Article Text

Abstract
Objective To determine the presence of mental disorder risk and associated factors in European patients with axial spondyloarthritis (axSpA).
Methods Data from 2,166 patients with axSpA in 12 European countries were collected from 2017 to 2018 through the European Map of Axial Spondyloarthritis online survey. Risk of mental disorders was assessed using the 12-item General Health Questionnaire. Possible predictors included age, gender, relationship status, patient organisation membership, job status, educational level, Bath Ankylosing Spondylitis Disease Activity Index (BASDAI), functional limitation (0–54) and self-reported depression or anxiety. Bivariate analyses were conducted to determine predictors of risk of mental disorders (Mann-Whitney and χ2) and multivariable analysis identified factors associated with risk of mental disorders.
Results 60.7% of patients reported risk of mental disorders: they were younger (41.7 vs 46.0 years), more likely female (68.2% vs 57.9%), unemployed (7.5% vs 2.7%), on temporary (15.9% vs 5.4%) or permanent sick leave (13.2% vs 8.0%), reported depression (45.2% vs 14.2%) or anxiety (41.3% vs 12.5%), higher disease activity (BASDAI ≥4; 87.6% vs 62.3%) and functional limitation (16.5 vs 10.8). The factors most associated with risk of mental disorders were disease activity (OR=2.80), reported depression (OR=2.42), anxiety (OR=2.39), being unemployed or on sick leave (OR=1.98), functional limitation (OR=1.02) and younger age (OR=0.97).
Conclusions Compared with the general population, patients with axSpA show disproportionately worse mental health associated mainly with disease activity and employment status. Healthcare professionals should pay close attention to patients with high disease activity and address internally or refer to specialist services, where appropriate to ensure optimal patient outcomes.
- spondylitis
- ankylosing
- patient reported outcome measures
- psychology
Data availability statement
The authors confirm that the data supporting the findings of this study are available within the article.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Key messages
What is already known about this subject?
Poor mental health in patients with axial spondyloarthritis (axSpA) is associated with disease outcomes and worsening functioning.
What does this study add?
The present study assesses mental health in a large sample of 2166 patients with axSpA in 12 European countries through the diagnosis of anxiety and depression and by means of the validated scale: the 12-item General Health Questionnaire.
60.7% of patients with axSpA in Europe had the risk of mental disorder, and the factors most associated were disease activity, being unemployed or on sick leave, greater functional limitation in daily activities and younger age.
30.0% reported previous experience of anxiety and 33.1% depression, these figures being six times greater among patients with axSpA in comparison with 5.4% and 4.5%, respectively in the general population in Europe.
How might this impact on clinical practice or future developments?
The results suggest the need to improve the mental well-being of patients with axSpA by monitoring their disease activity as well as early referral to mental health specialists.
Introduction
Axial spondyloarthritis (axSpA) is a long-term condition characterised by loss of mobility, chronic pain and fatigue, reduced quality of life1 and both physical and mental health.2
Although the association between axSpA and high levels of distress (anxiety and depression) has been investigated,3 few larger-scale studies have confirmed this link. Methodological differences across studies in measuring common mental disorders yield varying approximations, with the presence of depression ranging between 11% and 64%,3 and anxiety between 15.6% and 60.9%.4 5 This is further complicated as regular assessment of mental disorders within clinical practice is yet to be applied systematically in axSpA care.
It is well established that depression and anxiety are associated with increased disease activity in axSpA, chronic pain reporting and worsen functioning leading to poor health outcomes and quality of life.6 7 Previous studies have found that the factor most associated with the psychological health status of patients with axSpA was disease activity, although these findings need to be confirmed in a real-world sample.8 9
The European Map of Axial Spondyloarthritis (EMAS) aimed to capture factors influencing patients’ perspective of the burden of axSpA, in different European countries using validated measures.2 Unlike other studies, which tend to rely heavily on clinical records and patients presenting to rheumatologists, the EMAS survey allowed for the collection of real-world data focused on parameters deemed relevant by patients with axSpA. Furthermore, it took a comprehensive view in assessing mental health, including both self-reported diagnosed comorbidities as well as scores from the 12-item General Health Questionnaire (GHQ-12) - termed mental disorder here.
Using the EMAS data, the aim of this analysis was to determine the presence of risk of mental disorders in European patients with axSpA and to examine associated factors.
Materials and methods
Study design
EMAS was a cross-sectional online survey of patients with a self-reported diagnosis of axSpA encompassing 13 European countries: Austria, Belgium, France, Germany, Italy, the Netherlands, Norway, Russia, Slovenia, Spain, Sweden, Switzerland and the UK. The survey was adapted from the Spanish Atlas of Axial Spondyloarthritis 2017,10 the results of which were added retrospectively to the EMAS database. The methodology of the EMAS study is described in detail elsewhere.2 For the purpose of this analysis on mental health, data from Spain were excluded as they have been previously published,9 therefore our final sample size presented here is 2,166.
All patients who agreed to their participation through informed consent, were asked to provide explicit opt-in consent prior to participating in the EMAS survey. The participant data collected in the survey does not allow the identification of individual participants. In this study, no clinical trial was conducted. As it was not an interventional study, no ethics committee approval was required.
Working group
The EMAS project is a collaboration led by the Health & Territory Research group of the University of Seville, Axial Spondyloarthritis International Federation, Novartis Pharma AG and a steering committee composed of patient research partners and internationally recognised rheumatologists, psychologists and researchers specialised in axSpA.
Patients
Participants were recruited between July 2017 and March 2018 by Ipsos SA (formerly GfK), a market research agency, through their existing database of respondents. Patient advocacy groups supported recruitment by distributing the survey to their members in the following countries: Austria, Italy, the Netherlands, Norway, Russia, Slovenia and Sweden (figure 1).

EMAS sample selection flow chart. BASDAI, Bath Ankylosing Spondylitis Disease Activity Index; EMAS, European Map of Ankylosing Spondyloarthritis; GfK, market research agency currently known as Ipsos SA; PAG, patient advocacy group; mental disorder risk (defined as 12-Item General Health Questionnaire score ≥3).
The inclusion criteria were age ≥18 years, resident in one of the participating countries, a self-reported clinician-provided diagnosis of axSpA, including ankylosing spondylitis or non-radiographic axSpA and visit to a healthcare professional for axSpA in the 12 months prior to participation.
Measurement
The survey consisted of 108 items related to 12 different areas: sociodemographic and anthropometric characteristics, disability assessment, working life, daily life, lifestyle habits, diagnostic journey, healthcare utilisation, treatment, comorbidities (including extra-articular manifestations), mental health, axSpA-specific outcomes and patient disease-related attitudes and treatment goals. All variables collected for the EMAS survey were patient-reported.
Patient-reported outcome measures
We were mindful of the need to capture physical, psychological and social impact, while avoiding measurement fatigue and the risk of increasing social response bias. Therefore, we used both validated, commonly used measures and one developed with patients for the purpose of this survey. EMAS employed2 the Bath Ankylosing Spondylitis Disease Activity Index (BASDAI) to assess disease activity. Furthermore, to assess functional limitation, a non-validated tool referred to as the Functional Limitation Index, was specifically developed, with patients, for this study. The Functional Limitation Index assessed the degree of functional limitation in 18 activities of daily life (ie, dressing, bathing, showering, tying shoe laces, moving about the house, climbing stairs, getting out of bed, using the bathroom, shopping, preparing meals, eating, household tasks, walking down the street, using public transportation, driving, going to the doctor, doing physical exercise and intimate relations), some of which is not captured by validated tools. The Functional Limitation Index was generated by adding the non-weighted degree of functional limitation of all activities using a Likert scale of 0–3 (where 0=none, 1=low, 2=medium and 3=high limitation). Total scores indicated low (0–17), medium (18–35) or high (36–54) degree of limitation in daily life. Cronbach alpha of 0.97 demonstrated excellent internal reliability.2 11
Mental health
Mental disorder risk: assessed using the GHQ-12. It is a measure of psychological distress comprising symptoms of anxiety, social dysfunction and loss of confidence.12 It is not a psychiatric diagnostic instrument but is a validated screening tool for identifying common mental problems in the general population.13 Part of the value of the GHQ-12 is that it has been widely used across many long-term conditions, it has not yet been validated specifically in rheumatological conditions. The GHQ-12 scale consist of 12 items (1: Able to concentrate; 2: Loss of sleep over worry; 3: Playing a useful part; 4: Capable of making decisions; 5: Felt constantly under train; 6: Couldn’t overcome difficulties; 7: Able to enjoy day-to-day activities; 8: Able to face problems; 9: Feeling unhappy and depressed; 10: Losing confidence; 11: Thinking of self as worthless; 12: Feeling reasonably happy) to assess mental health problems during the previous 4 weeks using a 4-point Likert scale (less than usual, no more than usual, rather more than usual or much more than usual). Total GHQ-12 scores range between 0 and 36, with higher scores reflecting an increased the risk of mental disorders. To determine mental disorder risk among patients with axSpA, the Likert scale was transformed to 0, 0, 1, 1, and the threshold for mental disorder risk set at ≥3 as supported by literature.9
The GHQ-12 is a screening measure for identifying minor psychiatric disorders in the general population, used to encompass common symptoms of anxiety social dysfunction and loss of confidence.12 It is not a diagnostic instrument.
Mental health comorbidity: patients were asked to self-report if they had been previously diagnosed with anxiety or depression.
Statistical analysis
Bivariate analyses were conducted to determine possible relationships between the study variables and mental health (GHQ-12 cut-off). For quantitative variables (age, BASDAI and Functional Limitation Index), the Mann-Whitney test was used to evaluate differences in the distribution of variables between GHQ-12 cut-off points (<3 and ≥3). For categorical variables (gender, relationship status, educational level, job status, patient organisation membership, BASDAI cut-off, depression diagnosis and anxiety diagnosis), a χ2 test was used to compare the distribution of variables between GHQ-12 cut-off points.
Variables that showed statistical significance (p<0.05) in the bivariate analysis were introduced in the binary logistic multivariable regression model: age (years), sex (female), job status (unemployed or sick leave), anxiety diagnosis (yes), depression diagnosis (yes), BASDAI cut-off (≥4) and Functional Limitation Index (0–54). Each variable was introduced individually into the model to determine which was associated with mental disorder risk.
Data were analysed using IBM SPSS software, V.25 and differences were considered statistically significant at the 5% level.
Results
A total of 2,166 participants were included in this analysis, of whom 1314 (60.7%) were classified as at risk of mental disorders based on their GHQ-12 score, the mean of which was 4.8±4.0. See table 1 for a summary of the sample characteristics.
Socio-Demographic data, disease outcomes, treatment, and mental health sample characteristics
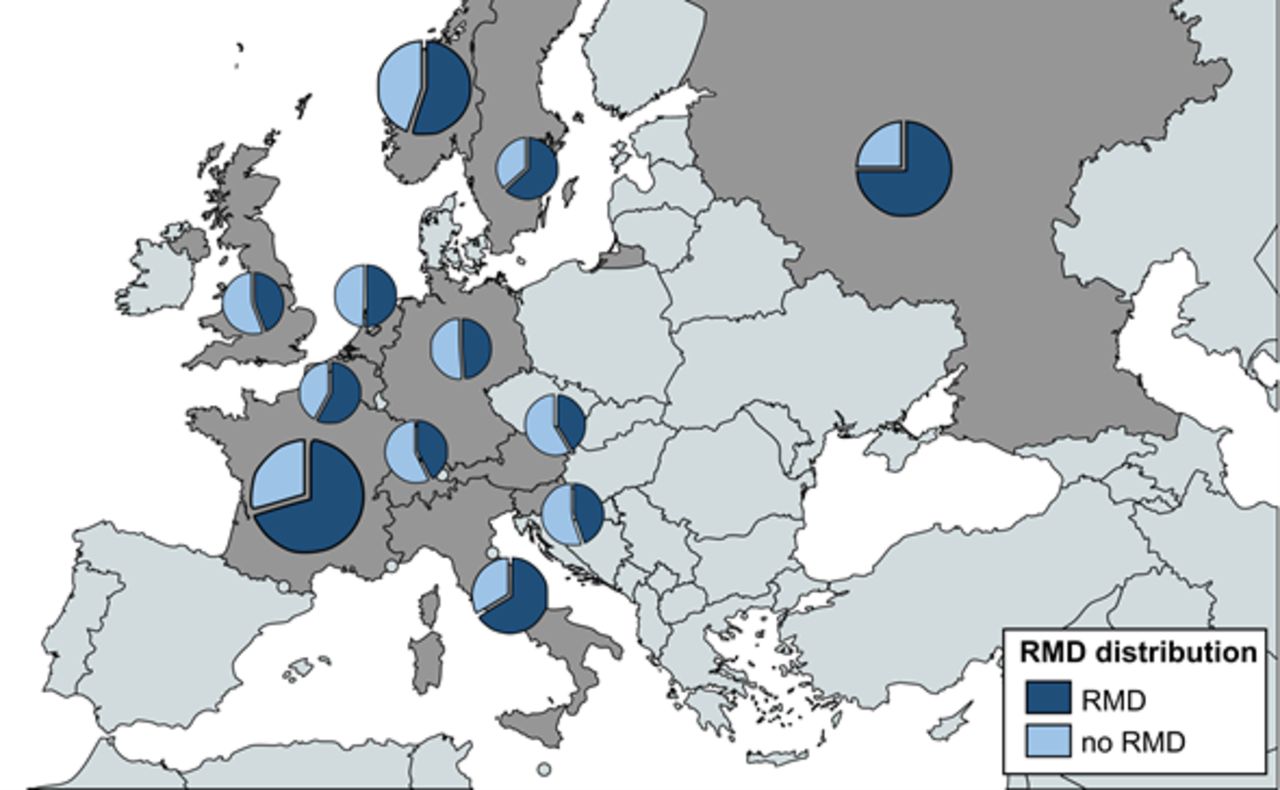
Mental disorder risk was unevenly distributed among countries, with Russia having the worst mental health (75.1%) followed by France (70.5%). Austria (41.5%) and Switzerland (42.5%) reported among the lowest (figure 2). Across Europe, 30.0% of participants reported previous experience of depression while 33.1% reported previous anxiety.

{kind=link}
{kind=link}
European sample distribution of patients for each EMAS country stratified by the presence of mental disorder risk. Based on 2166 respondents. sector diagrams show the proportion of patients with axial spondyloarthritis at worse mental health in the participating countries. Sector diagram size represents relative sample size of each EMAS participating country. EMAS, European Map of Ankylosing Spondyloarthritis; RMD, risk of mental disorders (defined as the 12-Item General Health Questionnaire Score ≥3).
The bivariate analyses showed that mental disorder risk (GHQ-12 ≥3) was significantly associated with the following variables: younger age, female sex, unemployment, temporary sick leave, permanent sick leave, previous anxiety diagnosis, previous depression diagnosis, higher level of disease activity (accounted by both the overall BASDAI score and a greater proportion of participants scoring >4 on the BASDAI scale), and worse functional limitation (p<0.001 for all comparisons). See table 2 for further details.
Bivariate analysis of factors associated with mental disorder risk by GHQ-12 cut-off
In the binary multivariable logistic regression, worse mental health was associated with younger age, female sex, being on unemployment or sick leave, a comorbid diagnosis of anxiety or depression, increased disease activity and worse functional limitation. Furthermore, the factors significantly associated with risk of mental disorders were: disease activity (OR=2.80; 95% CI=2.17 to 3.61), being diagnosed with anxiety (OR=2.39; 95% CI=1.78 to 3.19) or depression (OR=2.42; 95% CI=1.79 to 3.28), being unemployed or on sick leave (OR=1.98; 95% CI=1.53 to 2.56), higher functional limitation in daily activities (OR=1.02; 95% CI=1.01 to 1.03) and younger age (OR=0.97; 95% CI=0.97 to 0.98) (table 3).
Binary logistic regression to predict factors associated with the risk of mental disorders
Discussion
The results of the present study of patients with axSpA in Europe show mental disorder risk in 60.7%, according to the GHQ-12 scale. In the multivariable analyses, the factors significantly associated with the risk of mental disorders are: disease activity, being diagnosed with anxiety or depression, being unemployed or on sick leave, greater functional limitation in daily activities and being younger.
Furthermore, almost one-third reported previous experience of anxiety (30.0%) or depression (33.1%). These figures are six times greater among patients with axSpA in comparison with the general population in Europe, where the presence of anxiety and depression disorders was estimated at 5.4% and 4.5%, respectively.14
The high proportion of those experiencing mental disorder symptoms confirms a relationship between axSpA and poorer mental health. However, in clinical practice, there remains a gap in the systematic assessment of mental health which may be leading to an underdiagnosis and undertreatment of common mental disorders among patients with axSpA . We argue this compromises the quality of patient care and affects health outcomes.
Higher disease activity is likely to leave patients with axSpA feeling anxious and distressed about their uncontrolled pain, fatigue and joint stiffness. The relationship between disease activity and poor mental health is bidirectional, with worsening mental health also influencing disease activity.15–18 This can make patient management in clinical practice a challenge. However, clinicians well-trained in communication skills can adopt a more patient-centred approach to ask key questions that elicit the extent of the impact. For example, questions phrased as ‘which is the most problematic to you, the physical symptoms or the impact the condition has on your life’ with a follow-up of ‘which aspect is most problematic at the moment’ and ‘if you could change one aspect, what would you change?’ can guide the clinicians focus for treatment.19
Our analysis showed that mental disorder risk is associated with a previous diagnosis of anxiety or depression as well as being unemployed or on sick leave, in both the bivariate and multivariable regression. The link with previous diagnosis of anxiety and depression served to validate the appropriateness of using the GHQ-12 scale. The data illustrated that patients with axSpA with high levels of distress were more likely to be unemployed or require sick leave and similarly, patients with axSpA who are either unemployed or on sick leave were more likely to develop mental disorders.
We confirmed the previously documented association between disease activity and unemployment/sick leave among patients with axSpA,20 but on larger scale. We now believe it is critical to optimise axSpA care by adopting a holistic approach to patient management to address these wider consequences.
Of course, the primary role of the rheumatologist is to control disease activity as it influences all aspects of the patient’s life. However, it is also important to systematically assess mental health in rheumatology practice and facilitate early referral to mental health specialists when needed. This could be supported through enhanced clinician education and introduction of simple screening tools, such as the GHQ-12, which has been used extensively in non-psychiatric clinical settings.13
EMAS was the largest survey carried out to date for patients with axSpA, capturing differences in the experience of patients with axSpA across the European continent. Results of the present study confirmed the findings of the previous similar study carried out in Spain.9 Compared with the Spanish study, our study shows even higher rates of common mental disorders than the Spanish sample (33.1% vs 28.2% in the case of anxiety and 30.0% vs 20.8% in the case of depression). Additionally, mental disorder risk (GHQ-12 scores≥ 3) was present in 45.6% of patients in Spain and 60.7% in Europe.9 The difference in the prevalence of mental disorder risk presented by the different EMAS countries may be due to socioeconomic characteristics and healthcare resources available in each of these countries. However, the inclusion of all these countries helps us to gain a better geographical coverage of mental health in the different European countries.
As the survey questions were cocreated with patients, we are confident the data truly reflects the experience of patient with axSpA. However, EMAS is not without criticism, the information came from self-reported data, with no clinician confirmed assessments with the limitations that imply. Second, we appreciate the problem of using non-validated scales or indices for assessing functional limitations in daily life and stiffness. We took the decision to use the measures in this study because in the early phase of this work patients expressed their frustration at the limitations of other scales or indices that did not capture the full extent of the impact that living with axSpA had on their lives. Cronbach’s alpha coefficient obtained for the measures used in our study indicated the acceptability of these instruments. Finally, the possibility of selection bias cannot be ruled out for those countries that included a smaller sample size. In addition, the non-validated Functional Limitation Index was used to assess functional limitation in 18 activities of daily life, assessing the degree of functional limitation of all activities using a Likert scale of 0–3, obtaining a scale from 0 to 54, being 0–17 low, 18–35 medium and 36–54 high degree of limitation in daily life. The use of Functional Limitation Index was done out of necessity as the Assessment of SpondyloArthritis International Society Health Index (ASAS-HI) scale was not available at the time of our study. The ASAS-HI measures functioning and health across 17 aspects regarding functional limitation in daily activities with two possible answers for each: agree or disagree of health, resulting in a score ranging from 0 to 17, in which a lower score indicates a better functioning and health status. However, the Cronbach alpha coefficient supports the reliability of the Functional Limitation Index.2 11 The large numbers in our survey has given us confidence that the findings are representative of the subpopulations in those geographical areas. Given the nature of the survey, which was not targeted at specific individuals, we have no way of knowing how many people saw the notice and chose not to respond. Furthermore, the possibility of selection bias cannot be ruled out for those EMAS countries that included a smaller sample size and for those characterised by a dominant form of patient recruitment. However, as this was a cross-sectional study, we cannot establish causality between the results obtained and the results should be interpreted with caution. Finally, the use of the GHQ-12 in patients with underlying physical conditions is not without criticism. We chose this measure because it allows us comparison with a similar population in previously published work and, although being more conservative, we adopted a higher cut-off score indicating distress and we recognise the limitation of the measure and recommend disease-specific validation is performed in future research.
Conclusion
This study shows European patients with axSpA exhibit a disproportionately high levels of common mental disorders, compared with the general population. Worst mental health appears to increase with disease activity and is linked to employment status and the ability to perform daily and work-related tasks. Together, these findings highlight the need to optimise disease management of the whole person, ensuring disease activity is well-controlled but also addressing high levels of distress in those who require it. Systematic clinical assessments of mental health, clinician education on recognising and monitoring the mental health aspects of axSpA and prompt referral to mental health specialists are critical strategies to ensure optimal health of patients with axSpA.
Data availability statement
The authors confirm that the data supporting the findings of this study are available within the article.
Ethics statements
Patient consent for publication
Acknowledgments
The authors acknowledge the EMAS working group. The EMAS project is a collaboration led by the Health & Territory Research group of the University of Seville, the Ankylosing Spondylitis International Federation, and a steering committee composed of patient representatives and internationally recognised rheumatologists, psychologists, and researchers specialised in axSpA. The authors would like to thank all patients who participated in the study.
References
Footnotes
Twitter @MarcoGarridoCum
Collaborators We thank the researcher José Correa-Fernández for reviewing the manuscript.
Contributors All authors have contributed equally. MG-C is responsible for the overall content and acts as guarantor for this manuscript.
Funding This study was supported by Novartis Pharma AG.
Map disclaimer The inclusion of any map (including the depiction of any boundaries therein), or of any geographic or locational reference, does not imply the expression of any opinion whatsoever on the part of BMJ concerning the legal status of any country, territory, jurisdiction or area or of its authorities. Any such expression remains solely that of the relevant source and is not endorsed by BMJ. Maps are provided without any warranty of any kind, either express or implied.
Competing interests EMAS was funded by Novartis Pharma AG. All authors have received honoraria from Novartis Pharma AG for participating in EMAS. DP has received unrelated research grants from AbbVie, Merck Sharp & Dohme (MSD), Novartis and Pfizer, and unrelated honoraria from AbbVie, Bristol Myers Squibb (BMS), Celgene, Janssen, Lilly, MSD, Novartis, Pfizer, Roche and UCB. VN-C has received unrelated honoraria or research grants from AbbVie, BMS, Janssen, Lilly, MSD, Novartis, Pfizer, Roche and UCB. LC is employee of Novartis Pharma AG. SM has received unrelated honoraria from GlaxoSmithKline and Bayer. CB has received unrelated honoraria from AbbVie, Amgen, Janssen, Lilly, Novartis and Pfizer.
Provenance and peer review Not commissioned; externally peer reviewed.