaded as supplementary information. The data were pseudonymised by each centre before transferred to the data handling centre at Diakonhjemmet hospital, where it is stored on a central server. The data handling manager is Joe Sexton (joesexton0@gmail.com) and the data centre leader is Anne Grete Semb (a-semb@diakonsyk.no).
Ethics statements
Ethics approval
This is an audit of quality assurance of data in patient journals. The data were pseudonymised. The SURF-RA study has been approved by the Data Protection Officer (DPO) at the Oslo University Hospital-Ullevaal (2017/7243), and a general data protection regulation evaluation was performed by the DPO at Diakonhjemmet Hospital (10/10-2018), Oslo, Norway. Following this evaluation, an informed consent from participants was considered not necessary. Each participating centre was responsible for obtaining the correct regulatory approval for participating in SURF-RA.
Acknowledgments
We are grateful and in debt to all those clinicians and health personnel who have participated in gathering information for the SURF-RA.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Twitter @DurgaPrasannaM1
Contributors AGS contributed to conception, design, acquisition, analysis, interpretation and drafted including critically revised and gave final approval of the manuscript, AMK and SR contributed to conception and design of the analyses, interpretation, drafted, critically revised and gave final approval of the manuscript, JS contributed to design, acquisition, analysis, interpretation, critically revised and gave final approval of the manuscript, EI, GW contributed to conception, acquisition, interpretation, critically revised and gave final approval of the manuscript, IG, PvR, GK, CC contributed to conception, design, interpretation, critically revised and gave final approval of the manuscript, SR-D, GAK, MAG-G, PPS, BK, CH, MSS, VP-R, DAG-D, SM contributed to conception, design, acquisition, interpretation, critically revised and gave final approval of the manuscript, MT, AL, DV, PD, PF, DPM, AAB, RM, EMM, DG, LK, TVP, AT, MT, MV, JL, PH, TS contributed to conception, acquisition, interpretation, critically revised and gave final approval of the manuscript.
Funding The work was supported by grants from the South Eastern Regional Health Authorities of Norway (2013064 for AGS and 2016063 for SR) and FOREUM (the Foundation for Research in Rheumatology for AMK). Further support was through a collaborative agreement for independent research from Eli Lilly who had no role in the study design, data collection and analysis, decision to publish or preparation of the manuscript.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.