Article Text

Abstract
Objectives We engaged patients with systemic sclerosis (SSc) and healthcare professionals to assess electronic health (eHealth) literacy and needs relating to web-based support using internet-based information and communication technologies (ICT).
Methods We employed an explanatory sequential mixed methods design. First, we conducted a cross-sectional survey in patients (n=101) and professionals (n=47). Next, we conducted three focus groups with patients, family members and professionals (n=17).
Results Of patients, 89.1% used ICT at least weekly for private communication. Patients reported relatively high comprehension of eHealth information ( =6.7, 95% CI: 6.2 to 7.3, range 1–10), yet were less confident evaluating information reliability (
=6.7, 95% CI: 6.2 to 7.3, range 1–10), yet were less confident evaluating information reliability ( =5.8, 95% CI: 5.1 to 6.4) and finding eHealth apps (
=5.8, 95% CI: 5.1 to 6.4) and finding eHealth apps ( =4.8, 95% CI: 4.2 to 5.4). Patients and professionals reported little experience with web-based self-management support. Focus groups revealed ‘considering non-ICT-accessible groups’ and ‘fitting patients’ and professionals’ technology’ as crucial for acceptability. In relation to understanding/appraising eHealth, participants highlighted that general SSc information is not tailored to individual’s disease course. Recommendations included ‘providing timely, understandable and safe information’ and ‘empowering end-users in ICT and health decision-making skills’. Professionals expressed concerns about lacking resources. Patients were concerned about data security and person-centredness. Key eHealth drivers included ‘addressing end-user perceptions’ and ‘putting people at the centre of technology’.
=4.8, 95% CI: 4.2 to 5.4). Patients and professionals reported little experience with web-based self-management support. Focus groups revealed ‘considering non-ICT-accessible groups’ and ‘fitting patients’ and professionals’ technology’ as crucial for acceptability. In relation to understanding/appraising eHealth, participants highlighted that general SSc information is not tailored to individual’s disease course. Recommendations included ‘providing timely, understandable and safe information’ and ‘empowering end-users in ICT and health decision-making skills’. Professionals expressed concerns about lacking resources. Patients were concerned about data security and person-centredness. Key eHealth drivers included ‘addressing end-user perceptions’ and ‘putting people at the centre of technology’.
Conclusions Patients and professionals need education/training to support uptake of eHealth resources. Key elements include guiding patients to timely/reliable information and using eHealth to optimise patient–provider communication. Design that is responsive to end-users’ needs and considers individuals with limited eHealth literacy and/or ICT access appears to be critical for acceptability.
- systemic sclerosis
- health services research
- outcome and process assessment
- health care
- nursing
Data availability statement
Data are available upon reasonable request. All data relevant to the study are included in the article or uploaded as supplementary information. The datasets generated and/or analysed during this study are included in this published article or can be made available from the corresponding author on reasonable request. The datasets generated and/or analysed during this study are included in this published article or can be made available from the corresponding author on reasonable request.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Key messages
What is already known about this subject?
Internet-based information and communication technologies have become increasingly important for chronic disease management and hold promise for rare disease patients who are geographically dispersed.
In systemic sclerosis, little is known about electronic health (eHealth) literacy or how patients and providers use eHealth to inform clinical practice and make health decisions.
What does this study add?
Quantitative findings reveal patients have difficulty appraising the quality of eHealth information and both patients and professionals rarely use online information for health and care decisions.
Qualitative findings indicate patients and professionals lack experience with eHealth support (eg, apps, online forums, self-help groups) and desire support/guidance in appraising eHealth resources.
How might this impact on clinical practice or future developments?
Involving stakeholders early in the eHealth development process is important for user-centred design, supporting equity and producing high-quality eHealth resources that are responsive to patient/provider needs and complementary to face-to-face care/support.
Background
Internet-based information and communication technologies (ICT) have become increasingly recognised in healthcare as a means to improve health—termed eHealth.1 In the light of this trend, the Chronic Care Model (a reference model for chronic care improvement) was amended in 2015 to include ICT approaches.2 Broadly, the updated model aims to improve health outcomes through empowering patients and healthcare professionals by introducing web-based solutions to support self-management, delivery system design, clinical decision support, clinical information systems and eHealth education. Notably, eHealth literacy is a fundamental prerequisite for empowerment within such care models.
eHealth literacy is defined as people’s knowledge, motivation and competence to ‘access’, ‘understand’, ‘appraise’ and ‘apply’ health information from electronic sources to address or solve a health problem3 4: ‘Access’ refers to the ability to seek, find and obtain health information, ‘understand’ refers to the ability to comprehend information, ‘appraise’ refers to interpret and evaluate information and ‘apply’ describes the ability to use health information to make informed decisions. Greater eHealth literacy is associated with better access to healthcare, more proactive health/self-management behaviours and improved health-related outcomes.5 Similarly, provider eHealth education and attitudes toward ICT use have considerable impact on eHealth implementation.6 Therefore, it is crucial to assess eHealth literacy of patients and professionals eHealth literacy and their respective needs to ensure uptake and sustainability of eHealth services.
Prior research on rare multisystemic, autoimmune connective tissue disease such as systemic sclerosis (SSc) and systemic lupus erythematosus (SLE) has primarily focused on patient general health literacy and barriers to ICT use.7 8 There is a paucity of evidence on eHealth literacy among rheumatologic providers. In regard to SSc/SLE eHealth support, web-based resources are often of low quality, have inadequate readability and limited functionality.9–11 Several studies demonstrate that patients with rare connective tissue diseases and their providers are interested in web-based education and support.12–14 However, few online programmes focus on critical concepts of health equity, patient engagement and empowerment. The Lupus Interactive Navigator is a web-based self-management programme for SLE with high patient ratings of content, usability and acceptability.15 In SSc, several studies have shown that appropriate eHealth interventions can support high-quality care through reliable disease information, self-management support and disease monitoring.16–19 Despite such promising results, little is known about patient with SSc and health professional eHealth literacy or how eHealth is applied to inform clinical practice and daily life decisions. In particular, patients affected by rare diseases, such as SSc, often have limited access to health information and care. Thus, it is important to explore how web-based technologies can best facilitate access to high-quality, coordinated SSc care. Similarly, understanding stakeholder eHealth literacy, needs and perspectives is important for developing targeted, user-centred interventions that are accepted.20
The MANagement Of Systemic Sclerosis (MANOSS) project aims to fill existing gaps in SSc care by developing an eHealth-enhanced rare disease chronic care model for patients with SSc in Switzerland.21 Part of the MANOSS project involves conducting a contextual analysis with stakeholder involvement to inform user-centred design.
This explanatory mixed methods study aimed to describe eHealth literacy of patients and healthcare professionals as well as perspectives and needs for web-based chronic care support. The quantitative phase assessed how patients with SSc and professionals access, understand, appraise and apply web-based health information and technologies for aspects of chronic care. The quantitative results informed the subsequent qualitative phase that aimed to deepen our understanding of how eHealth literacy, perspectives and needs explain eHealth use and can be incorporated into user-centred eHealth solutions within a new model of care.
Methods
Study design
We employed an explanatory sequential mixed methods design22 involving multiple centres providing SSc care (figure 1). The first phase utilised quantitative data from a cross-sectional survey of Swiss patients with SSc and healthcare professionals. Analyses informed the qualitative inquiry consisting of three focus groups with Swiss/international patients and professionals. The qualitative findings were used to explain quantitative findings.
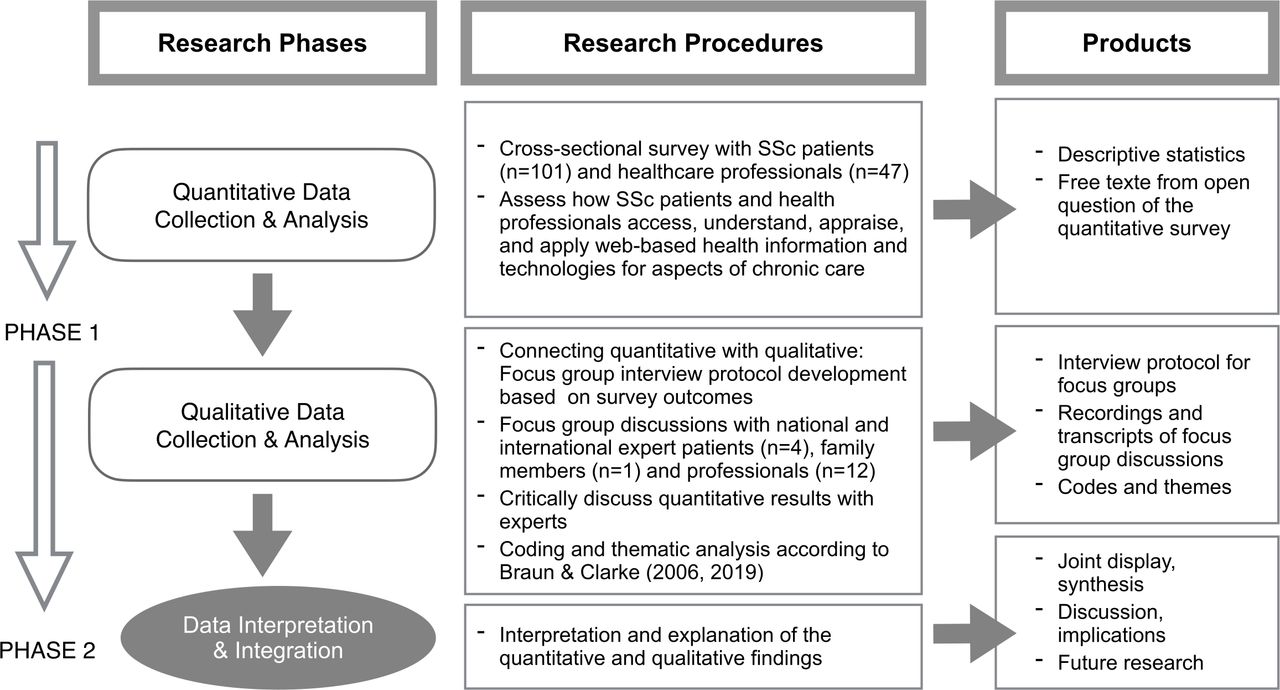
Study diagram for the explanatory, sequential mixed methods design. eHealth, usage of ICT for health; ICT, information and communication technologies; SSc, systemic sclerosis.
Patient and public involvement
Involvement of patient research partners and relevant stakeholders is strongly recommended for developing web-based technologies.23 24 Key stakeholders in this study were the Swiss League against Rheumatism, a patient research partner and the Swiss Scleroderma Association. Additionally, the European Alliance of Associations for Rheumatology (EULAR) study group, dedicated to improving and standardising non-pharmacological management of connective tissue diseases (CTDs), supported recruitment of participants for the qualitative inquiry.
Quantitative data collection
Sample and setting
We targeted a convenience sample of 100 adult patients (>18 years) spanning a range of SSc disease severity/experiences and 50 healthcare professionals with varied levels of experience in treating SSc. We recruited German-speaking and French-speaking participants (patients and professionals) from all Swiss University hospitals (Basel, Bern, Geneva, Lausanne, Zurich), one regional (state) hospital (Lucerne), rheumatology outpatient clinics, and the Swiss scleroderma patients’ association (www.sclerodermie.ch) according to the MANOSS study protocol.21
Variables and measurement
Validated patient-reported outcome measures for rare diseases such as SSc are scarce. Moreover, given the rate of technologic advances, available eHealth literacy measures do not adequately cover current technological developments.25–27 Hence, we constructed a set of pragmatic items tailored to SSc, including dimensions of instruments developed by Halwas et al28 and Vanhoof et al.29 Item selection was guided by the dimensions of eHealth literacy including ‘access’, ‘understand and appraise’ and ‘apply’ ICT/eHealth services (table 1). Participants were invited to provide open-ended, free text comments at the end of the questionnaire. Participants were given the option to complete the questionnaire online or in paper-pencil format (professionals online only).
Quantitative variables and measurements
Quantitative data analysis
We performed descriptive statistics (frequencies/percentages or means/medians with 95% CI and IQRs) to summarise quantitative survey data and sociodemographic characteristics (R, V.4.0.4). To compare groups (ie, sex, age groups, education, patient–professionals), we computed standardised mean differences (SMD) which are identical to Cohen’s d, using the tableone package for R. Compared with p values, SMD is more appropriate for calculating effect size estimates in small, uneven datasets—such as the ones analysed in this study.30 A SMD ≥0.2, ≥0.5 and ≥0.8 depict small, medium and large differences between groups, respectively. We calculated 95% CIs for means to facilitate visual comparison between ratings. Differences between groups were defined as means with distinct, non-overlapping CIs.
Qualitative data collection
Sample and setting
We used a purposeful sampling strategy to recruit 12–18 participants with expertise in SSc care/management. We defined participants with expertise as individuals with several years of experience with (1) SSc as a patient or (2) family member and/or (3) professional experience in chronic care, implementation science and/or health policy. Purposeful sampling focused on individuals with varied expertise in national or international care settings, across disciplines (eg, physicians, nurses, physiotherapists, occupational therapists and patient experts). Swiss professionals were recruited from Swiss University Hospitals (Bern, Lausanne, Zurich) and the Swiss League against Rheumatism (Rheumaliga Schweiz). International participants were recruited via the EULAR non-pharmacological management of CTDs study group.
Focus group discussions
The quantitative study results informed questions for focus group discussions. Due to the COVID-19 pandemic, focus groups were conducted using an online video conferencing system. With participant consent, focus group discussions were recorded. Briefly, findings of our systematic literature review and the quantitative study findings were provided to orient participants. Findings were discussed using open-ended prompts to elaborate quantitative results (ie, What is important/surprising? What fits your experiences? What is contradicting to your clinical experiences? What are important aspects that should be taken into account when improving chronic care for SSc patients?). Subsequently, primary care needs and problem areas for care were discussed for national (focus groups 1 and 2) and international contexts (focus group 3).
Qualitative data analysis
Focus group transcriptions and free text comments from the quantitative survey were analysed using reflexive thematic analysis.31 32 In brief, analysis was a recursive process that started with familiarisation with the data and coding of the text. Subsequently, codes were collated to build initial inductive themes (ie, patterns of shared meaning across all participants) and mapped to the corresponding eHealth literacy dimension. Finally, themes were refined and named based on original data (ie, quotes, codes).
Mixed methods data integration
As noted, quantitative data informed the structure of the qualitative study. Subsequently, the qualitative data were used to explain the quantitative findings. Importantly, the mixed methods approach provides deeper insight for model development than either method in isolation.22 We present our quantitative results first, followed by a joint display including key quantitative findings and qualitative in-depth themes for each eHealth literacy dimension. The resulting synthesis of quantitative and qualitative findings identified key targets for further model development and user-centred design.
Results
Participants’ characteristics
The quantitative survey was completed by 101 patients and 47 professionals (table 2). In total, 17 individuals (n=12 professionals; n=4 SSc patients; n=1 family member) participated in focus group discussions. All four patient participants were active members of a patient organisation and three had a medical and/or scientific background.
Participant characteristics (quantitative survey and qualitative focus groups)
Quantitative survey
The quantitative results are reported according to the described eHealth literacy dimensions (ie, ‘access’, ‘understand/appraise’, ‘apply’).
Access
Survey results indicate both patients and professionals have adequate access to ICT (table 3). The overwhelming majority of patients (91/101, 90.1%) had access to the internet. Professionals were commonly equipped with devices—yet smartphones, tablets and smartwatches were seldom used for clinical purposes.
Patient and healthcare professional access to ICT
Understand and appraise
The majority of patients felt confident using a smartphone/tablet (70/101, 69.3%) and/or portable/desktop computer (71/101, 70.3%). Patients indicated few problems comprehending health-related information on the internet ( =6.7, 95% CI: 6.2 to 7.3, range: 1–10). No notable differences were found in relation to sex or age. However, patients with less education (ie, compulsory education only) reported poorer understanding (
=6.7, 95% CI: 6.2 to 7.3, range: 1–10). No notable differences were found in relation to sex or age. However, patients with less education (ie, compulsory education only) reported poorer understanding ( =4.5 vs 7.1; SMD=0.81). Patients reported relatively limited ability to appraise eHealth information related to their health issues (
=4.5 vs 7.1; SMD=0.81). Patients reported relatively limited ability to appraise eHealth information related to their health issues ( =5.8, 95% CI: 5.1 to 6.4), find health apps (
=5.8, 95% CI: 5.1 to 6.4), find health apps ( =4.8, 95% CI: 4.2 to 5.4) and other eHealth offerings (
=4.8, 95% CI: 4.2 to 5.4) and other eHealth offerings ( =5.5, 95% CI: 4.9 to 6.2). Patients did not perceive that online resources increased their medical knowledge (
=5.5, 95% CI: 4.9 to 6.2). Patients did not perceive that online resources increased their medical knowledge ( =4.3, 95% CI: 3.7 to 4.9) or helped them making informed health decisions (
=4.3, 95% CI: 3.7 to 4.9) or helped them making informed health decisions ( =3.9, 95% CI: 3.4 to 4.5). Younger patients (<45 years) trended towards greater understanding of eHealth information (
=3.9, 95% CI: 3.4 to 4.5). Younger patients (<45 years) trended towards greater understanding of eHealth information ( =7.8 vs 6.6; SMD=0.48) and more confident decision-making based on online information (
=7.8 vs 6.6; SMD=0.48) and more confident decision-making based on online information ( =5.1 vs 3.8; SMD=0.43).
=5.1 vs 3.8; SMD=0.43).
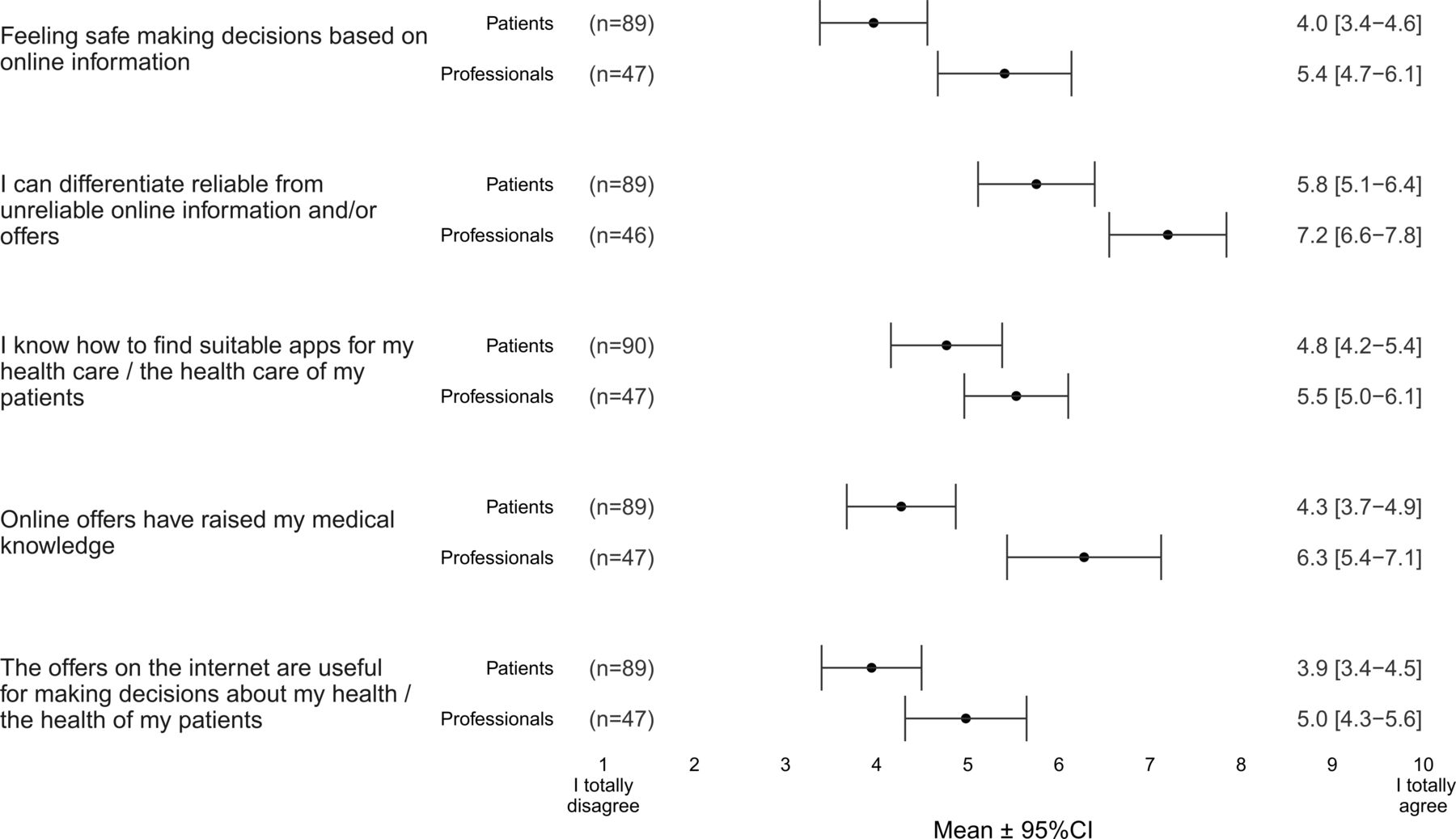
Compared with patients, healthcare professionals (figure 2) reported greater ability to assess reliability of online information ( =7.2 vs 5.8; SMD=0.55) and that eHealth resources increased their medical knowledge (
=7.2 vs 5.8; SMD=0.55) and that eHealth resources increased their medical knowledge ( =6.3 vs 4.3; SMD=0.70). Similar to patients, professionals reported limited benefit of online information for health decision-making (
=6.3 vs 4.3; SMD=0.70). Similar to patients, professionals reported limited benefit of online information for health decision-making ( =5.0, 95% CI: 4.3 to 5.6) and lacking knowledge in finding health apps (
=5.0, 95% CI: 4.3 to 5.6) and lacking knowledge in finding health apps ( =5.5, 95% CI: 5.0 to 6.1).
=5.5, 95% CI: 5.0 to 6.1).
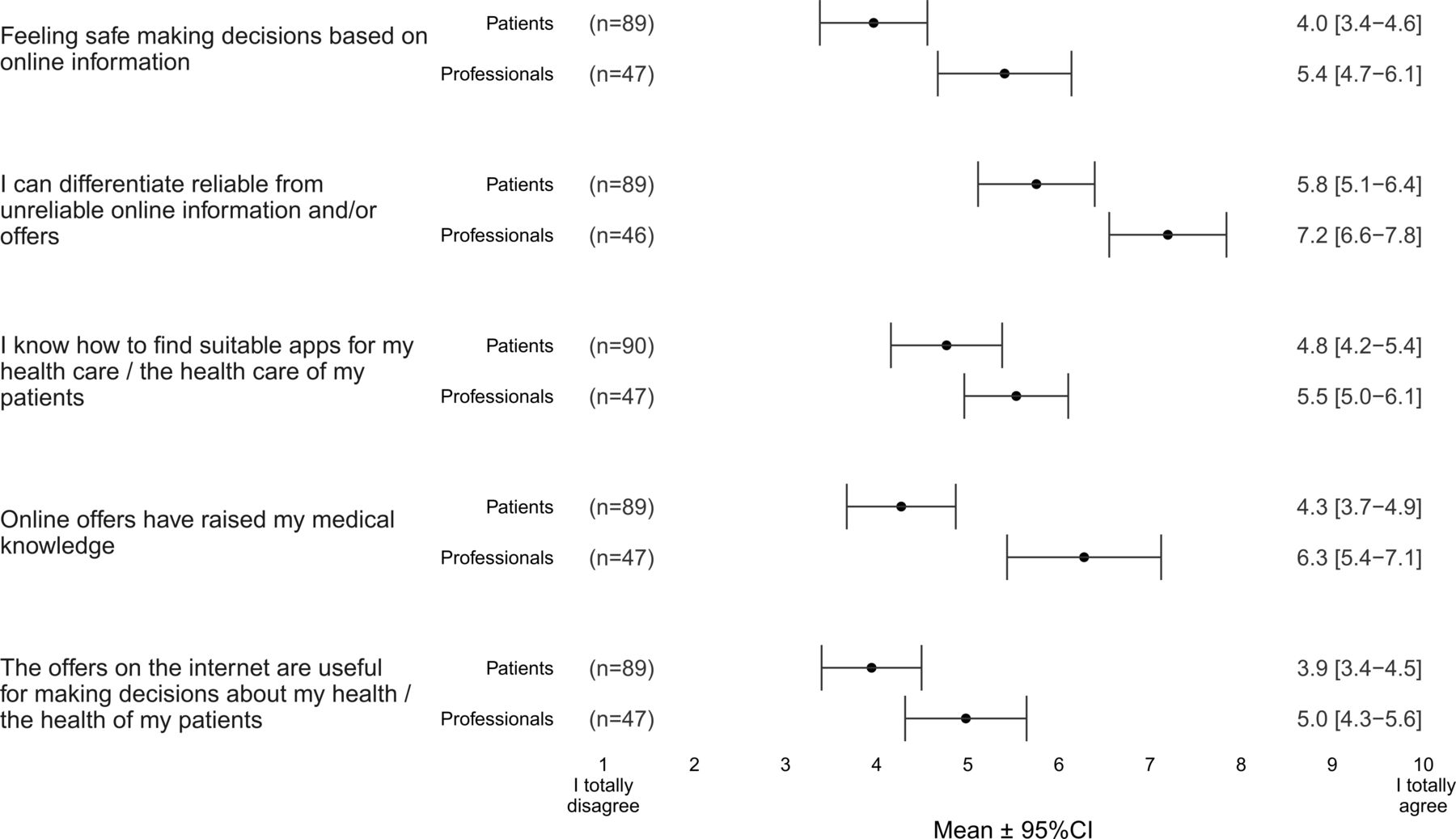
Patient and healthcare professional perceived understanding and appraising of eHealth (mean and 95% CI).
Apply
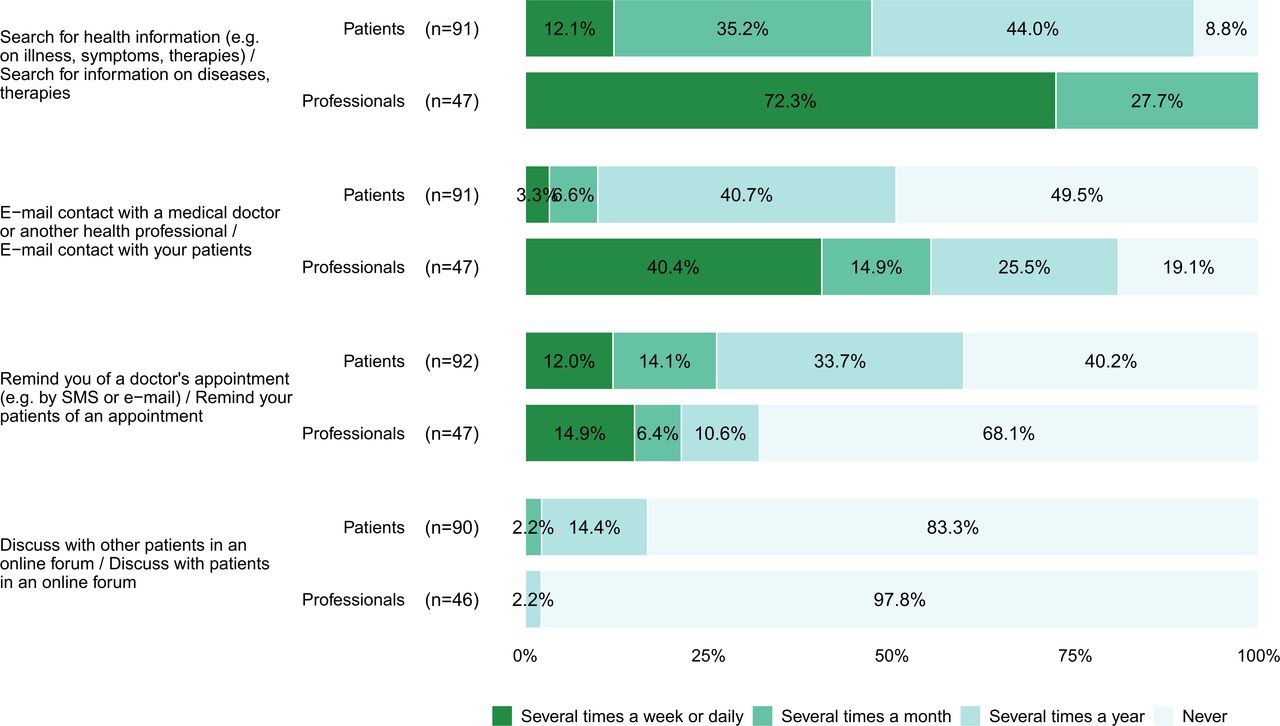
Notably, most patients (90/101, 89.1%) used the internet weekly—primarily for personal, private purposes (eg, communication, mobile applications, online news) (figure 3) but not for health purposes (figures 4 and 5). Similarly, almost all healthcare professionals had used the internet at least weekly for email communication (45/47, 95.7%), nevertheless only 19/47 (40.4%) used email weekly for patient communication. Both patients and professionals indicated relatively limited experience with web-based self-management support. Most patients had never used an online support group (70/92, 76.1%) or forum (75/90, 83.3%), while 45/46 (97.8%) of healthcare professionals had never participated in an online patient forum. Only 14/101 (13.9%) patients had used apps to improve their health compared with 20/47 (42.5%) professionals. In total, only 14/47 (29.8%) healthcare professionals had recommended eHealth apps to their patients.
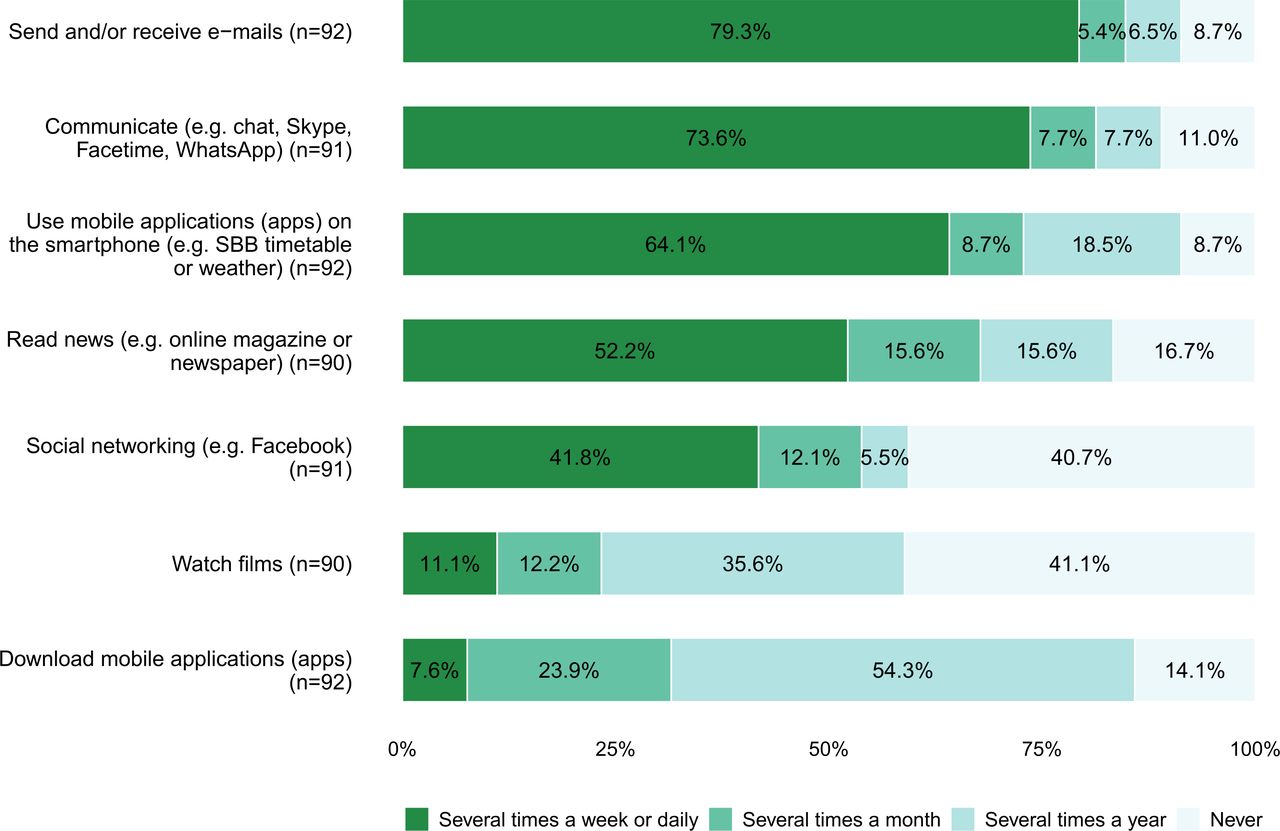
Internet use of patients for private purposes.

Internet use of patients and professionals for healthcare.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Internet use of patients for healthcare.
Qualitative results
Patient/professional eHealth perceptions and needs (ie, eHealth literacy and services) are described in six themes: ‘considering non-ICT-accessible groups’; ‘fitting patients’ and professionals’ technology’; ‘providing timely, understandable and safe information’; ‘empowering end-users in ICT and health decision-making skills’; ‘addressing perceptions of end-users’ and ‘putting people at the centre of technology’. These themes are described and illustrated (ie, participant quotes) in a joint display with key quantitative findings for each eHealth literacy dimension (table 4).
Joint display of key quantitative and qualitative findings for each eHealth literacy dimension
Synthesis of quantitative and qualitative findings on eHealth literacy domains
Access
Patients and healthcare professionals seem to be well equipped with hardware to access ICT and eHealth. However, our findings indicate it is important to consider those who are lacking ICT access when developing new eHealth services. Additionally, we need to consider interoperability to ensure that applications are fully supported by both patients’ and professionals’ devices and operating systems.
Understand and appraise
While patients and professionals feel confident using familiar technologies, they express needing guidance in understanding and appraising ICT/eHealth information. Valid, reliable information is key for empowering end-users to make high-quality decisions (ie, informed and aligned with values and preferences) for themselves or with their patients.
Apply
Most patients and professionals lacked experience with eHealth support (eg, apps, online forums, self-help groups), causing uncertainty and a variety of concerns. Involving stakeholders early in the development process is important for achieving user-centred design and supporting successful integration of onsite care and patient supports.
Discussion
This explanatory mixed methods study examined patient with SSc and healthcare professional eHealth literacy providing a deeper understanding of perspectives and needs for integrating web-based chronic care support. Notably, while technology is omnipresent in daily life, patients and professionals alike reported problems of interoperability of technology and indicated the need for education to effectively use eHealth applications. Additionally, the problem of equity in access was highlighted.
In respect to access, 89.1% of patients with SSc reported using the internet at least weekly—primarily for communication. These results mirror increasing numbers of people, especially older people, gained access to ICT/eHealth.33 In Switzerland, more than 90% of people use the internet—including more than half of people 75 years and older.34 However, our qualitative findings indicate the need for inclusive systems that are accessible to people with and without ICT access. In line with our findings, a European evaluation of more than 180 eHealth programmes/applications supporting integrated care for individuals with multiple morbidities highlighted eHealth barriers including insufficient ICT infrastructure and interoperability problems.35
We found that understanding and appraisal of eHealth in SSc are complicated by two interrelated factors—low-quality online information (as reported by focus group participants) and lack of confidence in using eHealth information for health decisions (as indicated by survey findings). We identified relatively low levels of perceived competency among patients with SSc and healthcare professionals in decision-making based on online information. These observations are similar to studies in patients with cancer.28 36 Patients with cancer as well as SSc indicated difficulties in locating valid, reliable internet content to support decision-making. Evaluation of online information is complicated by the low quality and sometimes false, frightening information on the web. Similarly, the variable disease trajectory of SSc and the many healthcare specialists involved can make it challenging for individuals to apply information to their specific SSc concerns. Participants in the present study echo challenges faced by rare disease patients worldwide,37 38 underscoring the importance of providing valid, reliable information that relates to an individual’s disease course and health decision-making needs (ie, patients and healthcare professionals). Importantly, our findings indicate that patients with SSc and professionals who care for them need guidance and support to better understand and appraise eHealth information/technologies. The eHealth-enhanced chronic care model recognises eHealth education as a critical component for chronic disease management2; yet theory-driven programmes to enhance end-users eHealth literacy are frequently lacking.35 39 Melchiorre et al35 evaluated eHealth within integrated care programmes and found that half of programmes provided healthcare professional training—yet few addressed patient training needs. Thus, recommendations guiding eHealth services are needed to generate a shared understanding of disease impact and self-management support.40 eHealth should be built on a scaffold of resources and information to support a shared illness perception and high-quality decision-making for patients and professionals alike.41 Key relational functions of eHealth applications include facilitating patient–provider communication, supporting shared decision-making and assuring productive technology-based interactions.2 24
In respect to apply, the present study highlights application as a critical roadblock to eHealth implementation for patients and professionals. Patients cited ethical, legal and social concerns (ie, data security, dependence on ICT, loss of interpersonal interactions) while providers noted logistical barriers (ie, lack of personnel, resources, time). Such concerns have been identified as factors limiting end-user acceptability and engagement sustainability of eHealth services.6 42 Nevertheless, our focus group discussions conducted during the quarantine imposed by the COVID-19 pandemic revealed positive attitudes about the utility of online support. Respondents expressed surprise about the quality of the online contact—even if they had not met the other person. Congruently, data from patients with chronic lung diseases show that experience using eHealth can demystify ICT and is associated with more positive attitudes about the usefulness of eHealth resources.43 Thus, providing patients with SSc and healthcare professionals with more ICT/eHealth experiences may help create more positive attitudes and beliefs—especially in relation to peer-led support groups. Lack of knowledge about what happens at support group meetings and not having reliable transportation to attend meetings are common barriers for patients with SSc.44 One way to surmount such barriers is to utilise online groups to overcome geographic distance. Indeed, existing literature supports the notion that rare disease patients can benefit from online peer-to-peer support and mentorship.45 Shaping patients’ and healthcare professionals’ attitudes may foster eHealth implementation. Specifically, providing guidance for using eHealth, as well as data supporting its utility for improving outcomes, can shift current perspectives and proper uptake of eHealth interventions.46
Additionally, our qualitative inquiry revealed user-centredness and equity as critical elements in developing eHealth-enhanced models of care. Participants highlighted the need to link eHealth and onsite care to ensure that resources are equitably accessible by individuals who lack ICT, have limited digital literacy (eg, less educated patients) and/or are geographically dispersed. For example, digital care for older adults may be most effective using a hybrid format (ie, combination of digital and in-person presence).47 It is worthwhile to note that videoconferencing (eg, for home-based groups) is feasible even for those with limited eHealth literacy as long as appropriate ICT infrastructure and eHealth training are provided.48 Importantly, eHealth may not directly reduce staff and costs49 and is intended as a complement to care rather than a means to replace current practices.50
Relative strengths of this study include diverse data sources (ie, quantitative and qualitative) from a range of stakeholders that were geographically diverse (ie, within Switzerland and Europe/USA) and spanned a range of experience with SSc. It merits mention that some expert patients had professional backgrounds including health policy, medicine, nursing and/or biomedical research, thus may not be representative of all patients with SSc. A limitation of the quantitative survey is the Swiss sample, making it difficult to broadly generalise our results internationally. The international focus group largely supported our findings. However, only one patient participated in the international focus group so caution is warranted in generalising findings more widely. Furthermore, we did not include general practitioners and non-rheumatology specialists in the focus groups what limits conclusions that can be made regarding multiprofessional management. Further research is needed to better understand and improve eHealth literacy and multiprofessional support in patients with SSc. Importantly, such work could include the European Reference Network on Rare and Complex Connective Tissue and Musculoskeletal Diseases (ERN ReCONNET) to increase generalisability.51 Moreover, measuring eHealth literacy is challenging as validated instruments have not been updated to fully address the current state of platforms (ie, social media) and internet use patterns.26 27 While rare disease populations have been considered internet ‘power users’, no tools specifically address the unique ways that rare disease patients use the internet to learn about their condition and crowdsource solutions.52 Future research may focus on eHealth literacy in broader rare disease populations to determine if findings are SSc-specific or representative of experiences of rare disease patients more broadly. Additional investigation may focus on the active role of patients with SSc in designing eHealth-enhanced care (ie, co-creating solutions).53 It would be important to know the optimal model of care to empower and support active involvement of patients and coordinate disease management across multiple healthcare professionals involved in the care pathway.
Conclusions
To develop an eHealth-supported model of care, the interoperability of patient and provider technology is foundational. Both patients and healthcare professionals could benefit from structured, systematic eHealth guidance and training to help them identify valid, reliable and pertinent patient information. A key aspect of eHealth-supported models of care is to facilitate patient–provider communication to support shared decision-making and self-management. To ensure equity, design must also consider those individuals who have limited eHealth literacy and/or lack access to ICT.
Data availability statement
Data are available upon reasonable request. All data relevant to the study are included in the article or uploaded as supplementary information. The datasets generated and/or analysed during this study are included in this published article or can be made available from the corresponding author on reasonable request. The datasets generated and/or analysed during this study are included in this published article or can be made available from the corresponding author on reasonable request.
Ethics statements
Patient consent for publication
Ethics approval
The overall MANagement Of Systemic Sclerosis (MANOSS)21 project was reviewed and approved by the responsible Swiss ethics committee in September 2018 (EKNZ 2018‐01206). Patient information forms and informed consent documents complied with the Swiss ethics committee’s templates. All participants received a written explanation of the purpose of the study, the voluntary nature of their participation and the use of their contributions.
Acknowledgments
We wish to thank the participating patients and healthcare professionals, the Swiss Scleroderma patient association and the focus group participants for their generosity and collaboration. Special thanks to Ms Sabine Herzig for her valuable support during the questionnaire data collection.
References
Footnotes
Twitter @kocheragnes
Contributors AK, MS, AAD, PMV and DN conceived and designed the work. AK, JB, PMV, DD, OD and UAW acquired the data of the first study phase; and AK, MS, CB, JB, PK-H and DN analysed it. AK, PK-H, JB and DN acquired and analysed the data of the second study phase. AK, MS, CB, JB, PK-H and DN contributed to interpreting the data and drafting the manuscript. All authors revised the subsequent drafts critically for important intellectual content. All authors read and approved the final manuscript.
Funding This publication is part of the Swiss MANagement Of Systemic Sclerosis (MANOSS) study and received funding from the Swiss Nursing Science Foundation and the Swiss League Against Rheumatism.
Competing interests AK has received financial support from the Swiss Nursing Science Foundation, Swiss League Against Rheumatism and University of Basel for her dissertation and from Sandoz to support the development of an eLearning module for patients with rheumatic diseases. She is an unpaid member of the EULAR recommendations for non-pharmacological management of autoimmune CTDs task force. AAD is an assistant professor of nursing at Boston College whose research focuses on developing more person-centered approaches to care. He received funding from Boston College and the US National Institutes of Health (USA) and received funding to cover travel expenses for his faculty participation in a Swiss rare diseases summer school. OD has/had consultancy relationship with and/or has received research funding from or has served as a speaker for the following companies in the area of potential treatments for systemic sclerosis and its complications in the last three years: Abbvie, Acceleron, Amgen, AnaMar, Arxx, Baecon, Blade, Bayer, Boehringer Ingelheim, ChemomAb, Corbus, CSL Behring, Galapagos NV, Glenmark, GSK, Horizon (Curzion), Inventiva, iQvia, Italfarmaco, Kymera, Lupin, Medac, Medscape, Mitsubishi Tanabe, MSD, Novartis, Pfizer, Roche, Roivant, Sanofi, Serodapharm, Topadur, Target Bioscience and UCB. Patent issued mir-29 for the treatment of systemic sclerosis (US8247389, EP2331143). The remaining authors declare they have no financial and non-financial interests that are directly or indirectly related to this work.
Provenance and peer review Not commissioned; externally peer reviewed.