Article Text

Abstract
Objective Genetic determinants of fibrin clot formation and fibrinolysis have an impact on local and systemic inflammatory response. The aim of the present study was to assess whether coagulation-related genotypes affect the predictive value of C-reactive protein (CRP) in regards of radiographic spinal progression in axial spondyloarthritis (axSpA).
Methods Two hundred and eight patients with axSpA from the German Spondyloarthritis Inception Cohort were characterised for genotypes of α-fibrinogen, β-fibrinogen (FGB) and γ-fibrinogen, factor XIII A-subunit (F13A) and α2-antiplasmin (A2AP). The relation between CRP levels and radiographic spinal progression defined as worsening of the modified Stoke Ankylosing Spondylitis Spinal Score (mSASSS) by ≥2 points over 2 years was assessed in dependence on the respective genetic background in logistic regression analyses.
Results Overall, CRP was associated with mSASSS progression ≥2 points: time-averaged CRP ≥10 mg/L, OR: 3.32, 95% CI 1.35 to 8.13. After stratification for coagulation-related genotypes, CRP was strongly associated with mSASSS progression in individuals predisposed to form loose, fibrinolysis-susceptible fibrin clots (FGB rs1800790GG, OR: 6.86, 95% CI 2.08 to 22.6; A2AP 6Trp, OR: 5.86, 95% CI 1.63 to 21.0; F13A 34Leu, OR: 8.72, 95% CI 1.69 to 45.1), while in genotypes predisposing to stable fibrin clots, the association was absent or weak (FGB rs1800790A, OR: 0.83, 95% CI 0.14 to 4.84; A2AP 6Arg/Arg, OR: 1.47, 95% CI 0.35 to 6.19; F13A 34Val/Val, OR: 1.72, 95% CI 0.52 to 5.71).
Conclusions Elevated CRP levels seem to be clearly associated with radiographic spinal progression only if patients are predisposed for loose fibrin clots with high susceptibility to fibrinolysis.
- spondylitis
- ankylosing
- inflammation
- arthritis
Data availability statement
Data are available upon reasonable request.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Key messages
What is already known about this topic?
C-reactive protein (CRP), presence of syndesmophytes and smoking are predictors for radiographic spinal progression in axial spondyloarthritis.
Inflammation and tissue repair are involved in pathogenesis of axial spondyloarthritis.
Genetic determinants of fibrin clot formation and fibrinolysis influence inflammatory processes.
What does this study add?
The predictive potential of CRP in respect of radiographic spinal progression in axial spondyloarthritis depends on genotype (constellations) influencing fibrin clot formation and fibrinolysis.
Elevated CRP levels at baseline are associated with radiographic spinal progression in axial spondyloarthritis only if patients are predisposed for loose fibrin clots with low antifibrinolytic capacity.
How might this impact on clinical practice or future developments?
Enhancement of prognostic evaluation of patients with axial spondyloarthritis by considering their genetic background could help to improve risk stratification and to focus treatment strategies.
Introduction
Structural damage in the spine in patients with axial spondyloarthritis (axSpA) is—together with inflammatory activity—one of the main determinants of spinal mobility and function, parameters, which are relevant for long-term outcome of disease.1–4 Even though the pathophysiology of structural spinal damage in axSpA is not fully understood, current data suggest that initial inflammation in vertebral bodies is followed by activation of repair processes with formation of fibrous tissue, activation of osteoblasts and formation of new bone.5 New spinal bone formation in patients with axSpA is usually assessed on plain spinal X-rays and, therefore, referred to as radiographic spinal progression. A number of predictors of radiographic spinal progression have been identified, including already existing syndesmophytes, cigarette smoking, male sex, manual work and high inflammatory activity reflected by elevated C-reactive protein (CRP), high Ankylosing Spondylitis Disease Activity Score and active inflammatory or postinflammatory changes on MRI.6–14
Fibrin and factor XIII play essential roles in inflammatory processes and bone development.15 16 Fibrin gel properties are affected by inflammation and genetic factors.15 17 18 Reciprocally, genetic factors affecting fibrinogen synthesis (α-fibrinogen, FGA, β-fibrinogen, FGB, γ-fibrinogen, FGG), fibrin clot formation (factor XIII A-subunit/B-subunit) and fibrinolysis resistance (α2-antiplasmin, A2AP) influence both local and systemic inflammatory activity.19–21 Thus, highly frequent genotype constellations predisposing for tight, fibrinolysis-resistant fibrin clot structures attenuate systemic inflammatory response as measured by CRP and those related to looser fibrin gels, which are more susceptible for fibrinolysis, are associated with stronger CRP responses.20 22–24
As genetic factors affecting fibrin clot properties influence CRP responses19 and processes with potential impact on reactive bone remodelling,15 25–27 this topic gives a target for evaluating its effect on CRP-based prediction models in axSpA. In the GErman SPondyloarthritis Inception Cohort (GESPIC), approximately 14% of patients exhibited radiographic spinal progression over 2 years and about 2/3 of progressing patients presented with CRP elevations.7 Currently, it is widely unclear, why some patients with unelevated CRP exhibit a progress and what differentiates progressing and nonprogressing patients with axSpA with high inflammatory activity.
The objective of this study was to investigate the performance of the above-mentioned CRP-based prediction model for radiographic spinal progression in patients with axSpA,7 when considering the genetic background with influence on fibrin clot formation and fibrinolysis.
Methods
Patients and clinical assessment
Patients with axSpA who completed a 2-year clinical and radiographic follow-up in GESPIC were studied.7 28 They were included in GESPIC if they had definite axSpA, either radiographic (r-axSpA, also referred to as ankylosing spondylitis) or non-radiographic form (nr-axSpA). All patients included were of European Caucasian origin. Clinical and laboratory data were collected at baseline, and every 6 months thereafter, radiographic data (cervical spine lateral view, lumbar spine lateral and anteroposterior views) were collected at baseline and after 2 years. Treatment of patients with GESPIC has been done according to local rheumatologists, without any limitations28 (table 1).
Baseline demographic and clinical characteristics of included patients with axial spondyloarthritis
Assessment of radiographic spinal progression
Cervical and lumbar radiographs (lateral views) were scored independently by two trained readers (DP and HH) in concealed and randomly selected order according to modified Stoke Ankylosing Spondylitis Spinal Score (mSASSS).29 Final mSASSS was calculated as mean of two scores produced by individual readers. Meaningful radiographic spinal progression was defined as worsening of mSASSS by ≥2 points after 2 years. In addition to mSASSS, we assessed syndesmophytes on both lateral views and lumbar anteroposterior view as described previously.7
Genotyping
Patients were analysed for fibrinogen genotypes influencing fibrinogen levels30–32: FGA rs6050A>G, FGA rs2070006G>A, FGA rs2070016T>C, FGB rs1800788C>T, FGB rs1800790G>A, FGG rs1049636T>C. Variants of F13A, F13B15 17 33 and A2AP34 35 were characterised, which influence fibrin cross-linking and/or susceptibility to fibrinolysis: F13A Val34Leu (rs5985G>T), F13A Tyr204Phe (rs3024477A>T), F13B His95Arg (rs6003A>G), A2AP Arg6Trp (rs2070863C>T). Genotypes were determined using LightSNiP assays (TIB MOLBIOL, Berlin, Germany).
Statistics
In logistic regression analyses, radiographic spinal progression (mSASSS by ≥2 points after 2 years) was used as dependent variable. A priori, risk covariable CRP elevation was defined either (1) as time-averaged CRP level (CRPmean) from up to five time points >6 mg/L7 or (2) ≥10 mg/L22. Additionally, CRP levels at baseline (CRPbaseline) ≥10 mg/L were used for categorisation. Analyses were adjusted for presence of syndesmophytes at baseline, smoking, presence of definite radiographic sacroiliitis according to modified New York criteria and sex. Analyses were performed separately for subgroups defined by presence/absence of minor allele carriage of respective genotypes. ORs with 95% confidence intervals (95% CIs) were calculated and given for presence/absence of the genotype tested, respectively. Subsequently, interaction terms between CRP and the stratifying variable (ie, presence/absence of minor allele) were included in logistic regression analyses to test for interaction between both variables. OR and 95% CI of interaction terms as well as p values for homogeneity were given. Hereby, a p<0.05 indicates that the relation between CRP and radiographic spinal progression significantly differs between both genotype-defined subgroups.
For testing our hypothesis, assessment was carried out in stepwise order: Primarily, FGB rs1800790G>A genotype with strong influence on fibrinogen synthesis36 was used for subgrouping. Second, subgrouping was performed by F13A Val34Leu,17 A2AP Arg6Trp35 and F13B His95Arg,37 which modulate influence fibrin cross-linking and/or fibrinolysis resistance. Subsequently, composite prothrombotic constellations of fibrinogen and F13A Val34Leu genotypes (PFGB rs1800790G>A and PFGA rs2070016T>C) were studied (online supplemental text).20 These prothrombotic constellations of fibrinogen and F13A Val34Leu genotypes predispose for highly crosslinked, dense (so-called prothrombotic) fibrin structures and influence CRP responses.20 Finally, additional fibrinogen genotypes were addressed.20
Supplemental material
To account for measurement errors in analyses using dichotomised mSASSS change,38 linear regression analyses were carried out with mSASSS change as continuous dependent variable that incorporates both, positive (progression) and negative (usually considered as measurement error of reading exercised blinded for time point) values of mSASSS change (online supplemental text). Performance of CRPbaseline≥10 mg/L in predicting mSASSS change was visualised in cumulative probability plots (figure 1). We used STROBE cohort reporting guidelines.39
Patient and public involvement
Representatives of the German patient with axSpA organisation provided advice on outcomes in GESPIC and recommend ways to facilitate study participation while minimising burden of study visits.
Results
Clinical characteristics and genotype distribution
A total of 208 of 210 patients with follow-up after 2 years were genotyped and included in this study. Baseline characteristics are presented in table 1. A total of 30 patients (14.4%) demonstrated radiographic spinal progression defined as worsening of the mSASSS (≥2 points) after 2 years. Genotype distributions in the total study population as well as in r-axSpA and nr-axSpA patients are given in online supplemental table 1.
Supplemental material
Relation of radiographic spinal progression and time-averaged CRP levels in dependence on FGB rs1800790G>A genotype
According to the predictive model described earlier,7 we performed analyses in respect of radiographic spinal progression stratified for FGB rs1800790 A-allele carriage using time-averaged CRP levels (CRPmean) categorised for >6 mg/L7 or ≥10 mg/L22 (table 2).
Analysis of parameters associated with radiographic spinal progression (worsening of mSASSS by ≥2 points after 2 years) in axial spondyloarthritis stratified by FGB rs1800790G>A genotype
As described earlier, using the model without genotype-defined subgrouping, CRPmean (>6 mg/L) was associated with radiographic spinal progression (mSASSS ≥2 points)7: OR: 2.56, 95% CI 1.03 to 6.35. When analysing genotype-defined subgroups separately, this association considerably depended on underlying FGB rs1800790G>A genotypes. In FGB rs1800790GG wild types, CRPmean exhibited a strong association with mSASSS progression (OR: 5.64, 95% CI 1.56 to 20.3), whereas it was completely missing in carriers of FGB rs1800790 A-allele (OR: 0.99, 95% CI 0.20 to 4.92). However, heterogeneity between both subgroups was not statistically significant (interaction term, OR: 0.28, 95% CI 0.04 to 1.76, p for homogeneity: 0.17). In respect of presence of syndesmophytes at baseline or current smoking as predictors of radiographic progression an opposite effect could be found. In both cases, associations with radiographic progression were restricted on carriers of the FGB rs1800790 A-allele (syndesmophytes, OR: 12.2, 95% CI 2.12 to 70.5; current smoking, OR: 6.08, 95% CI 1.18 to 31.2).
Based on CRPmean≥10 mg/L, the strength of association between CRPmean and mSASSS progression in FGB rs1800790GG wild-types was further increased (OR: 6.86, 95% CI 2.08 to 22.6) and heterogeneity between both subgroups was more pronounced compared with a cut-off level of CPRmean>6 mg/L (interaction term, OR: 0.22, 95% CI 0.03 to 1.42, p for homogeneity: 0.11) (table 2). Results of linear regression analyses are given in online supplemental table 2. In following sections, analyses were based on CRPmean≥10 mg/L.
Supplemental material
Analyses on relation between time-averaged CRP levels and radiographic spinal progression in dependence on F13A, A2AP and F13B genotypes
We tested whether variability of other genes related to fibrin cross-linking and/or fibrinolysis resistance influences association between CRPmean (≥10 mg/L) and radiographic spinal progression. Interestingly, for these genotypes, similar effects as for FGB rs1800790G>A could be found in the prognostic model (table 3).
Analysis of parameters associated with radiographic spinal progression (worsening of mSASSS by ≥2 points after 2 years) in axial spondyloarthritis stratified by A2AP Arg6Trp, F13A Val34Leu or F13B His95Arg genotype
Carriers of the respective minor allele(s) of F13A Val34Leu, A2AP Arg6Trp or F13B His95Arg exhibited a strong, highly significant relation between elevated CRPmean (≥10 mg/L) and radiographic progression. In contrary, in corresponding wild-type associations of CRPmean and mSASSS progression were clearly diminished. Results of linear regression analyses are given in online supplemental table 2.
Relation of radiographic spinal progression and time-averaged CRP levels in dependence on potentially prothrombotic genotype constellations
As the effect of fibrinogen and factor XIII genetics on inflammatory processes results from their interactive influence on fibrin clot formation, we assessed the performance of the predictive model in dependence of prothrombotic genotype constellations PFGB rs1800790G>A and PFGA rs2070016T>C, which are associated with inflammation.20
For both genotypes, in absence of the prothrombotic constellation, CRPmean (≥10 mg/L) was strongly associated with mSASSS progression and in presence of the prothrombotic constellation, this association was considerably diminished (table 4) (PFGB rs1800790G>A: interaction term, OR: 0.13, 95% CI 0.02 to 0.98, p for homogeneity: 0.048; PFGA rs2070016T>C: interactions term, OR: 0.15, 95% CI 0.02 to 1.39, p for homogeneity: 0.094).
Analyses of parameters associated with radiographic spinal progression (worsening of mSASSS by ≥2 points after 2 years) in axial spondyloarthritis stratified by the prothrombotic genotype constellations PFGB rs1800790G>A and PFGA rs2070016T>C
Influence of genetic variants in FGB, FGA and FGG on relation between time-averaged CRP levels and radiographic spinal progression
For FGB rs1800788C>T (wild-type, OR: 5.91, 95% CI 1.52 to 23.0; T-allele carriers, OR: 1.83, 95% CI 0.47 to 7.15; p for homogeneity: 0.50), FGA rs6050A>G (wild-type, OR: 4.76, 95% CI 1.48 to 15.3; G-allele carriers, OR: 2.23, 95% CI 0.40 to 12.4; p for homogeneity: 0.16), FGA rs2070016T>C (wild type, OR: 4.10, 95% CI 1.43 to 11.8; C-allele carriers, OR: 1.22, 95% CI 0.15 to 9.72; p for homogeneity: 0.66), again, a tendency for heterogeneity between wild-types and minor allele carriers in respect of association of CRPmean (≥10 mg/L) and mSASSS worsening was found.
Relation of radiographic spinal progression and CRP level at baseline
From a clinical and research perspective, prognostic information yielded from baseline data on course of structural damage progression would be of interest.
In the total study population, CRPbaseline elevation (≥10 mg/L) tended to be associated with mSASSS progression (OR: 2.25, 95% CI 0.91 to 5.56). In FGB rs1800790GG wild types, this association was highly significant (OR: 5.71, 95% CI 1.69 to 19.3) and completely missing in FGB rs1800790 A-allele carriers (OR: 0.38, 95% CI 0.06 to 2.53) with relevant heterogeneity between both subgroups (interaction term, OR: 0.13, 95% CI 0.02 to 0.92, p for homogeneity: 0.041) (table 5). The same holds true, when stratifying for absence (OR: 4.98, 95% CI 1.57 to 15.7) and presence (OR: 0.26, 95% CI 0.03 to 2.34) of PFGB rs1800790G>A (interaction term, OR: 0.09, 95% CI 0.01 to 0.72, p for homogeneity: 0.024) (table 5).
Analyses of parameters (including baseline CRP levels) associated with radiographic spinal progression (worsening of mSASSS by ≥2 points after 2 years) in axial spondyloarthritis stratified by the FGB rs1800790G>A or PFGB rs1800790G>A
For A2AP Arg6Trp (wild type, OR: 0.63, 95% CI 0.14 to 2.86; minor allele carrier, OR: 4.51, 95% CI 1.24 to 16.5; interaction term, OR: 5.66, 95% CI 0.88 to 36.6, p for homogeneity: 0.069) and PFGA rs2070016T>C (nonprothrombotic, OR: 4.63, 95% CI 1.59 to 13.8; prothrombotic, OR: 0.14, 95% CI 0.005 to 3.85; interaction term, OR: 0.063, 95% CI 0.005 to 0.86, p for homogeneity: 0.038) considerable heterogeneity between both subgroups could be found, as well.
The relation between CRPbaseline and mSASSS change in genotype-defined subgroups is visualised in cumulative probability plots (figure 1).
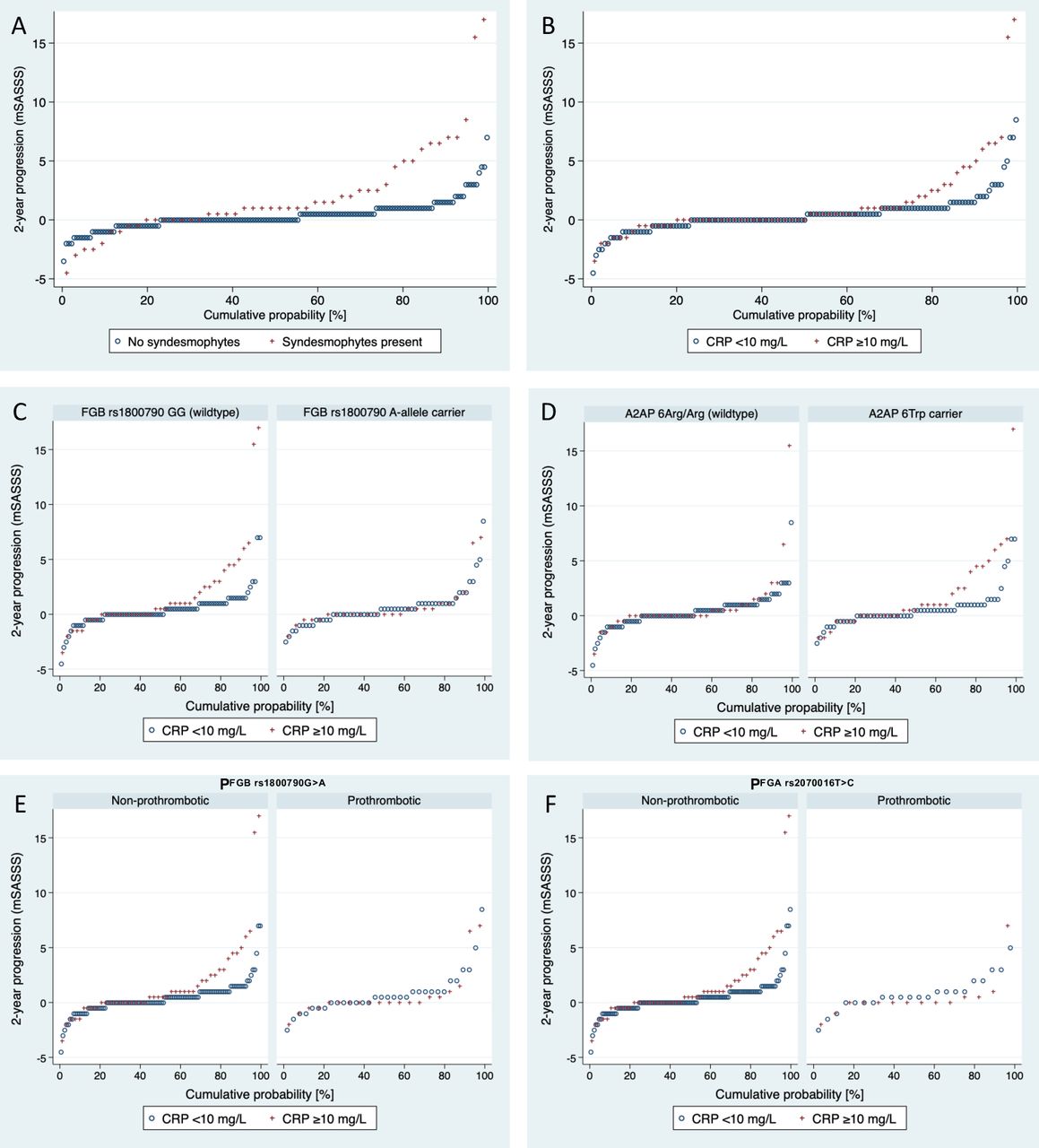
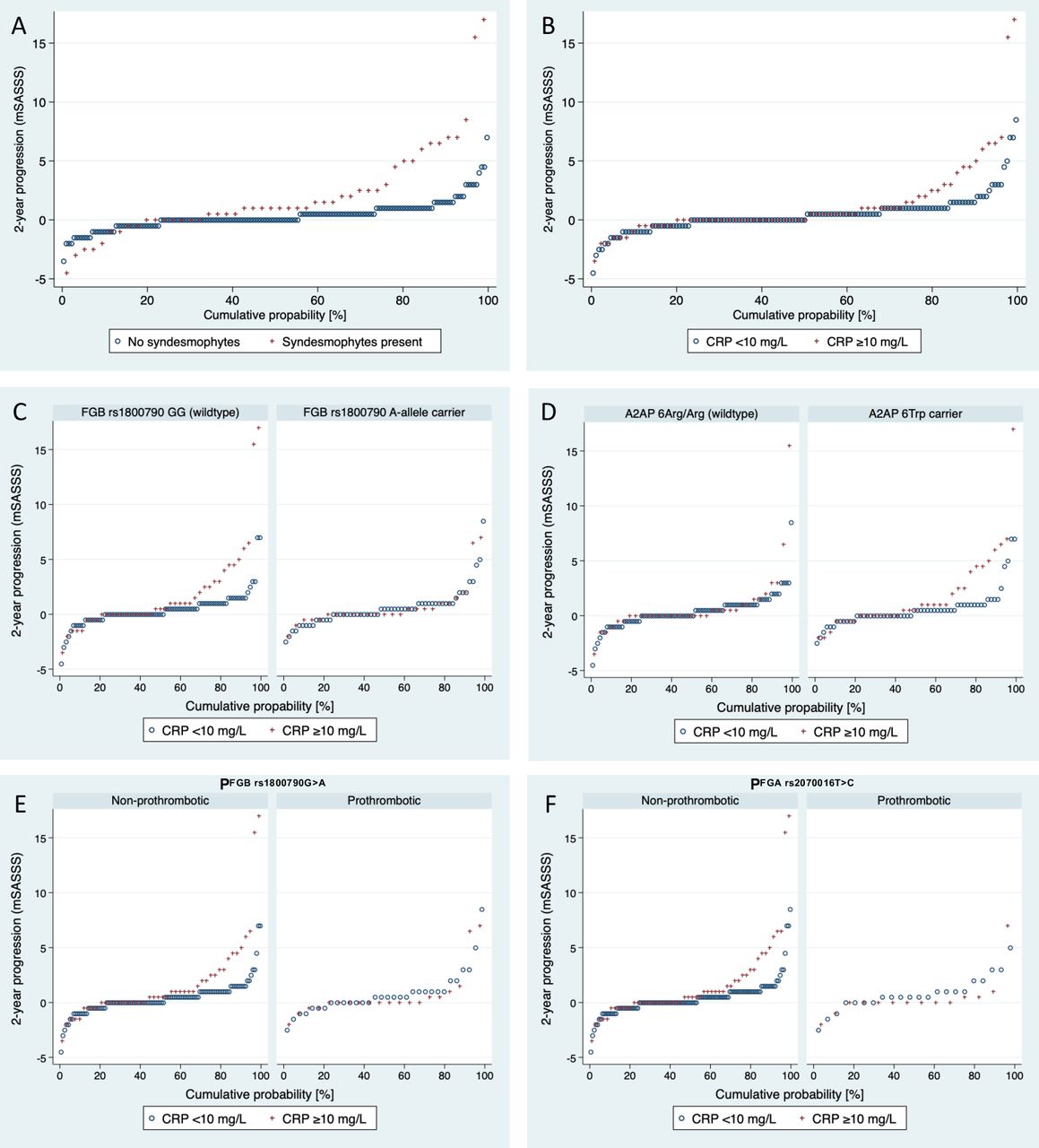{kind=link}
Cumulative probability plots of radiographic spinal progression after 2 years according to mSASSS in relation to the presence or absence of (A) syndesmophytes at baseline and (B) CRP elevations. Plots for CRP additionally are subgrouped for (C) FGB rs1800790G>A, (D) A2AP Arg6Trp, (E) PFGB rs1800790G>A and (F) PFGA rs2070016T>C. A2AP, α2-antiplasmin; CRP, C-reactive protein; FGB, β-fibrinogen; mSASSS, modified Stoke Ankylosing Spondylitis Spinal Score.
Results of analyses on a possible direct relation between the genotypes tested and radiographic spinal progression or CRP levels are given in online supplemental text and online supplemental table 3.
Supplemental material
Discussion
Pathology of axSpA is characterised by prolonged and/or increased inflammatory response at the interface between cartilage and bone, presumably triggered and/or perpetuated by mechanical stress and finally resulting in dysbalanced bone formation, that is the main pathologic process behind radiographic spinal progression.40 Until now, only CRP is used for risk stratification on top of already existing structural damage (syndesmophytes) in clinical practice.7 When conjointly considering syndesmophytes, current smoking and CRP elevations, presence of syndesmophytes is strongly associated with radiographic spinal progression, while CRP and current smoking moderately contribute to prognostic risk assessment (table 2).
Our study was triggered by two facts. (1) Fibrin(ogen) derivatives and proteins related to fibrin clot formation and fibrinolysis modulate inflammation and tissue repair15 16 and (2) genetic variants of gene loci, which influence fibrinogen synthesis,30 32 fibrin clot formation/structure17 or susceptibility to fibrinolysis17 34 35 41 42 and also influence the magnitude of inflammatory activity.20 22 24 Thus, we hypothesised that the genetic background of fibrinogen and related proteins could modify the predictive value of CRP in respect of radiographic spinal progression.
Data presented here are best comprehensible, when considering that genotype constellations predisposing for loose, fibrinolysis-susceptible fibrin clot structures are permissive for stronger CRP responses and that, vice versa, in genotype constellations resulting in tight, fibrinolysis-resistant so-called prothrombotic clot structures; CRP responses are comparatively diminished.20 22 24 Consequently, local inflammation in vertebral bodies in patients with the latter genetic background might not be associated with a strong systemic CRP response. A lack of predictive value of CRP for radiographic spinal progression in this patient subgroup is a sequel.
In our study population, genotypes predisposing for increased fibrinogen synthesis (FGB rs1800790 A-allele carriage) (table 2), strong fibrinolysis resistance (carriage of A2AP 6Arg/Arg wild-type) (table 3) or for prothrombotic clot structures (PFGB rs1800790G>A, PFGA rs2070016T>C) (table 4) abrogated completely association of CRP with radiographic spinal progression (mSASSS change) (figure 1). All these genotypes are known to diminish inflammatory activity.20 22 24 On the other hand, in individuals carrying genotypes related to lower fibrinogen synthesis (FGB rs1800790GG wild-types), higher susceptibility to fibrinolysis (A2AP 6Trp carriers, F13A 34Leu carriers) and/or less crosslinked, loose fibrin clot structures elevated CRP levels were strongly associated with radiographic spinal progression (tables 2–4 and figure 1). These genotype constellations are permissive for stronger CRP responses,20 22 and in those patients elevated CRP can be considered as good predictor of subsequent structural damage progression. Associations in these cases were considerably stronger compared with the association without considering the genetic background. Thus, our findings seem consistently to indicate that in axSpA, the predictive value of CRP elevation in respect of increased radiographic spinal progression may be limited to individuals, which are not genetically predisposed to form so-called prothrombotic fibrin clot structures under proinflammatory triggers.
We have analysed 10 genotypes and the sample size of GESPIC is rather low. For this reason, results of statistical testing should be interpreted carefully. However, the fact that results derived from genotypes from four chromosomal locations (FGB/FGA, chromosome 4; F13A, chromosome 6; F13B, chromosome 1 and A2AP, chromosome 17) were in agreement with the one tested hypothesis, in our view seems to support the assumption.
In our study population, even a single baseline CRP level (≥10 mg/L) was predictive for a meaningful radiographic progression, when the permissive genetic background was present. This finding could be relevant for prediction of progression and risk stratification in clinical practice and research.
In general, our results can be discussed in two ways. It could be assumed that only in individuals not genetically predisposed for prothrombotic fibrin clot structures, CRP-responses are sufficiently strong to reflect the magnitude of inflammation load in the axial skeleton. In other words, in patients predisposed for prothrombotic fibrin clots, CRP-responses could be diminished, hereby hampering the predictive value of CRP in respect of disease progress.
Otherwise, it could be hypothesised that loose fibrin gel structures with low anti-fibrinolytic potential are more permissive for cell migration into inflamed tissues, hereby modifying clinical course, allowing locally for stronger cytokine release and systemically for a more prominent CRP response. Hereby, genetics related to fibrin clot formation and fibrinolysis would be directly involved in processes of pathological inflammation and/or tissue repair in axSpA. This interpretation would help understand the missing association between these genotypes and CRP levels in patients with GESPIC (online supplemental table 3). FGB rs1800790G>A, PFGB rs1800790G>A and PFGA rs2070016T>C have been described to be strongly associated with CRP levels.20 22 Additionally, in patients with rheumatoid arthritis, both composite genotype constellations were related to clinical disease activity.20 If these genotype constellations in patients with axSpA would directly influence processes involved in pathogenesis, missing associations between genotypes and CRP could result from a direct influence of these genetic variants on clinical course in axSpA.
In respect of the inverse predictive behaviour of CRP and syndesmophytes/smoking in genotype-defined subgroups (tables 2–5), there are two possible explanations. Overall, CRP, smoking and syndesmophytes with some overlap are predictors for radiographic progression. In individuals with diminished CRP-response due to predisposition for tight fibrin gels, CRP does not adequately reflect inflammatory burden and consequently has reduced predictive value for progression. In these individuals, association strength between syndesmophytes/smoking with progression could increase due to the decreased predictive value of CRP. Another explanation could assume that individuals with a different genetic background behave biologically different.
The presented findings can be interpreted in a way that CRP cannot be considered without any limitation as a good predictive marker of radiographic spinal progression in the entirety of patients with axSpA or in a more conservative wording the findings could help to explain the clinical course in progressing patients without CRP elevations. The predictive potential of CRP in respect of radiographic spinal progression seems to be considerably increased, if a genetic background predisposing to loose, fibrinolysis-susceptible fibrin clots is given, and nearly absent otherwise. Further studies should address the question whether the same can also be true for CRP as predictor of treatment response in axSpA.
Data availability statement
Data are available upon reasonable request.
Ethics statements
Ethics approval
Study protocol was approved by the ethical committee of the coordinating centre (Charité–Universitätsmedizin Berlin, Germany) and by local ethical committees of participating centres (ethics approval number 188-19). All included patients provided written consent to participate.
Acknowledgments
We thank Prof. M. Leirisalo-Repo (Finland), Prof. D. van der Heijde (The Netherlands) and Prof. M. Dougados (France) for scientific advice on the design of the cohort. We are grateful to Beate Buss, Petra Tietz and Annegret Langdon for monitoring the cohort, Johanna Callhoff, Anja Weiss, Joachim Listing and Martina Niewerth for the data management support and statistical advice, Janis Vahldiek and Georg Heine for the X-ray images handling and for the development of the image scoring interface, Peggy Thiele for the genotyping, and to all patients who voluntarily participated in this cohort. Further, we would like to thank the following rheumatologists for inclusion of their patients: J. Brandt, H. Brandt, G.-R. Burmester, H. Deister, E. Edelmann, J. Emmerich, M. Enderlein, A. Gauliard, E. Gromnica-Ihle, F. Heldmann, S. Hermann, U. von Hinüber, Ü. Hübner, K. Karberg, H. Nüßlein, R. Pelle-Lohfink, D. Pick, G. Reichmuth, E. Riechers, M. Rihl, R. Schmidt, S. Schnarr, U. Schneider, I.-H. Song, I. Spiller, U. Syrbe, V. Walz, S. Wassenberg, H. M. Wisseler, S. Zinke.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Twitter @mprotopopov
Contributors BH and DP developed the hypotheses, and conceived and designed the study. DP, FP, H-GH, JS, MP, MR and VR collected clinical and radiographic data as well as biosample acquisition in the cohort. AE, BH and CS performed genotyping analyses. AE, BH, CS, DP and MV analysed the data and all other authors contributed to the data interpretation. BH and DP drafted the manuscript and all other authors critically revised the manuscript for important intellectual contents. All authors had full access to all data and approved the final version of the manuscript.
Funding This work was supported by the German Federal Ministry of Education and Research (Bundesministerium für Bildung und Forschung - BMBF) through ArthroMark (grants 01EC1009A and 01EC1401A). GESPIC was initially supported by the BMBF. As consequence of the funding reduction by BMBF according to schedule in 2005 and stopped in 2007, complementary financial support has been obtained also from Abbott, Amgen, Centocor, Schering–Plough, and Wyeth. Starting from 2010, the core GESPIC cohort was supported by AbbVie.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.